plasma sodium as a predictor of death and non-osmotic ... · plasma sodium as a predictor of death...
TRANSCRIPT

Plasma sodium as a predictor
of death and non-osmotic sodium storage
Prof. Mustafa ARICI, MD Hacettepe University Faculty of Medicine
Ankara-TURKEY
An update on sodium in CKD stage 5D

2 (new) questions ....
1) Will plasma sodium be a new marker of mortality in stage 5D CKD patients?
2) Is plasma sodium reflecting the “whole lot” of sodium in the body in relation to body water, or is there sodium “hidden” in elsewhere ?

We are eating too much salt....

in Turkey....

SALTURK Study
• 1970 participants (>18 years old and able to provide a medical history and 24-h urine sample)
• Random allocation from 14 cities
• February-April 2008
• The mean daily urinary Na+: 308.3±143.1 mmol/day
• Mean daily salt intake of 18.01 g/day
Erdem Y, Arici M, et al. Blood Press. 2010 Oct;19(5):313-8

CDC: Salt in US
About 90% of Americans aged 2 years or older eat too much sodium.*
44% of the sodium we eat comes from 10 types of foods.
.
Reducing the sodium Americans eat by 1,200 mg per day on average added up to $20 billion
a year in medical costs
http://www.cdc.gov/vitalsigns/Sodium/index.html
Top Sources of Sodium in the Diet
Breads and rolls
Cold cuts and cured meats
Pizza
Poultry
Soups
Sandwiches
Cheese
Pasta dishes
Meat dishes
Snacks
How much salt CKD patients are eating ?

• 373 consecutive outpatients with CKD stages 1–5 (not on dialysis; men: 52.3%, mean age: 51.6±15.4 years)
• All patients had at least 3 or more nephrology visits and received information on reducing their sodium intake
• 2 consecutive 24-hour urinary sodium levels were obtained
Kutlugün AA, Arıcı M, et al. Nephron Clin Pract. 2011;118(4):c361-6.
How much salt CKD patients are eating ?

Kutlugün AA, Arıcı M, et al. Nephron Clin Pract. 2011;118(4):c361-6.
How much salt CKD patients are eating ?
10.5
g/day
10.8
g/day 10.1
g/day 9.1
g/day 7.4
g/day

Mc Causland FR, et al. Kidney International (2012) 82, 204–211;
How much salt CKD 5HD patients are eating?

How much salt CKD 5HD patients are eating?
• A post-hoc analysis of the Hemodialysis (HEMO) Study
– 1770 subjects; mean age 58 (±14) years; 44% were men, 63% were black, and 44% were diabetic
– Reported dietary intake was assessed from 2-day diet diary assisted recalls. Recall was performed on one dialysis and one non-dialysis day (most often on consecutive days) at annual intervals.
Mc Causland FR, et al. Kidney International (2012) 82, 204–211;

Mean reported diet-Na was
2240 (±1050) mg/day,
Median was 2080
(IQR: 1490–2850)mg/day
Mean NaCl intake 5.5 (±2.6) g/day
Median NaCl intake 5.2 (3.7-7.1) g/day
How much salt CKD 5HD patients are eating?
Mc Causland FR, et al. Kidney International (2012) 82, 204–211;

Dietary Sodium in CKD 5HD UF requirement- Sytolic BP - Serum Na
Distribution of UF requirement, SBP, and serum Na, and associations with daily dietary sodium intake (g/day
Mc Causland FR, et al. Kidney International (2012) 82, 204–211;

Association between quartiles of dietary sodium intake and mortality. Hazard ratios (95% confidence intervals (CIs)) for all cause mortality according to quartiles
(Q; referent Q1) of reported daily dietary sodium intake (mg/day)
Mc Causland FR, et al. Kidney International (2012) 82, 204–211;
Dietary Sodium in CKD 5HD Mortality
• However, the clinical implications of these findings may be limited considering the small magnitude of association (90 ml requisite ultrafiltrate per 1000 mg increment in diet-Na intake; 130 ml ultrafiltrate per 1 mg/kcal increment in Na:Cal).
Dietary Sodium in CKD 5HD Mortality
Mc Causland FR, et al. Kidney International (2012) 82, 204–211;

• It is possible that in HD patients other sources of sodium (e.g., ‘loading’ from relatively hypernatremic dialysate), non-osmotically mediated thirst (e.g., from transient intravascular hypovolemia following dialysis), or habitual drinking may have a greater role in determining IDWG and pre-dialysis SBP than previously recognized.
Dietary Sodium in CKD 5HD Mortality
Mc Causland FR, et al. Kidney International (2012) 82, 204–211;

Dietary Sodium & Mortality in CKD-5D ?
• Problems with estimating dietary sodium intake ?
• 95 % confidence interval of the spline graphs crosses the hazard ratio of 1, which indicates that the null hypothesis cannot be rejected ?
• J-shaped or U-shaped association ?
• No relation with blood pressure ?
Mehdi Rambod, Ramin Tolouian. Kidney International (2012) 82, 130 – 132
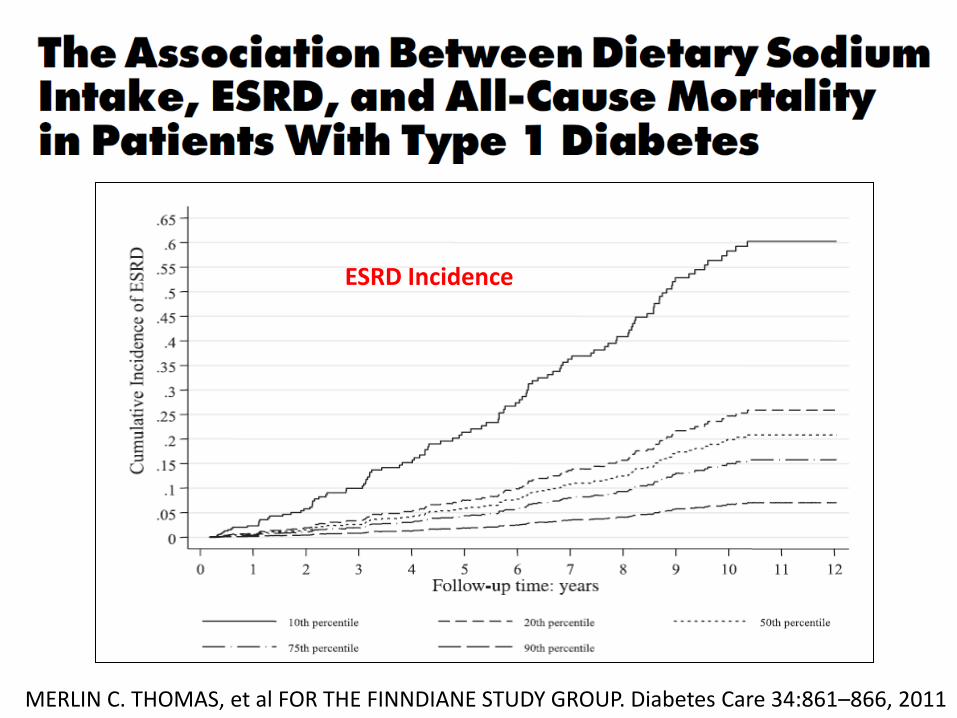
MERLIN C. THOMAS, et al FOR THE FINNDIANE STUDY GROUP. Diabetes Care 34:861–866, 2011
All-cause mortality ESRD Incidence

• 305 incident patients, (129 men, 176 women), mean age of 59.4±14.2 years
• Low average sodium intake independently predicted the increased risk for overall and cardiovascular death after adjusting for recognized confounders.
• Further adjustment for dietary protein, energy, and other nutrient intakes individually had minimal impact on the association between average sodium intake and overall death, with hazard ratios varying between 0.35 and 0.44, and cardiovascular death, with hazard ratios varying between 0.06 and 0.11.
Clin J Am Soc Nephrol 5: 240–247, 2010
My 1st question?
Will plasma sodium be a
new marker of mortality in
stage 5D CKD patients?

....or, what's so bad about plasma sodium??

Hyponatremia & Mortality
Hyponatremia is strongly associated with an increased risk of death (47
%); even mild hyponatremia (serum sodium concentration 130-134
mEq/L) is associated with a 37% increased risk of in-hospital mortality
Waikar SS, Mount DM, Curhan GC. Am J Med. 2009; 122(9):857-865.

Then, is plasma sodium also bad for CKD 5D ?
Waikar SS, Curhan GC, Brunelli SM. Am J Med. 2011; 1224:77-84

Serum Na & Mortality in CKD-5HD
• 1549 oligoanuric participants in the HEMO study
– Mean (SD) age was 57.7 (14.2) years; 57% of participants were women; 64.2% were black
• Primary outcome: time to death from any cause
• Secondary analyses: time to death from cardiovascular disease
• The median number of serum sodium measurements per subject was 5 (IQR:3-8)
Waikar SS, Curhan GC, Brunelli SM. Am J Med. 2011; 1224:77-84

Baseline Serum Na
Waikar SS, Curhan GC, Brunelli SM. Am J Med. 2011; 1224:77-84

Serum Sodium in CKD-5HD
• The most statistically significant bivariable predictors of
Waikar SS, Curhan GC, Brunelli SM. Am J Med. 2011; 1224:77-84
Higher serum sodium Black race Longer vintage Higher estimated Dry weight Serum albumin Serum creatinine
Lower serum sodium Diabetes Higher UF volume Serum glucose

• Lower serum sodium concentration was associated with greater all-cause mortality (P <.001).
• Considered as a continuous variable, each 4-mEq/L (the observed SD in the sample) increment in serum sodium concentration was associated with a hazard ratio (HR) for all-cause mortality of 0.84 (95% confidence interval [CI], 0.78-0.90).
Serum Na & Mortality in CKD-5HD
Waikar SS, Curhan GC, Brunelli SM. Am J Med. 2011; 1224:77-84

Upon multivariable adjustment, the association between serum sodium
concentration and mortality was modestly attenuated, but remained statistically significant: HR 0.89; 95%
CI, 0.82-0.96.
Serum Na & Mortality in CKD-5HD
Waikar SS, Curhan GC, Brunelli SM. Am J Med. 2011; 1224:77-84

Serum Na & Mortality in CKD-5HD
Quartile 1 (115-136) Quartile 2 (137-138) Quartile 3 (139-141) Quartile 4 (142-154)
Waikar SS, Curhan GC, Brunelli SM. Am J Med. 2011; 1224:77-84.

Serum Na & Mortality in CKD-5HD
Waikar SS, Curhan GC, Brunelli SM. Am J Med. 2011; 1224:77-84
Quartile 1 (115-136) Quartile 2 (137-138) Quartile 3 (139-141) Quartile 4 (142-154)

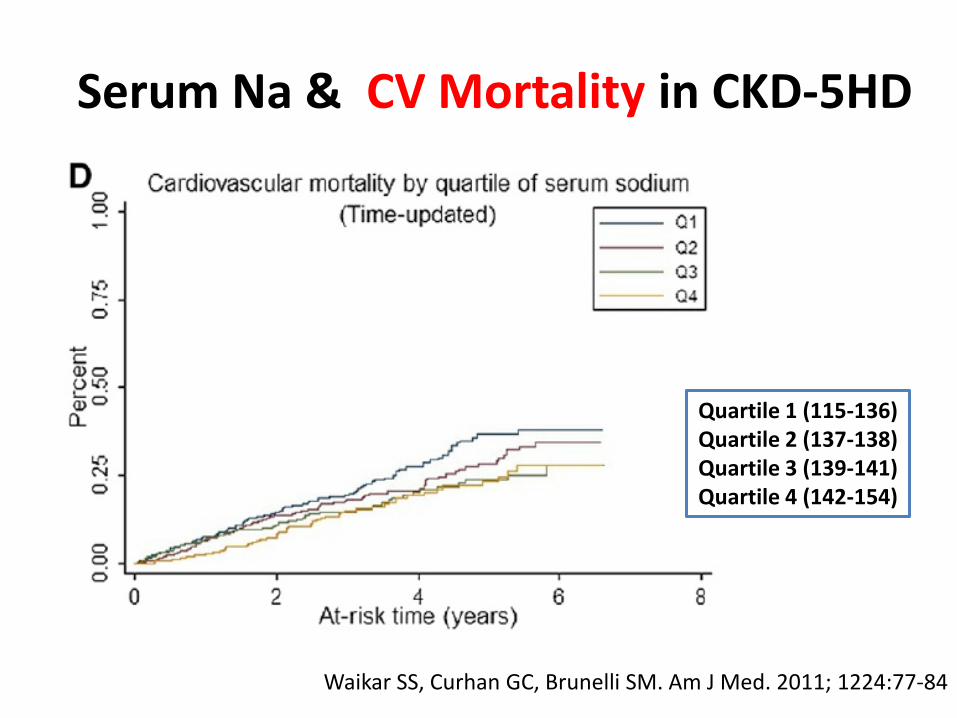
Serum Na & CV Mortality in CKD-5HD
Quartile 1 (115-136) Quartile 2 (137-138) Quartile 3 (139-141) Quartile 4 (142-154)
Waikar SS, Curhan GC, Brunelli SM. Am J Med. 2011; 1224:77-84
Serum Na & CV Mortality in CKD-5HD
Waikar SS, Curhan GC, Brunelli SM. Am J Med. 2011; 1224:77-84
Quartile 1 (115-136) Quartile 2 (137-138) Quartile 3 (139-141) Quartile 4 (142-154)

• That low serum sodium concentrations were associated with mortality in this population lends favor to the interpretation that hyponatremia might be directly toxic.
• The mechanism(s) by which low serum sodium concentration may affect survival are not entirely clear.
Serum Na & Mortality in CKD-5HD
Waikar SS, Curhan GC, Brunelli SM. Am J Med. 2011; 1224:77-84

• Excessive free water intake or reduced solute intake ?
• Angiotensin 2 as a potent dipsogenic effect ?
• Interdialytic weight gain ?
• Cyclical alterations in serum osmolality ?
– Dialysate sodium
– Sodium modeling ?
Serum Na & Mortality in CKD-5HD Alternative Explanations ?
Waikar SS, Curhan GC, Brunelli SM. Am J Med. 2011; 1224:77-84
Am J Kidney Dis. 59(2):238-248,2012
Is plasma sodium also bad for CKD 5D ?

• 11,555 patients from 12 countries in the Dialysis Outcomes and Practice Patterns Study (DOPPS), phases I (1996-2001) and III (2005-2008).
• Median follow-up was 12 months, with 1,727 deaths (15%) occurring during the study period (12,274 patient-years).
• The first 3 serum sodium measurements to compute each patient’s mean serum sodium level
Serum Na & Mortality in CKD-5HD
Am J Kidney Dis. 59(2):238-248, 2012

• Serum sodium level was associated
Serum Na Levels in CKD-5HD
Am J Kidney Dis. 59(2):238-248, 2012
Positively with Male sex Black race Body mass index Serum albumin Serum creatinine
Negatively with Neurologic disease Psychiatric disease WBC count Intradialytic weight loss (0.16 mEq/L lower per 1% loss)

Higher mean serum sodium level was associated with lower all-cause
mortality
Models with various levels of adjustment showed that this
association was significant and consistent.
Serum Na & Mortality in CKD-5HD
Am J Kidney Dis. 59(2):238-248, 2012

• After controlling for 10 patient characteristics, 14 comorbid conditions, 5 laboratory parameters, and facility clustering effects and stratifying by DOPPS phase and country, patients with serum sodium levels <137 mEq/L had a 45% higher risk of death compared with patients with serum sodium levels >140 mEq/L (hazard ratio [HR], 1.45; 95% confidence interval [CI], 1.26-1.67; model 5).
Serum Na & Mortality in CKD-5HD
Am J Kidney Dis. 59(2):238-248. © 2012

Serum Na & Mortality in CKD-5HD

Serum Na & Mortality in CKD-5HD
Am J Kidney Dis. 59(2):238-248. © 2012

• A scatterplot confirmed the lack of correlation between dialysate sodium concentration and mean serum sodium level.
• Compared with HD patients with mean serum sodium levels ≥140 mEq/L and a dialysate sodium prescription of 140 mEq/L (reference), mortality risk was higher in HD patients with mean serum sodium levels <140 mEq/L and dialysate sodium prescriptions of all 3 categories (P0.05).
Dialysate Na & Mortality in CKD-5HD
Am J Kidney Dis. 59(2):238-248. © 2012

Dialysate Na & Mortality in CKD-5HD
Am J Kidney Dis. 59(2):238-248. © 2012

• Although our mortality analyses were adjusted for patient characteristics and comorbid conditions, serum sodium level was associated with certain indicators of general health, which might point to an apparently “frail phenotype” of patients with lower serum sodium levels.
• Despite adjusting extensively for case-mix, the possibility of residual confounding remains and causality cannot be established in the setting of an observational study.
Dialysate Na & Mortality in CKD-5HD
Am J Kidney Dis. 59(2):238-248. © 2012

My 2nd question?
Is plasma sodium reflecting the “whole lot” of sodium in the body in relation to body water, or is there
sodium “hidden” in elsewhere ?

J Clin Invest. 1958 Sep;37(9):1236-56.
What is all going with serum Na?

Serum Sodium Concentration & Osmolarity
J Clin Invest. 1958 Sep;37(9):1236-56.

Serum Sodium Concentration in Relation to Nae + Ke / TBW
Edelman equation Plasma water [Na + ] = 1.11 x (Na e + K e )/TBW – 25.6
J Clin Invest. 1958 Sep;37(9):1236-56.
Clasical Sodium Model
• 2-compartment model
• Na + and its accompanying anions are the principal extracellular osmoles and act to hold water in the extracellular space; conversely K + salts account for almost all the intracellular osmoles and act to hold water within the cells.
Titze J. Blood Purif 2008;26:95–99

Accumulation of 140 mmol Na + thus must inevitably lead to 1
liter extracellular volume retention to maintain isosmolality
in this functional two-compartment model.
Clasical Sodium Model
Titze J. Blood Purif 2008;26:95–99

Water-free Na+ Retention

Water-free Na+ Retention
Heer M, et al. Am J Physiol Renal Physiol 278:F585-F595, 2000.

Water-free Na+ Retention
Heer M, et al. Am J Physiol Renal Physiol 278:F585-F595, 2000.

1) An osmotically inactive Na + storage mechanism (as characterized by a cation excess relative to water),
2) An osmotically neutral cation exchange mechanism (as characterized by a replacement of K + ions with Na + ions).
Water-free Na+ Retention
Titze J. Blood Purif 2008;26:95–99

Osmotically Inactive Sodium Storage in the Skin
• Compared with 0.1% NaCl diet, the skin Na + content in rats fed 8% NaCl diet was increased by 35–45%.
Am J Physiol Heart Circ Physiol 287:H203-H208, 2004
• This finding draws attention to the potential role of the polyanionic character of the skin GAGs in the regulation of osmotically inactive skin Na + storage.
Titze J. Blood Purif 2008;26:95–99

• Long-term salt deprivation was associated with decreased negative charge density of skin GAGs. This decrease in the polyanionic character was associated with the mobilization of osmotically inactive Na from reservoir tissue
Markus Schafflhuber, et al. Am J Physiol Renal Physiol 292:F1490-F1500, 2007
Osmotically Inactive Sodium Storage in the Skin

Traditional view of Na and fluid retention
British Journal of Nutrition (2009), 101, 1286–1294

Alternative view of Na and fluid retention
British Journal of Nutrition (2009), 101, 1286–1294

Salt is not “silent” under the skin....
NATURE MEDICINE VOLUME 15 [ NUMBER 5 [ MAY 2009

Salt is getting under our skin
Ton J. Rabelink and Joris I. Rotmans. Nephrol Dial Transplant (2009) 24: 3282–3283

Sodium sensing in the interstitium
• Extrarenal regulatory mechanisms at the tissue level are operating to maintain interstitial electrolyte homeostasis in a concerted action of local interstitial control of the internal environmental composition and that subsequent renal adjustments are distal to this process.
Titze J & Machnik A. Current Opinion in Nephrology and Hypertension 2010, 19:385–392

Classical view of Sodium Homeostasis
Titze J & Machnik A. Current Opinion in Nephrology and Hypertension 2010, 19:385–392

Alternative view of Sodium Homeostasis
Titze J & Machnik A. Current Opinion in Nephrology and Hypertension 2010, 19:385–392
tonicity-responsive enhancer binding protein


VEGF-C levels are increased by a high-salt diet in proteinuric CKD patients and in healthy
subjects, supporting a role for VEGF-C-mediated interstitial regulatory mechanisms in salt
homeostasis in humans

In conclusion.... Salt is still very dangerous

• Look carefully to your patient’s lab tests, especially the plasma sodium....
In conclusion.... there is more in plasma sodium than we think....


PNAS 104 (41): 16281-16286, 2007

In conclusion.... look carefully under the skin of your patients...there is more
happening there than we think...
In conclusion......
Medicine is
a science of
uncertainty and an
art of probability
William Osler

“The more I read,
the more I
acquire, the more
certain I am that
I know nothing.”
François-Marie Arouet de Voltaire
In conclusion......
