post ercp duioenal perforation ( a review of litearture)
TRANSCRIPT
DR Fiaz Fazili-Ac Care surgeon

1. Indication of ercp- in jaundice2. Complications of ercp.3. Tips and tricks to do ercp4. Who can do ercp?accreditation5. Risk factors for complications6. During Ercp- findings7. Management of duod perf during /after ercp8. Management- protocol- is ct scan essential9. 9.when to operate- when to watch-indic of
surgery—correct procedures10. Mort/morbdt-cholangitis –elderly- septic

This topic review will focus on the risk factors, diagnosis, and treatment of post-ERCP perforation. An overview of the complications of ERCP, and
Detailed discussions of other individual complications are presented separately.
"Overview of indications for and complications of ERCP and endoscopic biliary sphincterotomy”
"Post-ERCP pancreatitis“ "Post-ERCP bleeding" , "Rare complications of ERCP" )

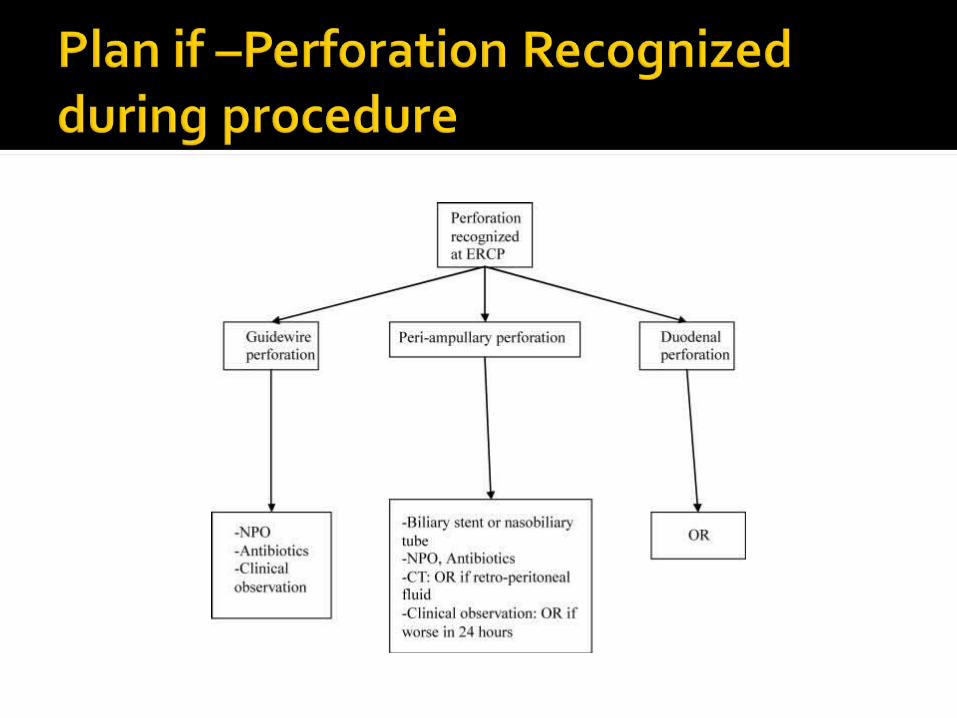
— Three types of perforation complicating endoscopic retrograde cholangiopancreatography (ERCP) are most frequently recognized-[1,2] :
Retroperitoneal duodenal perforationFree bowel-wall perforationPerforation of the bile ducts
Of these, retroperitoneal duodenal perforations are the most common. They usually occur as a result of a sphincterotomy that extends beyond the intramural portion of bile duct. Perforation of the bile ducts usually occurs following dilation of strictures, forceful cannulation, and guidewire insertion, or stent migration [ 3-9] .
Free abdominal perforation of the duodenum or jejunum is rare, usually occurring in patients with a stricture or anomalous anatomy such as Billroth II gastrectomy [ 10-12] .
Gastric and esophageal perforation [ 3,13,14] , and pneumomediastinum without evidence of perforation [ 15] have also been described after ERCP and sphincterotomy.
Intestinal perforation related to biliary stents is another uncommon complication. (See "Rare complications of ERCP

Perforation is rarely evident endoscopically ( show endoscopy 1 ).
Free abdominal perforation is almost always recognized immediately based upon during ERCP on fluoroscopic findings;or by . clinical symptoms, physical signs,
in contrast,Retroduodenal perforation is usually determined by the radiologic evidence of air or contrast in the retroperitoneal space outside the confines of the bile duct and duodenum during CT evaluation for post-ERCP pain. Patients with undetected leaks can present hours after the procedure with -pain, fever, and leukocytosis.
Pneumomediastinum and subcutaneous emphysema are unusual [ 15-19] . Pneumothorax [ 20] and gas in the portal system [21] have also been rarely described.

An abdominal CT scan should be obtained in patients who are suspected of having a perforation even if they do not have evidence of retroperitoneal air on plain films
since CT scan is the most sensitive means for detecting perforation [ 22,23]
The clinical or radiographic amount of air does not always indicate the size of the perforation or correlate with the severity of the complication, but rather reflects the degree of manipulation after the perforation occurred [ 22,24] .

perforation is typically associated with the presence of retroperitoneal air, which may be detected by plain radiographs or CT.
However, retroperitoneal air may also develop following sphincterotomy in patients who are clinically asymptomatic [23,25] . Such patients may not require intervention.
This was illustrated in a series of 21 patients studied prospectively who underwent an abdominal CT scan following sphincterotomy.
Retroperitoneal air was observed in six (29 percent) patients, all of whom were asymptomatic and had an uneventful postprocedural course [ 25] .
No clinical or procedure-related characteristics predicted the presence of air

The origin of retroperitoneal air in such patients is presumably related to dissection through an injured or macroscopically intact bowel, which has also been described after colonoscopy [ 26,27] , although sealed microperforations are also possible.
These findings suggest that the presence of retroperitoneal air in the absence of symptoms should warrant careful observation but may not require intervention
—The finding of retroperitoneal air may be challenging in
patients who are symptomatic following sphincterotomy in whom a distinction needs to be made between perforation, clinically insignificant retroperitoneal air, and pancreatitis,
particularly since pancreatitis and perforation can have a similar clinical presentation or occur simultaneously [ 21,22,28]
This was illustrated in a study that included 36 patients who developed prolonged abdominal pain following sphincterotomy who underwent a diagnostic CT scan.
Complications included acute pancreatitis in 23 patients (64 percent), and duodenal perforation in 11 (31 percent), and both pancreatitis and duodenal perforation in six patients (17 percent) [ 22] .
The diagnosis of retroperitoneal duodenal perforation associated with pancreatitis should be based upon the detection of retroperitoneal air or contrast in a symptomatic patient meeting criteria for post-ERCP pancreatitis. ( See "Post-ERCP pancreatitis" )
A retroperitoneal abscess should be suspected in patients with post-ERCP pancreatitis who develop back pain and persistent fever [ 29] .

To establish or exclude diagnosisTo know whether to observe or
operate----indic of surgeryAssociated problems- pn -
mediastinum; pancreatitis—Collection small- ct guided aspirationF up--

GRADING — Post-ERCP retroperitoneal perforation can be graded as
Mild,moderate or severe based upon a consensus definition [ 30] :
Mild — Possible, or only very slight leak of fluid or contrast, treatable by fluids and suction for three days or less
Moderate — Any definite perforation treated medically for 4 to 10 days
Severe — Medical treatment for more than 10 days, or intervention (percutaneous or surgical)
Ref;30.Cotton, PB, Lehmann, G, Vennes, J, et al. Endoscopic sphincterotomy complications and their management: An attempt at consensus.Gastrointest Endosc 1991; 37:383.

Retroduodenal perforation was reported in 0.5 to 2.1 percent of sphincterotomies in a number of large series, many of which were performed more than a decade ago [ 30] .
More recently, the incidence or perforation has appeared to decrease to less than 0.5 percent, probably because of improvement in experience and skill of the endoscopists [ 31] .
However, severe and fatal cases continue to occur [ 32,33] .
In a summary of 21 prospective studies involving 16,855 patients undergoing diagnostic and therapeutic ERCP between 1987 and 2003, post-ERCP perforations totalled 101 (0.60 percent), with 10 deaths (0.06 percent) [ 34]

The. A total of 30 perforations (0.4 percent) were reported in two prospective multicenter studies involving 7252 patients
undergoing mainly therapeutic ERCP [ 35,36] . Perforations were observed in 0.6 percent of 12,427
ERCPs in a report from the Mayo clinic [37] . The most common causes were due to guidewire
insertion (32 percent), sphincterotomy (15 percent), passage of the endoscope (11 percent) and stent migration (9 percent).
A documented perforation (esophageal, gastric, duodenal or bile duct) occurred in 33 of 9314 patients (0.3 percent) who underwent ERCP at the Duke University from 1987 to 1998 [ 3]

Retroduodenal or bowel wall perforation occurred in 8 of 2347 patients (0.3 percent) undergoing biliary endoscopic sphincterotomy in a prospective series from North America [ 38] .
It was severe in five (0.2 percent), and fatal in one patient (0.04 percent).
Forty patients with perforation were identified in a series of 6040 ERCPs
(0.6 percent), including 2874 endoscopic sphincterotomies, performed between1994 and 1998 [ 1] . Free peritoneal perforation occurred in 1 of 942 (0.1 percent)
patients undergoing diagnostic ERCP, and in 3 of 1827 (0.2 percent) patients undergoing therapeutic ERCP in a large Italian series [ 39] .
Retroperitoneal perforation occurred in 12 of 1827 patients (0.7 percent) who underwent therapeutic ERCP, with only one death (0.05 percent).
Over a two-year period an esophageal perforation, a free duodenal perforation, and 15 retroperitoneal perforations occurred in 3124 patients (0.5 percent) undergoing diagnostic and therapeutic ERCP

A number of patient- and procedure-related risk factors for perforation have been identified in individual reports and in large series.
A difficulty with interpreting the risk factors identified in these reports is that many of the studies combined free bowel wall perforation at a site remote from the
papilla (endoscope-related) and periampullary retroperitoneal perforation
(sphincterotomy-related). The mechanisms leading to the different types
of perforations are substantially different. Furthermore, the absolute number of patients
studied is small, reflecting the infrequent occurrence of these complications.
The following risk factors for both free abdominal or retroperitoneal perforation were identified by multivariate logistic regression analysis in a large retrospective case-control study that included 33 ERCP-related perforations out of 9,314 ERCP procedures [ 3] :

Procedure-related risk factors — Performance of a sphincterotomy, longer duration of the procedure, and biliary stricture dilation.
The risk of bowel wall perforation is increased in patients who have stenosis in the upper gastrointestinal tract or bile ducts, and in patients who have undergone gastric resection [10,11,43] .
Particular caution is required with the use of the side-viewing duodenoscope in patients with a Billroth II gastrectomy [ 43,44] .
(See "ERCP after Billroth II reconstruction" ).

The risk of retroperitoneal perforation is increased with precut sphincterotomy and larger sphincterotomies, particularly those that are created outside of the usually recommended landmarks (11 to 1 o'clock) [ 39,45-47] .
In one report, 7 of 13 sphincterotomy perforations were related to precutting [ 3] . (See "Precut
(access) papillotomy" ). Other risk factors identified in individual reports
includea small caliber bile duct [ 48] , the presence of a peripapillary
diverticulum [ 46]. intramural injection of contrast [ 39]

The risk of perforation can be minimized when ERCP is performed by well-trained endoscopists and assistants abiding by the
following technique-related principles [ 41] : Proper orientation of the sphincterotome between 11
and 1 o'clock Step-by-step incision Avoiding a "zipper" cut Sphincterotomy length tailored to the size of papilla,
bile duct, and eventual stone Judicious use of precut ( see "Precut (access)
papillotomy" ) Appropriate technique in cases of anatomical variants
such as peripapillary diverticula and Billroth II gastrectomy
( see "ERCP after Billroth II reconstruction" )
Patients with esophageal and free abdominal gastric,jejunal, or duodenal perforation usually require surgery [ 3,13,14,49 ] .
In contrast, a conservative approach to retroperitoneal perforation following endoscopic sphincterotomy has been adopted over the years [ 2,3,37,50,51] .
However, early surgical consultation and careful observation is mandatory since the outcome may be poor in patients who do not receive prompt and appropriate treatment [ 1,52,53] .


The successful non-surgical management of retroduodenal perforation following endoscopic sphincterotomy is reported in the literature
Two patients are described who developed gas in the retroperitoneum following endoscopic sphincterotomy. One patient developed retroperitoneal emphysema and cervical
emphysema, the second patient developed retroperitoneal emphysema and a
pneumothorax following endoscopic sphincterotomy. Both patients were treated conservatively and made uneventful
recoveries. An algorithm for assessment and treatment is proposed based on the
authors' experience and a literature review. Patients with confirmed ongoing duodenal leakage,
sepsis or collection should have expeditious surgery

Suspicion and diagnosis of a procedure-related perforation can be facilitated greatly by clinical findings and especially radiographic imaging with contrast studies, CT, and even magnetic resonance imaging.11, 21
Most important, suspicion of perforation should be high in patients with pain or fever after any periampullary endoscopic procedure. This concern is especially true when the procedure is therapeutic or technically difficult; the patient has local anatomic variations, such as periampullary diverticula22; strictures are dilated; there are changes in the usual anatomy related to previous operative interventions (eg, gastrectomy); or intubation is difficult. I
if there is any suspicion of perforation, prompt diagnosis and institution of systemic support with broad-spectrum antibiotics and intravenous resuscitation is mandatory;
Early diagnosis and prompt treatment during the endoscopic procedure are vital for a better outcome.1, 11, 18-20 .
when perforation is confirmed, external biliary, duodenal, and/or
pancreatic drainage may be indicated. Some patients could be managed by diversion or decompression of contents from the duodenum by placing a nasoduodenal tube alone or with internal pancreaticobiliary
drainage
1. Preetha M, Chung YF, Chan WH; et al. Surgical management of endoscopic retrograde cholangiopancreatography-related perforations. ANZ J Surg. 2003;73:1011-1014. FULL TEXT |. Masci E, Toti G, Mariani A; et al. Complications of diagnostic and therapeutic ERCP: a prospective multicenter study. Am J Gastroenterol. 2001;96:417-423. FULL TEXT | WEB OF SCIENCE | PUBMED .
Background: A retrospective review was carried out of consecutive cases of endoscopic retrograde cholangiopancreatography (ERCP)-related perforation to identify risk factors and technique affecting surgical outcome.
Methods: Eighteen patients (0.45%) out of 4030 ERCP performed were operated on for ERCP-related perforation at Singapore General Hospital.
Results: The group's median age was 72.5 years and 14 patients had ductal stone disease. Five perforations were discovered at ERCP while 10 required computed tomography for diagnosis. Eight patients were operated on within 24 h whereas 10 patients had surgery after 24 h. Five of six with type I (lateral duodenal) perforations had early surgery versus one of seven with type II (peri-Vaterian; P = 0.03). There were four type III (bile duct) perforations and one type IV (retroperitoneal air). Five of six patients with type I perforation had simple repair compared with five of seven type II requiring the complex duodenal diversion procedure (P = 0.10). Three patients (16.7%) succumbed after surgery due to sepsis and myocardial infarction. Advanced age>70 years resulted in higher mortality of 30% versus none in patients <70 years (P = 0.22).
Conclusions: Early diagnosis is important but difficult especially for the type II perforations. Duodenal diversion is used more frequently in patients with type II perforations and those operated on late. Advanced age contributes to poorer outcome in surgical treatment of ERCP perforations.

Guidewire manipulation was the presumed cause of perforation in 24 patients (32%), and 11 (15%) were sphincterotomy-related perforations, 8 (11%) were related to difficulties in passage of the endoscope, 8 (11%) occurred during cannulation, 7 (9%) occurred in the process of stent insertion, and 5 (7%) occurred
during stricture dilatation (Table 1). The exact mechanism of perforation was unknown in 11 patients (15%). The
duodenum and the bile duct were the most common sites of perforations (Table 1).
Of the 75 perforations, 45 were identified immediately: 26 (35%) by direct endoscopic visualization and 19 (25%) by fluoroscopic identification of extravasation of contrast.
Eight patients (11%) were suspected of having a perforation during the procedure, and it was confirmed using computed tomography (CT).
. Five other patients (7%) had the perforation diagnosed within 6 hours of the procedure, and in 8 (11%), the perforation was recognized within 6 to 24 hours.
A delayed diagnosis (>24 hours) occurred in 9 patients (12%). Patients who were identified as harboring a perforation during the procedure presented later with symptoms and signs of abdominal pain (44%), leukocytosis (35%), fever (17%), hypotension (3%), and chest pain (1%).
The modalities used to identify and confirm the suspicion of a perforation in these delayed presentations included CT (n = 19, 25%), abdominal radiographs showing free intraperitoneal or retroperitoneal air (n = 10, 13%), and magnetic resonance imaging (n = 1, 1%).

The pre-intervention plan was executed endoscopically with success in 45 patients (60%); however, 30 procedures (40%) were abandoned prematurely because of the perforation. After recognition of the perforation, overall, 53 patients (71%) were managed nonoperatively, and 22 (29%) were managed operatively. The mean hospital stay for the entire group was 8 ± 1 days, with 5
deaths (7%).
Endoscopic management of the perforation was attempted in 27 (36%) of these 75 patients, including 14 with duodenal perforations, 12 with biliary perforations, and 1 with pancreatic duct perforation.
Endoscopic treatments for perforation included biliary stents in 10 patients, a nasobiliary drain or nasogastric tube in 5 patients each, endoscopic placement of a clip(s) in an attempt to "close" the site of
perforation in 8 patients, a nasoduodenal tube in 3 patients, and a pancreatic duct stent in the 1 patient with a pancreatic duct
perforation. Five of these 27 patients failed endoscopic management and were
transferred to the operating room immediately. Twenty-two (81%) of the 27 patients were admitted for observation, 18
(80%)of whom were managed successfully using a nonoperative approach; 4 (20%) required operative treatment eventually.


The overall mortality due to perforations resulting from periampullary procedures was 7% (n = 5). Hospital mortality was greater in the operative group (13% vs 4%; P<.05). Four deaths were secondary to sepsis and multiorgan failure 10 to 35 days later. One patient, managed nonoperatively, died the evening of the endoscopic procedure from a tension pneumothorax. Complications after operative treatment included intra-abdominal abscess, hemorrhage, pancreatitis, and wound infection (n = 1 each). Patients in the operative group were older than those in the nonoperative group (64 ± 4 vs 55 ± 2 years; P = .02). The median ASA status was also greater (3 vs 2; P = .003), with 18 patients (82%) in the
operative group having an ASA status of at least 3, whereas only 22 nonoperative patients (42%) had an ASA status of 3 or greater.
Univariate analysis was performed to identify the association of variables such as age, sex, ASA status, grade of procedure, site of perforation, and duration of hospital stay between operative
and nonoperative management. This analysis revealed that the mean age of patients requiring operative management was
greater than that of those managed nonoperatively (65 ± 4 vs 55 ± 2 years; P = .02). An association was found between higher ASA status (3) and the need for an operative treatment (P = .003). Patients with duodenal perforations were more likely to require an operation than patients with bile duct perforations (P<.001). Increasing technical difficulty (grade) of the procedure was associated with requiring operative management (P = .02). The hospital stay was greater for patients requiring an operation vs those who could be managed nonoperatively (16 ± 4 vs 4 ± 1 days; P<.001). Sex difference and history of previous ERCP did not seem to predispose patients to require operative treatment; however, on applying the multivariate logistic regression model we found that the associations of ASA status and site of perforation with patients requiring operative management remained significant (P = .01 and .003, respectively).

The management of perforations after therapeutic periampullary
endoscopic procedures has remained a major controversy. The present data indicate that most ductal perforations caused
by guidewire passage (21 of 24) or during attempted cannulation (6 of 8) cause focal tears or perforations, which can be managed nonoperatively using sphincterotomy, nasobiliary drains, or endoluminal stents.23-25 .
Successful nonoperative management of sphincterotomy-related retroperitoneal perforations is also possible, despite extensive retroperitoneal air noted on CT, provided the patients remain nontoxic.26-
27.
In contrast, if patients develop abdominal pain or fever or appear toxic clinically, surgical consultation should be obtained, and operative exploration for effective repair or drainage should be considered, especially in elderly or otherwise chronically ill patients less able to withstand the physiologic stress.
We offer clinical management algorithms for patients noted to have a perforation either during or after completion of the procedure


Dr Sielaff also asked about a management algorithm. While the care of each patient should be individualized, there are some generalizations that can be made.
It is important to talk to your endoscopist and ask whether he or she noticed the complication at the time of the procedure or not.
Was the perforation guidewire related? Was it a perforation of the bile duct? If it was a guidewire perforation of the bile duct, it is highly likely that it can be managed nonoperatively.
A sphincterotomy perforation is a complication that can go either way.; In such a patient, CT to determine if there is objective evidence of
perforation and careful clinical monitoring of the patient to determine if toxicity is present would help to dictate the need for operative
intervention. Patients who have altered anatomy, such as prior gastrectomy and Billroth II
gastroenterostomy, those patients with peri-Vaterian diverticula, and those in whom scope passage resulted in a gaping perforation visible to the endoscopist or associated with gross extravasation on contrast examination represent a group of patients that will probably need to be operated on straight away. In this subset of patients, we would not wait for them to deteriorate clinically before making a recommendation to intervene operatively.
Richard C. Thirlby, MD, Seattle, Wash: I have 1 comment and a question. I think I would quibble just a little bit with 1 of your conclusions

CT scan is essential. Would you require extravasation of contrast? Do you know how many patients were attempted to be managed medically who failed and subsequently went to operation? That might be helpful information.
Dr Farnell: Dr Thirlby is making the point that judgment may be appropriate in patients who have sphincterotomy perforation. The patients that we have recommended be operated on immediately are those in whom passage of the endoscope results in an intraperitoneal gaping perforation.
For patients with biliary sphincterotomy-induced perforations, we would agree with you that the approach to these patients should be individualized. If there is evidence of a perforation after endoscopic sphincterotomy, both the clinical status of the patient and imaging are important. If the patient has a
negative abdominal examination, does not have signs of systemic
toxicity, and has minimal or no extravasation from the site of the sphincterotomy on abdominal CT with oral contrast, antibiotic therapy, fluid resuscitation, and careful observation would be appropriate.
operative intervention is our recommendation -iI there is gross extravasation
into the peritoneal cavity or retroperitoneum and if there is evidence of toxicity,.
Our endoscopists do have some experience using hemoclips to manage small endoscopic perforations; however, their use was so selective that I am unable to make generalizations about their use based on our data. Of 11 patients experiencing perforation as a result of sphincterotomy, 7 were managed nonoperatively and 4 were managed operatively.

Dr Farnell: Indeed, there were patients who underwent sphincterotomy in spite of the presence of a peri-Vaterian diverticulum. Our experienced interventional endoscopists are willing to take on such patients for both diagnostic and therapeutic procedures selectively. In the majority of these patients, the procedures are performed safely. There were 14 patients in whom perforation occurred in the presence of a peri-Vaterian diverticulum. Seven were managed nonoperatively and 7 operatively. Of the 7 who were managed operatively, the perforation was at the site of the peri-Vaterian diverticulum in 5.
There were 7 patients in whom stent insertion resulted in perforation. Five were managed nonoperatively and 2 operatively. In none of the 7 patients were the stents of the expanding metal variety.
Roger G. Keith, MD, Saskatoon, Saskatchewan: As an ERCPist, I think one of the problems that we encounter, and I think it is debated and you have mentioned it, is the presence of peri-Vaterian diverticula. There are numbers of interventional endoscopists who don't consider that a contraindication to sphincterotomy, and there are those who do. I wondered if you had in your review any evidence of patients who you had to operate on who had been perforated through the diverticulum?

Clinical and radiographic features can be used to determine the surgical or conservative treatment of ERCP-related duodenal perforations, whereas patient age and intraoperative findings can determine the final outcome and morbidity or mortality..
The interval between the perforation and the operation is of great significance. The mortality rate increases dramatically with late surgical management (>24 h). The overall
mortality rate was 20%
CONCLUSIONS; Perforations during endoscopic retrograde cholangiopancreatography (ERCP) are rare, and the management of these perforations is variable, with some patients requiring immediate surgery,
33 patients with confirmed ERCP-related perforations,only 7(21%) patients required surgical intervention; and others(79%) only conservative management.
Review of all ERCP-related perforations at this institution to determine: a) their incidence; b) clinical outcomes; c) which management approaches gave the best results; and d) which factors predict a perforation (i) The incidence of ERCP-related perforations is very low (0.35 %).
(ii) Esophageal, gastric and duodenal perforations usually require surgery, but sphincterotomy- and guide wire-related perforations rarely do so. (iii) Factors which carry increased risk of an ERCP-related perforation include suspected sphincter of Oddi dysfunction, greater age, a dilated bile duct, sphincterotomy, and longer duration of the procedure
Sphincter of Oddi dysfunction and a dilated common bile duct. Sphincter of Oddi dysfunction has also been recognized as a risk factor in other reports [ 41,42] ,
however usually in conjunction with a small rather than a dilated common bile duct [ 41,42]
A possible explanation for this difference was that the dilated common bile duct in the Duke series [ 3] was accounted for by a distal common bile duct stricture, and the increased risk of perforation in this group was related to the manipulations carried out to obtain deep cannulation.

Eighteen patients (0.45%) out of 4030 ERCP performed were operated on for ERCP-related perforation at Singapore General Hospital.RESULTSThe group's median age was 72.5 years and 14 patients had ductal stone disease. Five perforations were discovered at ERCP while 10 required computed tomography for diagnosis. Eight patients were operated on within 24 h whereas 10 patients had surgery after 24 h. Five of six with type I (lateral duodenal) perforations had early surgery versus one of seven with type II (peri-Vaterian; P = 0.03). There were four type III (bile duct) perforations and one type IV (retroperitoneal air). Five of six patients with type I perforation had simple repair compared with five of seven type II requiring the complex duodenal diversion procedure (P = 0.10). Three patients (16.7%) succumbed after surgery due to sepsis and myocardial infarction. Advanced age>70 years resulted in higher mortality of 30% versus none in patients <70 years (P = 0.22).CONCLUSIONSEarly diagnosis is important but difficult especially for the type II perforations. Duodenal diversion is used more frequently in patients with type II perforations and those operated on late. Advanced age contributes to poorer outcome in surgical treatment of ERCP perforations

Abstract--Duodenal perforation during endoscopic retrograde cholangiopancreatography (ERCP) is a rare complication, but it has a relatively high mortality risk. Early diagnosis and prompt management are key factors for the successful treatment of ERCP-related perforation.
The management of perforation can initially be conservative in cases resulting from sphincterotomy or guide wire trauma. However, the current standard treatment for duodenal free wall perforation is surgical repair.
Recently, several case reports of endoscopic closure techniques using endoclips, endoloops, or fully covered metal stents have been described. We describe four cases of iatrogenic duodenal bulb or lateral wall perforation caused by the scope tip that occurred during ERCP in tertiary referral centers.
All the cases were simply managed by endoclips under transparent cap-assisted endoscopy. Based on the available evidence and our experience, endoscopic closure was a safe and feasible method even for duodenoscope-induced perforations. Our results suggest that endoscopists may be more willing to use this treatment.
CONCLUSION of study--Skill and synchronous assistance are important factors for success of ERCP but a more unpredictable outcome and complications were encountered for the preoperative undiagnosable obstructive jaundice.
Hot and slow sphincterotomy would minimize the bleeding complication.
Duodenal diverticulum and those operated on for late obstruction were risk factors in patients with EST perforations.
Pondering to be minimally by invasive, Advanced age still contributes to a higher complication and mortality risk in the surgical treatment of ERCP.
Although the management of perforation after ERCP/EST is still controversial,
a selective management is proposed, based on the features of classification type.
Nevertheless, duodenal and biliary drainage is essential in both surgical and conservative therapy.

Surgery — Overall, surgery was required in 20 to 40 percent of patients with a perforation in several reports [ 3,30,37-39,49 ] .
Endoscopic therapy — The effective and safe placement of metallic clips in the treatment of duodenal perforation secondary to sphincterotomy has been reported [ 54-56] ,
More experience is needed before this approach can be recommended as a first-line option
Whether or not the therapeutic goal of ERCP was achieved, a nasobiliary tube can be placed in an attempt to aspirate bile and minimize retroperitoneal contamination if a retroperitoneal perforation is recognized during the procedure, but not at the price of marked prolongation of the procedure.
Percutaneous transhepatic drainage — In difficult cases, percutaneous transhepatic drainage may be a safer alternative. ( See "Percutaneous
transhepatic cholangiography" ) A nasobiliary or transhepatic drain is preferred
since an internal biliary stent does not permit external drainage of bile.

In addition to the above, patients should be kept fasting while receiving hydration, nasogastric or nasoduodenal suction, and intravenous antibiotics.
Percutaneous drainage may be an alternative to surgical drainage in patients who develop retroperitoneal collections.
Patients who are expected to remain on bowel rest for at least one week should be placed on total parenteral nutrition .
Surgery should be recommended for patients with persistent biliary obstruction, cholangitis, and those whose symptoms do not improve after a brief period of nonoperative management [ 53] .
The type of surgical intervention depends upon the clinicopathological condition.
Options include choledochotomy with stone extraction and T-tube drainage, repair of the perforation, drainage of abscess or phlegmon, choledochojejunostomy, or pancreatoduodenectomy [ 53,57,58] .

The prognosis of patients with a perforation depends upon the rapidity with
which it was recognized, the clinical setting, and patient comorbidities.
The overall mortality was 16 percent in a report that summarized the outcome of 153 perforations following endoscopic sphincterotomy that were collectedfrom different sources about two decades ago [ 30]
Mortality was 1 out of 8 [38] , 1 out of 16 [39] , and 1 out of 13 [ 59] in the more recent series.
There was only one death in the retrospective series discussed above that included 3 various ERCP-related perforations recorded between 1987 and 1998 [ 3]
The lower mortality in recent years may reflect the benefits related to a conservative team approach to the management of small retroperitoneal perforations.

— Educational materials on this topic are
available. We encourage you to subscribe to
www.uptodate.com/professionals , which includes this and other topics.

Howard, TJ, Tan, T, Lehman, GA, et al. Classification and management of
perforations complicating endoscopic sphincterotomy. Surgery 1999;
1. 126:658. Stapfer, M, Selby, RR, Stain, SC, et al. Management of
duodenal perforation after endoscopic retrograde
cholangiopancreatography and sphincterotomy. Ann Surg 2000; 232:191. 2. Enns, R, Eloubeidi, MA, Mergener, K, et al. ERCP-related
perforations: Risk factors and management. Endoscopy 2002; 34:293. 3. Jayaprakash, B, Wright, R. Common bile duct perforation--an
unusual complication of ERCP [letter]. Gastrointest Endosc 1986;
32:246. 4. Lambiase, RE, Cronan, JJ, Ridlen, M. Perforation of the
common bile duct during endoscopic sphincterotomy: Recognition on computed tomography and successful percutaneous treatment.
Gastrointest Radiol 1989; 14:133. 5. Coelho, JC, Campos, AC, Pisani, JC, et al. Common hepatic duct perforation: A rare complication associated with ERCP [letter]. Gastrointest Endosc 1990; 36:427. 6. Martin, DF, Tweedle, DE. Retroperitoneal perforation during
ERCP and endoscopic sphincterotomy: Causes, clinical features and
management. Endoscopy 1990; 22:174. 7
Siragusa, G, Gelarda, E, Epifanio, E, et al. Video laparoscopy in
abdominal emergencies. Minerva Chir 1999; 54:199. 8. Freeman, ML. Adverse outcomes of ERCP. Gastrointest
Endosc 2002; 56:S273. 9. Wilkinson, ML, Engelman, JL, Hanson, PJ. Intestinal
perforation after ERCP in Billroth II partial gastrectomy [letter].
Gastrointest Endosc 1994; 40:389. 10. Lin, LF, Siauw, CP, Ho, KS, Tung, JC. ERCP in post-
Billroth II gastrectomy patients: Emphasis on technique. Am J Gastroenterol
1999; 94:144. 11. Feitoza, AB, Baron, TH. Endoscopy and ERCP in the
setting of previous upper GI tract surgery. Part I: reconstruction without
alteration of pancreaticobiliary anatomy. Gastrointest Endosc 2001;
54:743. 12. Stermer, E, Levy, N. Esophageal perforation during
ERCP [letter]. Gastrointest Endosc 1993; 39:603. 13. Fireman, Z, Kyzer, S, Michalevicz, D, et al. Esophageal
perforation after endoscopic sphincterotomy during stone extraction
from the common bile duct. J Clin Gastroenterol 1994; 19:173.

Ciaccia, D, Branch, MS, Baillie, J. Pneumomediastinum after endoscopic
sphincterotomy. Am J Gastroenterol 1995; 90:475. 15. Colemont, LJ, Pelckmans, PA, Moorkens, GH, Van Maercke, YM.
Unilateral periorbital emphysema: An unusual complication of
endoscopic papillotomy. Gastrointest Endosc 1988; 34:473. 16. Tam, F, Prindiville, T, Wolfe, B. Subcutaneous emphysema as a complication of endoscopic sphincterotomy of the ampulla of
Vater. 17. Gastrointest Endosc 1989; 35:447. Scarlett, PY, Falk, GL. The management of perforation of the
duodenum following endoscopic sphincterotomy: A proposal for selective
therapy. Aust N Z J Surg 1994; 64:843. 18. Doerr, RJ, Kulaylat, MN, Booth, FV, Corasanti, J. Barotrauma
complicating duodenal perforation during ERCP. Surg Endosc 1996; 10:349. 19. Savides, T, Sherman, S, Kadell, B, et al. Bilateral
pneumothoraces and subcutaneous emphysema after endoscopic sphincterotomy. Gastrointest Endosc 1993; 39:814. 20. Merine, D, Fishman, EK. Uncomplicated portal venous gas
associated with duodenal perforation following ERCP: CT features. J
Comput Assist Tomogr 1989; 13:138
Kuhlman, JE, Fishman, EK, Milligan, FD, Siegelman, SS. Complications of
endoscopic retrograde sphincterotomy: Computed tomographic
evaluation. Gastrointest Radiol 1989; 14:127. 22. Hans de Vries, J, Duijm, LE, Dekker, W, et al. CT before and
after ERCP: Detection of pancreatic pseudotumor, asymptomatic
retroperitoneal perforation, and duodenal diverticulum. Gastrointest Endosc
1997; 45:231. 23. Evrard, S, Mendoza, L, Mutter, D, et al. Massive gas spread
through a duodenal perforation after endoscopic sphincterotomy.
Gastrointest Endosc 1993; 39:817. 24. Genzlinger, JL, McPhee, MS, Fisher, JK, et al. Significance of retroperitoneal air after endoscopic retrograde cholangiopancreatography with sphincterotomy. Am J
Gastroenterol 1999; 94:1267. 25. Heer, M, Altorfer, J, Pirovino, M, et al. Pneumatosis cystoides
coli: A rare complication of colonoscopy. Endoscopy 1983; 15:119. 26. Meyers, MA, Ghahremani, GG, Clements, JL Jr, Goodman, K.
Pneumatosis intestinalis. Gastrointest Radiol 1977; 2:91. 27. Humar, A, Barron, PT, Sekar, AS, Lum, A. Pancreatitis and
duodenal perforation as complications of an endoscopically placed
biliary stent. Gastrointest Endosc 1994; 40:365.

Riahi S, Hansen J, Bjerre J, Kragsbjerg P. ERCP complicated by a
retroperitoneal abscess caused by Haemophilus influenzae and
Haemophilus parainfluenzae. Gastrointest Endosc 1998; 47:417.
29. Cotton, PB, Lehmann, G, Vennes, J, et al. Endoscopic
sphincterotomy complications and their management: An attempt at
consensus. Gastrointest Endosc 1991; 37:383. 30. Rabenstein, T, Schneider, HT, Hahn, EG, Ell, C. 25 years of
endoscopic sphincterotomy in Erlangen: Assessment of the experience in
3498 patients. Endoscopy 1998; 30:A194. 31. Pierie, JP, van Vroonhoven, TJ. [Obstructive cholangiopathy:
Are endoscopic retrograde cholangiopancreatography and
papillotomy always really necessary?]. Ned Tijdschr Geneeskd 1999;
143:1497. 32. Vandervoort, J, Soetikno, RM, Tham, TC, et al. Risk factors for complications after performance of ERCP. Gastrointest Endosc
2002; 56:652. 33. Andriulli, A, Loperfido, S, Napolitano, G, et al. Incidence rates
of post-ERCP complications: a systematic survey of prospective
studies. Am J Gastroenterol 2007; 102:1781. 34. Williams, EJ, Taylor, S, Fairclough, P, et al. Risk factors for
complication following ERCP; results of a large-scale, prospective
multicenter study. Endoscopy 2007; 39:793.
Wang, P, Li, ZS, Liu, F, et al. Risk factors for ERCP-related complications:
a prospective multicenter study. Am J Gastroenterol 2009; 104:31.
36. Fatima, J, Baron, TH, Topazian, MD, et al. Pancreaticobiliary
and duodenal perforations after periampullary endoscopic
procedures: diagnosis and management. Arch Surg 2007; 142:448. 37. Freeman, ML, Nelson, DB, Sherman, S, et al. Complications of endoscopic biliary sphincterotomy. N Engl J Med 1996;
335:909. 38. Loperfido, S, Angelini, G, Benedetti, G, et al. Major early
complications from diagnostic and therapeutic ERCP: A prospective
multicenter study. Gastrointest Endosc 1998; 48:1. 39. Kayhan, B, Akdogan, M, Sahin, B. ERCP subsequent to
retroperitoneal perforation caused by endoscopic sphincterotomy.
Gastrointest Endosc 2004; 60:833. 40. Sherman, S, Ruffolo, TA, Hawes, RH, Lehman, GA.
Complications of endoscopic sphincterotomy: A prospective series with
emphasis on the increased risk associated with Sphincter of Oddi dysfunction
and nondilated bile ducts. Gastroenterology 1991; 101:1068. 41. Chen, YK, Foliente, RL, Santoro, MJ, et al. Endoscopic sphincterotomy-induced pancreatitis: Increased risk associated
with non dilated bile ducts and sphincter of Oddi dysfunction. Am J Gastroenterol 1994; 89:327

Faylona JM, Qadir A, Chan AC, Lau JY, Chung SC. Small-bowel
perforations related to endoscopic retrograde cholangiopancreatography (ERCP) in patients with
Billroth II gastrectomy. Endoscopy 1999; 31:546. 43. Kim, MH, Lee, SK, Lee, MH, et al. Endoscopic
retrograde cholangiopancreatography in patients with Billroth
II gastrectromy: A comparative study of the forward-viewing
endoscope and the side-viewing duodenoscope. Endoscopy 1997; 29:82. 44. 45. Cotton, PB, Williams, C. Technique of biliary
sphincterotomy. In: Practical Gastrointestinal Endoscopy, Fourth edition,
Blackwell Science Ltd, Oxford 1996. p.142. Boender, J, Nix, GA, de Ridder, MA, et al. Endoscopic
papillotomy for common bile duct stones: Factors influencing the
complication rate. Endoscopy 1994; 26:209. 46. Trap, R, Adamsen, S, Hart-Hansen, O, Henriksen, M.
Severe and fatal complications after diagnostic and therapeutic
ERCP: A prospective series of claims to insurance covering public
hospitals. Endoscopy 1999; 31:125. 47. Kaw, M, Kaw, P. Complications of diagnostic and
therapeutic ERCP (abstract). Gastrointest Endosc 2000; 51:AB70
48
Masci, E, Toti, G, Mariani, A, et al. Complications of diagnostic and
therapeutic ERCP: A prospective multicenter study. Am J Gastroenterol
2001; 96:417. 49. Guitron-Cantu, A, Adalid-Martinez, R, Gutierrez-
Bermudez, JA. [Conservative management of duodenal perforation
following endoscopic sphincterotomy of papilla of Vater]. Rev
Gastroenterol Mex 2003; 68:6. 50. Preetha, M, Chung, YF, Chan, WH, et al. Surgical
management of endoscopic retrograde cholangiopancreatography-
related perforations. ANZ J Surg 2003; 73:1011. 51. Chaudhary, A, Aranya, RC. Surgery in perforation
after endoscopic sphincterotomy: Sooner, later or not at all?. Ann R
Coll Surg Engl 1996; 78:206. 52. Chung, RS, Sivak, MV, Ferguson, DR. Surgical
decisions in the management of duodenal perforation complicating
endoscopic sphincterotomy. Am J Surg 1993; 165:700. 53. Baron, TH, Gostout, CJ, Herman, L. Hemoclip repair
of a sphincterotomy-induced duodenal perforation.
Gastrointest Endosc 2000; 52:566.

Masci, E, Toti, G, Mariani, A, et al. Complications of diagnostic and
therapeutic ERCP: A prospective multicenter study. Am J Gastroenterol
2001; 96:417. 49. Guitron-Cantu, A, Adalid-Martinez, R, Gutierrez-Bermudez,
JA. [Conservative management of duodenal perforation
following endoscopic sphincterotomy of papilla of Vater]. Rev
Gastroenterol Mex 2003; 68:6. 50. Preetha, M, Chung, YF, Chan, WH, et al. Surgical
management of endoscopic retrograde cholangiopancreatography-related
perforations. ANZ J Surg 2003; 73:1011. 51. Chaudhary, A, Aranya, RC. Surgery in perforation after
endoscopic sphincterotomy: Sooner, later or not at all?. Ann R Coll
Surg Engl 1996; 78:206. 52. Chung, RS, Sivak, MV, Ferguson, DR. Surgical decisions in
the management of duodenal perforation complicating
endoscopic sphincterotomy. Am J Surg 1993; 165:700. 53. Baron, TH, Gostout, CJ, Herman, L. Hemoclip repair of a sphincterotomy-induced duodenal perforation. Gastrointest
Endosc 2000; 52:566.
Thank u– njust bfor students