inpatient glycemic management - st. charles health system/media/grandroundsmedia/2017/... ·...
TRANSCRIPT

Inpatient Glycemic ManagementBethany Klopfenstein MD
Director, Inpatient Glycemic ControlAssociate Professor, Division of Endocrinology,
Diabetes, and Clinical NutritionOregon Health & Science University

Disclosures
• None

Objectives – to discuss:
• Impact of hyperglycemia in the hospital
• Glycemic targets for hospitalized patients
• Strategies for management of hyperglycemia in the hospital

2014 National Diabetes Statistics Report• 29.1 million individuals in the US have diabetes (9.3% of the
population)– Diagnosed: 21.0 million – Undiagnosed: 8.1 million (28% of people with diabetes are
undiagnosed)• 86 million have prediabetes
– 35% of adults ≥ 20 yrs and 50% of adults >65 yrs
• High prevalence of hyperglycemia in the hospitalized patient– > 60% of ICU patients experience BG >180– > 46% of non-ICU patients experience BG >180– ~ 30% of inpatients have a (patient-day weighted) mean BG
>180 mg/dL
National Diabetes Statistics Report. 2014. http://www.cdc.gov/DIABETES/pubs/estimates14.htm#6Cook et al. A Glycemic Survey of 126 US Hospitals. Journal of Hospital Medicine 2009; 4:E7-E17.

Economic Burden of Diabetes
• In 2012, estimated diabetes related-costs totaled $245 billion
–Direct medical costs totaled $176 billion (52% increase from 2007)
–Hospital inpatient care accounts for 43% of total medical cost
– Higher rates of admission and readmission– Longer LOS per admission
American Diabetes Association. Diabetes Care. 2008;31(3):596-615, andDiabetes Care. 2012 http://care.diabetesjournals.org/content/early/2013/03/05/dc12-2625.full.pdf+html

Hyperglycemia in the Hospital
• Diabetes:– Previously diagnosed– Previously undiagnosed
• HbA1c ≥ 6.5% during admission
• Hyperglycemia without diabetes diagnosis– Diabetes diagnosed on follow-up– Prediabetes with overt hyperglycemia during
acute physiologic stress– Hyperglycemia due to physiologic stress without
underlying metabolic abnormality • normal follow-up testing

Identifying Hyperglycemia in the Hospital
Inhospital hyperglycemia is defined as an admission or inhospital BG > 140 mg/dl.
HbA1c testing can be useful to: assess glycemic control prior to admission assist with differentiation of newly diagnosed diabetes
from stress hyperglycemia designing an optimal regimen at the time of discharge
HbA1c > 6.5% can be identified as having diabetes, and HbA1C 5.7%-6.4% is consistent with prediabetes.

Impact of Hyperglycemia in Hospitalized Patients

Relationship of Postoperative Hyperglycemia and Risk of Postoperative Infection
Ramos, M., et al., Relationship of perioperative hyperglycemia and postoperative infections in patients who undergo general and vascular surgery. Ann Surg, 2008. 248(4): p. 585-91.
Every 40 mg/dL increase in post-op glucose is associated with a 30% increased risk of post-op infection

In-Hospital Complication Rates are Increased in Patients with Diabetes
02468
101214
%
Non-diabetesDiabetes
Frisch et al. Diabetes Care. 2010;133(8): 1783-1788.
†p=0.1; *p<0.001; ‡p<0.017
† ‡
*
** *
*

Hyperglycemia Increases the Risk of Adverse Events in Surgical Patients with and without Diabetes
0
2
4
6
8
10
12
14
Compositeinfections
Allreoperative
interventions
In-hospitaldeaths
Prop
ortio
n of
pat
ient
s (%
) Glucose ≤ 180 (n=1729)
Glucose > 180(n=2369)
0
2
4
6
8
10
12
14
Compositeinfections
Allreoperative
interventions
In-hospitaldeaths
Prop
ortio
n of
pat
ient
s (%
) Glucose ≤ 180 (n=6512)
Glucose > 180(n=1013)
Kwon, Steve; MD, MPH et al. Importance of Perioperative Glycemic Control in General Surgery: A Report From the Surgical Care and Outcomes Assessment Program. Annals of Surgery. 257(1):8‐14, January 2013.
AEs among patients with diabetes AEs among patients without diabetes
*
*
*
*
*P<0.01
†
†P<0.05
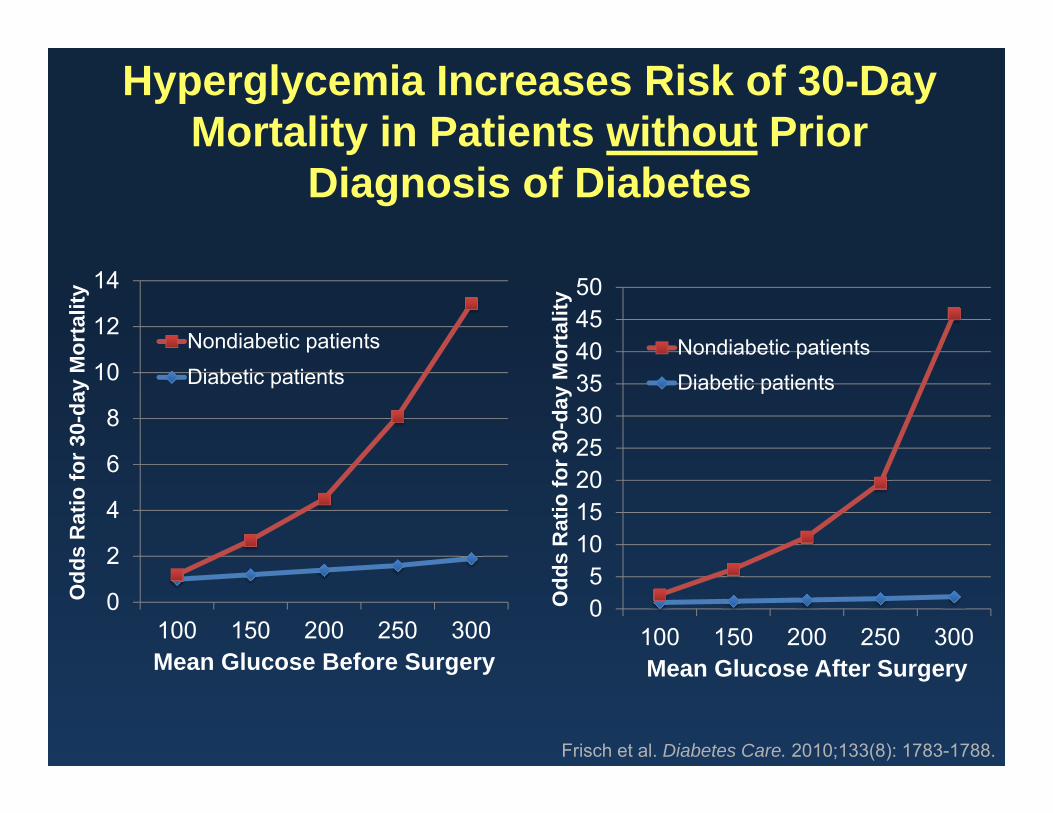
0
2
4
6
8
10
12
14
100 150 200 250 300
Odd
s R
atio
for 3
0-da
y M
orta
lity
Mean Glucose Before Surgery
Nondiabetic patients
Diabetic patients
Hyperglycemia Increases Risk of 30-Day Mortality in Patients without Prior
Diagnosis of Diabetes
05
101520253035404550
100 150 200 250 300
Odd
s R
atio
for 3
0-da
y M
orta
lity
Mean Glucose After Surgery
Nondiabetic patientsDiabetic patients
Frisch et al. Diabetes Care. 2010;133(8): 1783-1788.

Detrimental Physiologic Impact of Hyperglycemia
Deedwania P, et al. Circulation. 2008;117(12):1610-1619. Modified from Clement S, et al. Diabetes Care. 2004;27(2):553-591.
Metabolic stress response Stress hormones and peptides
Prolonged hospital stay Disability Death
Glucose Insulin
FFA Ketones Lactate
Immune dysfunction
Infection
Reactive O2 species
Transcription factors
InflammationImpaired healing
AcidosisElectrolyte fluxesVolume depletionTissue damage
Infarction/ischemia
Platelet aggregation
Thrombosis

Glycemic Targets for Hospitalized Patients
Strategies for Management of Inpatient Hyperglycemia
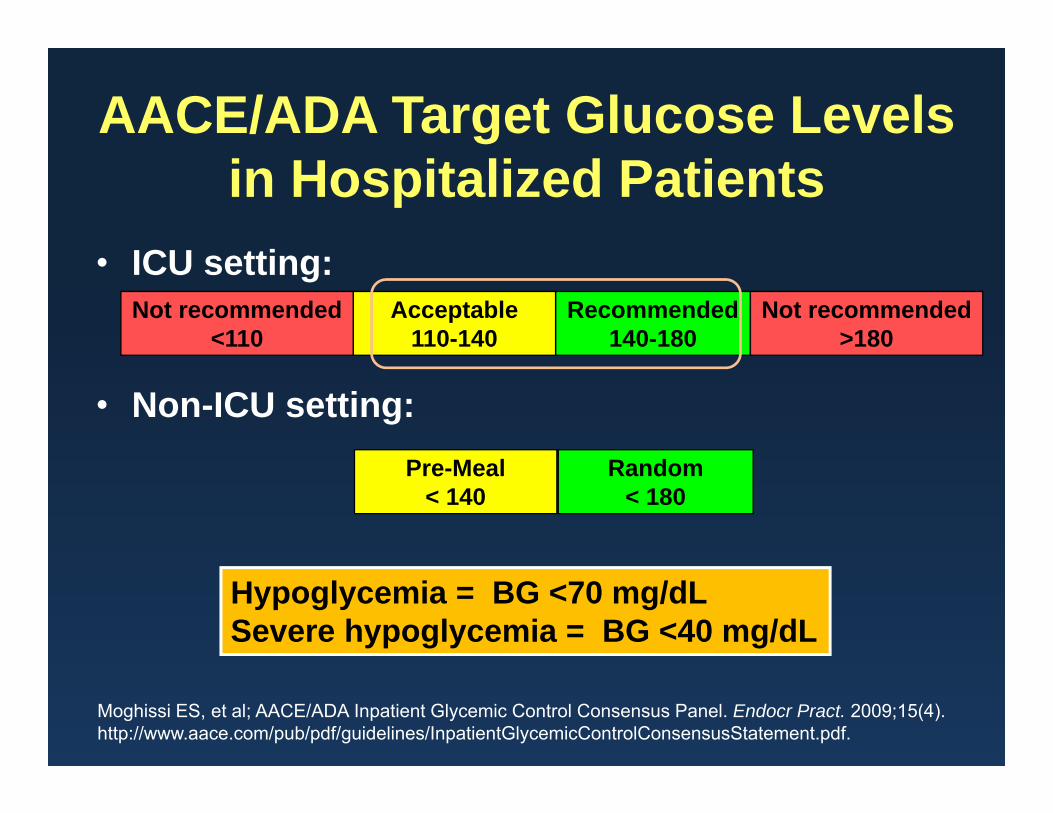
Moghissi ES, et al; AACE/ADA Inpatient Glycemic Control Consensus Panel. Endocr Pract. 2009;15(4). http://www.aace.com/pub/pdf/guidelines/InpatientGlycemicControlConsensusStatement.pdf.
AACE/ADA Target Glucose Levels in Hospitalized Patients
• ICU setting:
• Non-ICU setting:
Recommended140-180
Acceptable110-140
Not recommended<110
Not recommended>180
Hypoglycemia = BG <70 mg/dLSevere hypoglycemia = BG <40 mg/dL
Random< 180
Pre-Meal< 140

Antihyperglycemic Therapy
InsulinNon-Insulin
Antihyperglycemic Drugs
Recommendations for Managing Hyperglycemia in the Inpatient Setting
Moghissi ES, et al; AACE/ADA Inpatient Glycemic Control Consensus Panel. Endocr Pract. 2009;15(4). http://www.aace.com/pub/pdf/guidelines/InpatientGlycemicControlConsensusStatement.pdf.
AACE/ADA Consensus Statement
Non-insulin therapies in the hospital?
Sulfonylureas can cause hypoglycemiaMetformin contraindicated in setting of decreased renal
blood flow and with use of iodinated contrast dyeThiazolidinediones associated with edema and CHFα glucosidase inhibitors are weak glucose lowering agentsDPP-4 inhibitors not effective in the inpatient setting for
patients with CBG >180SGLT-2 inhibitors have potential risk of UTI and can
contribute to mild volume depletionPramlintide and GLP1-agonists can cause nausea and
have a greater effect on postprandial glucose
Moghissi ES, et al. AACE/ADA Inpatient Glycemic Control Consensus Panel. Endocr Pract. 2009

Antihyperglycemic Therapy
InsulinRecommended
Non-Insulin DrugsNot Generally
Recommended
Recommendations for Managing Inpatient Hyperglycemia
Clement S, et al. Diabetes Care. 2004;27(2):553-591.Moghissi ES, et al; AACE/ADA Inpatient Glycemic Control Consensus Panel. Endocr Pract. 2009;15(4). http://www.aace.com/pub/pdf/guidelines/InpatientGlycemicControlConsensusStatement.pdf.
What is the best approach?

Antihyperglycemic Therapy
InsulinRecommended
Non-Insulin DrugsNot Generally
Recommended
IV InsulinCritically ill patients
Perioperative
SC InsulinNon–critically ill
patients
Recommendations for Managing Inpatient Hyperglycemia
Clement S, et al. Diabetes Care. 2004;27(2):553-591.Moghissi ES, et al; AACE/ADA Inpatient Glycemic Control Consensus Panel. Endocr Pract. 2009;15(4). http://www.aace.com/pub/pdf/guidelines/InpatientGlycemicControlConsensusStatement.pdf.

Management of Hyperglycemia using Insulin Infusion

Intravenous Insulin
• Many different protocols published• Therapy of choice in the ICU• Best results in patients who are NPO• For best results in patients that are eating:
– Use IV insulin as basal insulin– Add SC mealtime insulin

B L D
IV Insulin
Overlap of IV / SCGlargine: 3 hoursNPH: 90 minutes
Rapid-acting Insulin based on
intake
Basal glargine
Basics of SC Insulin After IV

Management of Hyperglycemia using Subcutaneous Insulin

Sliding-Scale Insulin Alone Not Recommended
Adapted from :DeWitt DE, Dugdale DC. JAMA. 2003;289(17):2265-2269.Skyler JS. In: DeFronzo RA, ed. Current Therapy of Diabetes Mellitus. St Louis, MO: Mosby-Year Book, Inc;1998:36-49.
Concerns:Reactive approach:↑ Hyperglycemia
Insu
lin E
ffect
Time, h
BG = 220
0 2 4 6 8 10 12 14 16 18 20 22 24
BG = 280 BG = 247BG = 200
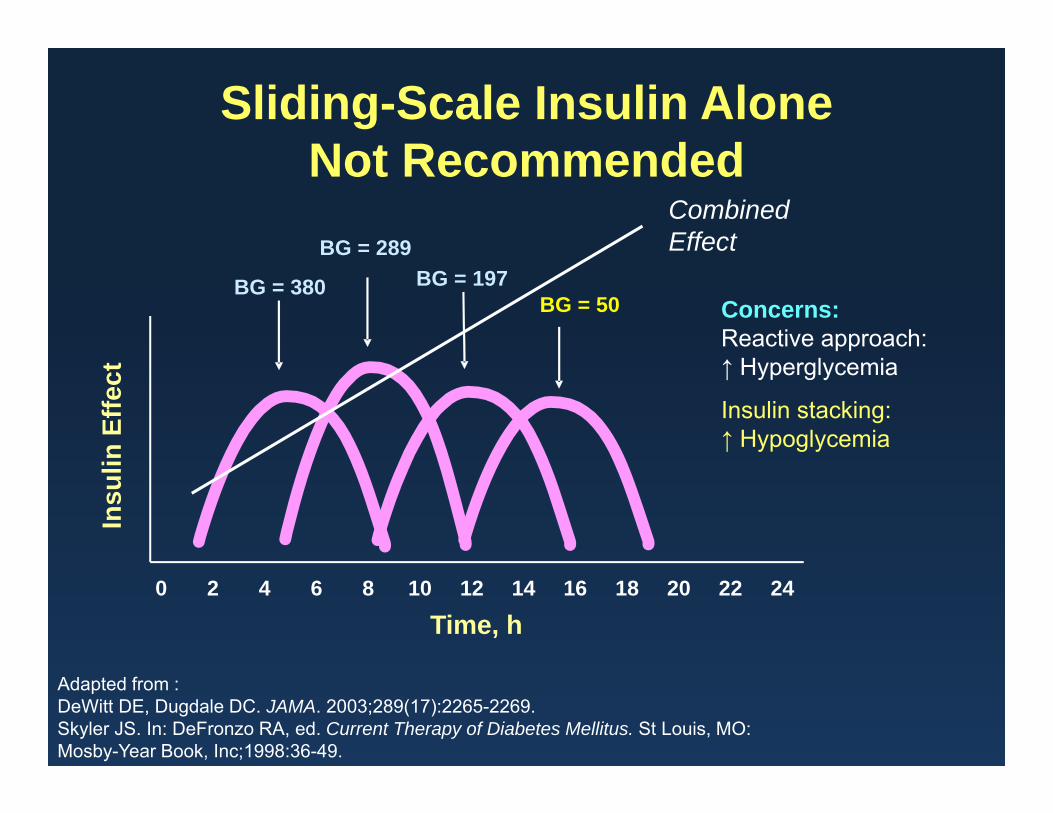
Sliding-Scale Insulin AloneNot Recommended
Adapted from :DeWitt DE, Dugdale DC. JAMA. 2003;289(17):2265-2269.Skyler JS. In: DeFronzo RA, ed. Current Therapy of Diabetes Mellitus. St Louis, MO: Mosby-Year Book, Inc;1998:36-49.
Concerns:Reactive approach:↑ Hyperglycemia
Insulin stacking:↑ Hypoglycemia
Insu
lin E
ffect
Time, h
BG = 380BG = 50
BG = 197BG = 289
0 2 4 6 8 10 12 14 16 18 20 22 24
Combined Effect
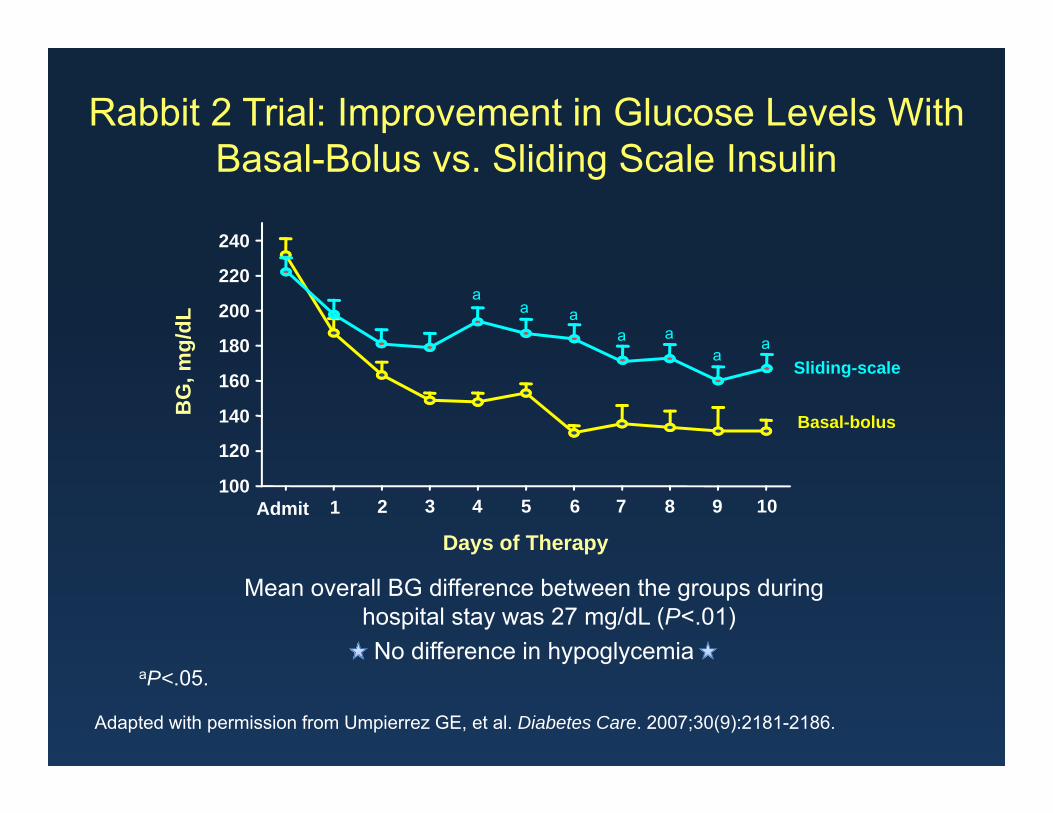
Rabbit 2 Trial: Improvement in Glucose Levels With Basal-Bolus vs. Sliding Scale Insulin
Mean overall BG difference between the groups during hospital stay was 27 mg/dL (P<.01) No difference in hypoglycemia
Adapted with permission from Umpierrez GE, et al. Diabetes Care. 2007;30(9):2181-2186.
Days of Therapy
BG
, mg/
dL
100
120
140
160
180
200
220
240
Admit 1
Sliding-scale
Basal-bolus
aP<.05.
aa a
a aa
a
2 3 4 5 6 7 8 9 10

0%
5%
10%
15%
20%
25%
30%
Sliding Scale Basal‐Bolus
Rabbit 2 Surgery Trial: Improved Outcomes with Basal-Bolus Insulin in Non-ICU Surgical Patients
% o
f Pat
ient
s w
ith C
ompl
icat
ions
Complications include:•Wound infection•Pneumonia•Acute respiratory failure•Acute renal failure•Bacteremia
n = 107
p = 0.003
Umpierrez et al. Diabetes 59:Suppl 1 Abstract 0033, 2010
n = 104
Mean BG POD1: 172 ± 47 (Sliding scale) vs. 145 ± 32 mg/dl (Basal-Bolus)

5 Step Approach to Inpatient Insulin Management

STEP 1: Estimate the Total Daily Insulin Requirement: Basal + Nutritional Insulin
= Total Daily Dose (TDD)• Weight-based estimate:
– TDD = 0.4-0.5 units/kg (for type 2 diabetes)– Adjust TDD down to 0.2-0.3 units/kg for those with hypoglycemia risk factors
• Elderly, renal failure, liver disease, low body weight, type 1 or no history of diabetes
– Adjust TDD up to 0.5-0.6 units (or more)/kg for those with hyperglycemia risk factors
• Obesity, glucocorticoids
• Insulin drip-based estimate (for patients treated with an insulin infusion)
• For patients on insulin prior to admission, consider the patient’s preadmission subcutaneous regimen TDD and glycemic control on that regimen

STEP 2: Assess the Patient’s Nutritional Situation
• Eating meals predictably• Eating meals but with unpredictable intake• Enteral feeding
– Continuous– Part of the day– Bolus
• TPN• Combinations of above• NPO
STEP 3: Divide the Total Daily Dose (TDD) into Basal and Nutritional Components
• Basal insulin can generally be estimated to be 50% of the TDD– Decrease to 40% if receiving AM corticosteroids
• Nutritional insulin can be estimated to be the remaining 50% of the TDD– Increase to 60% if receiving AM corticosteroids– If eating, divide boluses between meals
STEP 4: Decide Which Components of Insulin the Patient Will Require
• In the majority of cases, basal insulin should be provided
• When a patient is not receiving nutrition, nutritional insulin should not be given, however basal insulin should be continued
• Nutritional insulin needs must be matched to the actual nutritional intake (eating, tube feeds, TPN, etc.)• Patients with unpredictable PO intake: Bolus insulin can be given
immediately after the meal, in a ratio determined by amount eaten
• Generally, well-designed correction insulin regimens should also be provided in addition to scheduled bolus insulin

STEP 5: Assess Blood Glucose Pattern Daily (at a minimum) and Adjust Insulin Doses
• Adjust basal and bolus doses based on glucose patterns• If glucoses consistently >180-200, increase TDD by 20%• If any glucose < 70, decrease TDD by 20%
• Improvement of hyperglycemia and avoidance of hypoglycemia can only be achieved via continuous management of the insulin regimen
• There is no “autopilot” insulin regimen for a hospitalized patient

Inpatient Insulin Management:Tailor to the situation
• Patients that are eating (reliably or unreliably)
• Other nutrition (Tube feeds, TPN)• Corticosteroids • Procedures/surgery

Inpatient Insulin Management:Tailor to the situation
• Patients that are eating (reliably or unreliably)

Basal-Bolus Insulin Treatment With Glargine and Rapid-acting Analogs
Time4:00 8:00 12:00 16:00 20:00 24:00 4:00 8:00
Breakfast Lunch DinnerGlucoseGlargine, DetemirAspart/Lispro/ Glulisine
Glargine
Rapid acting insulin
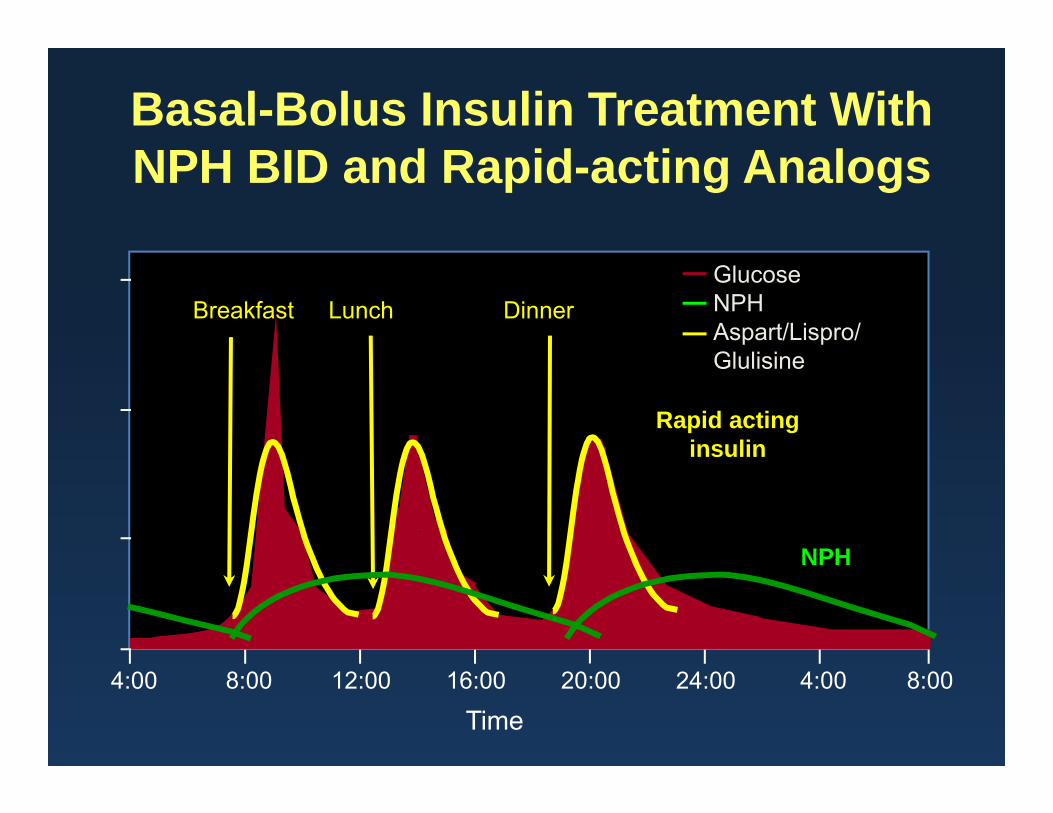
Basal-Bolus Insulin Treatment With NPH BID and Rapid-acting Analogs
Time4:00 8:00 12:00 16:00 20:00 24:00 4:00 8:00
Breakfast Lunch DinnerGlucoseNPHAspart/Lispro/ Glulisine
NPH
Rapid acting insulin

NPH + Regular/Rapid Acting Analog or 70/30, 2 injections per day: Not recommended for
Inpatient management
Time4:00 8:00 12:00 16:00 20:00 24:00 4:00 8:00
Breakfast Lunch DinnerGlucoseNPHAspart/Lispro/ Glulisine/Regular
NPH
Short acting insulin

Inpatient Insulin Management:Tailor to the situation
• Patients that are eating (reliably or unreliably)
• Other nutrition (Tube feeds, TPN)

Insulin Requirement During Continuous Enteral Nutrition
04:00 08:00 12:00 16:00 20:00 00:00 04:00

NPH q8 hours During Continuous Enteral Nutrition or TPN
04:00 08:00 12:00 16:00 20:00 00:00 04:00

NPH q 8 hours During Continuous Enteral Feedings (or TPN)
BG q 2 hr, dextrose if < 100 Enteral Feeding stopped, hold next NPH dose
TF restarted
04:00 08:00 12:00 16:00 20:00 00:00 04:00

Glargine During Continuous Enteral Feedings or TPN
glargine
04:00 08:00 12:00 16:00 20:00 00:00 04:00

Glargine During Continuous Enteral Feedings (or TPN)
glargine
10% dextrose at same rate IV, BG q2hrTF stopped
TF restarted, stop 10% dextrose
04:00 08:00 12:00 16:00 20:00 00:00 04:00

04:00 08:00 12:00 16:00 20:00 00:00 04:00
Overnight Enteral Feedings with Daytime Grazing

04:00 08:00 12:00 16:00 20:00 00:00 04:00
Bolus Enteral Feedings
GlucoseRapid acting analogGlargine

TPN
• Parenteral nutrition often causes hyperglycemia and often requires insulin treatment, even in patients who would not require insulin otherwise
• Consider IV insulin for first 1-2 days to gauge the insulin requirements
• Then place about 80% of the insulin requirement in the TPN and use a supplemental insulin scale
• Redistribution strategy – add 2/3’s of yesterdays correction therapy to today’s bag

Inpatient Insulin Management:Tailor to the situation
• Patients that are eating (reliably or unreliably)
• Other nutrition (Tube feeds, TPN)• Corticosteroids

Typical Blood Glucose Pattern With Morning Steroid Therapy
Breakfast Lunch Dinner
Glucose Level

Inpatient Therapy of Patients on AM Corticosteroids
Breakfast Lunch Dinner
Glucose Level
Basal insulin
Prandial insulin
20-25%
20%
25%
15%
15-20%
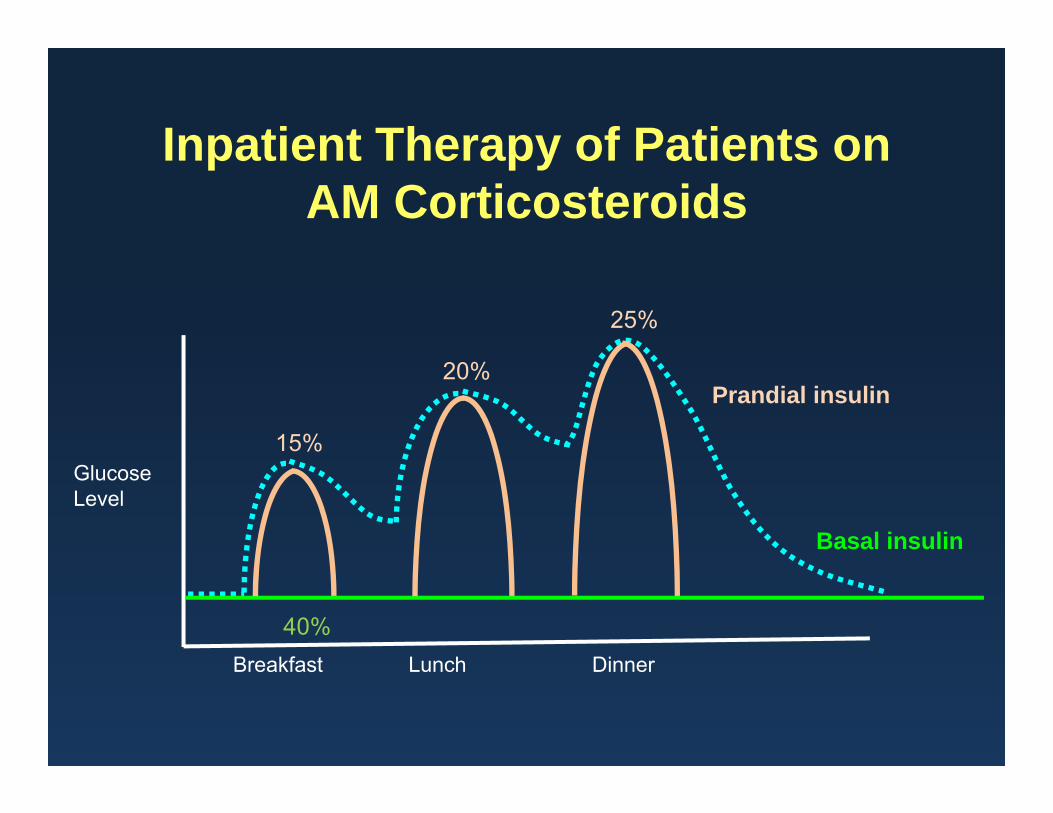
Inpatient Therapy of Patients on AM Corticosteroids
Breakfast Lunch Dinner
Glucose Level
Basal insulin
Prandial insulin
40%
20%
25%
15%

Inpatient Insulin Management:Tailor to the situation
• Patients that are eating (reliably or unreliably)
• Other nutrition (Tube feeds, TPN)• Corticosteroids • Procedures/surgery: NPO

Management while NPO
8 12 6 10
lispro
glargine
• Insulin Infusion• Patients on established basal/bolus regimens
• Basal dose does not need to be reduced• Hold the bolus doses when NPO

Transition to Outpatient Care

Can Patients Go Back to Oral Agents at Discharge?
• If preadmission control acceptable, yes!
• Admission HbA1C helpful
• Hospital discharge is an opportunity to adjust therapy
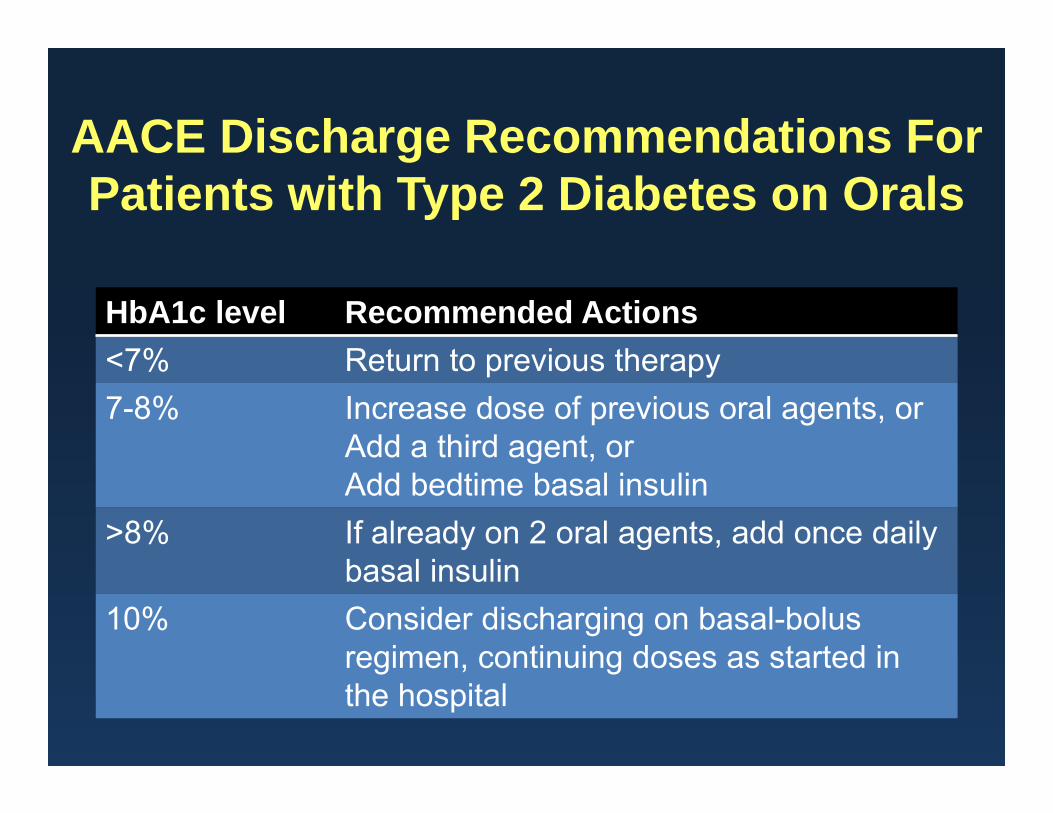
AACE Discharge Recommendations For Patients with Type 2 Diabetes on Orals
HbA1c level Recommended Actions<7% Return to previous therapy7-8% Increase dose of previous oral agents, or
Add a third agent, orAdd bedtime basal insulin
>8% If already on 2 oral agents, add once daily basal insulin
10% Consider discharging on basal-bolus regimen, continuing doses as started in the hospital

Improved HbA1c with Discharge Regimen Based on Admission HbA1c in Patients with Type 2 Diabetes
Umpierrez et al. Diabetes Care. 2014 Nov;37(11):2934-9.

58
Hospital Discharge Transition of Inpatients with Hyperglycemia
• Stabilize blood glucose prior to discharge
• Provide inpatient education (survival skills)
• Refer patient for outpatient education
• Prepare for outpatient follow-up with PCP
Magee MF. Hosp Physician. 2006;2(4):17-28.Clement S, et al. Diabetes Care. 2004;27(2):553-591.Inzucchi SE. N Engl J Med. 2006;355(18):1903-1911.Hassan E. Am J Health Syst Pharm. 2007;64(10 suppl 6):S9-S14.

Post-discharge Outcomes for Hyperglycemic Patients With No
Prior History of Diabetes
• 60% of patients with no prior history of diabetes who are found to have hyperglycemia (random BG >125 mg/dL) during hospitalization are likely to have diabetes on follow-up testing1
• ADA recommends follow-up testing for diabetes in such patients within 1 month of hospital discharge2
1. Greci LS, et al. Diabetes Care. 2003;26(4):1064-1068.2. Clement S, et al. Diabetes Care. 2004;27(2):553-591.

Summary• Inpatient hyperglycemia is associated with increased
morbidity and mortality in patients with and without diabetes
• Hyperglycemia in the hospital is best managed via physiologic insulin therapy (basal/nutritional), with additional supplemental insulin used if needed
• Choice of regimen needs to be individualized and account for source of nutrition, changing medical status, and factors increasing risk of hypoglycemia and hyperglycemia
• Insulin regimen should be adjusted daily depending on prior day’s results
