practical hematology diagnosing coagulopathy wendy blount, dvm
TRANSCRIPT

Practical HematologyDiagnosing Coagulopathy
Wendy Blount, DVM

Practical HematologyPractical Hematology
1. Determining the cause of anemia
2. Treating regenerative anemias– Blood loss– Hemolysis
3. Treating non-regenerative anemias
4. Blood & plasma transfusions in general practice
5. Determining the causing of coagulopathies
6. Treating coagulopathies in general practice
7. Finding the source of leukocytosis
8. Bone marrow sampling

Hemostasis
Primary hemostasis– Platelets plug up damaged blood
vessels• Von Willebrand Factor (vWF)
– Vasoconstriction
Secondary hemostasis– Platelet plug organized by fibrin– Fibrin generated by coagulation
cascade (factors)
Fibrinolysis

Coagulopathies
Poor Clotting– Not enough hemostasis– Problem with primary and/or
secondary hemostasis so that clots do not form and stabilize normally
Thromboembolic Disease– Too much hemostasis– Natural anticoagulants are
missing– Or Fibrinolytics are missing

Signs of Bleeding
Primary hemostasis – small vessel hemorrhage– Immediate bleeding– Petechiae (except vWDz) - <3 mm– Ecchymoses– Bleeding from surfaces
• Nose, mouth• Ocular - hyphema• GI – hematemesis, melena, hematochezia,
hematuria• repro
– Prolonged bleeding after injury or surgery

Signs of Bleeding
• Secondary hemostasis– Delayed bleeding after injury or surgery– Bleeding into cavities
• Joints, pleural space, abdomen• CNS• Muscular hematomas• Hemoptysis – can present as melena
– Blood coughed up, swallowed and digested
• Both primary and secondary– Epistaxis– Ecchymoses– If severe 1o and 2o bleeding types blend

Assessment of Coagulation
1. Is bleeding appropriate to injury?• Control arterial bleeding with
ligation
2. If not, assess coag status ASAP• Platelet count• PT, PTT/ACT• BMBT• FDPs, D-dimers• Factor assays

Coagulation Tests
Primary hemostasis• Platelet estimate
– Count platelets in 10 HPF (oil)– Divide by 10 to get average– Multiply by 15-20,000– 8-15 platelets/HPF is adequate
• Automated platelet count– Look at the feathered edge for
platelet clumping (cats!!)– If clumping, get a new sample– Use citrate (blue top) and count
immediately

Coagulation Tests
Primary hemostasis• MPV – Mean Platelet Volume
– Increased in dogs when immature platelets in circulation
– Indicates increased platelet pdxn• DIC, vasculitis, chronic hemorrhage
– Decreased with IMT - 50%
• Large, bizarre platelets– Otter hound thrombocytopathia– Cats with myeloproliferative
disease

Coagulation Tests
Primary hemostasis• Platelet function tests
– Academia– Must be performed within 2-3
hours of blood collection

Coagulation Tests
Primary hemostasis• Buccal mucosal Bleeding Time (BMBT)
– Assesses primary hemostasis– Prolonged if platelets <20,000/ul– Rebleeding can indicate problems with
secondary hemostasis– The only in clinic test that evaluates
vessel and platelet function– Screen for vWDz in likely suspects– Reasonable pre-operative estimate of
likelihood of surgical hemorrhage, if you check for rebleeding

Coagulation Tests
Primary hemostasis• How severe must Tpenia to cause
spontaneous bleeding?– Can happen <50,000/ul– More often <20,000/ul
• Splenomegaly of any kind can result in thrombocytopenia– Platelets sequestered in the
spleen, liver or lymph nodes

Coagulation Pathway

Coagulation Pathway

Coagulation Pathway

Coagulation Tests
Secondary hemostasis• Partial thromboplastin time (PTT)
– Intrinsic and common pathways– Heparin acts on intrinsic pathway
• Prothrombin time (PT)– Extrinsic and common pathways– PIVKA is a form of PT test– PIVKA is not specific for rodenticide toxicity
• Factor 7 deficiency• Common pathway - DIC, liver failure
• No clinical significance when PT/PTT are shorter than normal
• PT <3 sec and PTT <5 sec prolonged may not be clinically significant

Coagulation Tests
Secondary hemostasis• Activated clotting time (ACT)
– Less sensitive version of PTT• Intrinsic and common pathways•Platelets as well•Thrombocytopenia can elevate ACT
by <10%•No such platelet effect on PTT
– Factors must be 5% of normal for ACT to be elevated• If ACT is increased, things are really
bad
Coagulation Tests
Secondary hemostasis• Thrombin time (TT)
– Assesses fibrinogen activity•Part of common pathway
Coagulation Tests
Fibrinolysis• Fibrin degradation products (FDPs)
– AKA FSPs – fibrin split products– Measure fibrinolysis– High with clot formation and breakdown
over time• DIC• Chronic bleeding• Hypercoagulable state
– Neoplasia– Cushings Disease– PLN, PLE– IMHA

Coagulation Tests
Fibrinolysis• D-dimers
– Measure fibrinolysis– More specific for DIC than FDPs– Normal D-dimers exclude DIC as
a diagnosis with 99.5% confidence level

Anticoagulants
• Antithrombin III– Produced by the liver– Activated by heparin– Modulates excessive coagulation– Consumed by coagulation– Lost with albumin – PLN, PLE
• Protein C (vitamin K dependent)• Protein S (vitamin K dependent)• TFPI – Tissue Factor Pathway Inhibitor

Coagulation Pathway –THAT’S Not ALL!!

Fibrinolysis
• tPA – tissue Plasminogen activator converts plasminogen within the clot to plasmin
• Plasmin breaks down fibrin clot• So tPA promotes fibrinolysis, so that clots
are only temporary• Urokinase and streptokinase work
similarly• tPA, urokinase and streptokinase
are the “clot busters”

Excessive Fibrinolysis
• Enzymes prevent excessive fibrinolysis which would lead to rebleeding
• They break down the clot busters– Alpha2-antiplasmin
• inactivates plasmin– PA1-I: tPA-inhibitor1
• Inactivates tPA and uPA• uPA – urokinase plasminogen activator
• FDPs and d-Dimers inhibit the coagulation cascade by negative feedback

Coags in Practice
Why do them at all???– Patient shows signs of coagulopathy
• Excessive bleeding• thrombosis
– Presurgical evaluation• Patient predisposed to coagulopathy• Procedure increases risk of bleeding
– Rodenticide toxicity suspected– DIC suspected– Genetic screening for breeding– No expensive equipment for platelet
count, ACT, BMBT– Can send out the rest

Coags in Practice
Platelet count
Partial thromboplastin time (PTT)Prothrombin time (PT)
– Reference lab– Human hospitals often not calibrated for animals (Pluto)– Synbiotics SCA 2000
• $2000-3000– Idexx Coag Dx

Coags in Practice
Activated clotting time– Reference labs– Gray top tubes (other colors now)
• Diatomaceous earth (DE) or kaolin– http://www.haemtech.com/ACT.htm
• Warming block or hand heat• 2 ml whole blood in the tube immediately• Invert once every 15-30 seconds• First clot is the ACT• Normal less than 2 minutes
– SCA 2000– HESKA i-STAT

Coags in Practice

Coags in Practice

Coags in Practice
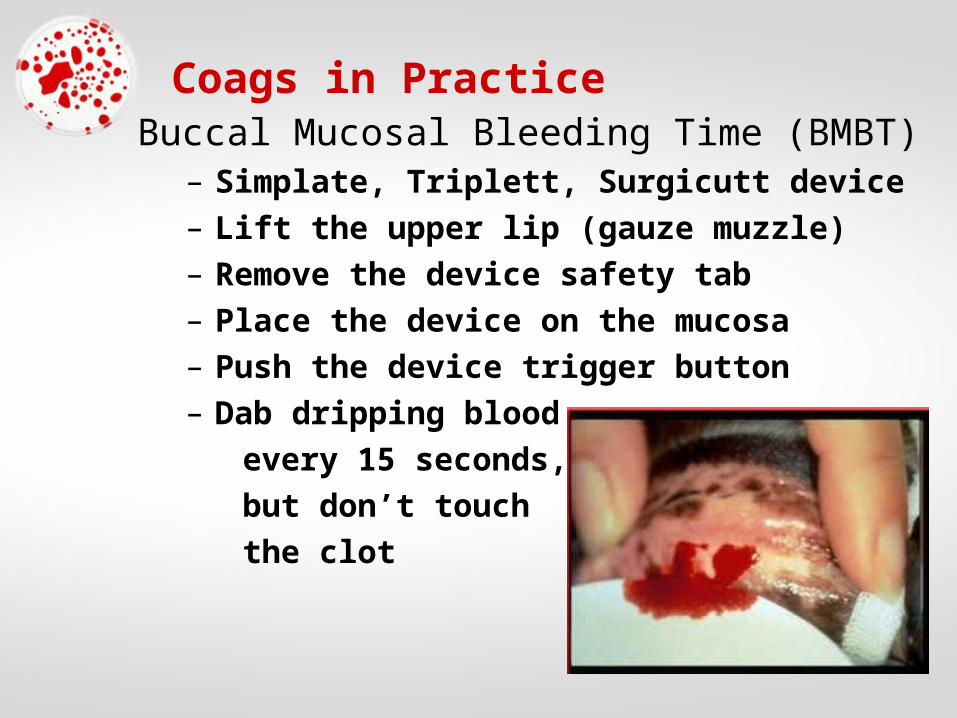
Coags in PracticeBuccal Mucosal Bleeding Time (BMBT)
– Simplate, Triplett, Surgicutt device– Lift the upper lip (gauze muzzle)– Remove the device safety tab– Place the device on the mucosa– Push the device trigger button– Dab dripping blood every 15 seconds, but don’t touch the clot

Coags in PracticeBuccal Mucosal Bleeding Time (BMBT)
– When bleeding stops, you have BMBT– Normal is 2-4 minutes– 5 minutes isn’t worrisome– Check the patient in 10-15 minutes for
rebleeding– DON’T DO BMBT IF:DON’T DO BMBT IF:
• Platelets <40,000/ulPlatelets <40,000/ul• Petechiae are presentPetechiae are present• ACT is increasedACT is increased

Coags in Practice
EVERY PRACTICE can have in house PLATELET COUNT, ACT & BMBT
EVERY PRACTICE can use a lab for the rest

Coags in Practice
Tips for coag test sample handling– Take blood from a peripheral vein– Avoid cystocentesis if coagulopathy– Holding the vein off for too long can
lead to platelet & fibrinolysis activation– Multiple sticks can lead to the same –
you want a clean first stick.– If you don’t get blood quickly, move to
another vein.– Hemolysis and severe lipemia can
prevent accurate results

Coags in Practice
Tips for coag test sample handling– 1 citrate:9 blood
• Vacuum tubes should autodraw– Run platelet count immediately– Run tests on whole citrated blood
within 2 hours– Centrifuge promptly to harvest plasma
for outside lab tests• Freeze immediately in plastic or siliconized
glass tubes• Ship frozen on dry ice
– May need special blue top clot tubes for FDPs – ask lab

Disorders of primary hemostasis– thrombocytopenia– thrombocytopathia– Von Willebrand Disease– vasculitis
Disorders of secondary hemostasis– Congenital factor deficiencies– Liver disease (poor pdxn)– Vitamin K antagonism– Snake bite envenomation
Disorders of both– Consumption – DIC, massive
hemorrhage– Paraneoplastic coagulopathy
Coagulopathies - DDx

Thrombocytopenia - DDx
• Bone marrow disease – lack of production• Consumption
– DIC– Massive hemorrhage
• Destruction– immune mediated
• Sequestration– Splenomegaly– Hepatomegaly– Lymphadenitis, lymphangitis– vasculitis

Thrombocytopenia - DDx
Infectious DiseasesMultiple causes• Viruses
– Canine – CDV, CHV, CPV, CAV2
– Feline – FeLV, FIV, panleukopenia, FIP
• Arthropod-Borne– Ehrlichia spp.– Babesia spp.– Heamobartonella
spp.
• Arthropod-Borne– Rickettsia spp.– Leishmania spp.– Cytauxzoon spp.– Borrelia spp.
• Bacterial– Sepsis– Borrelia spp.– Leptospira spp.
• Fungal– Histoplasma spp.– Candida spp.

Thrombocytopenia - DDx
NeoplasiaMultiple causes• Marrow suppression
– Metastatic disease– Hematopoietic
neoplasia• Lymphoma• Multiple myeloma• leukemias
• DIC– Hemangiosarcoma– Inflammatory
mammary carcinoma
• Vasculitis• Cytotoxic drug therapy
– Azathioprine– Chlorambucil– Cyclophosphamide– Doxorubicin

Thrombocytopenia - DDx
Drug TherapyMultiple causes• Impaired platelet pdxn • Immune destruction• Platelet dysfunction
Antibiotics• Penicillin• Chloramphenicol• Sulfonamides
Antifungals
NSAIDs• IbuprofenCardiopulmonary drugs• ProcainamideCytotoxic drugs• Azathioprine• Chlorambucil• Cyclophosphamide• DoxorubicinEstrogenMethimazole

Immune Mediated Thrombocytopenia
• Primary – autoimmune – Very rare in cats– Dog breeds predisposed
• Same as IMHA• Cocker spaniel• Poodle• Old English Sheepdog
– Diagnosis of exclusion• Rule out other causes of Tpenia (normal
coags, normal BMBT unless <5K platelets)• Rule out causes of secondary IMT• Platelets <50,000/ul• Increased megakaryocytes in the marrow• Response to immunosuppressive therapy

Immune Mediated Thrombocytopenia
• Secondary – same as for IMHA– infection– Drug therapy– Paraneoplastic– transfusion
• Anti-platelet antibodies– Doesn’t distinguish between 1o & 2o IMT– Sensitive for IMT– But not very specific (many false negatives)
• Low MPV – microthrombocytosis– MPV < 5.5 fL + platelets <20,000/ul is almost MPV < 5.5 fL + platelets <20,000/ul is almost
always IMT (primary or secondary)always IMT (primary or secondary)– But only 50% of dogs with IMT have this
combination of abnormalities

Breed Specific Thrombocytopenia
• Greyhounds– Normal platelet count 150,00/ul– Coags normal– Remember greyhounds also predisposed to
von Willebrand Disease and Babesia
• Cavalier King Charles Spaniel– Normal coags– Normal platelets 25,000/ul-100,000/ul– Giant platelets on blood smear
• CBC machines won’t count them– Platelet mass usually normal
• Platelet mass = Platelet count x MPV– Causes no clinical problems

Thrombocytopathia
• Platelet dysfunction– hereditary– acquired
• Acquired Thrombocytopathia– Drugs– Disease
• Anemia
• Liver failure (plus factor deficiency)
• Uremia (plus vasculitis)
• DIC (plus consumptive coagulopathy)
• Paraproteinemia– Monoclonal gammopathy– Ehrlichia, plasma cell myeloma

Thrombocytopathia - DDx
Drug TherapyAntibiotics• Beta lactams
– Carbenicillin– cephalosporins
AntifungalsNSAIDs• Aspirin• Phenylbutazone• Ibuprofen• Naproxen
Cardiopulmonary drugs• Aminophylline• Verapamil• Diltiazem• Isoproterenol• PropranololDextranPhenothiazines
CAUTION in pets with CAUTION in pets with thrombocytopenia, thrombocytopenia, undergoing surgery or undergoing surgery or signs of coagulopathysigns of coagulopathy

Thrombocytopathia
• Hereditary Thrombocytopathia– Likely underdiagnosed– Otter hound, Great Pyrenees – thrombasthenia– Basset hound, Spitz– Persian cat – Chediak-Higashi– Cocker spaniel– Collie – cyclic neutropenia (stem cell defect)– Boxer
– German shepherd– Consider BMBT prior to major surgery

von Willebrand DiseaseMost common canine hereditary coagulopathy in Most common canine hereditary coagulopathy in
dogsdogs• Does not occur in cats• Clinical signs of primary hemostasis defect
– Mucosal hemorrhage, prolonged bleeding after injury
– Petechiae are rare – (Indy)
• von Willebrand Factor is not a coagulation factor– Made by the endothelium– Acts as carrier protein for factor 8– Severe vWDz can cause result in bleeding due
to lack of secondary hemostasis

von Willebrand Disease
• Three subtypes of vWDz– Type 1 vWDz – most common – complex
genetics• Mild to moderate bleeding• Low plasma vWAg, normal multimer distribution
– Type 2 vWDz – simple recessive• Moderate to severe bleeding• Low vWAg, loss of high MW multimers
– Type 3 vWDz – simple recessive• Severe bleeding• Total lack of vWF
von Willebrand Disease• Diagnosis
– Platelet count• Normal (may be mildly low if hypothyroid)
– PT, PTT/ACT• Normal (increased of Type 3)
– BMBT• Type 1: 5-12 minutes• Type 2&3: >12 minutes
– vWFAg assay• carriers: 35-65%• Type 1: 5-30% (clinical <15%)• Type 2: 1-5%, no high MW multimers• Type 3: <0.1%

von Willebrand Disease
Type 1 - mild
Airedale
Akita
Dachshund
Doberman
German shepherd
Golden retriever
Greyhound
Irish wolfhound
Manchester terrier
Pembroke Corgi
Poodle
Schnauzer
Sheltie
Type 2 - moderateGerman shorthair
pointerGerman wirehair
pointer
Type 3 - severeChesapeake Bay
RetrieverDutch kooikerScottish terrierSheltie
Less commonly:Cocker spanielSpitzLabrador retrieverPit bull terrierRottweiler
DNA Tests available for some breeds

Vasculitis – Clinical Signs
• Peripheral edema (dependent)• Proteinuria• Exudative skin lesions• Ascites, pleural/pericardial effusion• Necrosis of extremities
– Nose– Ear tips– Nail beds & toes– Tail tip
• hypoalbuminemia

Vasculitis - DDx• Systemic inflammation
– Infection• Bacterial – sepsis, Lepto, endocarditis,
pyelonephritis, pyometra, prostatitis, abscess• Viral - FIP• Fungal – systemic infection• Parasitic – heartworm Dz, rickettsiae
– Immune mediated• Primary – autoimmune• neoplasia
– Uremia
• Infection of the blood vessels– Rocky Mountain Spotted Fever– Ehrlichia spp.

Vasculitis – Work-Up• CBC, panel, lytes, UA
– Urine P:C ratio if proteinuria on dipstick– Urine culture if dilute urine– Anti-platelet-Ab if platelets <50,000/ul
• FeLV/FIV in cats, HWAg in dogs• Chest x-rays
– Echo if murmur– Blood culture if endocarditis
• Abdominal x-rays and/or ultrasound• Tick panel - RMSF, Ehrlichia, Borrelia• ANA• Definitive diagnosis of elusive vasculitis Definitive diagnosis of elusive vasculitis
is by skin biopsyis by skin biopsy

Vasculitis – Coags
• Platelet count– <150,000/ul– May see E platys in platelets, or morulae
from other species in WBC
• PT, PTT/ACT– Normal– ACT may be <10% prolonged if
thrombocytopenia
• BMBT– Prolonged

Thrombocytosis
• Falsely increased platelets– Lipid droplets in lipemic animals– Small RBC – iron deficiency anemia– Schistocytes
• IMHA• DIC• RBC fragility – congenital, liver disease• Zinc toxicity• Iron deficiency anemia• Microangiopathy
– Sharp spikes on the platelet histogram and Sharp spikes on the platelet histogram and low MPV make you suspect thislow MPV make you suspect this
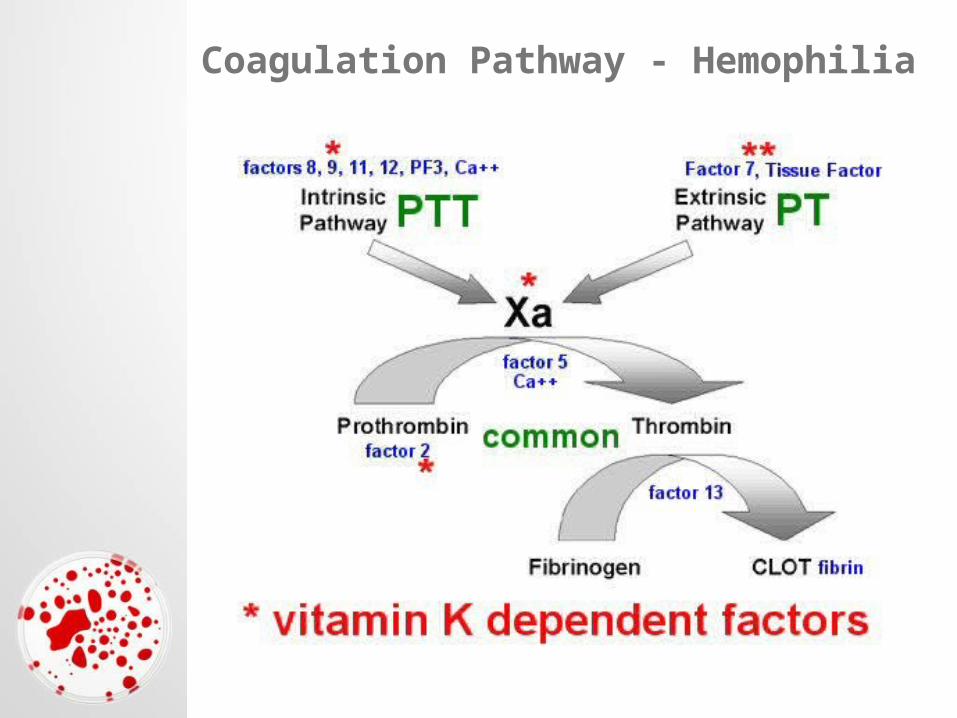
Coagulation Pathway - Hemophilia

Hemophilia
• See the chart • Hemophilia A (Factor 8) and B (factor 9) are
sex linked recessives– Most affected individuals are male
• Factor must be <5% for spontaneous bleeding
• Secondary hemostatic defects– Delayed bleeding, into cavities
• Often evident at a very young age– Bleeding out from umbilicus
• Almost always evident prior to 2-3 years
Hemophilia• Factor 7 deficiency
– increased PT and normal PTT
• Factor 10 deficiency – increased PT and PTT
• Most of the rest increased PTT and normal PT– Factor 11 and 12 (Hageman) deficiencies rarely cause
clinical bleeding
• There is a deficiency of all vitamin K dependent factors in the Devon Rex– 2, 7, 9, 10– Causes severe bleeding– Increased PT and PTT– Long term vitamin K Tx can normalize
• Cockers and Kerry Blues can have prothrombin deficiency– Common pathway – increased PT, PTT/ACT, TT

Hemophilia
• Factor assays are diagnostic (Cornell)– http://ahdc.vet.cornell.edu/coag/test/– Coag panels – individual tests – Submission form
• DNA Tests are available fro some defects in some breeds– www.vetgen.com– www.dog-dna.com– www.healthgene.com– www.optigen.com

Hemophilia

Vitamin K Antagonism

Vitamin K Antagonism
• Vitamin K1 found in green leafy vegetables– phytonadione
• Vitamin K3 is found in drugs– menadione
• Causes of Vitamin K deficiency– Neonate born to malnourished mother– Severe bacterial deficiency in ileum– Decreased vitamin K absorption
• Bile duct obstruction• Exocrine pancreatic insufficiency• Lymphangiectasia
– Rodenticide toxicity is by far most commonRodenticide toxicity is by far most common

Vitamin K Antagonism
• Disorder of secondary hemostasis– Delayed bleeding, into cavities– Signs begin 2-5 days after ingestion

Vitamin K Antagonism• Diagnosis
– platelets• Decreased if prolonged bleeding• Usually ingested at least 3-4 days before
– PT elevated first for 12 hours or less• Some say PIVKA elevated before PT• PIVKA = procoagulant Proteins Induced by
Vitamin K Antagonism – then PTT within 12-24 hours, then ACT– FDPs and d-Dimers could be elevated with
chronic bleeding– TT should be normal– Send anticoagulant toxicology screen out– Vitamin K therapy will not affect results

Vitamin K Antagonism
1st GenerationCoumadin
Warfarin
Pindone
Shorter half life
2nd GenerationBromadioloneBrodifacoumDiphacinone
Longer half lifeLower incidence of
drug resistance
3rd GenerationOthers
Longest half life

Heparin Toxicity
• Causes– Iatrogenic– Mast cell tumor degranulation
• Heparin prolongs PTT > PT• Monitor PTT for heparin therapy for
thromboembolic disease• INR is an even better monitor for coumadin
therapy– International Normalization ratio

Liver Failure• Define liver failure
– Significantly elevated bile acids– Can’t be explained by prehepatic or posthepatic
icterus• Prehepatic icterus (hemolysis)• Posthepatic icterus (biliary obstruction)
• More than half of liver failure patients have at least one abnormal coag test
• Only 2% of liver patients develop hemorrhage• Concurrent coagulopathies
– Biliary obstruction can cause vit K deficiency– DIC
• Disorder of secondary hemostasis

Liver Failure
• Diagnosis of coagulopathy due to liver failure– Blood film
• Acanthocytes• Target cells = leptocytes = codocytes

Liver Failure
• Diagnosis of coagulopathy due to liver failure– Blood film
• Acanthocytes• Target cells = leptocytes = codocytes
– Factor Assays• Some say PIVKA most sensitive indicator for
risk of hemorrhage due to liver failure’• PT and PTT elevated• ACT elevated if severe
– BMBT• Normal, then rebleeding if severe
– AT3, TT• AT3 low, TT prolonged

Paraneoplastic Coagulopathy• Thrombosis
– Iatrogenic– Mast cell tumor degranulation
• Hemorrhage– Thrombocytopenia
• inflammatory activation of platelets• Microangiopathy• Secondary IMT• Chemotherapy induced bone marrow
suppression– Thrombocytopathia– DIC – HAS and inflammatory MGC– Disruption of blood vessels by tumor invasion

Paraneoplastic Coagulopathy
• 2/3 of dogs with MGT have at least one abnormal coag test
• Dogs with stage III or IV cancer are more likely to have coagulopathy
• 83% of dogs taking chemo have at least one abnormal coag test
• Only 20% of cats with neoplasia have coaguloapthy
• LSA and HSA are commonly associated with coagulopathy.

Chemo Drugs Affecting Coagulation
Marrow Suppression• CCNU• doxorubicin• Bleomycin• Cytosine arabinoside• Melphalan• Methotrexate• Cisplatin, carboplatin• Actinomycin DThrombocytosis• Vincristine, vinblastine
Thrombocytopathia• Melphalan• vincristineFactor Pdxn Suppression• L-asparaginaseVitamin K Antagonism• Actinomycin DDysfibrinogenemia• MelphalanIncreased fibrin• Doxorubicin• Daunorubicin

Snake Bite Coagulopathy• Cause
– Toxins in the snake venom affect coagulation in many ways
– The most common affect is lack of fibrin– Lack of secondary hemostasis, though bleeding is
rare
• The Mojave rattler causes no coagulopathy• Diagnosis
– Locate the snake bite injury– Decreased platelets– Prolonged PTT, PTT, ACT– Low fibrinogen– Elevated FDPs– d-dimers often normald-dimers often normal
• True DIC can occur if toxicity is severe

Thrombocytosis
• > 800,000-900,000/ul platelets• DDx
– Chronic blood loss– Paraneoplastic– Systemic inflammation– Primary bone marrow disease– Cushing’s Disease– Post-splenectomy
• Work-up (after CBC, panel, UA):– Endoscopy, chest x-rays, abdominal US,
abdominal x-rays, fecal cytology

Thrombosis
• Hypercoagulable states– IMHA
• 80% of dogs who died of IMHA had evidence of thromboembolic disease on necropsy
– Hyperadrenocorticism
– Protein losing enteropathy and nephropathy• AT3 is similar size as albumin• AT3 level is a good assessment for risk of thrombosis
– AT3 60-75% at risk)– AT3 <60% - grave prognosis
– Systemic amyloidosis
– Canine parvovirus
– Neoplasia – 30% have PTE

Thrombosis
• Symptoms of Thromboembolism– Caused by ischemia of the organ affected– PTE – pulmonary thromboembolism
• Acute dyspnea– Renal artery
• Acute renal failure– Jugular vein
• Swelling of the head
• Diagnosis– Doppler ultrasound– Angiography, venography– Nuclear scans

Disseminated Intravascular Coagulopathy (DIC)
• End result of systemic thrombosis• Rarely recognized in cats• Always secondary disease• Cause
– Any conditions of increased coagulation– Systemic inflammation triggering thrombosis– Hyperthermia is one of the causes that might
have a more favorable prognosis
• Two flavors– Acute and uncompensated– Chronic and compensated

Disseminated Intravascular Coagulopathy (DIC)
Blood film– Schistocytes (10% of the time)
Platelet count– <150,000/UL
Partial thromboplastin time (PTT)– prolonged
Prothrombin time (PT)– Prolonged
Activated clotting time (ACT)– Prolonged if severe

Disseminated Intravascular Coagulopathy (DIC)
Fibrin degradation products (FDPs)– increased
D-dimers– increased
Antithrombin III– Decreased (<75%)
Thrombin Time– prolonged
Fibrinogen– decreased

Ecchymoses/Petechiae Algorithm
Platelet count
Low (next slide) Normal or increased
PT, PTT/ACTnormal
One prolonged
Both prolonged
BMBT
•PT: congenital def. 7 early antiVitK•PTT: congen def 8 9 11 12
severe vWDz - 8 heparin toxicity
FDPs, TT, AT3
normal prolonged
vasculitisor problem resolving
vWDzVasculitis
thrombopathia
ObserveWork up vasculitis
Factor assays to CornellvWF assays
Rodenticide tox screen or treat with VitKCheck for MCT
vWF assaysWork up vasculitisplatelet function
VitK deficiency•All normalLiver Failure•TT prolonged•AT3 lowFactor 10 deficiency•All normal – blood to Cornellprothrombin deficiency•TT prolongedSnake Bite•FDP increased•TT prolonged•AT3 normalChronic Bleeding•FDPs increased

Ecchymoses/Petechiae Algorithm
low platelet count
50-150,000/ul
PT, PTT/ACTnormal
BMBT
FDPs, D-dimers, TT<50,000/ul
Both prolonged
normal prolonged
platelet clumps
hyperlipidemia
Cavalier
mild vasculitis
mild rickettsial
Vasculitis
rickettsial dz
Some thrombocyto
-pathias
bone marrow
neoplasia
rickettsial dz
Aplasia
Infection
toxicity
normal
1o or 2o IMT
ACT < 10 sec prolonged
Severe platelet problem
Severe bleeding – platelet consumption•Advanced Vitamin K deficiencyDIC•Increased FDPs, D-dimers, TTSnake Bite•Increased FDPs, TT
FDPs elevated
Hypercoagulable state

Ecchymoses/Petechiae Algorithm
FDPs elevated
Platelets, PT, PTT, ACT, BMBT, D-dimers, TT, AT3 normal
Hypercoagulable state
Remember…..Remember…..
Some animals will have multiple Some animals will have multiple coagulopathies simultaneouslycoagulopathies simultaneously
•DICDIC
•HypercoagulationHypercoagulation
•Severe bleedingSevere bleeding
•VasculitisVasculitis
•IMTIMT

Epistaxis Algorithm
Onset
history of nasal discharge
acute onset
serosanguinous to mucopurulent hemorrhagic
History of trauma?
check out local processes check blood pressure and
go to petechia-ecchymoses algorithm
no yes
supportive and symptomatic care, surgical
repairnormal
normal

Epistaxis – Local Processes
DDx• Nasal foreign body
– Inhalation– Reflux into caudal nasopharynx
• Infection– Chronic allergic rhinitis leading to 2o bacterial– Fungal– Viral– Parasites - Nasal mites, Cuterebra, Capillaria– Rickettsial infection
• Nasopharyngeal polyps• Aneurysm or ruptured AV fistula

Epistaxis – Local Processes
DDx• Neoplasia
– TVT• Young animals
– Adenocarcinoma– Sarcoma – melanoSA, chondroSA, fibroSA– Lymphoma
• cats >dogs• Young animals
• Dental disease– Tooth root abscess– Oronasal fistula

Epistaxis – Local Processes
Other signs of nasal disease• Sneezing• Reverse sneezing• Gagging – caudal nasopharynx• Pawing at face – rostral nasal cavities• Melena, hemoptysis
Bilateral epistaxis• Check out coagulopathy first• Neoplasia can begin on one side, invade the
septum and eventually affect both sides

Epistaxis – Work Up• CBC
– Iron deficiency anemia
– thrombocytopenia
• Profile– Panhypoproteinemia indicates blood loss
– High globulins indicate chronic inflammation• Neoplasia• Chronic rhinitis• Chronic infection – fungal, viral, bacterial, rickettsial
– Renal disease, Hepatic disease
– Hyperadrenocorticism – hypertension
– Triglycerides - hyperviscosity
• Cats - FeLV/FIV; Dogs – heartworm test

Epistaxis – Work Up
• UA– Proteinuria – PLN, hypertension– Confirm with urine protein:creatinine ratio
• Coags– PT, PTT/ACT high
• Tests for DIC – FDPs, D-dimers, ATIII• Factor Assays
– Normal PT/PTT, prolonged BMBT• vWF Assays• Platelet function tests• Look for causes of vasculitis
• Blood pressure – if high– T4/Free T4 in cats

Epistaxis – Work Up
• Imaging– Chest x-rays
• Hemoptysis can present as epistaxis– Nasal x-rays under sedation– Dental x-rays if indicated– CT is nice
• Nasal flush, rhinoscopy and biopsies– Only if coagulopathy has been ruled out– Culture is rarely helpful
• Exploratory rhinotomy if all else fails

Epistaxis – Supportive Care
• Ice packs• Intranasal epinephrine• Cage rest• If coagulopathy or severe bleeding,
transfusion may be necessary