pneumonia by dr. abdelaty shawky assistant professor of pathology
DESCRIPTION
Pneumonia By Dr. Abdelaty Shawky Assistant professor of pathology. PNEUMONITIS. * Classification: 1. Bacterial pneumonia: lobar pneumonia & bronchopneumonia. 2. Viral (interstitial) pneumonia: influenza, measles, chicken pox. - PowerPoint PPT PresentationTRANSCRIPT
PneumoniaPneumoniaByBy
Dr. Abdelaty ShawkyDr. Abdelaty ShawkyAssistant professor of pathologyAssistant professor of pathology
PNEUMONITIS
* Classification:1. Bacterial pneumonia: lobar pneumonia & bronchopneumonia.
2. Viral (interstitial) pneumonia: influenza, measles, chicken pox.
3. Loeffler’s (parasitic) pneumonia: Bilharziasis, ascaris &
ankylostomiasis.
4. Granulomatous pneumonia: T.B, sarcoidosis, leprosy, syphilis,
actinomycosis .
5. Lipoid pneumonia: due to aspiration of oily nasal drops.
6. Irradiation pneumonia.

LOBAR PNEUMONIALOBAR PNEUMONIA

* Def: acute diffuse fibrinous inflammation of one or
more lung lobes.
* Etiology:
• Age: middle age.
• Predisposing factors: low resistance.
• Causative organism: pneumococci.
• Route of infection: droplet infection.

* Pathogenesis:• Pneumococci are inhaled to reach alveoli.
They cause acute inflammaion with excess fluid exudate. This fluid exudate pass from one alveolus to another rapidly through the inter- alveolar pores of cohn to involve the whole lung lobe. The fluid exudate expel air away from the alveoli producing a firm airless lobe leading to consolidation (hepatisation) of the affected lobe.
1 .Stage of congestion 2 .Stage of red hepatization
3 .Stage of gray hepatization
4 .Stage of resolution
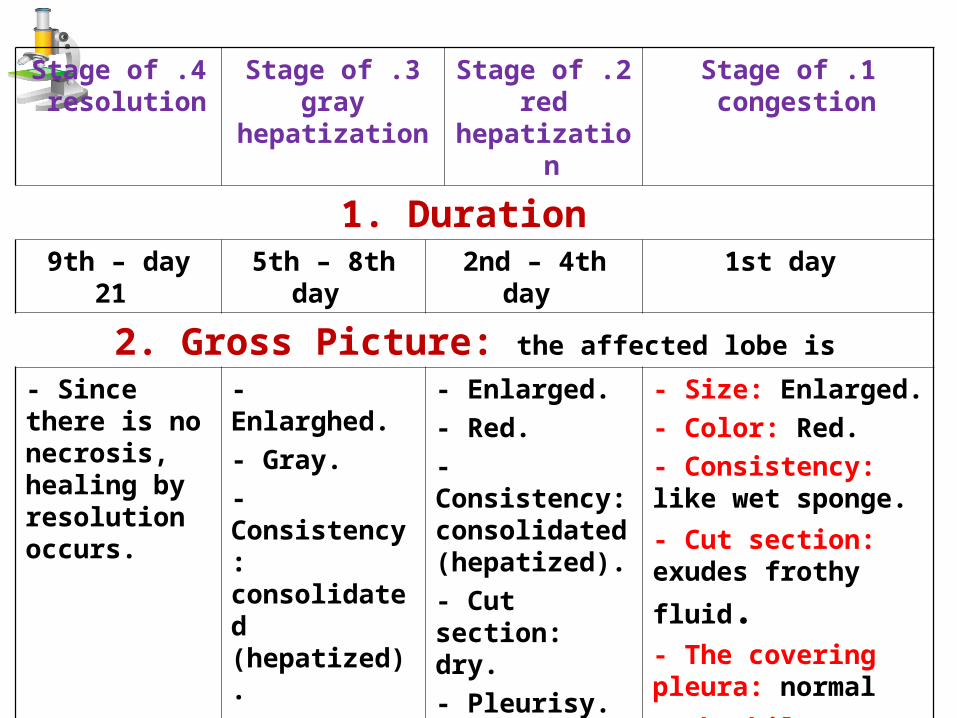
1. Duration 1st day 2nd – 4th day 5th – 8th day 9th – day 21
2. Gross Picture: the affected lobe is
- Size: Enlarged.- Color: Red.- Consistency: like wet sponge.
- Cut section: exudes
frothy fluid.- The covering pleura: normal
- The hilar L.Ns.: normal
- Enlarged.- Red.- Consistency: consolidated (hepatized).- Cut section: dry.- Pleurisy.- Enlarged hilar LNs.
- Enlarghed.- Gray.- Consistency: consolidated (hepatized).- Cut section: dry.- Pleurisy.
- Enlarged hilar
LNs.
- Since there is no necrosis, healing by resolution occurs.

Lobar pneumonia of Lobar pneumonia of upper lobeupper lobe
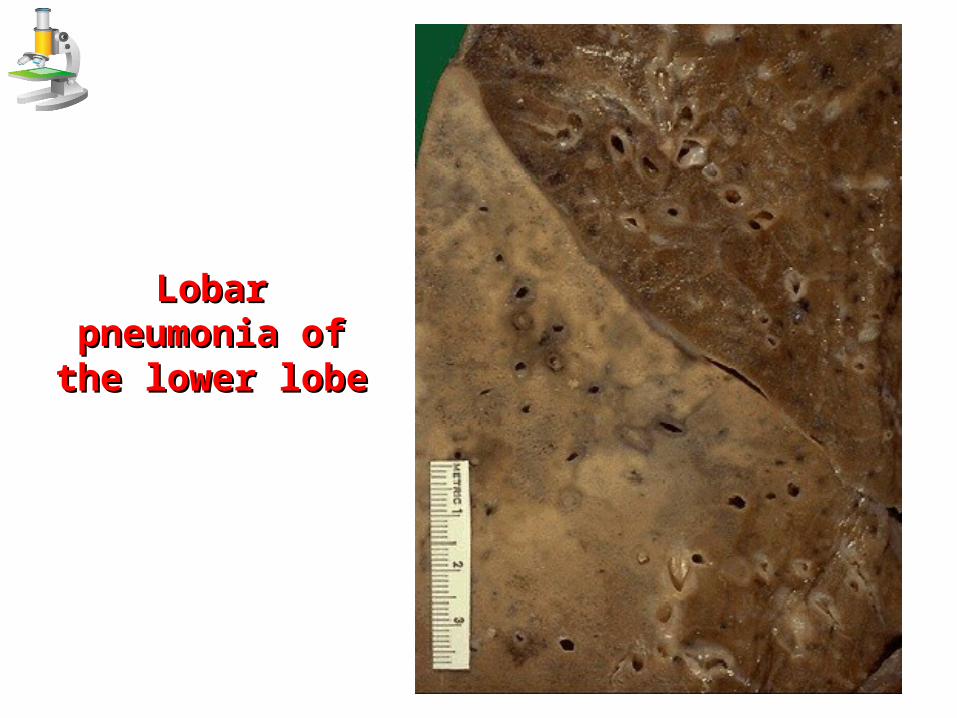
Lobar pneumonia of Lobar pneumonia of the lower lobethe lower lobe

1 .Stage of congestion
2 .Stage of red hepatization
3 .Stage of gray hepatization
4 .Stage of resolution
3. Microscopic Picture 3. Microscopic Picture a. Alveolar capillaries:Congested.b. Alveolar walls: thickened.c. Alveolar spaces:Show bacteria & fluid exudate.
a. Alveolar capillaries:Congested.b. Alveolar walls: thickened.c. Alveolar spaces:
Show bacteria, fibrin, RBCs and
polymorphs.
a. Alveolar capillaries:Less congestedb. Alveolar walls: thin.c. Alveolar spaces:Show dead bacteria, shrinked fibrin, hemolysed RBCs, excess polymorphs and macrophages.

Lobar pneumonia; red hepatization
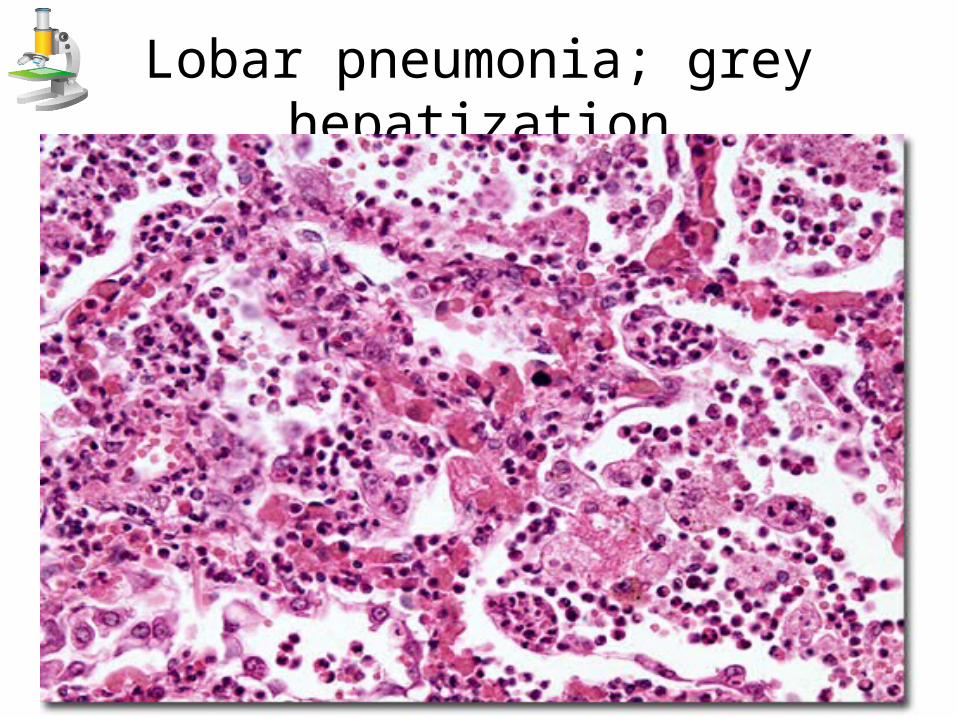
Lobar pneumonia; grey hepatization

1 .Stage of congestion
2 .Stage of red hepatization
3 .Stage of gray hepatization
4 .Stage of resolution
4. Clinical course - Fever, cough, dyspnea and chest pain.
- At about 9th day the disease ends by crisis (sudden improvement), however
death may occur due to severe toxaemia.
1 .Stage of congestion
2 .Stage of red hepatization
3 .Stage of gray hepatization
4 .Stage of resolution
5. Complications
1. Spread of infection: direct, lymphatic and blood (toxaemia, septicaemia).
2. Lung fibrosis due to failure of resolution.3. Post-pneumonic lung abscess.

BRONCHOPNEUMONIA BRONCHOPNEUMONIA

* Def: Acute suppurative inflammation of bronchioles and
adjacent alveoli characterized by patchy lung consolidation.
* Etilogy:
– Age: extremes of age (young & elderly).
– Predisposing factors: low resistance and bronchitis.
– Causative bacteria: staphylococci, streptococci & H.
influenza.
– Route of infection: endogenous invaders and exogenous
invaders (droplet infection).

* Gross picture: Bilateral.Basal.Multiple consolidated yellowish patches
exuding pus on pressure. Several patches may coalesce to produce confluent bronchopneuomonia.
Enlarged hilar L. nodes.

BronchopneumoniaBronchopneumonia

BronchopneumoniaBronchopneumonia

* Microscopic Picture:I. The broncioles show:
Their lumen shows: necrotic epithelial cells, polymorphs & pus cells.
Their lining: ulceration. Their walls: congested capillaries, neutrophils and
pus cells & exudate.II. The adjacent alveoli show: 3 successive zones: zone
of alveolitis then zone of alveolar collapse and a zone of alveolar dilatation (compensatory emphysema).


* Complications:1. Spread of infection: direct, lymphatic and
blood (toxaemia, septicaemia).2. Lung fibrosis due to failure of resolution.3. Post-pneumonic lung abscess.4. Bronchiectasis.
ThanksThanks