posture - ksu facultyfac.ksu.edu.sa/sites/default/files/kinesiology_lecture-10.pdf · posture and...
TRANSCRIPT

Posture
KinesiologyRHS 341
Lecture 10Dr. Einas Al-Eisa

Posture
• = body alignment
• = the relative arrangement of parts of the body
• Changes with the positions and movementsof the body throughout the day and throughout life

Good posture
• “the state of muscular and skeletal balance which protects the supporting structures of the body against injury and progressive deformity”
• “when the muscles function most efficiently”
(The American Orthopedic Association, 1946)

Factors affecting posture
• General health• Body build• Gender• Strength and endurance• Kinesthetic awareness• Personal habits• Demands of the work place• Social and cultural traditions

Posture description
• Static (rest) posture = posture in rest or without anticipated action (e.g., lying, sitting, standing)
• Dynamic posture = posture in action or in anticipation of action

Posture description
• Efficiency of motion is determined by:
The posture maintained in the trunk
Positioning of the vertebral segments(stresses imposed upon the spine)

The spine (vertebral column) has to meet 2 functions
Strength Mobility


Posture and life cycle
• Infants’ ability to assume and maintain upright posture is limited because their postural reaction still needs to be perfected
• Upright standing posture is inherently unstable because the body’s center of gravity is situated high above a relatively small base of support


Posture and life cycle
• Spinal curvature:– In the neonate: the whole spine is flexed
forming a “C” shaped curve (convex posteriorly) from the occiput to the sacrum
– When the infant begins to lift his head: the cervical curve reverses to become convex anteriorly
– As the toddler begins to sit and stand: the lumbar curve reverses like the cervical


Posture and life cycle
Once the standing position is achieved, the spine has four curves:
1. Cervical curvature: convex anteriorly (secondary) 2. Thoracic curvature: convex posteriorly (primary) 3. Lumbar curvature: convex anteriorly (secondary) 4. Sacral curvature: convex posteriorly (primary)

Posture and life cycle
• In old age:the shape of the spine tends to revert back to the “C” shaped curve
spinal flexibility is greatly reduced
in some elderly, the cervical curve may increase as they try to keep their eyes directed parallel to the floor, so that they can look ahead

The seven ages of man

Abnormal posture
• Lordosis = an increase in the anterior lumbar curve
• Kyphosis = an increase in the posterior thoracic curve
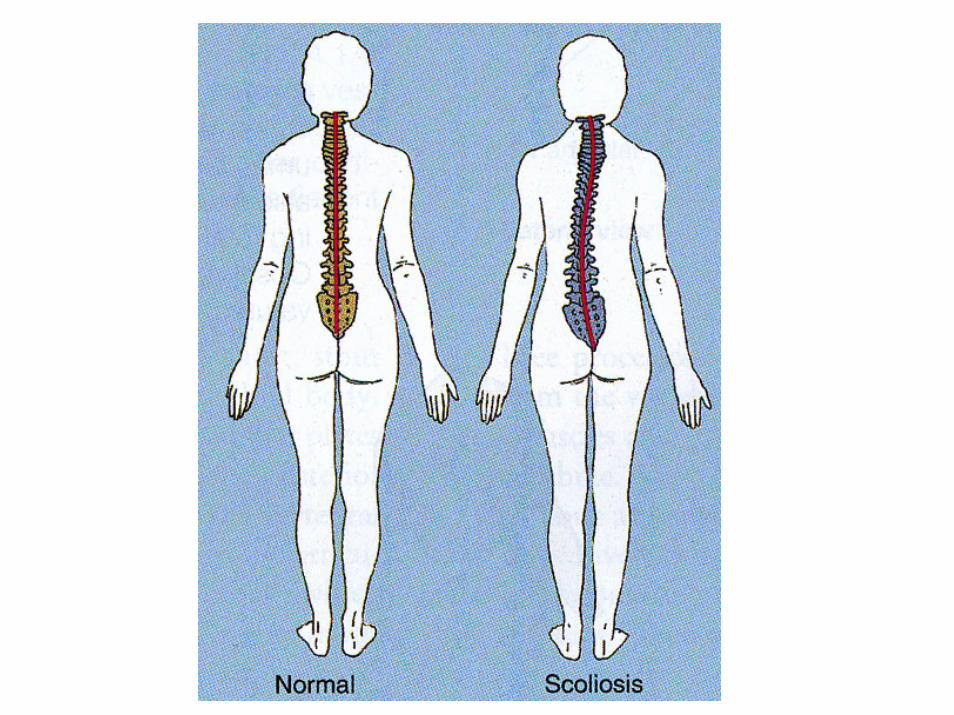
• Scoliosis = lateral curvature


Kyphosis

Abnormal posture
• High heels shoes throw the body weight forward, so the spine may adapt by increasing the lumbar curvature (lordosis)
• Scoliosis may affect the shape of the thorax, which may create problems in breathing

Abnormal posture
• Degenerative changes in the spine due to disease or aging may lead to permanent deformity

Standing posture
• To maintain upright standing posture, the “S” shaped spine acts as an elastic rod to support the weight

Standing posture
• Since the center of gravity lies in front of the spine
a continuous forward bending moment is imposed upon the trunk in standing
the posterior muscles and ligaments must control and maintain the standing posture

Standing posture
• Erect posture: activity in the erector spinae muscle (trunk extensors)
• Slouched posture: the ligaments and joint capsules take most of the responsibility for maintaining the posture

Postural sway
• Standing is not a static position: the upright position is maintained by the alternating action of various muscles to keep the body’s center of gravity over the base of support
• The magnitude of sway (as determined by the path of the body’s line of gravity) tends to be larger in the very old and very young

Postural sway
• Prevents fatigue (because of the alternating periods of activity and inactivity in the motor units)
• Assist venous return

Postural sway
• Affected by:
Vision
Ankle and foot proprioceptors

Standing posture
• Postural sway in standing is controlled by:The erector spinae musclesThe abdominal musclesThe psoas major
• All of these muscles are slightly active in standing, with more activity in the thoracic region than the lumbar and cervical regions……….why?

Standing posture
• The ideal standing posture is one in which the line of gravity runs:
Through the mastoid process Just in front of the shoulder jointJust behind the hip jointJust in front of the center of the knee jointIn front of the ankle joint

Line of gravity


Standing posture
• An ideal balanced posture reduces the work needed by the muscles to maintain the body in erect position

Standing posture
• Muscles active in standing:Soleus is continuously active because gravity tends to pull the body forward over the feetIliopsoas remains constantly activeGluteus medius and tensor fascia lata are active to counteract lateral postural swayErector spinae muscles are active to counteract gravity’s tendency to pull the trunk forward

Sitting posture
• Requires less energy expenditure and imposes less load on the lower limb than standing
• But, prolonged sitting can have negative effects on the lumbar spine

Sitting posture
• Unsupported sitting: high muscle activity in the thoracic region, with low levels of activity in the abdominals

Sitting posture
• Unsupported sitting places more load on the lumbar spine because it creates:
a backward pelvic tilt a flattening of the lower back forward shift in the center of gravity
places load on the discs and the posterior structures of the vertebral column (ligaments, capsules, muscles)

Sitting posture
• Supported sitting: the load on the lumbar vertebrae is less than unsupported sitting

Sitting posture
• Prolonged sitting in a flexed position may:
increase the resting length of the erector spinae muscles
overstretch the posterior ligamentousstructures

Sitting posture
• Ergonomic intervention:Raising the height of the work station (to reduce flexion of the cervical and lumbar regions)The use of foot rest (to relieve strain)Symmetrical working position (to reduce the incidence of twisting which stretches the posterolateral structures, particularly the annulus)
Lifting
• Lifting may result in a back injury as a result of:
the weight of the load
the distance of the load from the body

Identify the best lifting strategy and explain why?



Lifting
• Proper lifting posture is one in which: the back is erect knees are bentweight is close to the bodymovement occurs through one plane only (avoid twisting)

Lifting
• Stooped lifting posture reduces the activity in the trunk extensor
so the forward moment is resisted by passive structures (discs, ligaments, fascia)
placing these structures at risk of injury