presentazione standard di powerpoint - esim2014 sepsis daniele coen.pdf · acute osteomyelitis 50%...
TRANSCRIPT
Sepsis
Daniele Coen
Esim
06/16/2014

You are working in the ED late one evening when an 82-year-old man is brought in by his son. His son reports thatearlier today, his father had been in his usual state ofhealth, but this evening he found his father confused, withlabored breathing.
On arrival, the patient has the following vital signs:temperature, 38°C; heart rate, 130 beats/min; bloodpressure, 110/60 mm Hg; respiratory rate, 34 breaths/min;and oxygen saturation, 89% on room air. He is delirious andunable to answer questions.
A focused physical examination demonstrates tachycardiawithout extra heart sounds or murmurs, right basilarcrackles on lung auscultation, a benign abdomen, andminimal lower extremity pitting edema.
A further history obtained from the son reveals that his father hasarterial hypertension, congestive heart failure, and a history of priormyocardial infarction that was treated with stent placement tenyears earlier.
While you check an ECG which shows sinus tachycardia and thesigns of a previous inferior infarction and ask for labs, you askyourself:
COULD THIS PATIENT BE SEPTIC?

Infection SIRS Sepsis Severe Septic
sepsis shock
1. T > 38.3 o < 36°C
2. WBC <4.000 o >12000 o >10% bands
3. HR > 90/min
4. RR > 20/min5. Other inflammatory variables
6. Organ dysfunction variables
7. Haemodynamic variables
8. Tissue hypoperfusion variables
SEPSIS
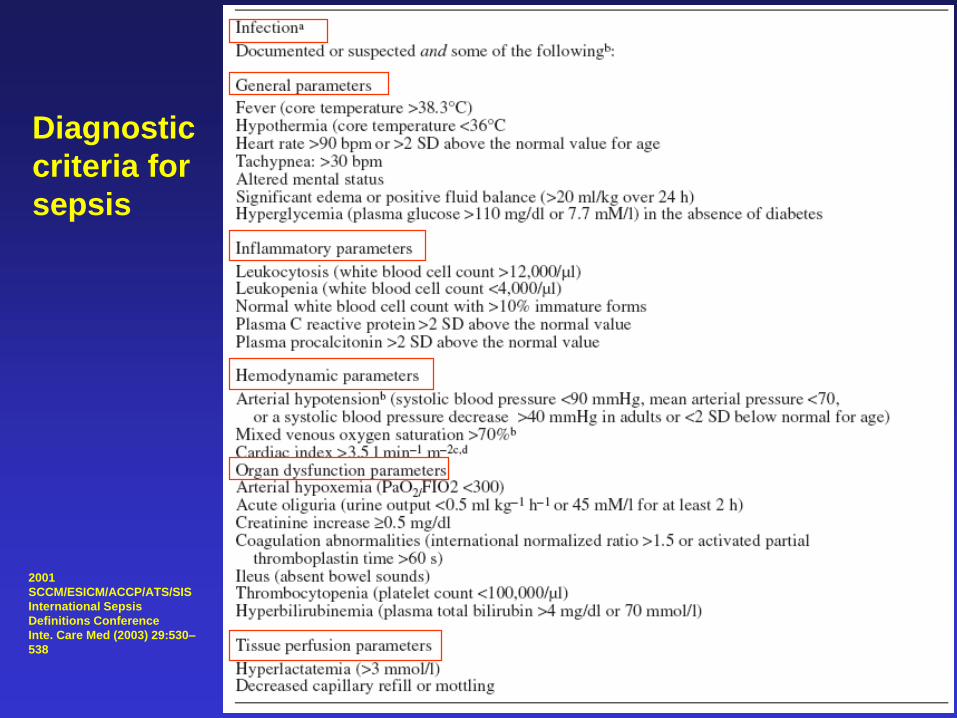
2001 SCCM/ESICM/ACCP/ATS/SIS International Sepsis Definitions Conference
SIRS in the setting of an infection
2001
SCCM/ESICM/ACCP/ATS/SIS
International Sepsis
Definitions Conference
Inte. Care Med (2003) 29:530–
538
Diagnostic
criteria for
sepsis
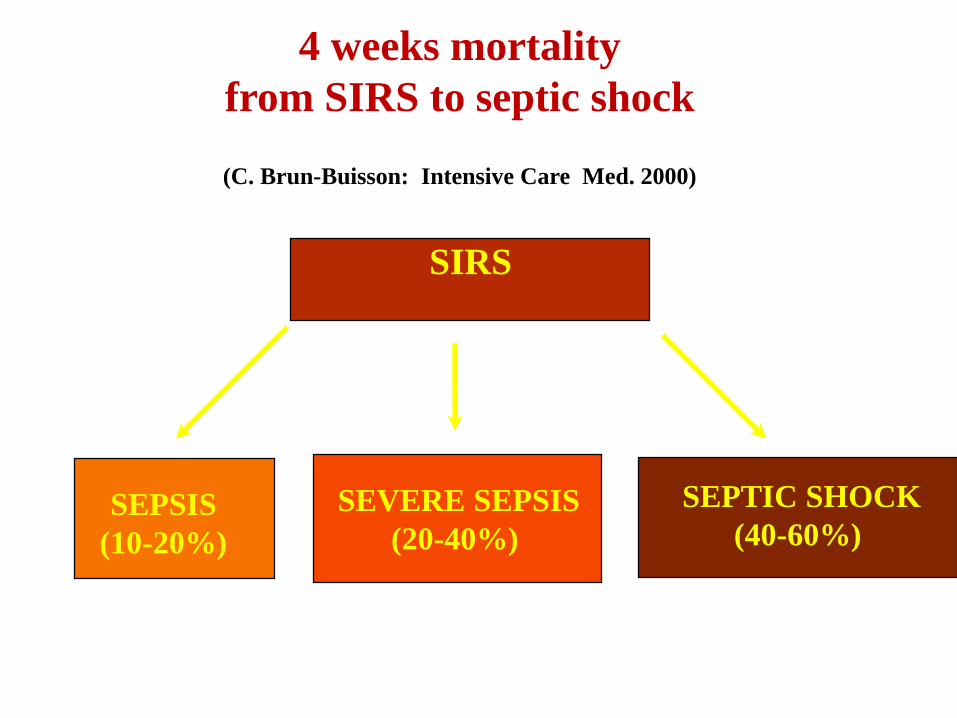
SIRS
SEPSIS
(10-20%)
SEPTIC SHOCK
(40-60%)SEVERE SEPSIS
(20-40%)
4 weeks mortality
from SIRS to septic shock
(C. Brun-Buisson: Intensive Care Med. 2000)
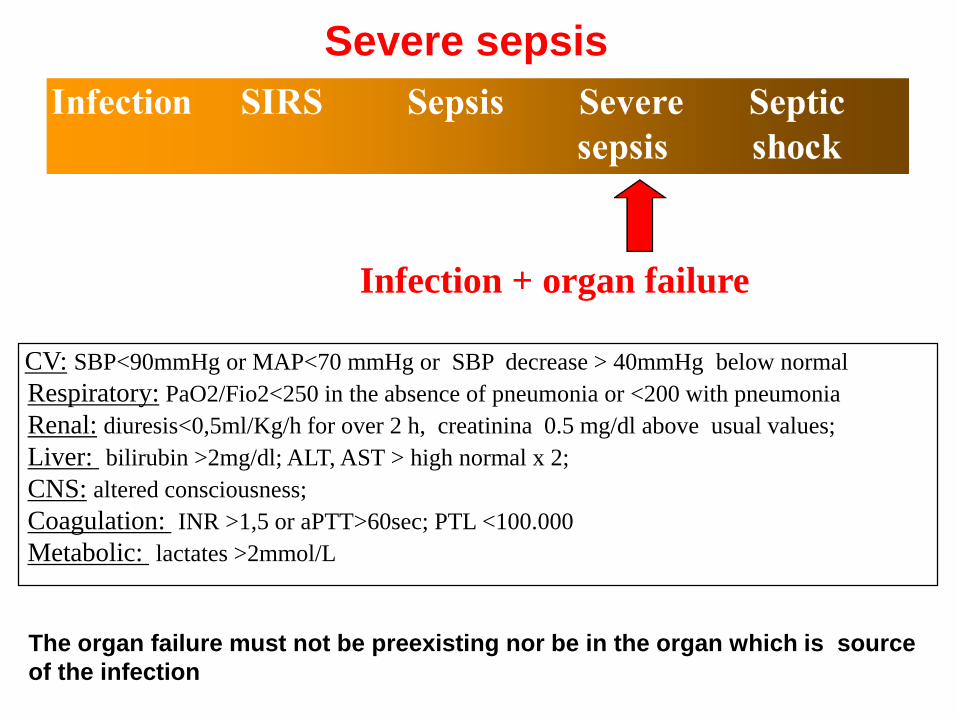
CV: SBP<90mmHg or MAP<70 mmHg or SBP decrease > 40mmHg below normal
-Respiratory: PaO2/Fio2<250 in the absence of pneumonia or <200 with pneumonia
-Renal: diuresis<0,5ml/Kg/h for over 2 h, creatinina 0.5 mg/dl above usual values;
-Liver: bilirubin >2mg/dl; ALT, AST > high normal x 2;
-CNS: altered consciousness;
-Coagulation: INR >1,5 or aPTT>60sec; PTL <100.000
-Metabolic: lactates >2mmol/L
Infection + organ failure
Severe sepsis
The organ failure must not be preexisting nor be in the organ which is source
of the infection
99
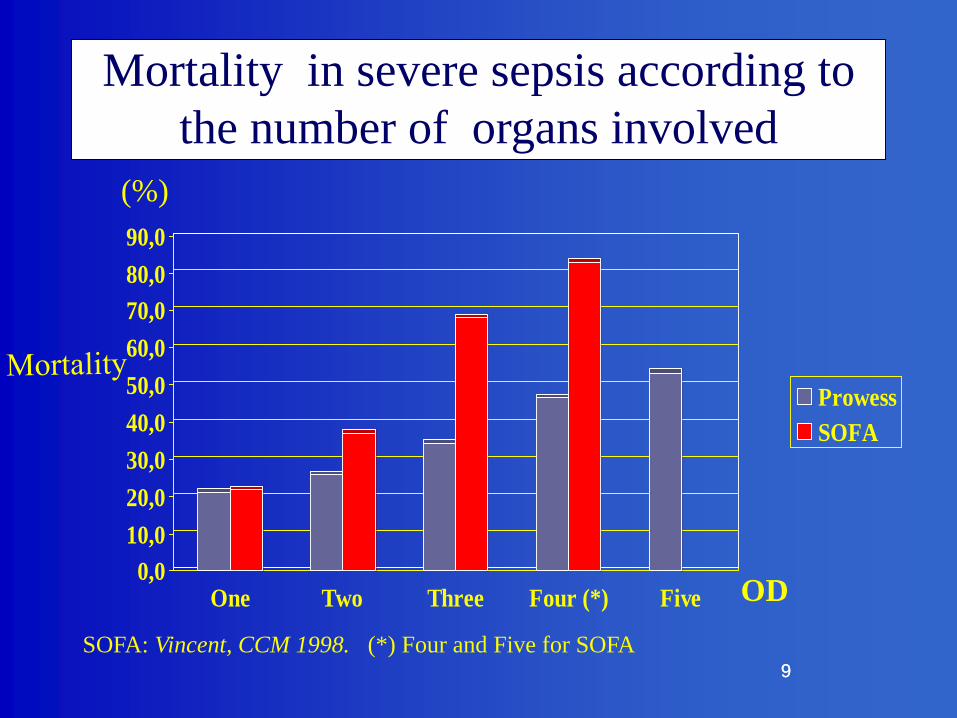
0,0
10,0
20,0
30,0
40,0
50,0
60,0
70,0
80,0
90,0
One Two Three Four (*) Five
Prowess
SOFA
Mortality in severe sepsis according to
the number of organs involved
(%)
OD
SOFA: Vincent, CCM 1998. (*) Four and Five for SOFA
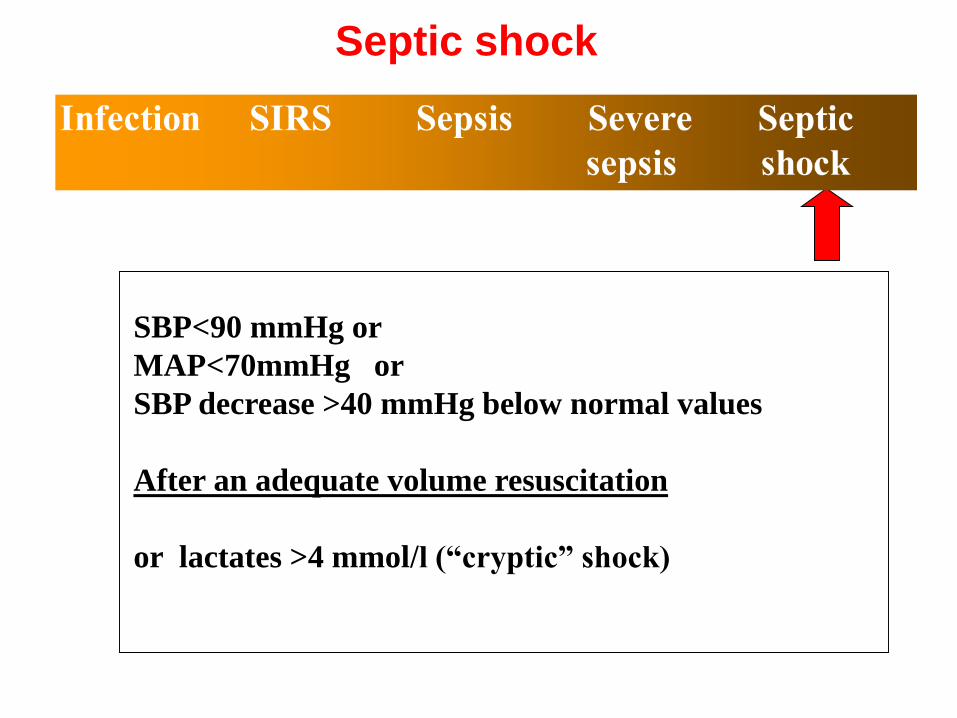
SBP<90 mmHg or
MAP<70mmHg or
SBP decrease >40 mmHg below normal values
After an adequate volume resuscitation
or lactates >4 mmol/l (“cryptic” shock)
Septic shock

Back to your patient
• BP 110/60 (in previously hypertensive)
• HR 130
• RR 34
• SaO2 89%
• Confused
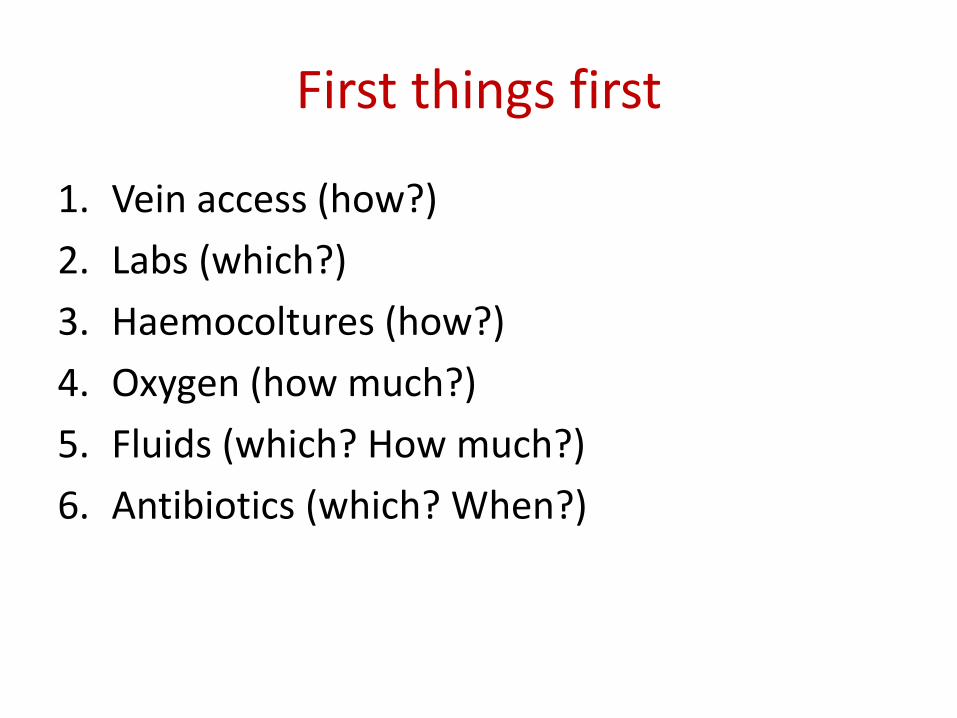
First things first
1. Vein access (how?)
2. Labs (which?)
3. Haemocoltures (how?)
4. Oxygen (how much?)
5. Fluids (which? How much?)
6. Antibiotics (which? When?)

1. Vein access
• Large bore
• Preferably two
• Delay CVC

14 G short 175-200
15014 G long
16 G short 100-150
16 G long 100
18 G long 50
ml/minGauge, length and reach
2. Labs
• Lactate (high prognostic value)
• Procalcitonin (?)
• Chemistry
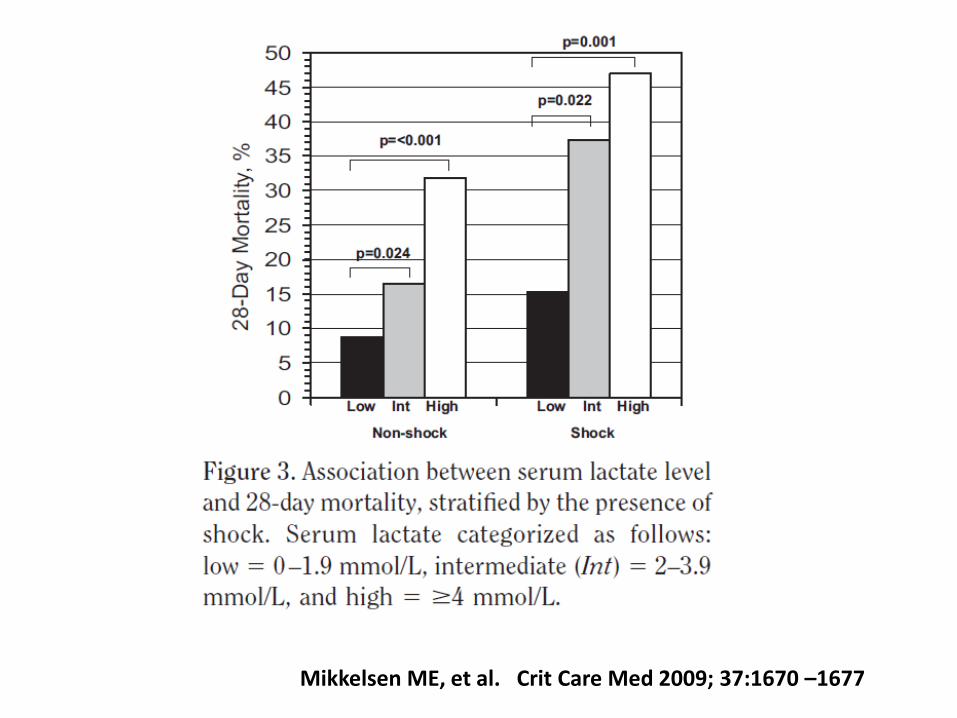
Mikkelsen ME, et al. Crit Care Med 2009; 37:1670 –1677

Procalcitonin for early diagnosis and differentiation of SIRS, sepsis, severe sepsis, and septic shock
Brunkhorst E:M: et al Intensive Care Med 2000, 26: S148- S152
3. Haemocoltures
• Soon
• Aerobes and anaerobes
• Adequate technique
• Adequate volume
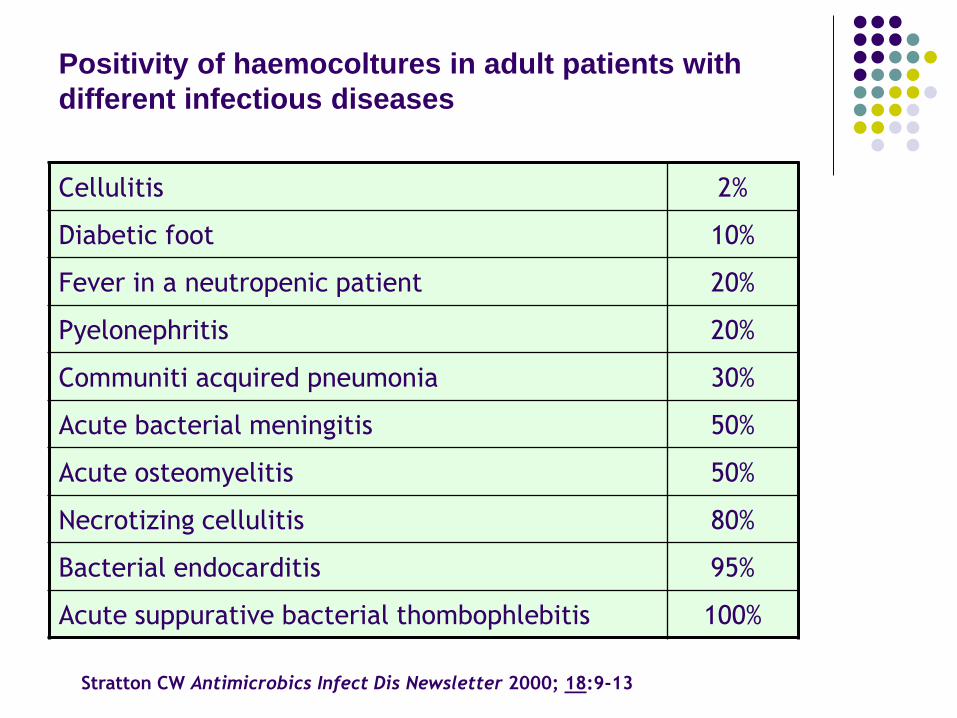
Positivity of haemocoltures in adult patients with
different infectious diseases
Cellulitis 2%
Diabetic foot 10%
Fever in a neutropenic patient 20%
Pyelonephritis 20%
Communiti acquired pneumonia 30%
Acute bacterial meningitis 50%
Acute osteomyelitis 50%
Necrotizing cellulitis 80%
Bacterial endocarditis 95%
Acute suppurative bacterial thombophlebitis 100%
Stratton CW Antimicrobics Infect Dis Newsletter 2000; 18:9-13

Sampling
Bacteriaemia 30-90 min Shivering Fever
No advantage by any sampling time
No advantage between contemporary and refractedsampling
Volume increase 20 to 40 mL + 19% positive results
Volume increase 40 to 60 mL + 10% positive results
Conclusions:
Draw simultaneously, no less than 2 sets (40 mL) possiblyfrom 2 different sites
Li J et al. J Clin Microbiol 1994; 32:2829-2831
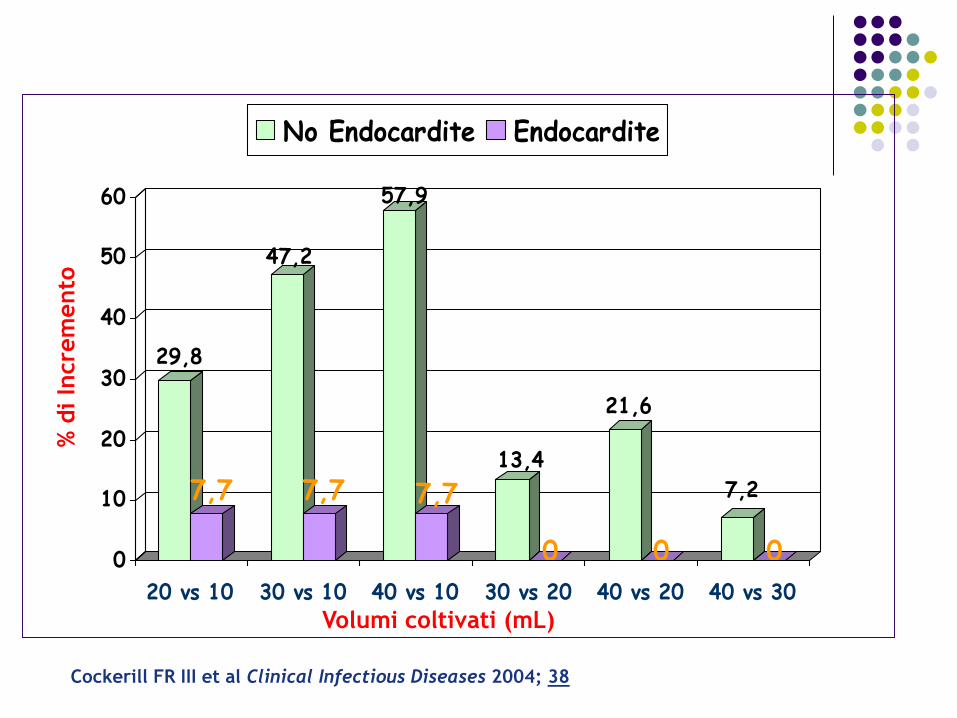
29,8
7,7
47,2
7,7
57,9
7,713,4
0
21,6
0
7,2
00
10
20
30
40
50
60
20 vs 10 30 vs 10 40 vs 10 30 vs 20 40 vs 20 40 vs 30
No Endocardite Endocardite
Volumi coltivati (mL)
% d
i In
cre
mento
Cockerill FR III et al Clinical Infectious Diseases 2004; 38
4. Oxygen
• Soon
• Targeted to an adequate SaO2
• Remember that oxygen delivery to tissuesdepends also on CO and the haematocrit
• Enough but not too much
BTS Guideline for emergency oxygen use in adult patients –Jan 2008
Assessing patients
• For critically ill patients, high concentration oxygen should be administered immediately and this should be recorded afterwards in the patient’s health record.
• Oxygen saturation, ‘‘the fifth vital sign’’, should be checked by pulse oximetry in all breathless and acutely ill patients (supplemented by blood gases when necessary) and the inspired oxygen concentration should be recorded on the observation chart with the oximetry result.
• Pulse oximetry must be available in all locations where emergency oxygen is used.
Besides adequate CaO2 and PaO2, delivery of
oxygen depends upon adequate flow of oxygenated
blood. Cardiac output in turn depends upon
adequate blood (circulating) volume, adequate
venous return and adequate and optimal myocardial
function. To avoid tissue hypoxia, attention must
therefore be paid to the volume status of the patient
and the adequacy of cardiac function, as well as
initiating oxygen therapy.
BTS Guideline for emergency oxygen use in adult patients –Jan 2008
Oxygen prescription
• Oxygen should be prescribed to achieve a target saturation of 94–98% for most acutely ill patients or 88–92% for those at risk of hypercapnic respiratory failure .
• The target saturation should be written on the drug chart .
BTS Guideline for emergency oxygen use in adult patients –Jan 2008
Table 1 Critical illnesses requiring high levels of supplemental oxygen
• The initial oxygen therapy is a reservoir mask at 15 l/min.• Once stable, reduce the oxygen dose and aim for target
saturation range of 94–98%• If oximetry is unavailable, continue to use a reservoir mask until
definitive treatment is available.• Patients with COPD and other risk factors for hypercapnia who
develop critical illness should have the same initial target saturations as other critically ill patients pending the results of blood gas measurements, after which these patients may need controlled oxygen therapy or supported ventilation if there is severe hypoxaemia and/or hypercapnia with respiratory acidosis.
BTS Guideline for emergency oxygen use in adult patients –Jan 2008
6.3.7 Summary of risks of hyperoxia and supplemental oxygen therapy
Physiological risks
(1) Worsened V/Q mismatch.
(2) Absorption atelectasis.
(3) Coronary and cerebral vasoconstriction.
(4) Reduced cardiac output.
(5) Damage from oxygen free radicals.
(6) Increased systemic vascular resistance.
Clinical risks
(1) Worsening of hypercapnic respiratory failure.
(2) Delay in recognition of clinical deterioration.
(3) Worse outcomes in mild to moderate stroke.
(4) Specific risk in patients with previous bleomycin lung
damage or with paraquat poisoning or acid aspiration.
(5) Unknown risk-benefit balance in acute coronary artery
disease with normal oxygen saturation.
BTS Guideline for emergency oxygen use in adult patients –Jan 2008
5. Fluids
• Ask Rodolfo…
• Trust crystalloids
• Administer with a fluid challenge technique
• Strike soon (30 mL/Kg ) then slow down

6. Antibiotics
• Soon• Adequate (follow a hospital protocol)• Don’t mind renal function for the first dose• Mind dilution and timing• Re-evaluate at 24hrs
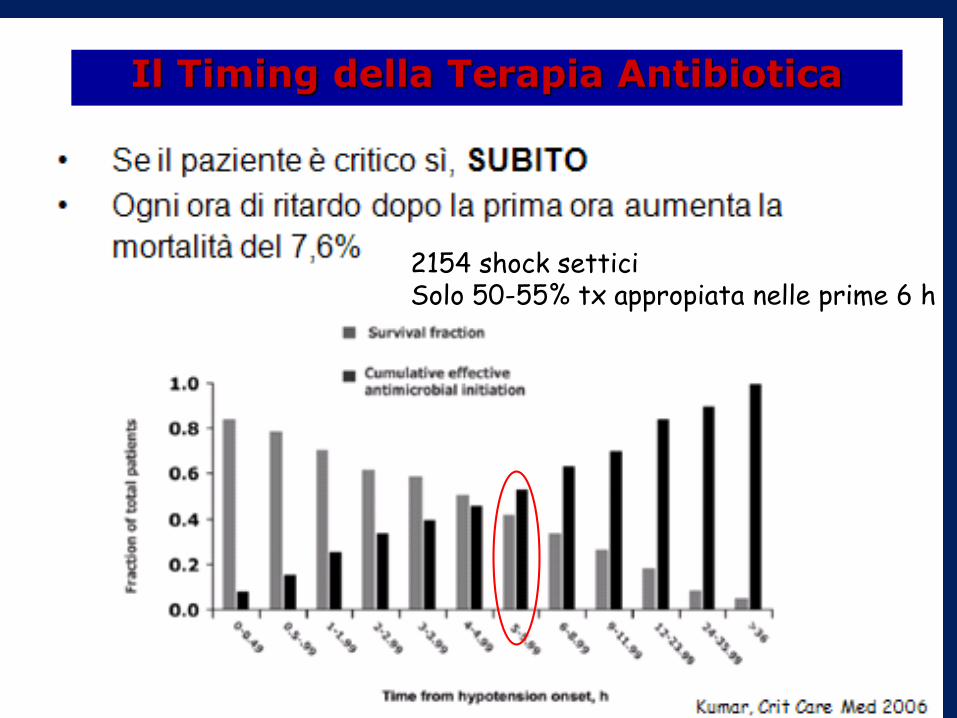
•2154 shock settici•Solo 50-55% tx appropiata nelle prime 6 h
Il Timing della Terapia Antibiotica
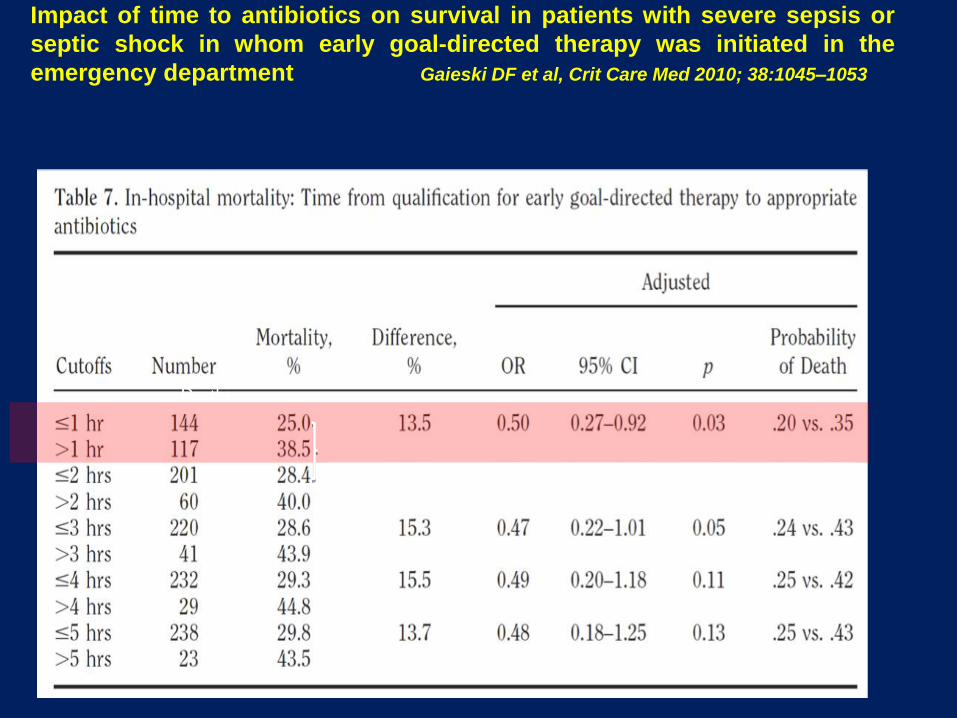
Impact of time to antibiotics on survival in patients with severe sepsis or
septic shock in whom early goal-directed therapy was initiated in the
emergency department Gaieski DF et al, Crit Care Med 2010; 38:1045–1053
Deaths
36% mortality treatment after 1 and before 2 hrs.
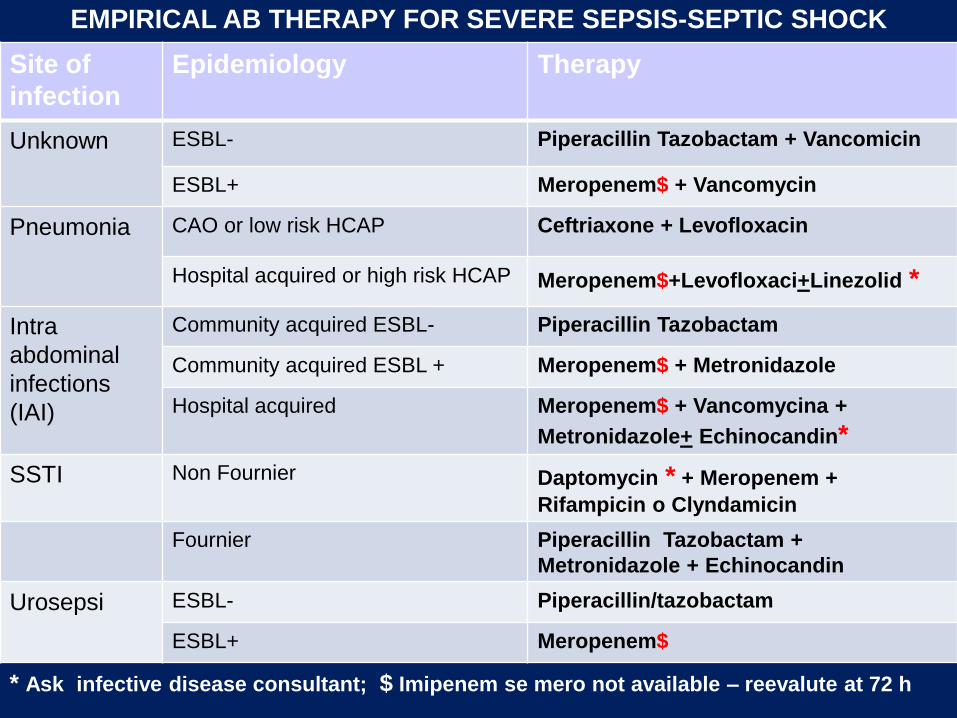
Site of
infection
Epidemiology Therapy
Unknown ESBL- Piperacillin Tazobactam + Vancomicin
ESBL+ Meropenem$ + Vancomycin
Pneumonia CAO or low risk HCAP Ceftriaxone + Levofloxacin
Hospital acquired or high risk HCAP Meropenem$+Levofloxaci+Linezolid *
Intra
abdominal
infections
(IAI)
Community acquired ESBL- Piperacillin Tazobactam
Community acquired ESBL + Meropenem$ + Metronidazole
Hospital acquired Meropenem$ + Vancomycina +
Metronidazole+ Echinocandin*
SSTI Non Fournier Daptomycin * + Meropenem +
Rifampicin o Clyndamicin
Fournier Piperacillin Tazobactam +
Metronidazole + Echinocandin
Urosepsi ESBL- Piperacillin/tazobactam
ESBL+ Meropenem$
* Ask infective disease consultant; $ Imipenem se mero not available – reevalute at 72 h
EMPIRICAL AB THERAPY FOR SEVERE SEPSIS-SEPTIC SHOCK
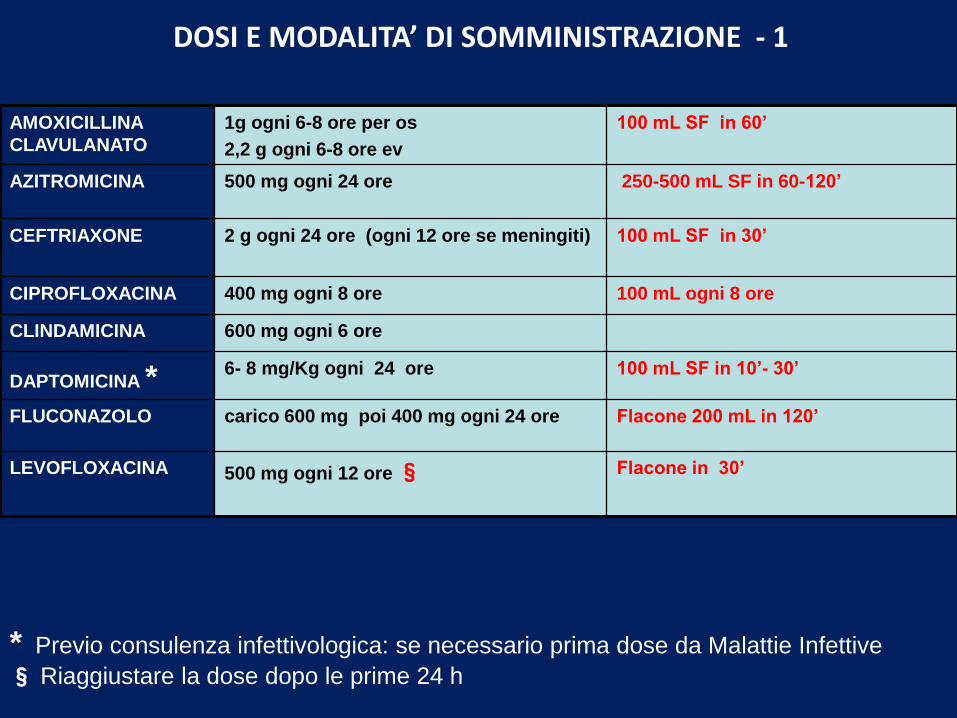
AMOXICILLINA
CLAVULANATO
1g ogni 6-8 ore per os
2,2 g ogni 6-8 ore ev
100 mL SF in 60’
AZITROMICINA 500 mg ogni 24 ore 250-500 mL SF in 60-120’
CEFTRIAXONE 2 g ogni 24 ore (ogni 12 ore se meningiti) 100 mL SF in 30’
CIPROFLOXACINA 400 mg ogni 8 ore 100 mL ogni 8 ore
CLINDAMICINA 600 mg ogni 6 ore
DAPTOMICINA * 6- 8 mg/Kg ogni 24 ore 100 mL SF in 10’- 30’
FLUCONAZOLO carico 600 mg poi 400 mg ogni 24 ore Flacone 200 mL in 120’
LEVOFLOXACINA 500 mg ogni 12 ore § Flacone in 30’
* Previo consulenza infettivologica: se necessario prima dose da Malattie Infettive
§ Riaggiustare la dose dopo le prime 24 h
DOSI E MODALITA’ DI SOMMINISTRAZIONE - 1
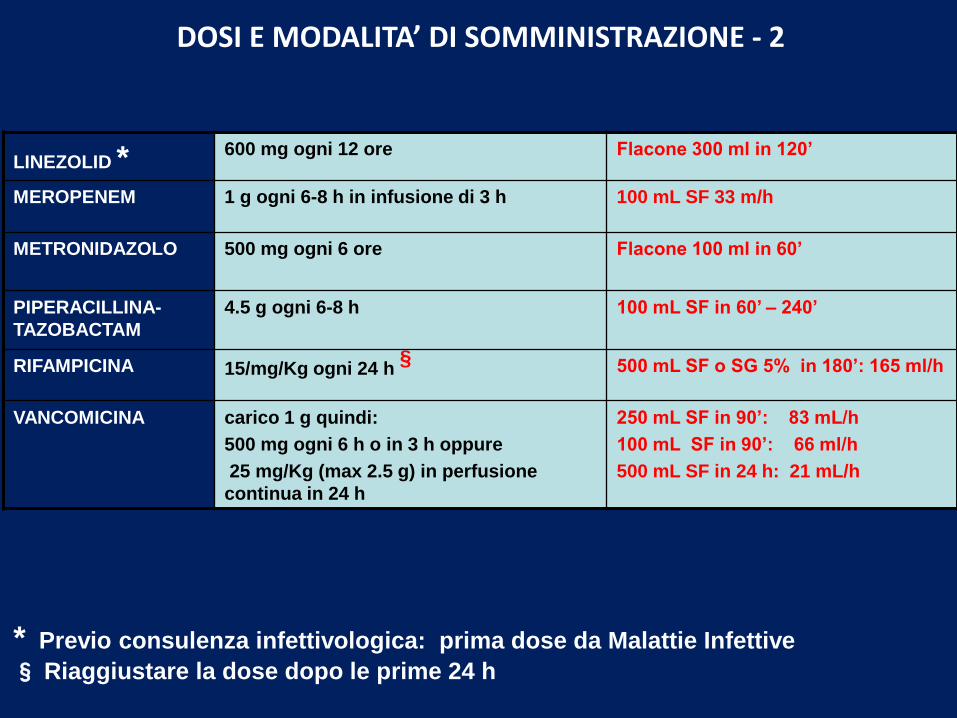
LINEZOLID * 600 mg ogni 12 ore Flacone 300 ml in 120’
MEROPENEM 1 g ogni 6-8 h in infusione di 3 h 100 mL SF 33 m/h
METRONIDAZOLO 500 mg ogni 6 ore Flacone 100 ml in 60’
PIPERACILLINA-
TAZOBACTAM
4.5 g ogni 6-8 h 100 mL SF in 60’ – 240’
RIFAMPICINA 15/mg/Kg ogni 24 h § 500 mL SF o SG 5% in 180’: 165 ml/h
VANCOMICINA carico 1 g quindi:
500 mg ogni 6 h o in 3 h oppure
25 mg/Kg (max 2.5 g) in perfusione
continua in 24 h
250 mL SF in 90’: 83 mL/h
100 mL SF in 90’: 66 ml/h
500 mL SF in 24 h: 21 mL/h
* Previo consulenza infettivologica: prima dose da Malattie Infettive
§ Riaggiustare la dose dopo le prime 24 h
DOSI E MODALITA’ DI SOMMINISTRAZIONE - 2
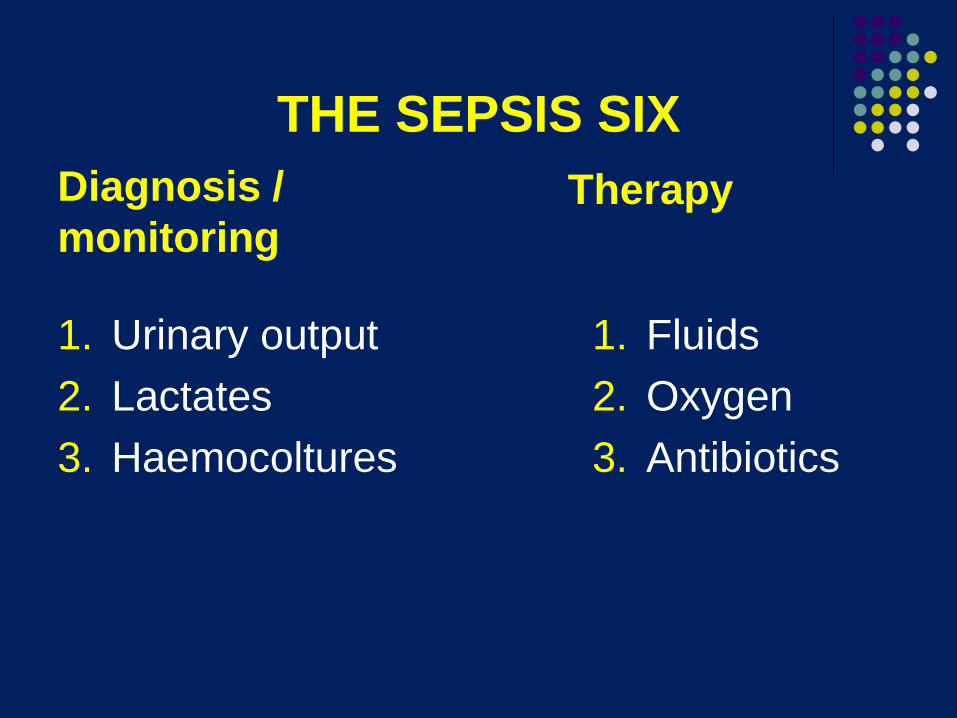
THE SEPSIS SIX
Diagnosis /
monitoring
1. Urinary output
2. Lactates
3. Haemocoltures
Therapy
1. Fluids
2. Oxygen
3. Antibiotics

Back to your patient
By this time you have:
1. secured a vein with two 16G short cannulae2. sent blood for coltures, lactate and chemistry3. infused 2000 ml Ringer lactate4. administered oxygen to a SaO2 of 98%5. administered ceftriaxone2g and levofloxacin
750mg6. started monitoring urinary output
Back to your patient
You are proud of what you have done, but your patientdoesn’t seem to be improving:
• SBP 90/60• HR 125• RR 30• SaO2 95% (O2 10l/min)• Still confused• Lactate: 5.7 mmol/L• Creatinine: 2.5• INR: 1.7
What next ?
1. Identify (and remove if possible) the septicsource
2. Keep working on haemodynamics
We recommend that a specific anatomical
diagnosis of infection requiring consideration
for emergent source control (eg, necrotizing
soft tissue infection, peritonitis, cholangitis,
intestinal infarction) be sought and diagnosed
or excluded as rapidly as possible, and
intervention be undertaken for source control
within the first 12 hr after the diagnosisis made, if feasible (grade 1C).
SSC Guidelines 2012
When source control in a severely septic patient is
required, the effective intervention associated with the
least physiologic insult should be used (eg,
percutaneous rather than surgical drainage of an
abscess) (UG).
If intravascular access devices are a possible source
of severe sepsis or septic shock, they should be
removed promptly after other vascular access has beenestablished (UG).
SSC Guidelines 2012
Remove the septic source
1. Use bedside echo as a first choice
2. Plan in advance if you want to be effective
3. Use the least invasive approach
Keep working on haemodynamics
1. More fluids (is he/she still fluid responsive?)2. Vasopressors (which? when?)3. Inotropes (which? when?)4. Transfusion?5. Other ?
The easy way out
Get the guidelines and follow EGDT
Emanuel Rivers, Bryant Nguyen, Suzanne
Havstad, et al. Early goal-directed
treatment in severe sepsis and septic
shock. New England Journal of Medicine
2001;345:1368-1377.
Donnino MW, Bryant Nguyen, Gordon
Jacobsen, Michael Tomlanovich,
Emanuel Rivers. Cryptic septic shock:
a subanalysis of early goal directed
therapy. Chest 2003;124:90s
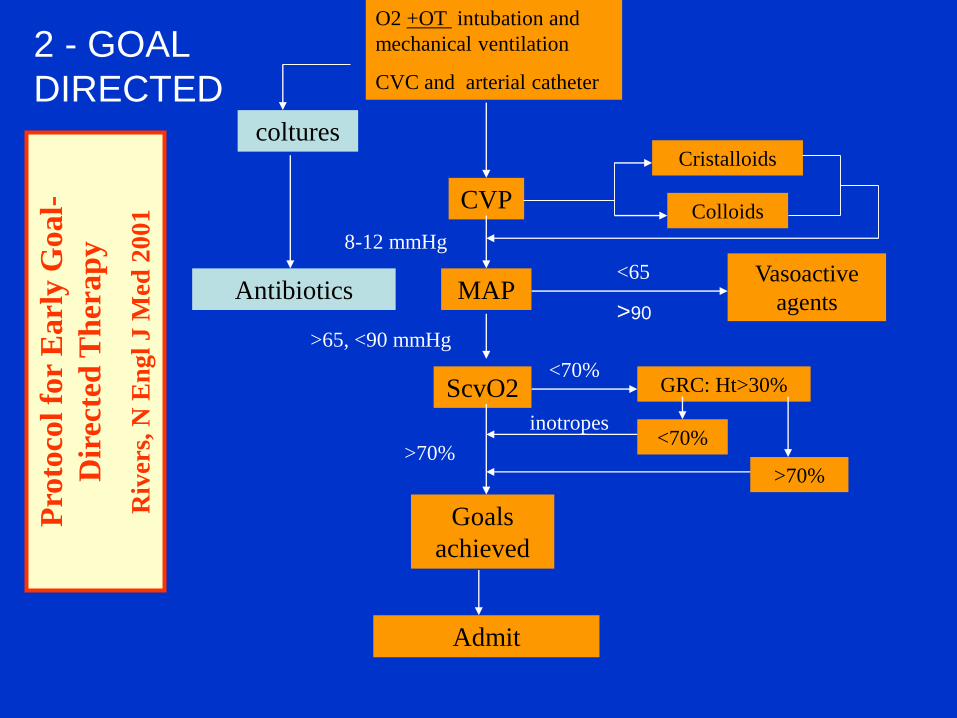
O2 +OT intubation and
mechanical ventilation
CVC and arterial catheter
CVP
MAP
ScvO2
Goals
achieved
Admit
Vasoactive
agents
Cristalloids
Colloids
8-12 mmHg
<65
>65, <90 mmHg
GRC: Ht>30%<70%
<70%
>70%
inotropes
>70%
Pro
toco
l fo
r E
arl
y G
oal-
Dir
ecte
d T
her
ap
y
Riv
ers,
N E
ng
l J M
ed 2
001
coltures
Antibiotics>90
2 - GOAL
DIRECTED

In-hospital mortality
(all patients)
0
10
20
30
40
50
60 Standard therapyEGDT
28-day mortality
60-day mortality
Mo
rtality
(%
)
The Importance of Early Goal-Directed
therapy
Adapted from Table 3, page 1374, with permission from Rivers E, Nguyen B, Havstad S,
et al. Early goal-directed therapy in the treatment of severe sepsis and septic shock. N
Engl J Med 2001; 345:1368-1377
46,5
30,5

Treatment administered (6 hrs)
0
10
20
30
40
50
60
70
Fluids x100ml
Blood % Dopa % Dobu %
EGDT
Controls
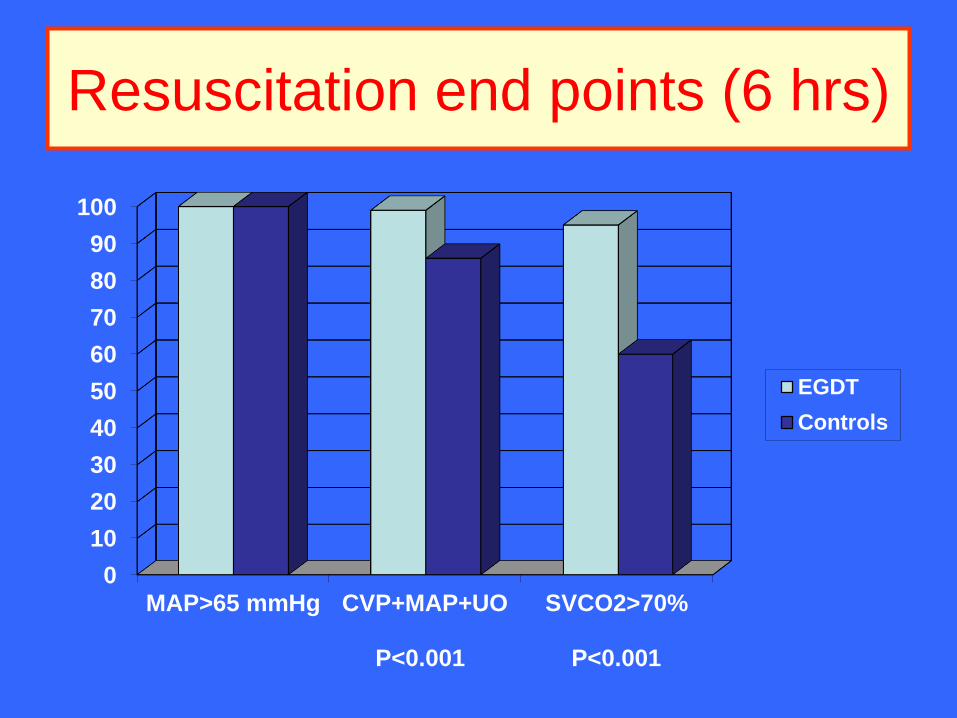
Resuscitation end points (6 hrs)
0
10
20
30
40
50
60
70
80
90
100
MAP>65 mmHg CVP+MAP+UO SVCO2>70%
EGDT
Controls
P<0.001P<0.001

Living with uncertainty
• Are you sure you want to place a CVC?
• Are you sure that CVP is a good parameter to assess fluid responsiveness?
• Are you ready to tolerate a low BP muchlonger (while you continue fluid infusions)?
• Are you ready to transfuse every patient with a Hct < 30%?
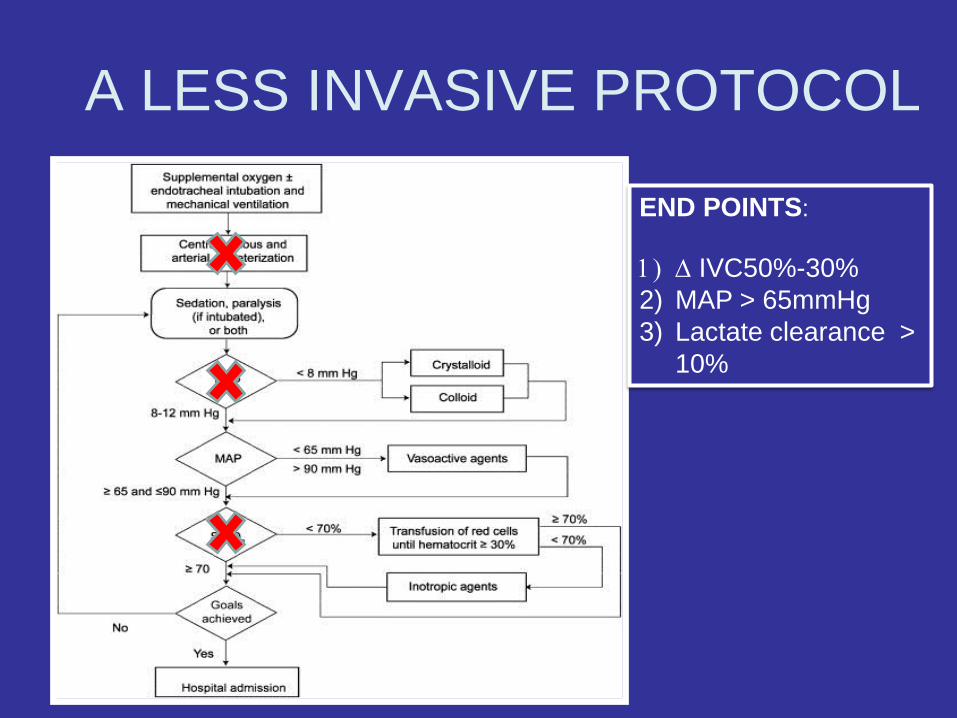
A LESS INVASIVE PROTOCOL
END POINTS:
1) D IVC50%-30%
2) MAP > 65mmHg
3) Lactate clearance >
10%
Turning to the literature
• New studies do not support EGDT as the only
possible approach
• Physiopathology must be kept intoconsideration
• Technology is evolving
Three options (1341 pts)
1. EGDT
2. Modified protocol. No CVP nor ScVO2 measurement. Fluid replenishment guided by clinical criteria alone . CVC only for difficultveins.
3. Wild card approach: «dealer’s choice»


Question marks
• Are the two trials comparable?
• Did they enroll similar populations?
• Do the PROCESS results mean that we
should quit EGDT?
• And now what?
The point of this study is that if you are aggressive with your resuscitation, it doesn'tmatter what you measure to tell you whetheryou have given enough fluid -- ScvO2, lactate, end-organ perfusion -- in terms of mental status or urine output. You need to continue to resuscitate the patient. You can't just leave themin the back. You can't just give them 500 cc of crystalloid and walk away.
Andy Shorr – Washington Hospital Center
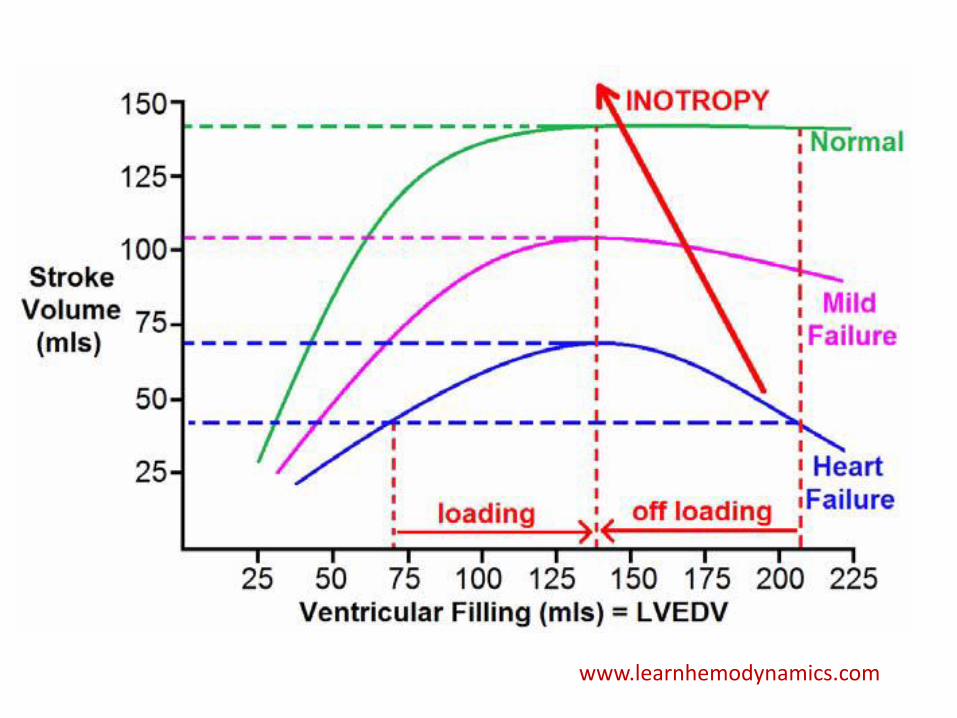
Fundamentally, the only reason to give any patient a fluid challenge is to increase their stroke volume
Marik PE. BJA 2014
Think in terms of stroke volume
www.learnhemodynamics.com

Marik PE. BJA 2014
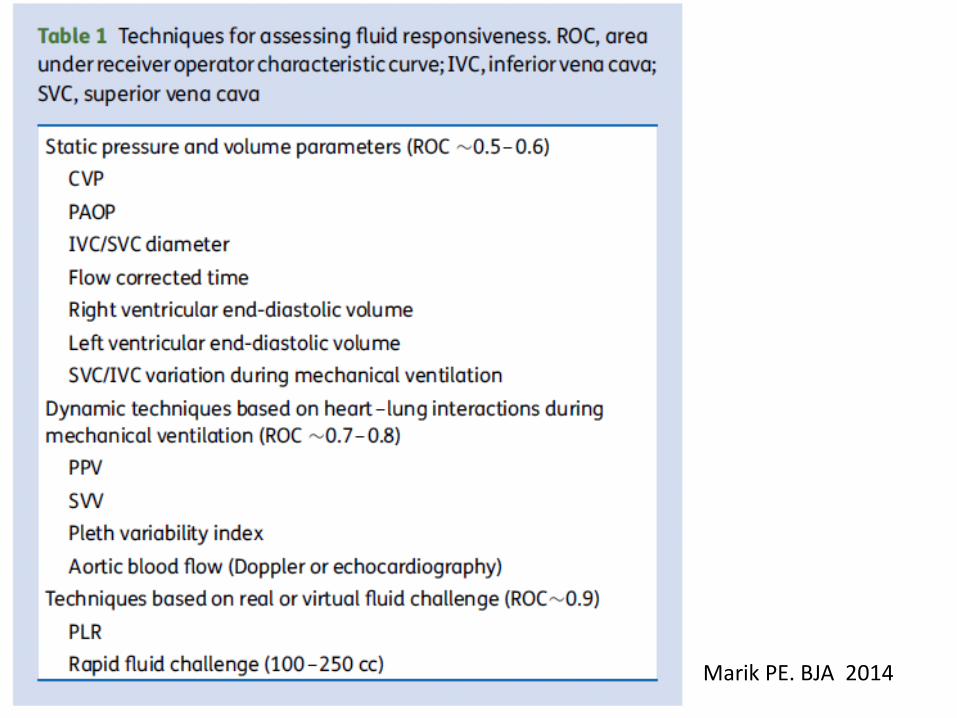
Marik PE. BJA 2014
Ultimately, only two techniques are currently
available that can be used to determine fluid
responsiveness with a high degree of
accuracy, namely the passive leg raising
(PLR) manoeuvre and the fluid
challenge.These techniques are best coupled
with minimally invasive cardiac output
monitors that can track changes in SV and cardiac output dynamically and in real time.

Possible approaches
• Invasive monitoring
• Echocardiography
• Non invasive monitoring (USCOM, Nikom, …)
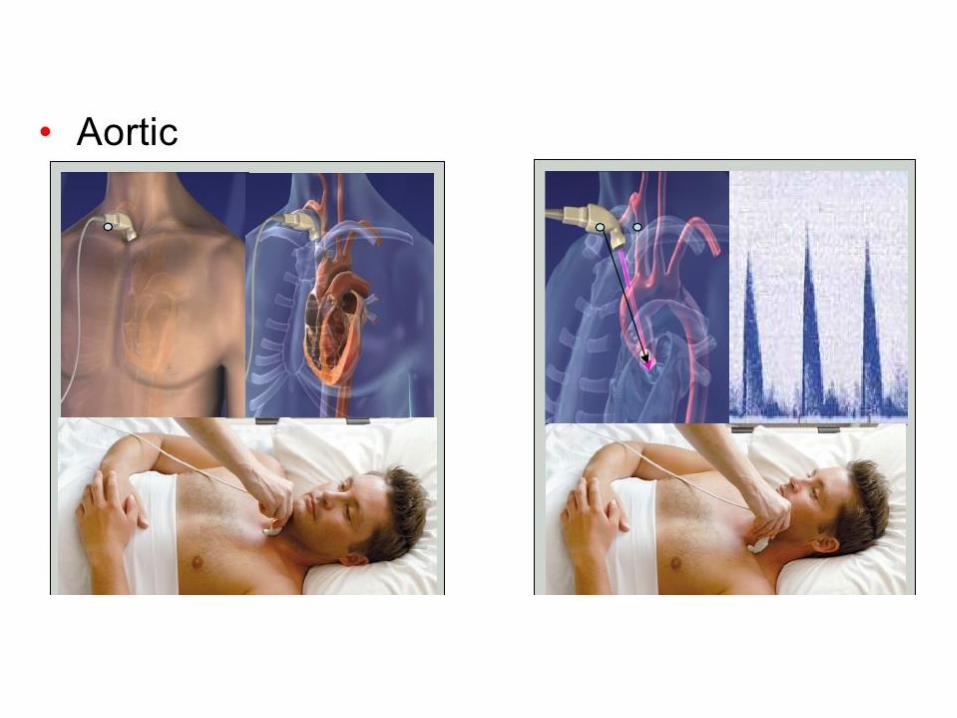
Cardiac output can be calculated by echo across any structure where one can measure cross sectional area and some information about velocity of blood flow. This could be the aorta, the pulmonic artery, or across any of the valves.
The easiest and least variable place to measure cardiac output is at the left ventricular outflow tract (LVOT). The LVOT diameter changes very little through systole and diastole and is assumed to be constant and closely approximating a circle in shape, however this introduces some error as it is in fact elliptical in many patients.
Echocardiographer.org

The USCOM and
HaemodynamicsA Guide for Junior Medical and Nursing
Staff
Brendan E Smith MB, ChB., FFA, RCS. Professor, School of Biomedical Sciences,
Charles Sturt University, Bathurst, Australia.
Specialist in Anaesthetics and Director of Intensive Care,
Bathurst Base Hospital, Bathurst, Australia.

Drug Inotropy Heart Rate SVR
Adrenaline ↑↑ ↑↑ ↑↑
Noradrenaline ↑ ↑ - ↓ ↑↑
Dopamine ↑↑ ↑ - ↑↑ ↑ - ↑↑
Dobutamine ↑↑ ↑ ↓
Conclusions - 1
• Sepsis is a time dependent disease. It shouldbe suspected and actively researched in ptswith signs and symptoms of infection and/or altered vitals signs and/or organ failure.
• Sepsis is a time dependent disease. It shouldbe treated early and aggressively.
Conclusions - 2
• Learn and practice the Sepsis Six. Whenstarted quickly they are probably the mostimportant interventions you can offer yourpatients.
• Have and follow a hospital AB protocol. Earlyand adequate antibiotic treatment isparamount.
Conclusions - 3
• Take a probe in your hands. Look for the septic source and take care of them asap.
• Take a probe in your hands. Use it to guide fluid infusion
• Take a probe in your hands. Have a look at the heart and reason in terms of stroke volume.
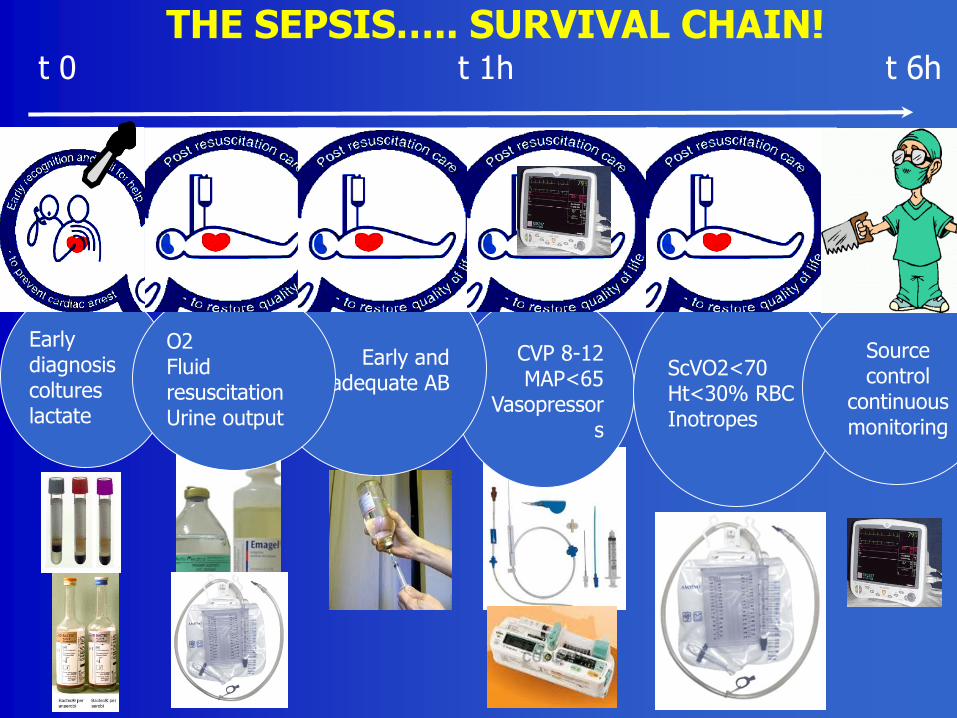
THE SEPSIS….. SURVIVAL CHAIN!
Early diagnosis coltureslactate
CVP 8-12MAP<65
Vasopressors
ScVO2<70Ht<30% RBCInotropes
Early and adequate AB
O2Fluid resuscitationUrine output
Source control
continuous monitoring
t 0 t 1h t 6h

83
THANK YOU