postpartal pueperal infection
TRANSCRIPT

POSTPARTAL PUEPERAL INFECTION
Irish Jane B. CubilloIII BSN-1

The postpartum period is a time of increased physiologic stress and major psychological transition. Energy depletion and fatigue of late pregnancy and labor, soft-tissue trauma from delivery, and blood loss increase the woman’s vulnerability to complications.

The potential seriousness of many postpartum complications; associated pain, procedures and medications; frequent need to be isolated or separated from the newborn; emotionally disruptive effects of the physiologic malfunction can interfere with the maternal-newborn bonding process.

Postpartum Puerperal Infection
Postpartum infections of the genital tract associated with childbirth; usually are the result of bacteria ascending from the genital tract.
Often remain localized, but they extend along vascular or lymphatic pathways to produce extensive pelvic and systemic infections.
One of the most common causes of morbidity in the postpartum period.
The course of the illness varies according to: the size of the bacterial inoculum
virulence of the organism
the pelvic tissues affected
the host’s defense mechanisms including general health and immunologic status

Fever: principal sign
Etiology Idiopathic
Risk factors: Related to general infection risk Related to labor events Related to operative risk factors

Related to general infection risk- Anemia
- Nutritional deficiencies
- Lack of prenatal care
- Obesity
- Low socioeconomic status
- Sexual intercourse after rupture of membranes
- Immunosuppression

Related to labor events - Prolonged labor
- Prolonged rupture of membranes
- Chorioamionitis
- Greater number of vaginal examinations
- Hemorrhage

Related to operative risk factors- Cesarean delivery
- General anesthesia
- Urgency of operation
- Breaks in operative techniques
- Manual placental removal
- Forceps delivery
- Episiotomy
- Lacerations

Causative agents:
Anaerobic (not requiring oxygen for growth): gram negative bacilli- Bacteroides species
Aerobic (requiring oxygen for growth): most common; gram positive cocci- Streptococcus species
Nursing Assessment Focuses on early identification of signs
and symptoms; Monitor progress and physiologic function
including uterine involution Note needs for comfort and education Identify emotional reactions and needs Vital Signs

Assess: Condition of the perineum and uterus
Character of lochiaCondition of extremities and breastsStatus of bladderBowel function

Nursing Intervention Prompt diagnosis and treatment of the
postpartum infection to minimize serious sequelae and reduce their effects on the client’s ability to function are essential.
Antibiotic Therapy Specimen collection Wound debridement or cleansing Analgesic administration and monitoring
Comfort measures for pain relief Health teaching about the infectious
process
Prevention of InfectionAvoid possible sources of infection
Careful hand washingStandard precautions

Endometritis A localized infection of the inner uterine
wall Begins at the placental site and may spread
to involve the entire endometrium Bacteria gain access to the uterus through
the vagina and enter the uterus either at the time of birth or during the post partal period

Following vaginal delivery, about 2%-3% develop endometritis
may occur with any birth, but the infection is usually associated with chorioamnionitis and cesarean birth

Clinical Manifestations
benign temperature elevation (first post partal day)
increase in white blood cells increase in oral temperature to more than
38° C for two consecutive 24-hour periods Chills loss of appetite

Clinical Manifestations
general malaise uterus not well contracted and painful to touch lochia is dark brown and has foul odor if the infection is accompanied by high fever,
lochia may be scant or absent if the infection is caused by hemolytic
Streptococcus, the lochia usually is odorless
Diagnostic Procedures
Ultrasound: to confirm the presence of placental fragments that are a possible cause of the infection
Lochia culture Hysterosalpingogram

Nursing Management
Emotional support Fowler’s position or walking: promote
lochial drainage Hand washing technique Monitor:
progress of uterine involution fundal height and firmness
tenderness characteristics of lochia
Increased fluid intake(3L-4L/day) Well-balanced diet Advise mother to avoid breast-
feeding if necessary

Treatment
Antibiotics: Clindamycin (Cleocin) Metronidazole Gentamicin Aztreonam Aminoglycoside
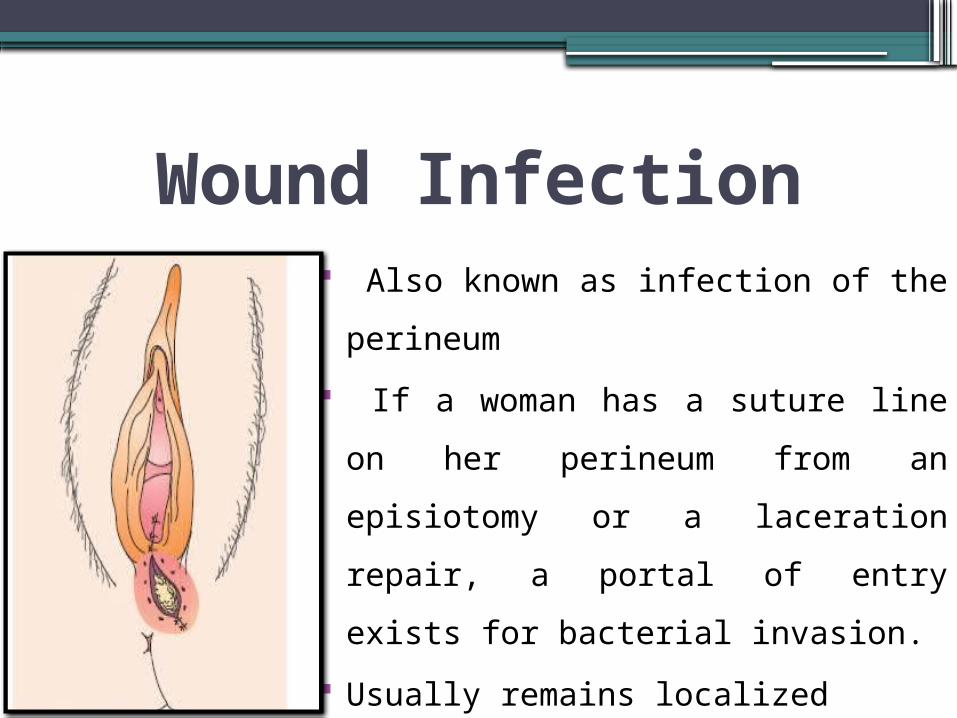
Wound Infection Also known as infection of the
perineum If a woman has a suture line on
her perineum from an episiotomy or a laceration repair, a portal of entry exists for bacterial invasion.
Usually remains localized

Clinical Manifestations Pain Heat Feeling of pressure May or may not have elevated temperature Inflammation on the suture line Suture line may be open with
presence of purulent discharge

Diagnostic Procedures
Culture of the discharge using a sterile cotton-tipped applicator

Nursing Intervention
Nurse-midwife may remove the perineal suture to allow drainage
Packing, such as iodoform gauze may be placed in the open lesion
Systemic or topical antibiotics Analgesics to alleviate discomfort Sitz bath

Moist warm compress Hubbard tank treatment Remind patient to change perineal pad
frequently Wipe front to back after bowel movement
Urinary Tract Infection
A woman who is catheterized at the time of childbirth or during the postpartal period is prone to development of a urinary tract infection, because bacteria may be introduced into the bladder at the time of catheterization

Physiologic urinary stasis, dilatation of the ureters and vesicoureteral reflux that occur during pregnancy persist for several months after delivery
Occurs 5% of postpartum client and are usually caused by coliform bacteria (E. coli, enterococci, Klebsiella pneumonia)

Postpartum urinary retention and incomplete emptying of the bladder are common because of increased bladder capacity, decreased tone and decreased perception of the urge to void caused by perineal trauma.

If client is unable to empty the bladder fully, the remaining urine is a culture medium for the bacterial growth, often leading to cystitis (inflammation of the bladder) or pyelonephritis (inflammation of the renal pelvis).
Risk factors Cesarean birth Use of forceps or vacuum extraction Epidural anesthesia And catheterization during labor

Clinical Manifestations
Burning on urination Blood in the urine (hematuria) Feeling of frequency in urinating Sharp pain on urinating Low grade fever Lower abdominal pain

Diagnostic Procedures
Physical examination
Urinalysis: Obtain a clean-catch urine specimen; examine the following: Leukocytosis Red blood cells Bacteria

Nursing Interventions
Encourage a woman: to drink large amounts of fluid to perform proper perineal care to use of cotton underclothing to void frequently to void before and after the
intercourse

Broad -spectrum antibiotic Amoxicillin Ampicillin
Oral analgesic: to reduce
the pain of urination Acetaminophen (Tylenol)

References Maternal and Child Nursing by Adele
Pillitteri 6th Ed. (pg. 682~690)
Maternity Nursing family, Newborn and Women’s Health Care 8th Ed. (pg.1028~1041)

THANK YOU!