practical considerations for assessing & progessing
TRANSCRIPT
PRACTICAL CONSIDERATIONS FOR
ASSESSING & PROGESSING
FUNCTION FOR WORK
ANGELA SUTHERLAND, LEAD PHYSIOTHERAPIST NHS GREATER GLASGOW
& CLYDE
PROPOSED LEARNING OUTCOMES
• To be able to identify simple and effective
functional tools that can be used in any
clinical setting
• To understand and interpret the results of the
functional measures
• To be able to use those results to inform our
practice to making suitable return to work and
activity recommendations
How do we assess fitness
for work?
• Subjective history - Relevant medical history, HPC
• Clinical Examination – S&S, diagnosis, prognosis
• Investigations – MRI, X-ray, etc
• Measuring impact on patient’s functional capacity
(FCE, questionnaires, etc)
• Psychosocial screening (yellow, orange, blue and
black flags)
• Analysis work activities / demands
• Ask
Functional tools
• Back Performance Scale
• Grip Strength
• Timed Sit to Stand Test
Back Performance Scale
• Developed to measure dynamic spinal mobility in
people with back problems
• Easy to administer in clinical setting
• Inter tester reliability high
• Intra tester reliability moderate to high
• Face validity
• Clinically significant change in BPS sum score of 4.5
• Score of below 6 was associated with those at work
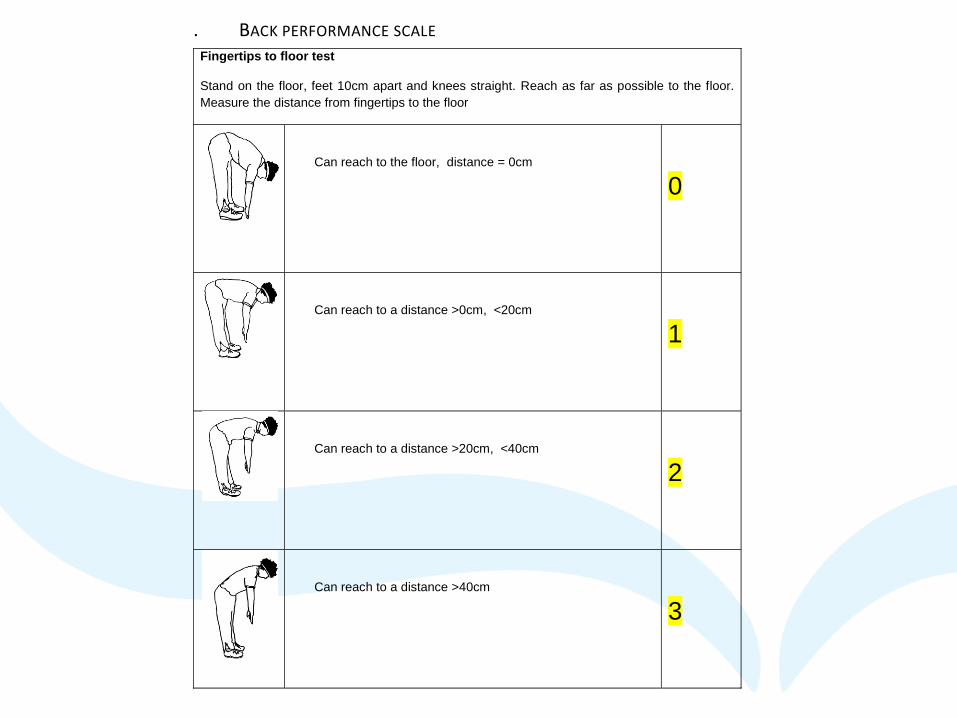
. BACK PERFORMANCE SCALE Fingertips to floor test
Stand on the floor, feet 10cm apart and knees straight. Reach as far as possible to the floor.
Measure the distance from fingertips to the floor
Can reach to the floor, distance = 0cm
0
Can reach to a distance >0cm, <20cm
1
Can reach to a distance >20cm, <40cm
2
Can reach to a distance >40cm
3
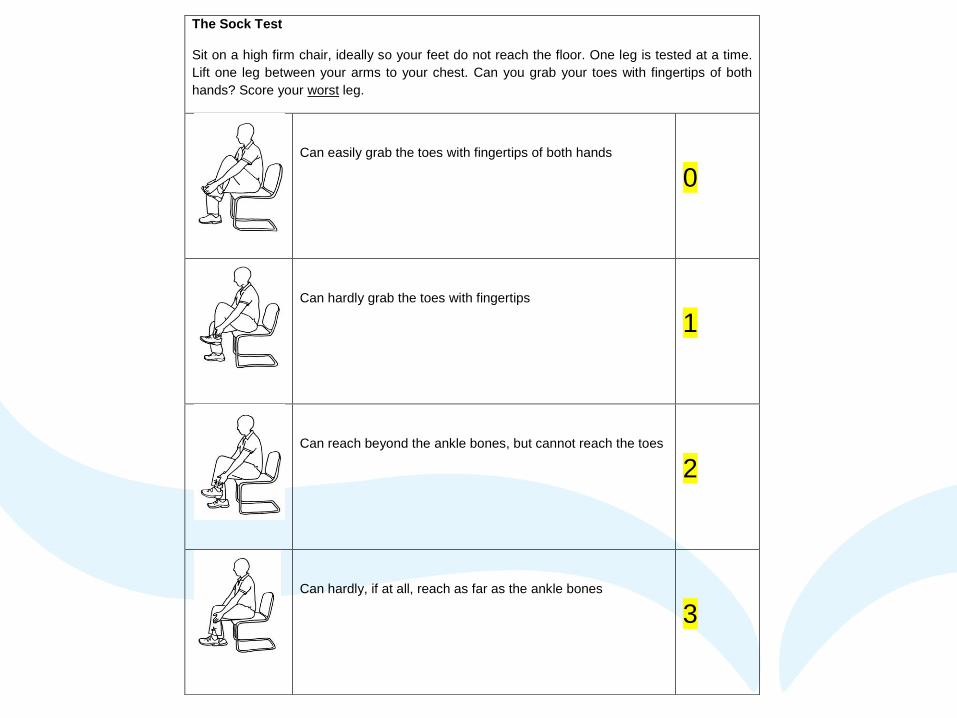
The Sock Test
Sit on a high firm chair, ideally so your feet do not reach the floor. One leg is tested at a time.
Lift one leg between your arms to your chest. Can you grab your toes with fingertips of both
hands? Score your worst leg.
Can easily grab the toes with fingertips of both hands
0
Can hardly grab the toes with fingertips
1
Can reach beyond the ankle bones, but cannot reach the toes
2
Can hardly, if at all, reach as far as the ankle bones
3
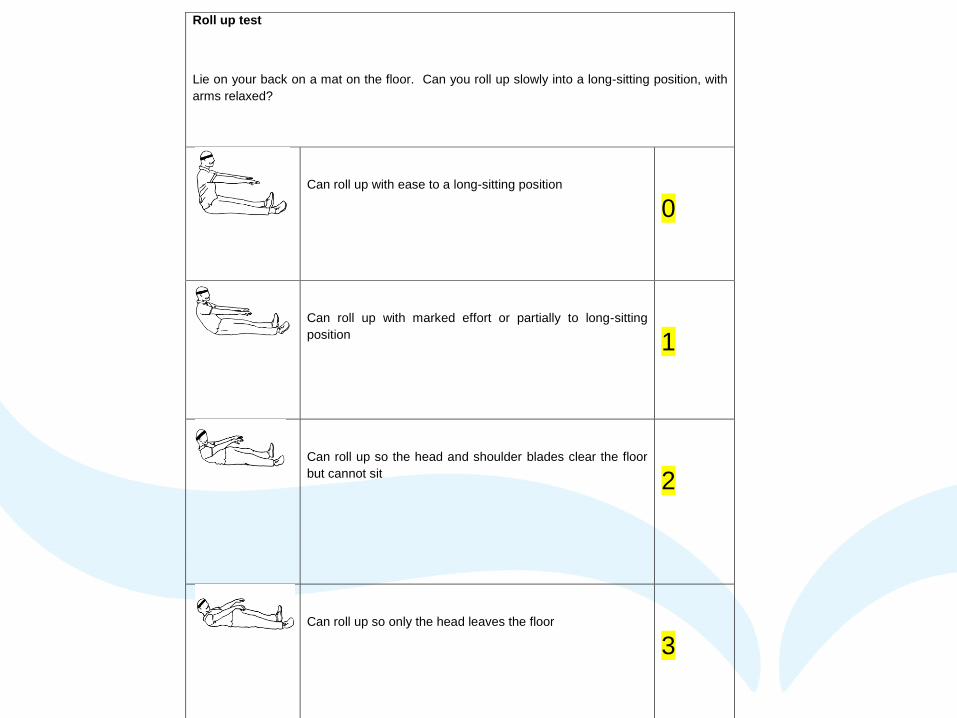
Roll up test
Lie on your back on a mat on the floor. Can you roll up slowly into a long-sitting position, with
arms relaxed?
Can roll up with ease to a long-sitting position
0
Can roll up with marked effort or partially to long-sitting
position
1
Can roll up so the head and shoulder blades clear the floor
but cannot sit
2
Can roll up so only the head leaves the floor
3
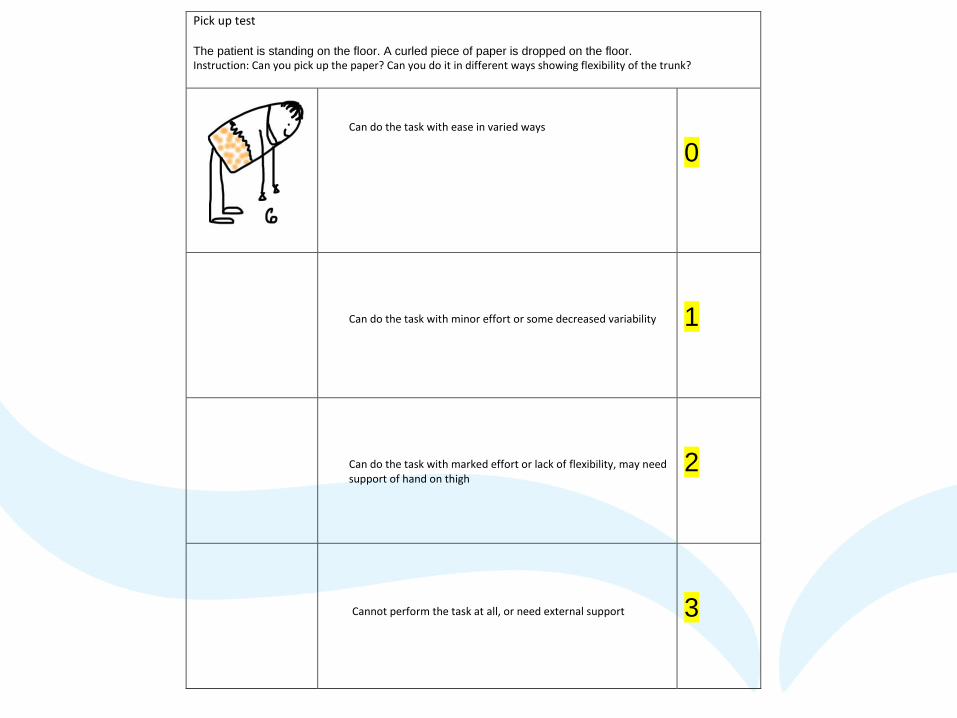
Pick up test
The patient is standing on the floor. A curled piece of paper is dropped on the floor.
Instruction: Can you pick up the paper? Can you do it in different ways showing flexibility of the trunk?
Can do the task with ease in varied ways
0
Can do the task with minor effort or some decreased variability
1
Can do the task with marked effort or lack of flexibility, may need support of hand on thigh
2
Cannot perform the task at all, or need external support
3
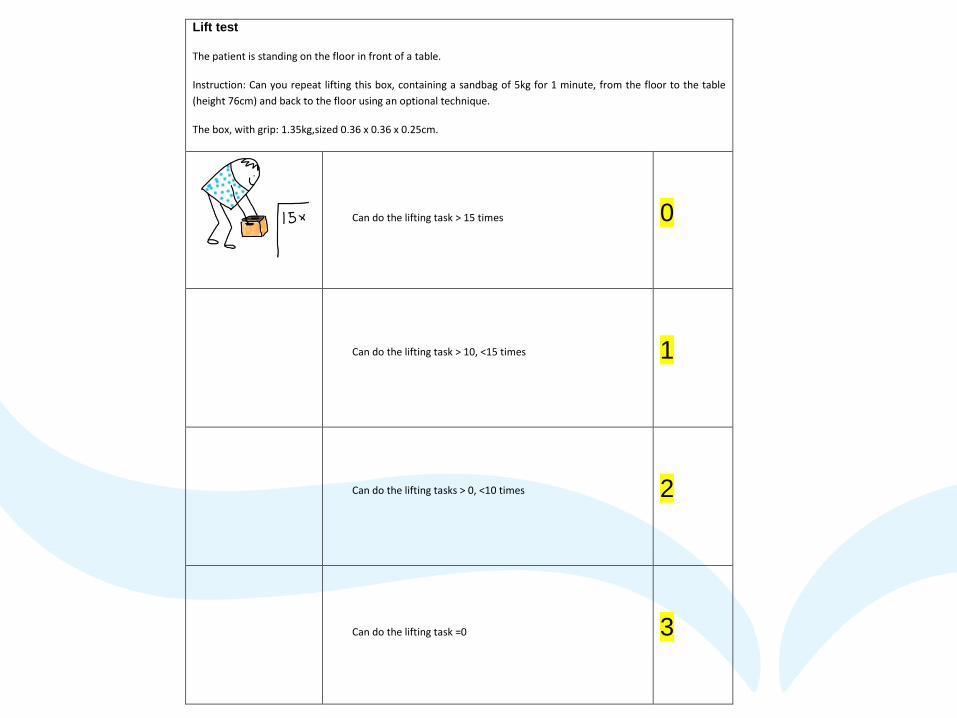
Lift test
The patient is standing on the floor in front of a table.
Instruction: Can you repeat lifting this box, containing a sandbag of 5kg for 1 minute, from the floor to the table
(height 76cm) and back to the floor using an optional technique.
The box, with grip: 1.35kg,sized 0.36 x 0.36 x 0.25cm.
Can do the lifting task > 15 times
0
Can do the lifting task > 10, <15 times
1
Can do the lifting tasks > 0, <10 times
2
Can do the lifting task =0
3
Hand Grip Strength
• Measure of Isometric Grip Strength
• In a seated position with shoulder
adducted and neutrally rotated, elbow
flexed 90 degrees & forearm & wrist in
neutral position.
• Average of 3 trials should be used
• Both hands should be tested
Timed Sit to Stand
• Simple test to identify lower extremity muscle
strength
• Time it takes to perform 10 sit to stands as
quickly as possible
• Not allowed to use upper limbs
• Score is time it takes patient to perform 10
stands to the nearest 10th of a second
• Time is then compared to the mean predicted
time in following table.
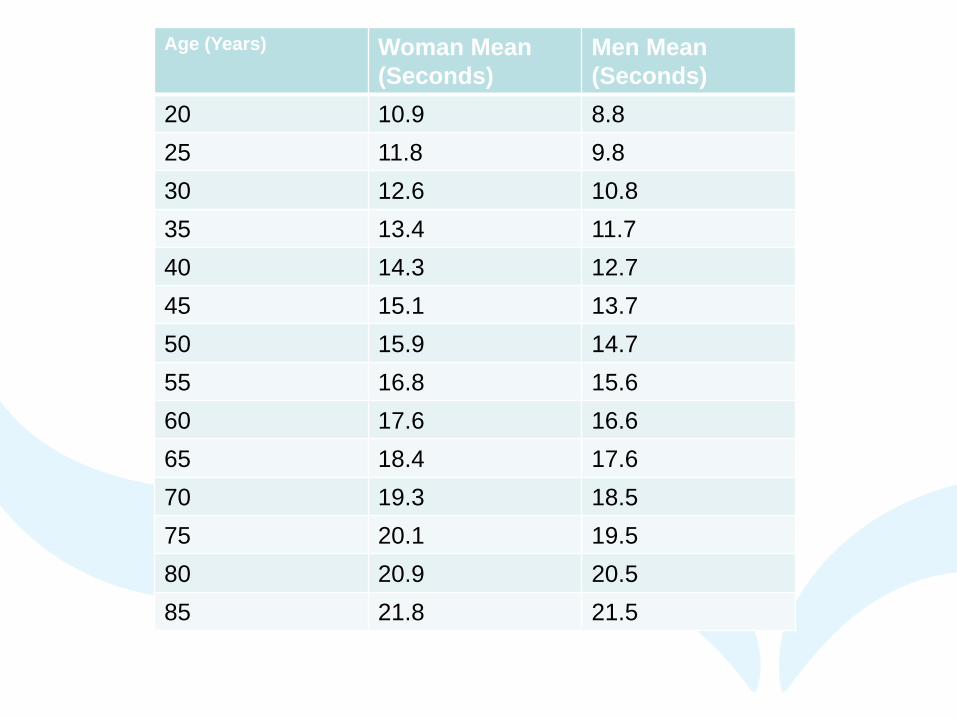
Age (Years) Woman Mean
(Seconds)
Men Mean
(Seconds)
20 10.9 8.8
25 11.8 9.8
30 12.6 10.8
35 13.4 11.7
40 14.3 12.7
45 15.1 13.7
50 15.9 14.7
55 16.8 15.6
60 17.6 16.6
65 18.4 17.6
70 19.3 18.5
75 20.1 19.5
80 20.9 20.5
85 21.8 21.5
Vocational Rehabilitation (VR)
• VR should be at the heart of our practice
• Rehabilitation should focus on work, home
and hobbies
• Treatment programmes should include
relevant functional work activities e.g.
pushing, pulling, lifting
• Return to Work/Remain in work should be a
goal in treatment planning and in outcome
measuring
Return to Work Planning
• Agree realistic goals and expectations of health care.
• Encourage incremental increase in activity levels.
• Agree clear goals and timeline for return to work.
• Discuss what patients can do rather than what they cannot do.
• Discuss how to overcome any obstacles to return to work, and think about communication with the employer but if possible encourage patient to speak to their employers directly.
• Talk about possible sources of support to help cope with the condition.
Benefits of ACPOHE
• Monthly e-newsletters
• ACPOHE Journal 3 times a year
• Advice for issues within field of OH & Ergonomics
• Access to Member Zone:
Guidance Documents
Resources to support CPD
ACPOHE annual pay & grading scales
Reduced rates for courses & conferences
Access to regional CPD groups
References
• Strand L, Moe Nilseen R, 2002 Back Performance Scale for the Assessment of Mobility- related activities in back painPhysical Therapy 2002 82 12 213 -223
• Magnussen et al, 2004 Reliability and Validity of the Back Performance Scale Observing Activity Limitations in Patients with Back Pain Spine V 29 No 8 903-907
• Rehab Measures : 30 second sit to stand test –http://www.rehabmeasures.org/Lists/RehabMeasures/DispForm.aspx?ID=1122
• Mathiowetz et al, 1985 Grip and Pinch Strength: Normative Data for Adults Arch Phys Med Rehabil 66: 69-72.