inpatient glycemic management: time to shed our scales? deric morrison oct. 2014
TRANSCRIPT

Inpatient Glycemic Management:
Time to shed our scales?Deric Morrison
Oct. 2014
Objectives• At the end of this presentation
you will:1. Understand the current guidelines for inpatient
glycemic management.2. Know the evidence that supports these
guidelines.3. Have an approach to managing inpatients with
hyperglycemia.

A word about Type 1 DM
• ALWAYS NEED basal insulin.
• Options:o Intermediate (NPH) SQ insulin q8-24hourso Long-acting (glargine/detemir) SQ insulin q12-
24ho Insulin pump basal rateo Intravenous Insulin Infusion

Why Do We Care?• Both Hyper and Hypo -glycemia are
associated with ↗ mortality and morbidity in-hospital.
• There has been little evidence to guide appropriate glycemic targets or glycemic management strategy in non-critically ill inpatients.

guidelines.diabetes.ca | 1-800-BANTING (226-8464) | diabetes.caCopyright © 2013 Canadian Diabetes Association
• Approximately 1/3 of in-patients have been found to have hyperglycemia
• Many have pre-existing diabetes prior to admission
Hyperglycemia
In-hospital Hyperglycemia is Common

What do you want to avoid
• In order of importance?oSevere hypoglycemic eventoDKAoSymptomatic hypo/hyperglycemiaoPersistent hyperglycemia
• Complications (association vs. causal)oThe “ready for discharge - except
requiring high doses of sliding scale insulin and has no long term diabetes management plan” syndrome

Why are sugars different in hospital?
• HigheroStress/concomitant illnessoNutrition (TPN, tube feeds, IV
dextrose)oDrugs (steroids)
• LoweroNutrition (diet, portions, NPO)oRenal failureo Liver failureoSevere illness

guidelines.diabetes.ca | 1-800-BANTING (226-8464) | diabetes.caCopyright © 2013 Canadian Diabetes Association
Hyperglycemia
Decreased immune
function, wound healing,
increased oxidative stress
Acute Illness
Increased stress hormones, use of glucocorticoids,
decreased level of activity
Inzucchi SE. NEJM 2006;355;1903
Hyperglycemia and Acute Ilness

guidelines.diabetes.ca | 1-800-BANTING (226-8464) | diabetes.caCopyright © 2013 Canadian Diabetes Association
Hyperglycemia
Increases risks of postoperative infections and
delirium
Prolonged hospital stay,
resource utilization
Increased renal dysfunction and renal allograft
rejection in transplant
Adverse Effects of Hyperglycemia

Armamentarium• Metformin• Sulfonylureas (Glyburide, Gliclazide)• Meglitinides (Repaglinide)• Alpha glucosidase inhibitor (Acarbose)• Incretins
• GLP-1 analogues (Exenatide, Liraglutide)• DPP-4 inhibitors (Sita/Lina/Saxa – gliptin)
• Thiazolidinediones (Rosi/Pio – glitazone)• SGLT2 inhibitors – cana (and other)
gliflozin(s) • Insulins

Insulins• Which ones do you know?


Guidelines• Canadian Diabetes Association –
2013• Endocrine Society – 2012
o Accompanied by Meta-Analysis
• American Diabetes Association – 2014
• American College of Physicians – 2011o Accompanied by Meta-Analysis

American College of Physicians
• Use of intensive insulin therapy for the management of glycemic control in Hospitalized patients: A CPG from the ACP: Feb. 2011.
• Intensive Insulin Therapy in Hospitalized Patients: A Systematic Review. Annals of Internal Medicine Feb. 2011.
• Organized into different clinical scenarios

Myocardial Infarction• 3 Trials (fair); 2 Trials (poor)• Target 4.0-11.0 mmol/L vs unspecified• Target 7.0-11.0 mmol/L + insulin on
dischargeo Mortality reduction o RR 0.69 (CI 0.49 – 0.96)
• Overall, no mortality reduction

Stroke• 2 Trials (fair); 2 Trials (poor)• Overall, no mortality reduction

Perioperative Control• 1 Trial (fair); 2 Trials (poor)• Target 3.9 – 10.0 mmol/L vs
unspecified
• No difference in health outcomeso Small studieso Low event rates

Infection Risk• 9 Trials (fair); 7 Trials (poor)• Sepsis
o Reduction of sepsis with Intensive Insulin o RR 0.79 (CI 0.62 – 1.00)
• Pooled result of wound infection, UTI, pneumonia or combinationo No significanceo RR 0.68 (CI 0.36 – 1.30)

Effects of intensive insulin therapy on rates of infection in various inpatient settings. We included inpatients in the MICU, SICU, and perioperative settings as well as patients with
stroke or acute brain injury.
Kansagara D et al. Ann Intern Med 2011;154:268-282
©2011 by American College of Physicians
sepsis
infx

General Medical Ward• 0 Trials

ACP• Recommendations deal with intensive
insulin in ICU (this presentation does not).
• Highlights lack of evidence regarding other hospitalized patient populations.

Intensive insulin ~ <7.8 pre-meal, <10 random


• This meta-analysis included observational studies (ACP did not)
• Main conclusion: Intensive Insulin may reduce risk of infection in non-critically ill patients (surgical)
• Low quality evidence• Intensive insulin ~ <7.8 acMeal, <10
random

Travel Plans• Now, that we’ve established we don’t
really know where we should go…
• How do we get there?

Cases

guidelines.diabetes.ca | 1-800-BANTING (226-8464) | diabetes.caCopyright © 2013 Canadian Diabetes Association
Patient Type Glucose Target (mmol/L)
Therapy of choice
Non-critically ill Fasting 5-8
Random <10
Pre-hospital regimen OR basal-bolus-correction
Critically ill 8-10 IV insulin infusion
CABG intraop 5.5-10 IV insulin infusion
Other periop 5-10 As appropriate
CABG = coronary artery bypass graft; IV = intravenous; Intraop = intraoperative; periop = perioperative
In-hospital Glycemic Targets

Targets (< 8 acMeal, < 10 Random)
Editorial
• No evidence for these targets in hospital (Outpatient targets)
• Reasonable place to start
• Safety first• Conservative dosing, avoid catastrophic hypos• Glucoses slightly above targets may be acceptable
• Try to maintain close to target• Symptomatic or severe hyperglycemia should
prompt action
• REASSESS targets and treatments daily

guidelines.diabetes.ca | 1-800-BANTING (226-8464) | diabetes.caCopyright © 2013 Canadian Diabetes Association
1. Provided that their medical conditions, dietary
intake, and glycemic control are acceptable, people
with diabetes should be maintained on their pre-
hospitalization oral anti-hyperglycemic agents or
insulin regimens [Grade D, Consensus]
Recommendation 1



guidelines.diabetes.ca | 1-800-BANTING (226-8464) | diabetes.caCopyright © 2013 Canadian Diabetes Association
Use BASAL + BOLUS + CORRECTION
In-hospital circumstances may warrant temporarily holding
other antihyperglycemic medications (eg. renal or
hepatic impairment)
Insulin = treatment of choice
BASAL + BOLUS + CORRECTION
Insu
lin
BOLUS + CORRECTION
BASAL
Breakfast Lunch Dinner

guidelines.diabetes.ca | 1-800-BANTING (226-8464) | diabetes.caCopyright © 2013 Canadian Diabetes Association
In the absence of routine
insulin, sliding scale insulin
regimen (bolus insulin on a prn
basis) is purely reactive rather
than proactive and allows for
hyperglycemia to occur before
responding
BG (mmol/L) Bolus insulin (U)
<4 Call MD
4.1 – 10.0 0
10.1 – 13.0 2
13.1 – 16.0 4
16.1 – 19.0 6
>19.0 Call MD
Queale WS. et al. Arch Int Med 1997;157
Sliding Scale Alone is Inefficient

guidelines.diabetes.ca | 1-800-BANTING (226-8464) | diabetes.caCopyright © 2013 Canadian Diabetes Association
4.0
10.0
Breakfast Lunch Dinner Bedtime
BG (mmol/L) Bolus insulin (U)
< 4 Call MD
4.1 – 10.0 0
10.1 – 13.0 2
13.1 – 16.0 4
16.1 – 19.0 6
> 19.0 Call MD
6.0
Bolus insulin QID
14.0
6.0
16.5
3.0
Sliding Scale alone
What do you do?
What do you do?
What do you do?
What do you do?
+4 U
0 U 0 U
+6 U
QID: four times daily; SSI: sliding-scale insulin; BG: blood glucose
Sliding Scale Insulin Alone Results in Variable Glucose Control
BG (mmol/L)

guidelines.diabetes.ca | 1-800-BANTING (226-8464) | diabetes.caCopyright © 2013 Canadian Diabetes Association
BASAL + BOLUS + CORRECTION Results in Smoother Glycemic Control
4.0
10.0
Breakfast Lunch Dinner Bedtime
BG (mmol/L) Bolus insulin (U)
< 4 Call MD
4.1 – 10.0 0
10.1 – 13.0 2
13.1 – 16.0 4
16.1 – 19.0 6
> 19.0 Call MD
6.0
12.0
6.0
Correctional Insulin AC meals
What do you do?
What do you do?
What do you do?
6+2 U
6+0 U
6U 6U
What do you do?
6+0 U
6.0
ROUTINE Bolus insulin
Basal insulin
6U
18 U
Routine Basal

Rabbit -2 Trial Medicine
• At 2 American Academic Hospitals • Open label, randomized study• 130 insulin naïve non-surgical
inpatients, known history of diabetes and initial BG 7.8 – 22.2.
• OHAs stopped, randomized to SSI or basal-bolus with glargine + glulisine.
• Admission BG = 12.7, A1c = 8.8%

Scheduled Dose

Sliding scale

Sliding scale/Supplemental
doses
7.8 – 10
>22.2
14.4 – 16.7

Comment on doses• Scheduled routine dosing
o 0.4 – 0.5 Units/kg/dayo 50% glargine, 50% glulisine
o E.g. 70 kg person• 30-35 Units/day• ~15 Units glargine• ~5/5/5 Units glulisine
o Conservative?


RABBIT 2 Results
10
13.3
5.6

Rabbit 2 Surgery 2011• Similar to Rabbit trial, similar glycemic results.

guidelines.diabetes.ca | 1-800-BANTING (226-8464) | diabetes.caCopyright © 2013 Canadian Diabetes Association
*
*
ŧŧ
††
RABBIT 2 RABBIT 2 Surgery
Adapted from: Umpierrez GE, et al. Diabetes Care 2007;30:2181-86. Adapted from: Umpierrez GE, et al. Diabetes Care 2011;34:256-61.
Basal-Bolus (BBI) Regimen Achieves Better Control than Sliding Scale (SSI) Alone
Blo
od
glu
cose
(m
mo
l/L
)
¶
¶
¶
***
Admit 1 2 3 4 5 6 7 8 9 10
Duration of treatment (days)
5.6
6.7
7.8
8.9
10.0
11.1
12.2
13.3
*p < 0.01; ¶p < 0.05.
¶
SSI
BBI
1Randomi-zation
2 3 4 5 6 7 8 9
Duration of treatment (days)
6.7
7.8
8.9
10.0
11.1
13.3
*p < 0.001, ŧp = 0.02, †p = 0.01
SSI
BBI

RABBIT 2 Results• End point:
o Target BG <7.8; o 66% in Basal/Bolus, 38% SSI
• No differences in hospital stay or hypoglycemia

Basal Plus Trial• Umpierrez GE, et al. Randomized
Study Comparing a Basal Bolus With a Basal Plus Correction Insulin Regimen for the Hospital Management of Medical and Surgical patients With Type 2 Diabetes: Basal Plus Trial. Diabetes Care. 2013 Feb 22. [Epub ahead of print].

Basal Plus• Multicentre, 375 DM2 patients• Home regimen: diet, oral agents, or
low dose insulin, randomized 2:2:1
1. Basal-Bolus-Correction [glargine-glulisine]
2. Basal Plus (sliding scale) [glar-glu]3. Sliding Scale (alone) [regular]

Basal-Bolus-Correction

Basal Plus

Sliding Scale – Added to Basal
bolus or Plus (glulisine) OR alone
SSI (R)

Insulin adjustment• Basically increase insulin by 10%
if mildly high, 20% if high.
• Reduce by 20% if low.


Basal Plus Trial• Treatment Failure (mean glucose
or 2 consecutive > 13.3)o Basal Bolus 0, Basal Plus 2%, SSI 19%
• Hypoglycemiao Less than 3.8
• Significantly less in SSIo Less than 3.3
• Trend to less in SSIo Less than 2.2
• 1 event each in basal bolus and basal plus, 0 in SSI

Basal Plus Trial Conclusions
• DM2 patients who are not on high doses of insulin can be managed by a Basal Plus (SSI) routine
• Basal Plus controls hyperglycemia = Basal Bolus, and better than a SSI with Insulin R
• Concern about hypoglycemia risk in basal bolus/basal plus.o Assumption is risk is low and outweighed by risks of
hyperglycemia with SSI• Evidence?

guidelines.diabetes.ca | 1-800-BANTING (226-8464) | diabetes.caCopyright © 2013 Canadian Diabetes Association
CONTINUE pre-hospital diabetes regimen if
appropriate, otherwise …
USE insulin as the treatment of choice
DO NOT use sliding scale insulin alone
DO use BASAL + BOLUS + CORRECTION insulin
regimen
AVOID hypoglycemia
2013In-hospital Management Checklist
guidelines.diabetes.ca | 1-800-BANTING (226-8464) | diabetes.caCopyright © 2013 Canadian Diabetes Association
Recommendation 2
2. For hospitalized patients with diabetes treated with
insulin, a proactive approach that includes basal,
bolus, and correction (supplemental) insulin,
along with pattern management, should be used to
reduce adverse events and improve glycemic
control, instead of the reactive sliding-scale
insulin approach that uses only short- or rapid-acting
insulin [Grade B, Level 2]

guidelines.diabetes.ca | 1-800-BANTING (226-8464) | diabetes.caCopyright © 2013 Canadian Diabetes Association
3. For the majority of non critically ill patients treated
with insulin, pre-meal BG targets should be 5.0 to
8.0 mmol/L in conjunction with random BG values
<10.0 mmol/L, as long as these targets can be
safely achieved [Grade D, consensus]
4. For most medical/surgical critically ill patients
with hyperglycemia, a continuous IV insulin
infusion should be used to maintain glucose levels
between 8.0-10.0 mmol/L [Grade D, consensus]
2013
2013
Recommendations 3 and 4

guidelines.diabetes.ca | 1-800-BANTING (226-8464) | diabetes.caCopyright © 2013 Canadian Diabetes Association
5. To maintain intraoperative glycemic levels between
5.5-10.0 mmol/L for patients with diabetes
undergoing CABG, a continuous IV insulin infusion
protocol administered by trained staff, [Grade C, Level 3]
should be used
6. Perioperative glycemic levels should be maintained
between 5.0-10.0 mmol/L for most other surgical
situations, with appropriate protocol and trained staff
to ensure safe and effective implementation of
therapy and to minimize the likelihood of
hypoglycemia [Grade D, Consensus]
2013
Recommendations 5 and 6

guidelines.diabetes.ca | 1-800-BANTING (226-8464) | diabetes.caCopyright © 2013 Canadian Diabetes Association
7. In hospitalized patients, hypoglycemia should be
avoided:
– Protocols for hypoglycemia avoidance, recognition
and management should be implemented with nurse
–initiated treatment, including glucagon for severe
hypoglycemia when IV access is not readily available [Grade D, consensus]
– Patients at risk of hypoglycemia should have ready
access to an appropriate source of glucose (oral or
IV) at all times, particularly when NPO or during
diagnostic procedures [Grade D, Consensus]
2013Recommendation 7




guidelines.diabetes.ca | 1-800-BANTING (226-8464) | diabetes.caCopyright © 2013 Canadian Diabetes Association
8. Healthcare professional education, insulin
protocols and order sets may be used to improve
adherence to optimal insulin use and glycemic
control [Grade C, Level 3]
9. Measures to assess, monitor, and improve glycemic
control within the inpatient setting should be
implemented, as well as diabetes-specific
discharge planning [Grade D, Consensus]
2013Recommendation 8 and 9

guidelines.diabetes.ca | 1-800-BANTING (226-8464) | diabetes.caCopyright © 2013 Canadian Diabetes Association
CONTINUE pre-hospital diabetes regimen if
appropriate, otherwise …
USE insulin as the treatment of choice
DO NOT use sliding scale insulin alone
DO use BASAL + BOLUS + CORRECTION insulin
regimen
AVOID hypoglycemia
2013In-hospital Management Checklist

Question• 55 yr old person with Type 2 DM on
oral agents (metformin and gliclazide) who will be NPO for an indefinite period of time.
• What are your options for in hospital treatment?

DM2: NPO on Gliclazide and Metformin
What do you want to avoid
• In order of importance?oSevere hypoglycemic eventoDKAoSymptomatic hypo/hyperglycemiaoPersistent hyperglycemiao The “ready for discharge except
requiring high doses of sliding scale insulin and has no long term diabetes management plan” syndrome
• Hold Oral agents when NPO

Insulin Strategies• Basal Bolus
o Scheduled bolus inappropriate if NPOo Risk of hypoglycemia
• Basal Plus (SSI)o Reasonable
• Basal dose ~0.1-0.25 U/kg (half of a total estimated daily dose of ~0.2-0.5 U/kg)
• SSI aloneo Reasonable – IF TEMPORARY
• If very concerned about hypoglycemia, can use gentle DOSE FINDING sliding scale.
• REASSESS in 12-24 hours consider basal insulin

If Not NPO - Insulin• Basal Bolus
o Reasonable• Total daily dose ~0.2-0.5 U/kg/day
o 50% Basalo 50% Bolus (divided by 3 to be given at 3 meals)
• I would use gentle sliding scale option to start, but reassess often
• Basal Plus (SSI)o Reasonable
• 50% of total daily dose as basal• ~0.1-0.25 U/kg/day• Consider more aggressive sliding scale option
• Sliding Scale Aloneo Only if high concern for hypoglycemiao If requires sliding scale doses in first ~12 hours strongly
reconsider strategy

If Not NPO – Oral agents
• Discontinue Metformin if:o Liver failureo Heart Failureo Renal Failureo Radiocontrast dyeo Acidosis
• Usually discontinue gliclazide (sulfonylurea) re: hypoglycemiao Consider re-instituting if no hypoglycemia and clinically
stableo Renal/liver/cardiac function stableo Not expected to be NPOo Want to try transitioning off insulin before d/c

Rational Sliding Scale• Reassess DAILY!
o If no or very few sliding scale doses sugars are <10 and no change required.
o If sliding scale is being used blood sugars are >10
• i.e. add OHA, add Basal, premix or MDI insulin
• Unless expect insulin requirements to decrease
Ac Breakfast
Ac Lunch Ac Supper qhs
13 – 4 Units
11 – 2 Units
17 – 8 Units
13 – 4 Units
10 – 0 Units
15 – 6 Units

Rational Sliding Scale• Reassess DAILY!
o In addition to assessing need for DM mgmt plan assess scale
• If constantly increasing and very high sugar then consider tightening scale
• If there are BGs <6 reassess scaleo Risk of hypos – consider loosening
• If there are BGs less than 4 decrease insulino Scale, scheduled, OHAs or a combination
acBreakfast
acLunch acSupper Bedtime
9 – 0 Units 12 – 2 Units
14 – 4 Units
18 – 8 Units
13 – 4 Units
16 – 8 Units

Consider DM1 made NPO
• Home insulin lispro 6/6/8 U and glargine 20 U
• Options?o IV insulin infusion = “Right” answero Glargine (usual, slight decrease, slight increase?) + scale if
sugars stable/easy to manageo Can stabilize with IV insulin infusion then when stable
transition to basal insulin based on requirements• E.g. add up 24 hour insulin requirement and deliver slightly
less as basal SQ + corrective scale for highs (remember may be insulin sensitive if requirements are low)
• Bottom line – DO NOT interrupt insulin delivery!o Sliding scale only is WRONG!

Approach to Hospitalized Patient with severe insulin
resistance
• J Clin Endocrinol Metab Sept 2011

Causes of insulin resistance in hospitalized patients
• Stress response• Obesity• Electrolyte disturbance: low K/Ca/Mg or high Ca• Feeds• Fatty emulsion eg. Propofol• Steroids/Tacrolimus/Sirolimus• Anesthetic Agents: volatile agents• Hormonal agents: octreotide, leuprolide, bicalutamide• Hormonal disorders: Cushing’s Syndrome,
Acromegaly, Hyperaldosteronism, Pheochromocytoma

Approach to Patient• Rule-out pseudo-resistance
o Check IV bag, tubing, IV site
• Review medications• Assess for concurrent diseases• Check electrolytes• Check if dextrose is used• Assess feeds
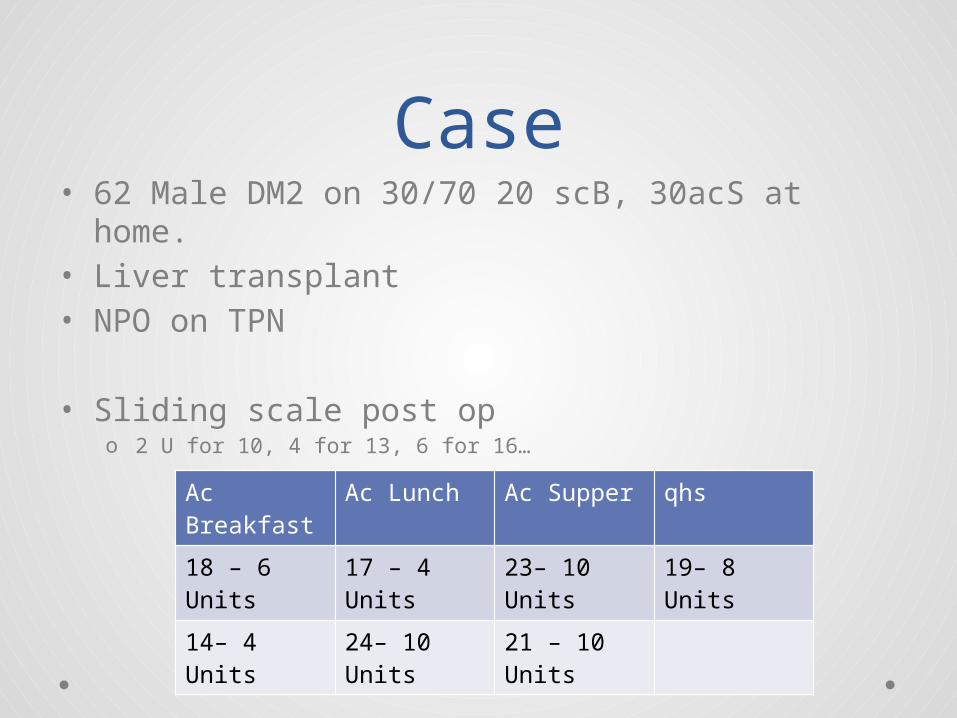
Case• 62 Male DM2 on 30/70 20 scB, 30acS at home.• Liver transplant• NPO on TPN
• Sliding scale post opo 2 U for 10, 4 for 13, 6 for 16…
Ac Breakfast
Ac Lunch Ac Supper qhs
18 – 6 Units
17 – 4 Units
23– 10 Units
19– 8 Units
14– 4 Units 24– 10 Units
21 – 10 Units

• If patient receiving SCo Consider change to IV insulin infusiono SC insulin may be poorly absorbed due to
edema poor perfusion etc


Feeds/TPN• May consider adding regular insulin
to TPN bago Will decrease risk of hypoglycemia if TPN heldo Max dose 50% of daily requirement of insulin
• Change feed to enteral feeds• Decrease or hold TPN with
consultation • Decrease Intralipid
o Changing from FFA infusion to soybean fat

Transition from IV to SC
• Patient on and staying on continuous feeds?
• IV insulin 3-5 U/hr over last 24 hours

Patient on and staying on continuous feeds
• Requirement for Basal and Supplemental Insulino Estimates 24hr insulin requirements from the IV infusion
(eg. units/hr x 24 hrs)o Options:
• 1/3 dose as NPH q8h• ½ dose as glargine or detemir q12h• Full dose as glargine or detemir q24h

• Overlap IV with SC for 3 hrs; sorter if glucose falls < 5.5 mmol/L
• Change BG checks to q4h once IV is off
• Add fast acting analog or regular insulin q4h
• Reassess and adjust

Transition from IV to SC
• Currently on continuous feeds with plans to stop and advance diet?
• On 3-5U/hr IV

Currently on continuous feeds with plans to stop and advance
diet• Requirement for Basal, Bolus and
Supplemental insulino Stop feeds while continuing with the IV infusiono After 4-5 hrs estimate basal requirements
• New rate while off feeds eg. 2 units/hr • ~24hr req 48 units
o Options• Give entire basal dose as once daily glargine or detemir or
use split dosing half in the morning, half at HS• Use NPH: 2/3 ACB and 1/3 evening or 50:50 split

• Estimate requirement for mealso Give fast acting analog or regular using a CHO ratio with
meals, if previous ratio unknown start with 1:15; if resistant use 1:7 1:5
o Use fixed dose approx 50% of basal insulin dose divided for each meal
• (units of basal/3 = units for each meal)o If limited intake may need small doses with adjustment as
intake improves
• Overlap IV insulin• Blood glucose checks AC meals and HS,
consider 3 AM checks

Transition from IV to SC
• Currently on continuous feeds with plan for intermittent or overnight feeds?
• On 3-5U/hr IV

Currently on continuous feeds
with plan for intermittent or
overnight feeds• Scheduled overnight feeds
o Calculate 24hr requirements as previouslyo At initiation of feeds: administer NPH in the
evening with additional 5-10 units of fast acting analog or regular insulin
o Check BG at 3AM and at the end of the feedso Adjust as requiredo If patient eating during the day assess BG
levels and treat if required

• If bolus feedsoAdd fast acting insulin at the time of
planned feedsoBase dose on CHO count and use a ratio
or fixed dose insulin

Steroids• May need additional insulin• NPH may be used in the AM when steroids
are given and adjusted as the dose of steroids is tapered
• Meal time insulin may also need to be increased for 4 – 8 hrs after the steroid is given
• Multiple doses of dex have a long T1/2

Take Home Messages• Safety first
o Avoid lows and significant highso Consider whether to continue or stop orals
• Insulin Strategyo Basal +/- Boluso Almost never should use Sliding scale alone
• Reassess and adjust• Plan for discharge
o When medically stable consider• Taper insulin/re-introduce orals• Plan for discharge on insulin with appropriate education
and follow up