$$$presentation title$$$ - ias-usa | physician … 3 (54.3 million: 30.1%); genotypes 2, 4, and 6...
TRANSCRIPT

5/12/2016
1
Debika Bhattacharya, MD, MS
Associate Clinical Professor of Medicine
University of California Los Angeles School of Medicine
Los Angeles, California
What Clinicians Should Know About
Hepatitis C Virus
San Francisco, California: May 5, 2016
FLOWED: 04/28/16
Slide 2 of 33
Learning Objectives
After attending this presentation, participants will
be able to:
Summarize hepatitis C virus (HCV) screening
recommendations and rationale for screening
Describe the natural history of HCV infection
Describe emerging treatments for HCV and how the
changing landscape will impact treatment decisions in
the near future
Slide 3 of 33
Objectives
Hepatitis C epidemiology and screening
Natural History
Evaluation
Genome and Drug Targets
Current Treatments
What Does SVR Really Mean?

5/12/2016
2
Slide 4 of 33
Objectives
Epidemiology and screening
Natural History
Evaluation
Genome and Drug Targets
Current Treatments
What Does SVR Really Mean?
Slide 5 of 33
HCV Worldwide
170 million infected
Highest Asia & Africa
Egypt > 15%
USA 1.6%– 3-4 million infected
www.cdc.gov
Slide 6 of 33
Worldwide prevalence of each HCV genotype by GBD
HCV genotype 1 (83.4 million cases: 46.2%)- one-third of which are in East Asia.
Genotype 3 (54.3 million: 30.1%); genotypes 2, 4, and 6 (22.8%); genotype 5 <1%.
While genotypes 1 and 3 dominate in most countries irrespective of economic
status: largest proportions of genotypes 4 and 5 are in lower-income countries.
5/12/2016
3
Slide 7 of 33
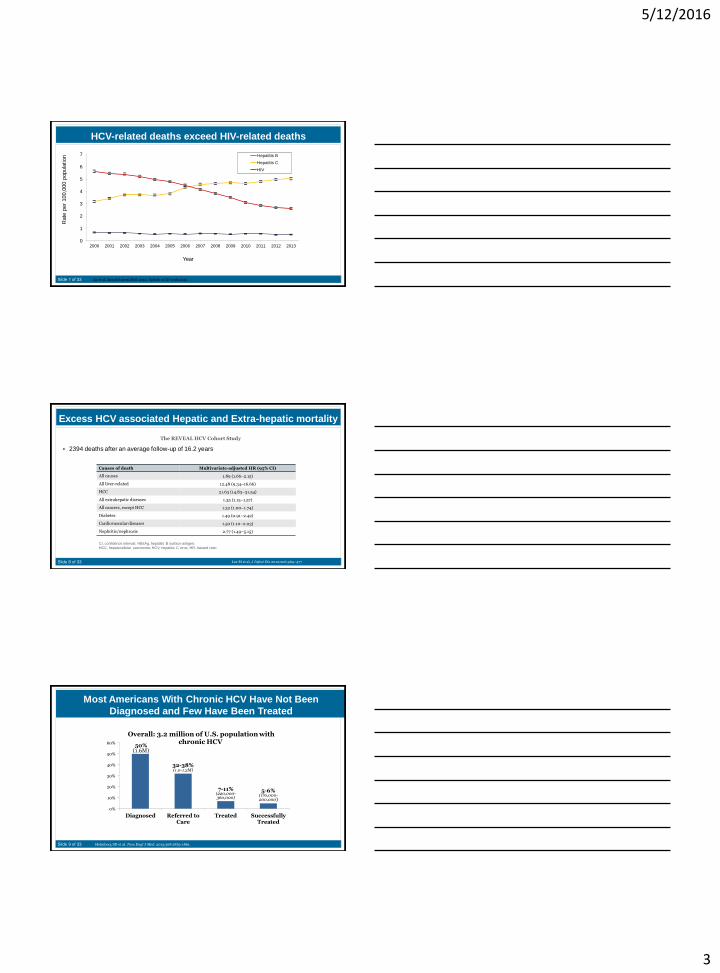
HCV-related deaths exceed HIV-related deaths
0
1
2
3
4
5
6
7
2000 2001 2002 2003 2004 2005 2006 2007 2008 2009 2010 2011 2012 2013
Rate
per
100,0
00 p
opula
tion
Year
Hepatitis B
Hepatitis C
HIV
Ly et al. Annals Intern Med 2012, Update at ID week 2015
Slide 8 of 33
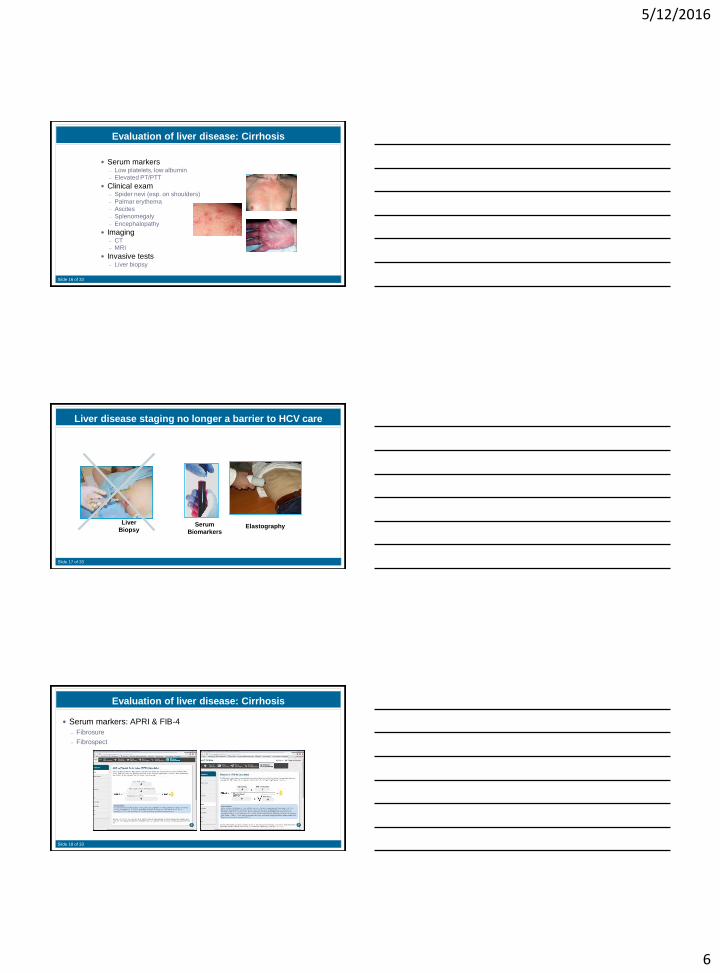
Excess HCV associated Hepatic and Extra-hepatic mortality
2394 deaths after an average follow-up of 16.2 years
Lee M et al, J Infect Dis 2012;206:469–477
Causes of death Multivariate-adjusted HR (95% CI)
All causes 1.89 (1.66–2.15)
All liver-related 12.48 (9.34–16.66)
HCC 21.63 (14.83–31.54)
All extrahepatic diseases 1.35 (1.15–1.57)
All cancers, except HCC 1.32 (1.00–1.74)
Diabetes 1.49 (0.91–2.42)
Cardiovascular diseases 1.50 (1.10–2.03)
Nephritis/nephrosis 2.77 (1.49–5.15)
The REVEAL HCV Cohort Study
CI, confidence interval; HBsAg, hepatitis B surface antigen;
HCC, hepatocellular carcinoma; HCV, hepatitis C virus; HR, hazard ratio
Slide 9 of 33 Holmberg SD et al. New Engl J Med. 2013;368:1859-1861.
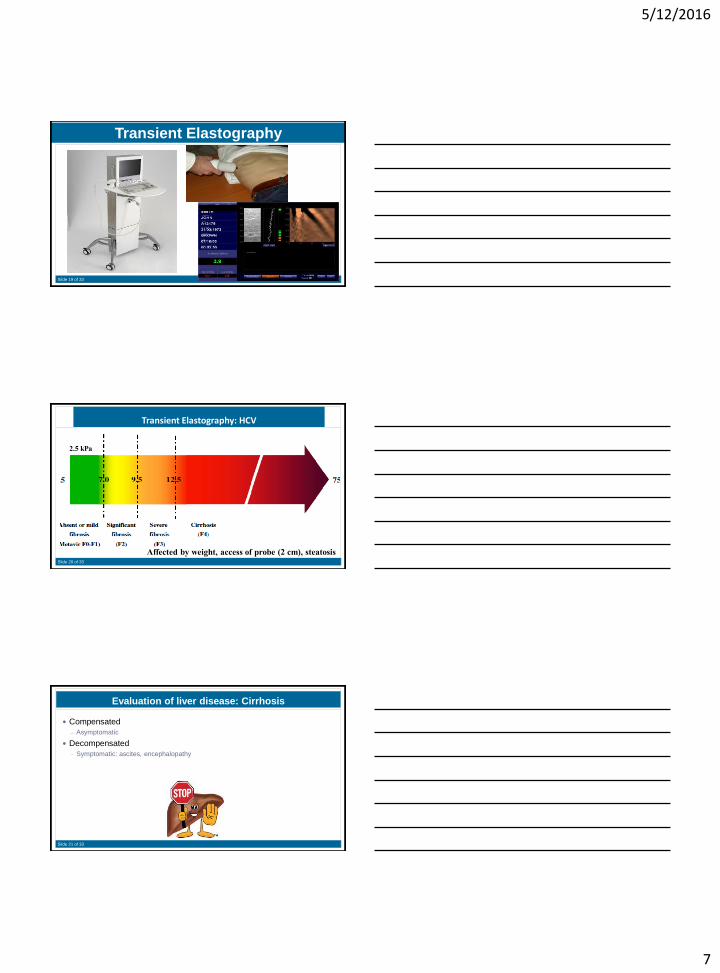
Most Americans With Chronic HCV Have Not Been
Diagnosed and Few Have Been Treated
50%(1.6M)
32-38%(1.0-1.2M)
7-11%(220,000-360,000)
5-6%(170,000-200,000)
0%
10%
20%
30%
40%
50%
60%
Diagnosed Referred toCare
Treated SuccessfullyTreated
Overall: 3.2 million of U.S. population with chronic HCV

5/12/2016
4
Slide 10 of 33
HCV Screening
Screen with hepatitis C antibody test
Slide 11 of 33
Hepatitis C Tests
Hepatitis C antibody tests
– Turn positive 8 weeks after exposure
– Immunoassays performed in lab
Sensitivity 99%, Specificity 100%
– Rapid immunoassays
HCV Rapid antibody test
Sensitivity and specificity >99% on blood
– Home-based self-collected tests
HCV RNA test
– Confirm presence or absence of infection
– Quantify HCV RNA
Slide 12 of 33
HCV testing algorithm
Consider simultaneous anti-HCV and HCV RNA
A. Immunocompromised patients• Patients on hemodialysis• Transplant recipients• Advanced HIV
B. Acute HCV / Recent exposure
hcvguidelines.org

5/12/2016
5
Slide 13 of 33
Objectives
Epidemiology & screening
Natural History
Evaluation
Genome and Drug Targets
Current Treatments
What Does SVR Really Mean?
Slide 14 of 70
Slide 14 of 33
Resolved
Stable
Slowly
Progressive
Transplant/Death
~20%
~15% ~85%
~3%-4%/yr
~80%
~75%
~ 20-year progression rate may beaccelerated with HIV, HBV,
alcohol, and steatosis1,2
Exposure(Acute Phase)
Chronic
Cirrhosis
~4%/yr~6%/yr
ESLD HCC
10 20 30Time(yrs)
5-year survival in patients with HCC is <5%*
ESLD: end-stage liver disease
*NIH Consens Statement. June 10-12, 2002;19(3):1-46. NIH Consens Statement. March 24-26, 1997;15(3):1-41.
1. Di Bisceglie AM. Hepatology. 2000;31(4):1014-1018. 2. Bialek SR, Terrault NA. Clin Liver Dis. 2006;10(4):697-715.
Natural History of HCV Infection
Slide 15 of 33
Objectives
Epidemiology & screening
Natural History
Evaluation
Genome and Drug Targets
Current Treatments
What Does SVR Really Mean?
5/12/2016
6
Slide 16 of 33
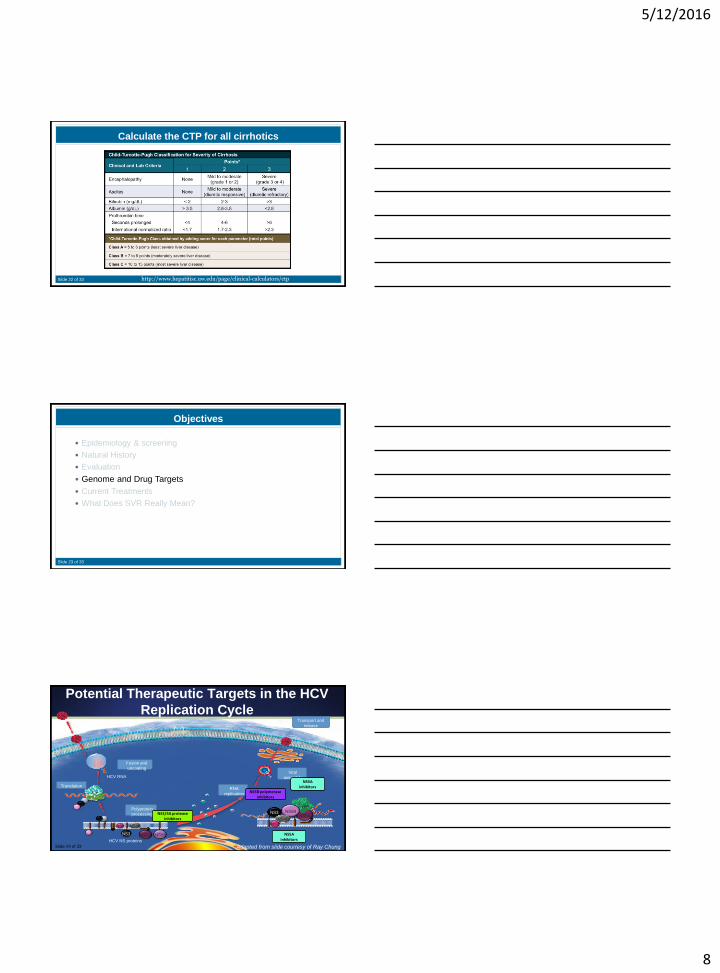
Evaluation of liver disease: Cirrhosis
Serum markers– Low platelets, low albumin
– Elevated PT/PTT
Clinical exam– Spider nevi (esp. on shoulders)
– Palmar erythema
– Ascites
– Splenomegaly
– Encephalopathy
Imaging– CT
– MRI
Invasive tests– Liver biopsy
Slide 17 of 33
ElastographySerum
Biomarkers
Liver disease staging no longer a barrier to HCV care
Liver
Biopsy
Slide 18 of 33
Evaluation of liver disease: Cirrhosis
Serum markers: APRI & FIB-4
– Fibrosure
– Fibrospect
5/12/2016
7
Slide 19 of 33
Transient Elastography
Slide 20 of 33
Transient Elastography: HCV
2.5 kPa
Affected by weight, access of probe (2 cm), steatosis
Slide 21 of 33
Evaluation of liver disease: Cirrhosis
Compensated
– Asymptomatic
Decompensated
– Symptomatic: ascites, encephalopathy
5/12/2016
8
Slide 22 of 33
Calculate the CTP for all cirrhotics
http://www.hepatitisc.uw.edu/page/clinical-calculators/ctp
Slide 23 of 33
Objectives
Epidemiology & screening
Natural History
Evaluation
Genome and Drug Targets
Current Treatments
What Does SVR Really Mean?
Slide 24 of 33
Translation
HCV NS proteins
NS2
Polyprotein
processing
NS3
NS4B
NS5A NS5B
HCV RNA
Fusion and
uncoating
RNA
replication
NS5A
CypA
NS5B
NS2
NS3
NS4B
Viral
assembly
Transport and
release
NS3/4A protease inhibitors
NS5A inhibitors
NS5B polymerase inhibitors
NS5A inhibitors
Potential Therapeutic Targets in the HCV
Replication Cycle
Adapted from slide courtesy of Ray ChungSlide 24 of 33
5/12/2016
9
Slide 25 of 33
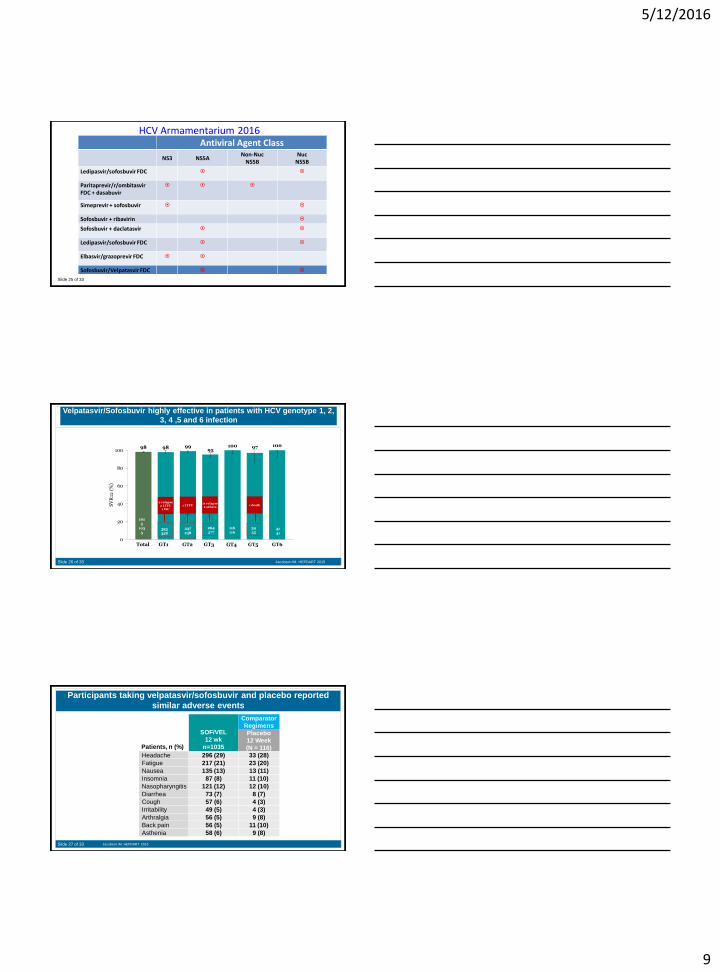
HCV Armamentarium 2016Antiviral Agent Class
NS3 NS5ANon-Nuc
NS5BNuc
NS5B
Ledipasvir/sofosbuvir FDC
Paritaprevir/r/ombitasvir FDC + dasabuvir
Simeprevir + sofosbuvir
Sofosbuvir + ribavirin
Sofosbuvir + daclatasvir
Ledipasvir/sofosbuvir FDC
Elbasvir/grazoprevir FDC
Sofosbuvir/Velpatasvir FDC
Slide 26 of 33
98 98 9995
100 97 100
0
20
40
60
80
100
SV
R12
(%
)
Velpatasvir/Sofosbuvir highly effective in patients with HCV genotype 1, 2,
3, 4 ,5 and 6 infection
Jacobson IM. HEPDART 2015
Total GT1 GT2 GT3 GT4 GT5 GT6
323
328
237
238
264
277
116
116
34
3541
41
101
5
103
5
1 death2 relapse2 LTFU
1 WC
11 relapse2 others
1 LTFU
Slide 27 of 33
Participants taking velpatasvir/sofosbuvir and placebo reported
similar adverse events
SOF/VEL
12 wk
n=1035
Comparator
Regimens
Placebo
12 Week
(N = 116)Patients, n (%)
Headache 296 (29) 33 (28)
Fatigue 217 (21) 23 (20)
Nausea 135 (13) 13 (11)
Insomnia 87 (8) 11 (10)
Nasopharyngitis 121 (12) 12 (10)
Diarrhea 73 (7) 8 (7)
Cough 57 (6) 4 (3)
Irritability 49 (5) 4 (3)
Arthralgia 56 (5) 9 (8)
Back pain 56 (5) 11 (10)
Asthenia 58 (6) 9 (8)
Jacobson IM. HEPDART 2015

5/12/2016
10
Slide 28 of 33
Don’t rain on my parade
HCV RAVS
Slide 29 of 33
HCV RAVs
Resistance-associated variants (RAV) arise when a specific amino
acid change occurs at a position that modifies the interaction with
a drug
RAVs lead to decreased viral replication (“fitness”)
Baseline prevalence of NS5A RAVs: up to 12%, depending on
sequencing methodology
RAVs increase the concentration of drug needed to inhibit viral
replication (EC50) (“resistance”)
– <2 - >1000-fold more drug needed to inhibit virus
Slide 30 of 33
84%No NS5A polymorphisms
at baseline
0
16%NS5A polymorphisms
at baseline
n=294/318
93% SVR
n=318
n=1629*
*5 Subjects not successfully sequenced
Polymorphisms analyzed by deep sequencing
97% SVR
Effect of Baseline NS5A Resistance-Associated Polymorphisms on SVR
ION Phase 3 Program (ION-1, ION-2, ION-3)
Afdhal N, et al. N Engl J Med 2014; 370: 1889-98;Afdhal N, et al. N Engl J Med 2014; 370: 1483-93;
Kowdley K, et al. N Engl J Med 2014; 370: 1879-88.
AASLD/IDSA. Recommendations for testing, managing, and treating
hepatitis C. http://www.hcvguidelines.org. Accessed July 11, 2014
5/12/2016
11
Slide 31 of 33
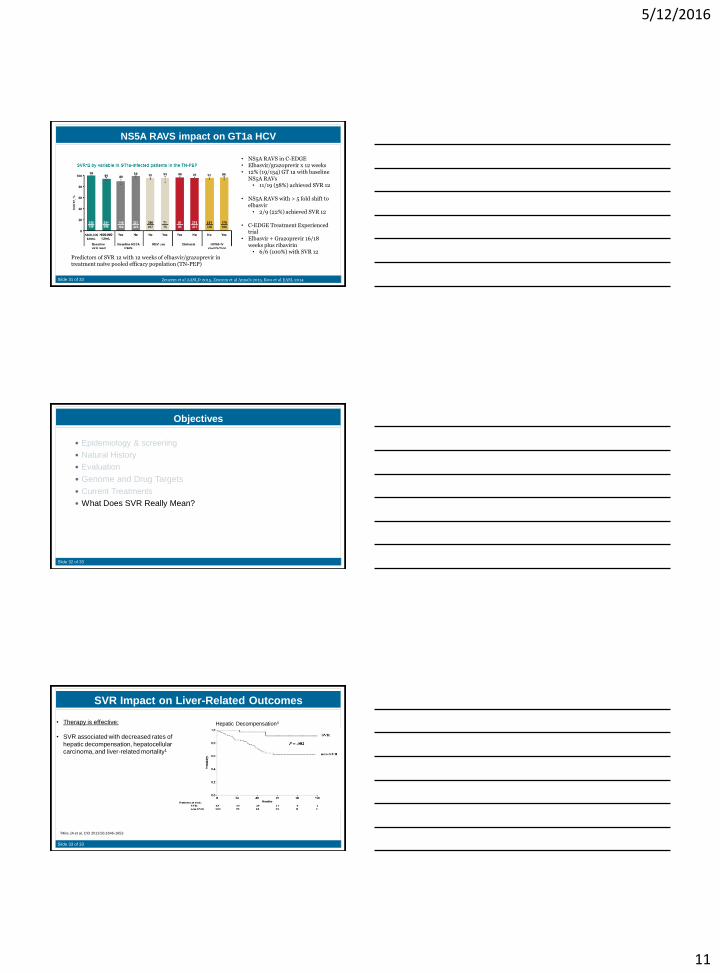
NS5A RAVS impact on GT1a HCV
• NS5A RAVS in C-EDGE• Elbasvir/grazoprevir x 12 weeks • 12% (19/154) GT 1a with baseline
NS5A RAVs• 11/19 (58%) achieved SVR 12
• NS5A RAVS with > 5 fold shift to elbasvir
• 2/9 (22%) achieved SVR 12
• C-EDGE Treatment Experienced trial
• Elbasvir + Grazoprevir 16/18 weeks plus ribavirin
• 6/6 (100%) with SVR 12
Zeuzem et al AASLD 2015, Zeuzem et al Annals 2015, Kwo et al EASL 2014
Predictors of SVR 12 with 12 weeks of elbasvir/grazoprevir in treatment naïve pooled efficacy population (TN-PEP)
Slide 32 of 33
Objectives
Epidemiology & screening
Natural History
Evaluation
Genome and Drug Targets
Current Treatments
What Does SVR Really Mean?
Slide 33 of 33
SVR Impact on Liver-Related Outcomes
1Mira JA et al, CID 2013;56:1646-1653
Hepatic Decompensation4• Therapy is effective:
• SVR associated with decreased rates of
hepatic decompensation, hepatocellular
carcinoma, and liver-related mortality1