poor glycemic control during hospitalization · poor glycemic control during hospitalization . ......
TRANSCRIPT

Poor Glycemic Control During Hospitalization
Robert J. Rushakoff, MD Professor of Medicine
University of California, San Francisco
Rational Approach at a Time of Uncertainty

Disclosures
Speaker: Merck* Speaker: Novo-Nordisk* * Nonbranded

"Each blind man perceived the elephant as something different: a rope, a wall, tree trunks, a fan, a snake, a spear..."
Education Nurses
Physicians Students
Patient Education
Transitions Outpatient to Inpatient Inpatient to Inpatient
Inpatient to Outpatient
Data Collection
Medical Errors Glucometrics
Diabetes Management
Order Entry Smart Orders
Dosing Calculators
Jargon CQI
Patient Assessment of Skills, Education
Diabetes Assessment Form
1.-----------------------------------------------------------------------------
2.-----------------------------------------------------------------------------
3.-----------------------------------------------------------------------------
4.-----------------------------------------------------------------------------
5.-----------------------------------------------------------------------------
6.-----------------------------------------------------------------------------
7.-----------------------------------------------------------------------------
8.-----------------------------------------------------------------------------
9.-----------------------------------------------------------------------------
10.----------------------------------------------------------------------------
11.----------------------------------------------------------------------------
12.----------------------------------------------------------------------------
13.----------------------------------------------------------------------------
14.----------------------------------------------------------------------------
15.----------------------------------------------------------------------------
16.----------------------------------------------------------------------------
17.----------------------------------------------------------------------------
18.----------------------------------------------------------------------------
19.----------------------------------------------------------------------------
20.----------------------------------------------------------------------------
21.----------------------------------------------------------------------------
22.----------------------------------------------------------------------------
23.----------------------------------------------------------------------------
Page 1 of 6
Coordination of Outpatient Care
Home care services
Outpatient diabetes classes
Medical Errors JCAHO
ICU Protocols Periop Management Secondary Diagnosis

Insulin Administration Order Written Order Sent to Pharmacy Order Entry by Pharmacist Drug Preparation by pharmacy Insulin delivery to unit Medication Administration Documentation

Inpatient Diabetes Goals
Who Cares
Just get patient home
Sliding Scales are fine
Avoid that scary hypoglycemia
Inpatient Diabetes Goals
Normal glucoses for
everyone
A high glucose means failure
Sliding Scales are banned
Some hypoglycemia is acceptable

Inpatient Diabetes Goals
Who Cares
Just get patient home
Sliding Scales are fine
Avoid that scary hypoglycemia
Inpatient Diabetes Goals
Normal glucoses for
everyone
A high glucose means failure
Sliding Scales are banned
Some hypoglycemia is acceptable

Inpatient Diabetes Goals
Who Cares
Just get patient home
Sliding Scales are fine
Avoid that scary hypoglycemia
Inpatient Diabetes Goals
Normal glucoses for
everyone
A high glucose means failure
Sliding Scales are banned
Some hypoglycemia is acceptable
Inpatient Diabetes Goals
Who Cares
Just get patient home
Sliding Scales are fine
Avoid that scary hypoglycemia
Inpatient Diabetes Goals
Normal glucoses for
everyone
A high glucose means failure
Sliding Scales are banned
Some hypoglycemia is acceptable
Inpatient Diabetes Goals
Appropriate Glucose Control Based on
physiology and outcome studies

Target Glucose Levels
Alive

No DKA or Hyperosmolar Coma
Target Glucose Levels

No hypo- or hyperglycemia
•Prevent fluid and electrolyte abnormalities secondary to osmotic diuresis •Improve WBC function •Improve gastric emptying •Decrease surgical complications •Earlier hospital dischange
•Decreased post-MI mortality
•Decreased post-CABG morbidity and mortality
Target Glucose Levels

Normal Glucoses
Decreased Morbidity and Mortality
Target Glucose Levels

Problems With High Glucoses

Glucose and Post-CABG Morbidity and Mortality
Diabetes and Coronary Artery Bypass Surgery An examination of perioperative glycemic control and outcomes
• Retrospective review of 291 patients surviving 24 h post-op • 40% with retinopathy, nephropathy, or neuropathy
Inpatient complications: For each 1 mmol/l (18 mg/dL) increase in post-op day 1 over 6.1 mmol/l (110 mg/dL), a 17% increased risk of complications
McAlister FA et al. Diabetes Care. 2003; 26:1518-1524.

High Blood Glucose Levels Associated With Increased Mortality in ICU
● Retrospective review of 259,040 critically ill patients conducted by the Veterans Affairs Inpatient Evaluation Center based in Cincinnati
• Hyperglycemia was an independent predictor of mortality starting at 111 mg/dL
• Effect was greatest with acute myocardial infarction, unstable angina, and stroke – Raised MI risk from 1.7 to 6 times – Raised stroke risk from 1.8 to 29 times – Raised unstable angina from 1.4 to 3 times
Falciglia M et al. Crit Care Med. 2009; 37:3001-3009.
• A significant but weaker effect was seen in patients with sepsis, pneumonia, and pulmonary embolism
• Hyperglycemia was not found to be associated with mortality in diseases such as COPD and hepatic failure, hip fractures
• In diabetes patients, the increase in mortality risk was not seen until mean glucose was >146 mg/dL

Hyperglycemia–related mortality in critically ill patients varies with admission diagnosis
Falciglia M et al. Crit Care Med. 2009; 37:3001-3009.

TPN: Adverse Outcomes Hyperglycemia Is Associated With Adverse Outcomes in
Patients Receiving Total Parenteral Nutrition
Cheung et al: Diabetes Care, 28:2367-2371, 2005
Risk of complications in relation to mean daily blood glucose level
OR (95% CI) P
Any infection 1.40 (1.08–1.82) 0.01
Septicemia 1.36 (1.00–1.86) 0.05
Acute renal failure 1.47 (1.00–2.17) 0.05
Cardiac complications 1.61 (1.09–2.37) 0.02
Death 1.77 (1.23–2.52) <0.01
Any complication 1.58 (1.20–2.07) <0.01

Intervention Studies

Decreased Infections Insulin infusion improves neutrophil function in diabetic cardiac surgery patients
Perioperative IV insulin infusion
Neutrophil phagocytic activity
% baseline
Control 47
Insulin 75
Rassias AJ et al. Anesth Analg. 1999; 88:1011-1016.
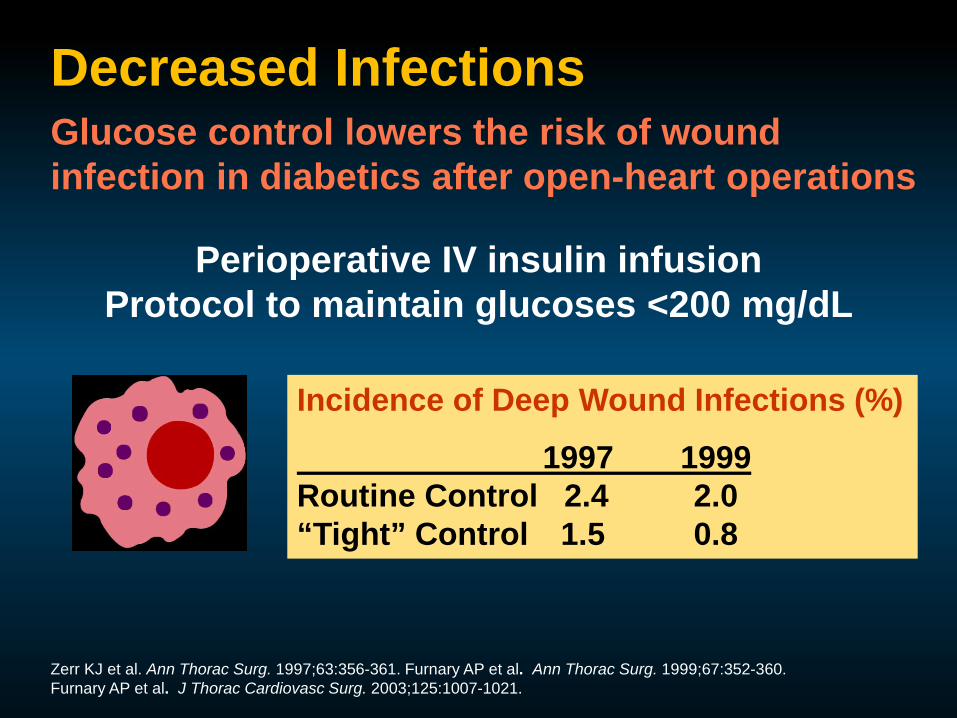
Decreased Infections Glucose control lowers the risk of wound infection in diabetics after open-heart operations
Perioperative IV insulin infusion Protocol to maintain glucoses <200 mg/dL
Incidence of Deep Wound Infections (%)
1997 1999 Routine Control 2.4 2.0 “Tight” Control 1.5 0.8
Zerr KJ et al. Ann Thorac Surg. 1997;63:356-361. Furnary AP et al. Ann Thorac Surg. 1999;67:352-360. Furnary AP et al. J Thorac Cardiovasc Surg. 2003;125:1007-1021.

Decreased Mortality Glucose control decreases mortality in diabetics after open heart
operations Furnary et al. J Thoracic Cardiovascular Surgery 2003, 125: 1007-1021
024
68
1012
1416
<150 150-175 175-200 200-225 225-250 >250
Mor
talit
y (%
)
Cardiac-relatedmortality
Noncardiac-related Mortality
0.9% 1.3%
2.3%
4.1%
6.0%
14.5%

Declining In-Hospital Mortality in Patients Undergoing Coronary Bypass Surgery in the United States Irrespective of Presence of Type 2 Diabetes or Congestive
Heart Failure
Clin Cardiol. 2012 Feb 23. (ahead online)
Steady decline in the coronary artery bypass grafting (CABG)-related total mortality in recent years.

Intensive Insulin Therapy in Critically Ill Patients
Decreased Morbidity and Mortality
● Patients (all) on mechanical ventilation in ICU
● Randomly assigned to IV insulin maintaining glucoses between 80-110 mg/dL or conventional treatment (IV insulin if glucose >215 mg/dL then maintain glucose between 180-200)
Van den Berghe G et al. N Engl J Med. 2001;345:1359-1367.
% given insulin 24-hour dose AM glucose
Intensive 99 71 units 103
Conventional 39 33 units 153
12 month mortality
Intensive 4.6%
Conventional 8.6%
Main effect on patients in ICU >5 days

Van den Berghe, G. et al. N Engl J Med 2006;354:449-461
Kaplan-Meier Curves for In-Hospital Survival

NICE-SUGAR
• 6104 adults who were expected to require treatment in the ICU on 3 or more consecutive days randomized to intensive blood glucose control (target range, 81 to 108 mg/dL) or conventional blood glucose control (<180 mg/dL)
• Primary endpoint death from any cause within 90 days after randomization
• Baseline characteristics similar
The NICE-SUGAR Study Investigators. N Engl J Med. 2009;360:1283-1297.

NICE- SUGAR: Data on Blood Glucose Level, According to Treatment Group
The NICE-SUGAR Study Investigators. N Engl J Med 2009;360:1283-1297

NICE-SUGAR: Probability of Survival and Odds Ratios for Death, According to Treatment Group
The NICE-SUGAR Study Investigators. N Engl J Med 2009;360:1283-1297

Problems With Low Glucoses

Hypoglycemia and Mortality in Insulin-treated vs Non–Insulin-treated
AMI Patients
Kosiborod M, et al. JAMA. 2009;301(15):1556-1564.
Hypoglycemia
No hypoglycemia P=.92 P<.001
Mor
talit
y, %
10.4
18.4
9.2 10.2
0
10
20
No Insulin Treatment Insulin Treatment
Hypoglycemia was a predictor of
higher mortality in patients not treated with insulin, but not
in patients treated with insulin
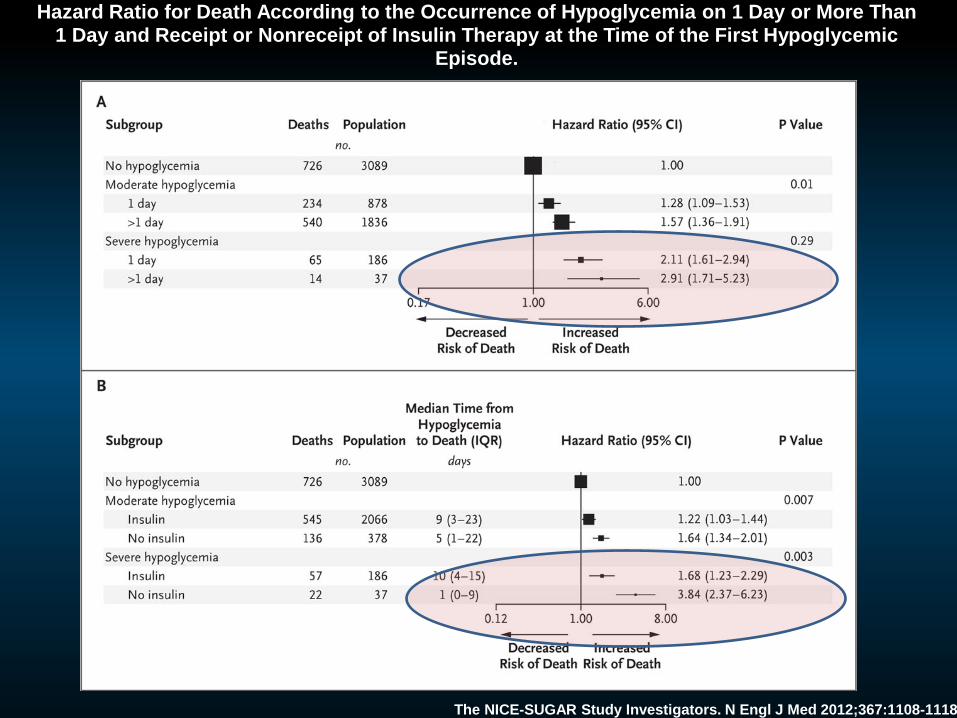
Hazard Ratio for Death According to the Occurrence of Hypoglycemia on 1 Day or More Than 1 Day and Receipt or Nonreceipt of Insulin Therapy at the Time of the First Hypoglycemic
Episode.
The NICE-SUGAR Study Investigators. N Engl J Med 2012;367:1108-1118

Severe Hypoglycemia (glucose<40 mg/dl) 4 month audit
Unit Total Glucose Checks
# Low from report (% low)
False lows # of Actual Low (% low)
ICU (IV) 3378 3 (0.09%) 2/3 1 (0.03%) ICU (SQ) 5241 9 (0.17%) 8/9 1 (0.02%) Med/Surg 15661 18 (0.11%) 17/18 1 (<0.01%)
Unit Total False lows
Immediate repeat not low (and no rx
given)
No low glucose found (and no rx
noted)
ICU (IV) 2 2 0 ICU (SQ) 8 8 0 Med/Surg 17 12 5
False Low explanation
In ICU, both patients with lows did die within 24 hours, but on review, these patients were both end stage and plans were already being discussed for withdrawal of life support prior to the low glucose.

2013 Inpatient Glucose Goals
Organization ICU Non-ICU Prepandial
Non-ICU Maximum
AACE/ACE 140-180 mg/dl <140 mg/dl 180 mg/dl
ADA 140-180 mg/dl <140 mg/dl 180 mg/dl
ACP 140-200 mg/dl Avoid <140 mg/dl
Endocrine Society <140 mg/dl 180 mg/dl
Society of Critical Care Medicine 100-150 mg/dl
UCSF 100-160 mg/dl 100-180 mg/dl

Blood Glucose Levels During Isulin Treatment
Days of Therapy
Bloo
d gl
ucos
e (m
g/dL
)
100
120
140
160
180
200
220
240
Admit 1 2 3 4 5 6 7 8 9 10
SSRI
Lantus + glulisine
Mean Blood Glucose Levels During Insulin Therapy
* p<0.01 ¶ p<0.05
¶ * * *
¶ ¶ ¶
Day 3: P=0.06
Umpierrez GE Et al. Diabetes Care. 2007;30:2181–2186.

How to Obtain “Tight” Control
Bedside glucose monitoring IV insulin drips Diabetic Flow sheets Discourage the use of traditional Sliding Scale
insulin

INSULIN
SLIDING
SCALE

INSULIN
SLIDING
SCALE

Roller Coaster Effect of Insulin Sliding Scale

Mr. And Mrs. XXXXX are admitted for “Giants” fever.
Mr. XXXXX has Type 2 diabetes and takes a total of 75 Units insulin per day (2 shots). Glucoses at home are “poorly controlled.”
Mrs. XXXXX also has Type 2 diabetes but she has good control taking about 25 units of Lispro premeal and 40 Units glargine at night.

Fingerstick qid with regular insulin SQ coverage:
FSBG Action
< 50 1 amp D50 iv and call HO
51-80 give juice and repeat in 0.5-1 hr
81-150 no coverage
151-200 2U regular insulin SQ
201-250 4U regular insulin SQ
251-300 6U regular insulin SQ
301-350 8U regular insulin SQ
351-400 10U regular insulin SQ
>400 12U regular insulin SQ, call HO

Glucocorticoids and Diabetes Peripheral
Tissues (Muscle)
Glucose
Liver
Impaired insulin secretion
Increased glucose production
postreceptor defect
Insulin resistance
Pancreas

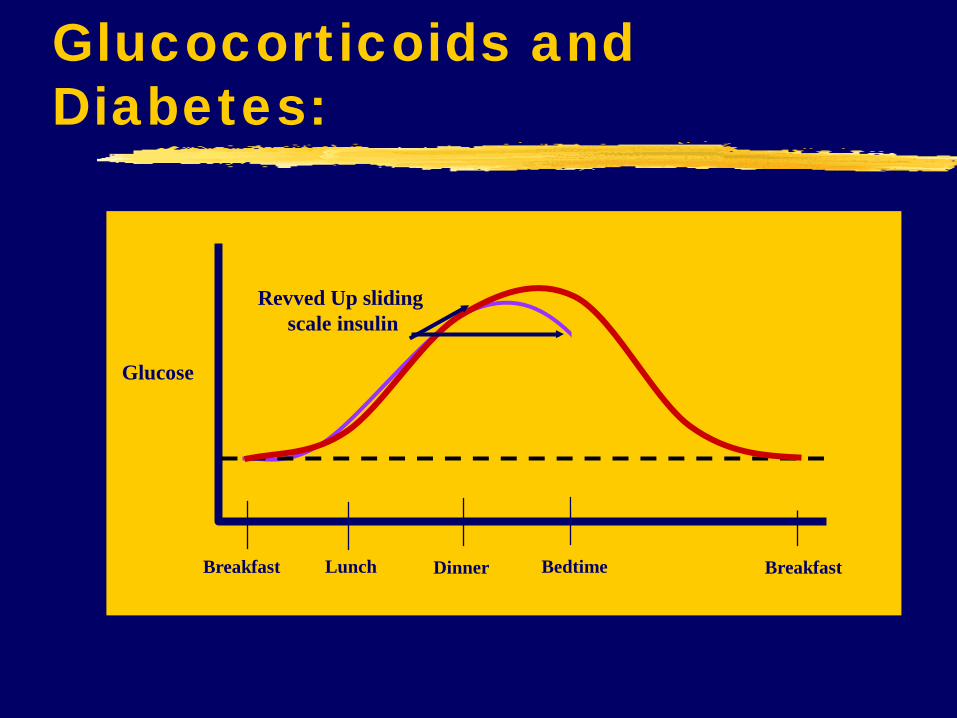
Glucocorticoids and Diabetes:
Breakfast Dinner Lunch Breakfast
Glucose
Bedtime

Glucocorticoids and Diabetes:
Breakfast Dinner Lunch Breakfast
Glucose
Bedtime
Typical sliding scale insulin

Glucocorticoids and Diabetes:
Breakfast Dinner Lunch Breakfast
Glucose
Bedtime
Typical sliding scale insulin
Glucocorticoids and Diabetes:
Breakfast Dinner Lunch Breakfast
Glucose
Bedtime
Revved Up sliding scale insulin

Glucocorticoids and Diabetes:
Breakfast Dinner Lunch Breakfast
Glucose
Bedtime
Revved Up sliding scale insulin
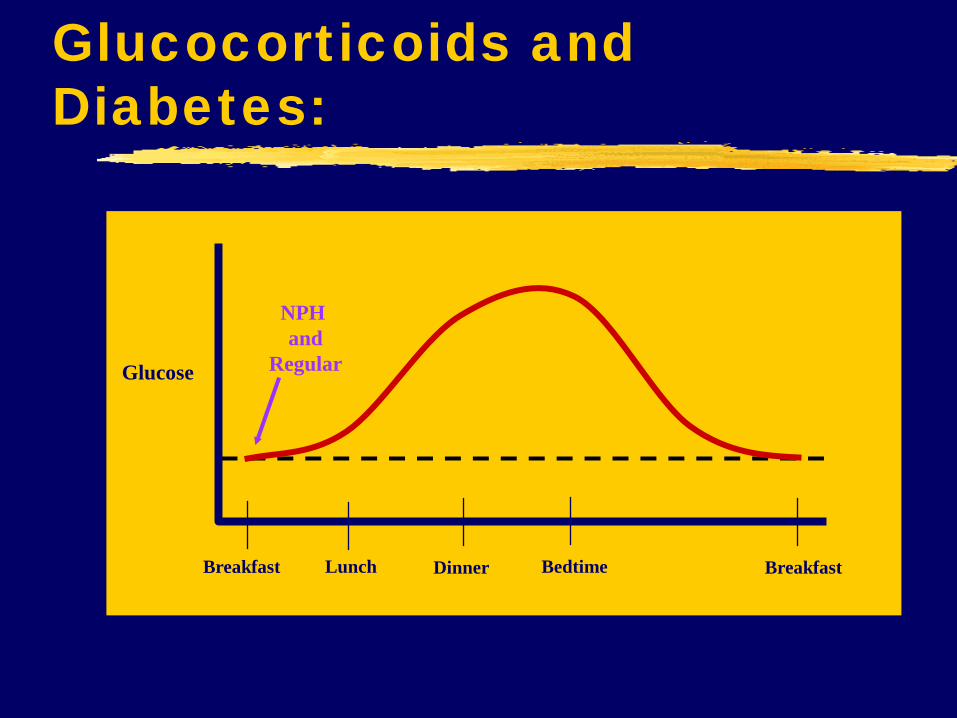
Glucocorticoids and Diabetes:
Breakfast Dinner Lunch Breakfast
Glucose
Bedtime
NPH and
Regular

Glucocorticoids and Diabetes:
Breakfast Dinner Lunch Breakfast
Glucose
Bedtime
NPH and
Regular

Glucocorticoids and Diabetes:
Breakfast Dinner Lunch Breakfast
Glucose
Bedtime
Increase NPH and
Regular

INSULIN
SLIDING
SCALE

Use of Insulin

Physiologic Insulin Secretion: Basal/Bolus Concept
Breakfast Lunch Supper
Insu
lin
(µU
nits
/mL)
G
luco
se
(mg/
dL)
Basal Glucose
150
100
50
0 7 8 9 10 11 12 1 2 3 4 5 6 7 8 9
A.M. P.M. Time of Day
Basal Insulin
50
25
0
Nutritional Glucose
Nutritional (Prandial) Insulin
Suppresses glucose production between meals & overnight
The 50/50 Rule

Relative Insulin Level
Time
Breakfast 12pm Lunch Dinner
Insulin Regimens

Relative Insulin Level
PM glargine
glargine
Insulin Regimens
Time
Breakfast 12pm Lunch Dinner

Relative Insulin Level
Time
Breakfast
TID lispro/aspart/glulisine and hs glargine
Lunch Dinner 12pm
glargine
Lispro/aspart/glulisine
Insulin Regimens

Past Paper Insulin Order Forms
● Adult – DKA – Adult SQ Insulin – Patient
eating – Adult SQ Insulin – NPO,
TPN, Tube Feeding – IV insulin – ICU protocol – IV insulin – Med-Surgical
Unit protocol – Adult Insulin pump
• Patient waver form – Adult SQ insulin algorithm
for NPO patients** – CV Surgery Specific orders
– PREO-OP Pathway**
● OB-GYN – SQ Insulin – Patient eating – IV Insulin form - delivery – Pump Form
• Pump waiver form
● Pediatrics – SQ Insulin – Patient eating – Pump Form
• Pump waiver – DKA – IV insulin
** under development

Order set
Adult SQ Insulin – Patient eating: set premeal dose
Premeal Dosing
Postmeal Dosing (based on amount consumed)
Adult SQ Insulin – Patient eating: CHO Counting
Premeal Dosing CHO dependent
Postmeal Dosing (based on CHO consumed)
Adult SQ Insulin – NPO, TPN
Q4h nutrition and correction
Nutrition dose timed to cycle TPN, correction q4h
Adult SQ Insulin –Tube Feeding
Q4h nutrition and correction
Nutrition dose timed to cycle feedings, correction q4h
Adult Insulin Pump
IV Insulin protocol: ICU Specific initial rate for CVS/DKA/other
IV insulin protocol: Medical/surgical units Specific initial rate for CVS/DKA/other
DKA



Big Brother
Daily Reports: 2 or more glucoses>225 Glucose <60 On insulin pump Dx type 1 DM

Pharmacologic Classes of Agents to Control Hyperglycemia in Type 2 Diabetes
Thiazolidinediones—e.g., rosiglitazone, pioglitazone
Class
Biguanides—e.g., metformin
Alpha-glucosidase inhibitors—e.g., acarbose & miglitol
Insulin secretagogues—e.g., sulfonylureas (glyburide, glipizide); repaglinide
Takes 2-3 weeks to see initial effect. Effects continue for weeks or months after discontinuation of medication
Keep in mind the metabolic t1/2 of each drug. High risk for hypoglycemia
Withhold in conditions predisposing to renal insufficiency and/or hypoxia
CV collapse Acute MI or acute CHF Severe infection Use of iodinated contrast material Major surgical procedures
In case of hypoglycemia (due to sulfonylurea or insulin treatment)
Glucose (dextrose) must be administered
Sucrose and complex carbohydrates should not be administered
Special Considerations

Pharmacologic Classes of Agents to Control Hyperglycemia in Type 2 Diabetes
DDP 4 Inhibitor Class
SGLT-2 inhibitor
Other: Colesevelam Dopamine Agonist
GLP-1 Agonist
Minimal Data. Low risk of hypoglycemia
Minimal Data. GI side effects, delayed gastric emptying. Low risk of hypoglycemia
No Data. Risk of dehydration, urinary and yeast infections
No Data. GI side effects Colesvelam: binds medications
Special Considerations

What does it take to Implement Change?
Physicians Administration


Committee Members Physicians: Endocrinologist, Hospitalist Clinical Nurse Specialists: Diabetes, education Nurses: ICU Manager, at least one manager from
medical floor (or their representative) Clinical Pharmacist Administration presence – from level of quality
assurance or similar title Discharge Coordinator – not required for initial
discussions and implementation, but needed later Nutritional services – not required for initial design
and implementation of forms.

TASKS Formulary
Clean up insulin Clean up oral agents
Nursing Issues Policy on IV insulin use Policy on frequency of glucose monitoring
Forms Design forms
IV insulin forms SQ insulin forms ?DKA treatment forms

Other Committees To be Conquered Pharmacy and Therapeutics
Formulary issues Oral agents Insulins Insulin Forms – iv, sq
Forms Insulin forms – iv, sq
Quality Improvement Need buy in at this level to achieve administrative
support

Other People To be Conquered Smaller Hospitals
CEO Chief of Staff
Larger Institutions Chairs of Medicine, Surgery Heads of training programs from Medicine,
Surgery Chief of Staff, Chief Medical Officer, CEO Chairs of other Departments Chief Residents Dean for Education

Implementation Smaller Hospitals
Entire Institution Larger Institutions
? One unit at a time ? One service at a time
Make certain forms are available Unit clerks must be aware!!!! If orders written in ER, forms must be in ER If forms not available, this will fail.

UCSF Implementation Committee: Endocrinologists, Hospitalist,
Diabetes Nurse Specialist, Clinical Pharmacists, QA administrators, others
Formulary Limited number of insulins now available
Forms IV insulin forms – ICU, Floor SQ insulin form DKA treatment forms

Physicians Robert Rushakoff Umesh Masharani Melissa Weinberg Sarah Kim Aaron Neinstein Bonnie Kimmel Saleh Adi Stephen Gitelman Jan Hirsch Kathryn Rouine-Rapp David Robinowitz Michael Hwa Heather Nye Steve Pantilat
Pharmacists Heidemarie Windham Lisa Kroon Kethen So Thomas Bookwalter Anna Seto
Administration Rosanne Rappazini Jennifer Pacholuk Joy Pao
Dietary Marian Devereaux
Nurses Mary Sullivan Pauline Chin Marlene Bedrich Craig Johnson Molly Killion Jeanne Buchanan Noraliza Salazar Lynn Dow
PEOPLE CHANGING INPATIENT DM MANAGEMENT AT UCSF

UCSF Implementation Nursing Education
Diabetes Nurse Specialist Intranet Training

UCSF Implementation Nursing Education
Diabetes Nurse Specialist Intranet Training
Physician Training Small group sessions Internet training



Pediatric Nursing Training
Pre-implementation
N=24
Post-implementation
N=22
Test of significance
Total errors 127 17
Total possible errors
882 1107
Mean # errors/pt 5.29 0.77 2-tailed t, independent samples with
unequal variance p.=.004
Error rate Denominator = possible errors
0.14 0.02 Z-test, 2-tail p=0.02

Community Hospital Physician Training
Annenberg Project

Robert J. Rushakoff, MD Director Inpatient Diabetes, UCSF
Cheryl W. O’Malley, MD Program Director, Internal Medicine Banner Good Samaritan Medical, Phoenix, Arizona
Kendall M. Rogers, MD Chief, Hospital Medicine University of New Mexico Health
Sciences Center Albuquerque, New Mexico
Archana Sadhu, MD Director, Inpatient Diabetes Program, The Methodist
Hospital System Houston, Texas

Carol Manchester, MSN, ACNS, BC-ADM, CDE University of Minnesota Medical Center, Minneapolis, Minnesota
Jane Jeffrie Seley, DNP, MPH, BC-ADM, CDE New York Presbyterian/Weill Cornell Medical Center
Mary M. Sullivan, RN, DNP, ANP-BC, CDE University of California, San Francisco
Eric D. Peterson, EdM, FACME Annenberg Center for Health Sciences at Eisenhower


Faculty team visits each site 1 physician (inpatient endocrinologist or hospitalist)
1 nurse with inpatient glycemic control experience
Team Meeting Review experience, goals, barriers
Refine the team project who they need to involve Data collection to characterize their current performance Common barriers that they are likely to face and strategies that have been used by other
institutions to overcome them Implementation and measurement that they may want to consider to evaluate both process and
outcome
Presentation to other stakeholder groups Physician or nursing staff forums

3 Web conferences planned #1 Sites share their project plans
#2 Sites present interim progress and challenges
#3 Sites present data generated from their project
Primarily intended as a tactic to keep sites “on task” and to facilitate interaction between sites

Community, non-teaching; No Endocrinology
Lots of forms – main was self adjusting SS
Many MD groups, hospitalist group
No education, Meal timing

Lots of forms – main was self adjusting SS SS form gone; BB mainly used (CHO based postmeal for
meals on demand) Many MD groups, hospitalist group Hospitalist contract dispute
No education Case studies – CDs, in person for specific populations
Meals Refreshment centers closed Still get meals on demand
CDE Involvement Assist with insulin orders Call MDs for consistently high numbers

Hyperglycemia in Hospitalized Patients
ucsf.logicnets.com
Transition from Home to Hospital
Issues at Discharge ● Patient new to diabetes ● Patient new to insulin or other medications ● Not metabolically stable (eg, steroid taper), unclear
what any requirement will be ● Oral agents, incretins - when, how, why ● Changing medications (TPN, etc.) on the day of
discharge ● Inability to perform self management ● Who follows patient ● Communication of inpatient care plan to outpatient
providers ● Short-term and long-term goals

UCSF Survey of Patients on Insulin Discharged to Home
