prevalence of bancroftian filariasis on the thai-myanmar...
TRANSCRIPT
ASIAN PACIFIC JOURNAL OF ALLERGY AND IMMUNOLOGY (2003) 21: 179-188
Prevalence of Bancroftian Filariasis onthe Thai-Myanmar Border
Surang Nuchprayoon 1.4, Vivornpun Sanprasere, Chantima Porksakorn3 and Issarang Nuchprayoon2,4
Lymphatic filariasis mainlycaused by Wuchereriabancrojti andBrugia malayi is still a major publichealth problem in the tropics andsubtropics.I The disease affects over120 million people in 73 countrieswith more than 40 million cases ofovert clinical disease? More than90% of the disease burden is due toW bancrojti. The disease pathologyis associatedwith inflammation and
fibrosis of the lymphatic system,resulting in blockage of the lym-phaticdrain.The majorityof infectedindividuals have asymptomatic mi-crofilaremiawhich makes the diseasedifficult to diagnose in the earlystages.
Lymphaticfilariasishas beenacknowledged by the World HealthOrganization (WHO) as a majorpublic health problem and targetedto be eliminated by the year 2020.3Therefore, control programs havebeen launched worldwide with anemphasis on community-wide treat-mentwith diethylcarbamazine(DEC)and ivermectin or albendazole.1 Toachieve this goal, effective control
SUMMARY To achieve the goal of eliminating lymphatic filariasis by the year2020, close monitoring systems and effective control strategies need to beimplemented and the real disease burden needs to be assessed. Bancroftianfilariasis is endemic at the Thai-Myanmar border. However, there are onlylimited data on the prevalence of this disease in Thailand available. Weemployed microscopic examination, together with ELlSA kits to detect W.bancrofti-specific Og4C3 circulating antigen and specific anti-filarial IgG4antibodies to determine the burden of bancroftian filariasis in an endemicarea at the Thai-Myanmar border in Umphang District, Tak province, Thailand.A total of 433 Thai-Karen blood samples were analyzed. The microfilarialrate determined by microscope was 6% and the W. bancrofti-specific Og4C3antigenemia rate was 22%, while the specific anti-filarial IgG4 antibody ratewas 54%. There were statistically significant higher levels of W. bancrofti-specific Og4C3 antigen in the microfilaremic-antigenemic group than in theamicrofilaremic-antigenemic group (unpaired Student's t-test; p < 0.001),similar to the specific anti-filarial IgG4 antibody results (unpaired Student'st-test; p < 0.001). A statistically significant correlation of moderate degreebetween the presence of W. bancrofti-specific Og4C3 antigen and of specificanti-filariallgG4 antibody was found in the amicrofilaremic group (r = 0.474,P < 0.001),but not in the microfilaremicgroup (r=0.291,P > 0.05).Ourstudyrevealed a very high prevalence of bancroftian filariasis in this endemicarea and thus emphasized the importance of using highly sensitive andspecific diagnostic tools to evaluate the true prevalence of the disease.
strategies and close monitoring sys-tems need to be implemented andthe real disease burden needs to beassessed. Close monitoring of theintervention programs requires sen-sitive and cost-effective diagnosticassays. The conventionalmethod fordiagnosis of lymphatic filariasis isby detecting microfilariae in noctur-nal peripheral blood.4-6The reason
for this is that, in most geographicalareas, W bancrojtimicrofilariaehavea nocturnal periodicity or subperi-odicity, with the highest concentra-
From the 10epartment of Parasitology,20epartment of Pediatrics, 3Chula MedicalResearch Center, Faculty of Medicine, and'Medical Microbiology Program, GraduateSchool, Chulalongkorn University, Bangkok10330, Thailand.Correspondence: Surang Nuchprayoon

180 NUCHPRAYOON, ET AL.
tion in the peripheral blood at night,and few or no microfilariae duringthe day.7 Besides being time-con-suming and tedious, the conventionalparasitological procedures fail toidentify amicrofilaremic infectionsor individuals with very low micro-filaria levels.8
Detection of the circulatingfilarial antigen has now emerged asan alternative method for the diag-.
fWb .fj"J:":' 69nosls 0 . ancroJtl 1ll1ectJon.'Like the conventional method, theantigen assay is a good indicator foractive infection. Commercial kits
utilizing specific monoclonal anti-bodies for W bancrojti antigen de-tection are now available.IO,11 An
enzyme-linked immunosorbent assay(ELISA) based on Og4C3 mono-clonal antibodyll has been used todiagnose microfilaremic as well asamicrofilaremic individuals with
high specificity and sensitivity.4,11-13The sensitivity of this antigen assayis the same whether serum samplesare collected during the day or atnight.14 Besides the Og4C3 ELISA,another antigen assay for the diag-nosis of W bancrojti has been de-veloped as immunochromatographic(ICT) Filariasis card.1OThe efficacyof the ICT Filariasis card is compa-rable to the W bancrojti-specificOg4C3 antigen test. 10 Due to theease of use, this card test is a prom-ising point-of-care (Poe) diagnostictool highly suitable for remote
1015-17 M. '
dareas. . oreover, It proVI esresults in 15 minutes using finger-prick blood. However, the W ban-crojti-specific Og4C3 ELISA showsa slightly higher sensitivityl6,18es-pecially in detecting amicrofilare-mics,18compared to the ICT Fila-riasis card test. For multiple sam-ple testing, such as during and aftermass treatment programs, the W
bancrojti-specific Og4C3 ELISA ismore practical. The Og4C3 ELISAseems to be highly valuable for largescale screening!7 as well. Therefore,it depends on the situation which ofthese two antigen tests is more ap-propriate to use.
Serological assays based onthe detection of anti-filarial IgGantibodies are widely used for epi-demiological and diagnostic pur-poses. The main advantage of theanti-filarial IgG antibody detectionis the ability to detect filarial infec-tion duringthe incubationperiod andin occult filariasis (tropical pulmo-nary eosinophilia [TPE]), in whichmicrofilariae are not found in the
peripheral blood. Furthermore, dueto the long persistenceof antibodies,past as well as current cases can bedetected by this ELISA. However,the anti-filarialantibodytest is knownto have a relatively low specificity,Specific subclasses of IgG anti-bodies have been shown to improvethe specificity over total IgG anti-bodies for the diagnosis of manyparasitic infections, such as ascaria-,19 h . . 2° I
'h
.SIS, ec IllOCOCCOSIS,els mallla-sis/1 and gnathostomiasis.22 Thespecific anti-filarial IgG4 antibodyhave also been shown to enhance
the sensitivity of the immunodiag-nostic assay for lymphatic filaria-sis.5,6,23-28However, the specificanti-filarial IgG4 antibody assayhas a lower specificity than theparasitological or antigenic diag-nostic techniques.29The serum lev-els of the specific anti-filarial IgG4antibodies are elevated in personswith active W bancrojti infection22-24
and decline following treatmentwith DEC.3o
In Thailand, lymphatic fila-riasis has been well controlled, re-
suiting in a Iow prevalence rate of1.62 per 100,000 population/I asassessed by the conventional mi-croscopic method. The data indicatethat only 86,000 individuals in 106sub-districts are at risk of acquiringlymphatic filariasis. Areas of activetransmission of bancroftian filaria-sis are limited to certain districts in
Tak, Kanchanaburi, and Mae Hong ISon provinces, located in the North-west of Thailand at the Thai-Myan-mar border, Individuals in endemicareas receive bi-annual DEC treat- I
ment and health education including Iprevention and control of lymphatic
I
'
filariasis from public health per-sonnel. Among the active transmis-sion areas of bancroftian filariasis
in Thailand, Umphang district inTak province, is considered to beone of the most afflicted, The mainreasons are its distant location, dif- I
ficult access and that it is coveredwith rain forests, Records from the
Thai Meteorological Department(TMD) during 1998to 2000 indicatethat Umphang district had higherannual rainfalls than Kanchanaburiand Mae Hong Son provinces.31Umphang district has about 1,399,5mm rainfall with a total of 164rainy days per year. Such conditionscreate many water reservoirs servingas breeding sites for Aedes niveus,the main mosquito vector for ban-croftian filariasis in Thailand.32However, very few studies on ban-croftian filariasis in this remoteareas have been done/3 and there-fore the epidemiology of the diseaseis poorly known. The real situationof lymphatic filariasis in endemicareas in Thailand has not been in-vestigated using highly sensitiveand specific tests like the W ban-crojti-specific Og4C3 circulatingantigen and the specific anti-filarialIgG4 antibody assays.

BANCROFTIANFILARIASIS IN THAILAND 181
To accurately assess thereal burden of the bancroftian fila-riasis situation, we studied theprevalence of bancroftian filariasisin a Thai-Karenpopulation residingin sub-districts of Umphang dis-trict, Tak province, Thailand, usingthe conventional microscopicmethod, the W. bancrofti-speCificOg4C3ELISA, and the ELISA foranti-filarial IgG4 antibodies, anddiscuss their results in relationshipto each other.
MATERIALS AND METHODS
Study area and population
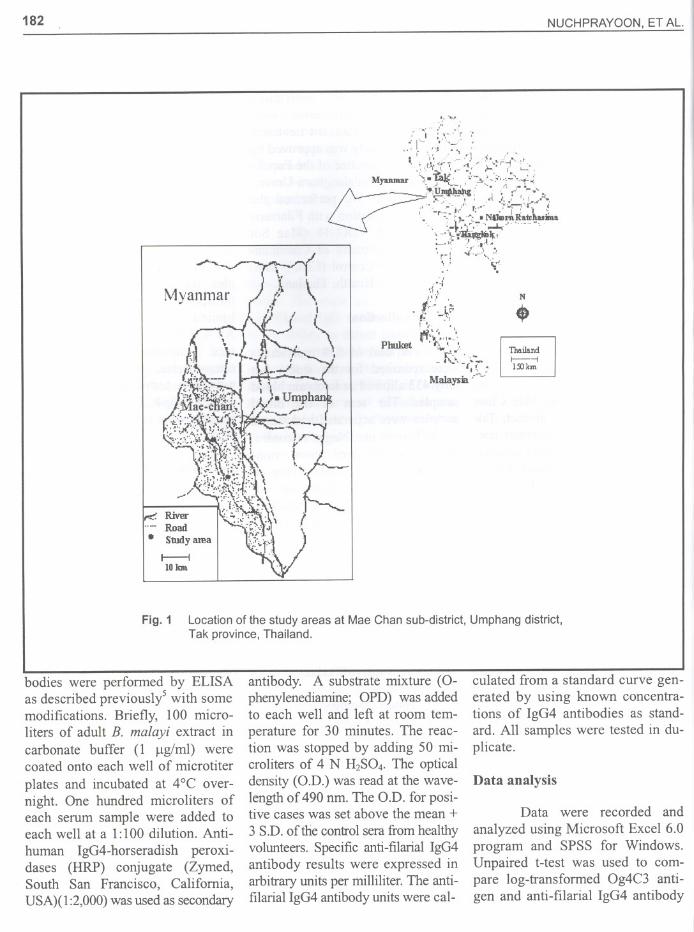
Two villages of Mae Chansub-district,Umphang district, Takprovinceat the Thai-Myanmar bor-der,Thailand(Fig. 1), were selectedfor the study.The Umphang districtis located about 165 km from MaeSot district of Tak province. How-ever,it takes about 4-6 hours to getthere from Mae Sot by a tortuoussecondary road. The Center of VectorBorne Disease Control (VDC) 18 islocated in Mae Sot district, about500 km northwest of Bangkok. Thevillagers were very cooperative andpleased with our visit.
Among the study popula-tion, 55% (238/433) were men and45% (195/433) were women. Themajority of the population wasbetween 15 and 30 years (44%).Nineteenpercent were children lessthan 15 years old. Most of individu-alslivinghereworkedon agriculture.
Verbal informed consent wasobtained from each individual or
child's parents or guardian in thepresence of two witnesses. All par-ticipants were informed about thepurpose of this study and the danger
of lymphatic filariasis. Individualswho were microfilaremic weretreated with the standard treatment
(DEC). This study was approved bythe Ethics Committee of the Facultyof Medicine, ChulalongkornUniver-sity, Bangkok. We performed thestudy in cooperation with FilariasisDivision, and VDC 18 (Mae Sotdistrict), Department of Communi-cable Disease Control (CDC), Min-istry of Public Health, Thailand.
Sample collection
A total of 539 individualswere recruited for the study, butonly 433 allowed us to obtain bloodsamples. The sera of the bloodsamples were separated and storedat -20°C until use. Negative controlsera were obtained from non-infected healthy people living innon-endemic areas. Sera from pa-tients infected with other parasites,diagnosed by stool examination35-36and Giemsa stain of thin and thickblood films,5,6,27,28,34including B.malayi, Onchocerca volvulus, Op-isthorchis viverrini, Strongyloidesstercoralis, Trichuris trichiura, Gi-ardia lamblia and hookworms,were also tested.
Detection of microfilariae
Blood samples were col-lected between 8.00-12.00p.m., thepreferential time for the detectionof the nocturnal subperiodic micro-filariae. Two to five milliliters ofvenous blood were obtained fromeach individual by a sterile tech-nique. For identification of micro-filariae, thick blood films were pre-pared in duplicate as described pre-viously.5,6,27,28,34Briefly, about 60microliters of each of the 433 bloodsamples were smeared onto micro-
scope slides in duplicate.After beingair-dried, the slides were stored atroom temperature until examinationin the laboratory. The microscopeslides were stained with Giemsa'stechnique. Species identificationwasperformed independently by 2 indi-viduals.
We had difficulties to beable to process all 433 blood sam-ples for all 3 tests, because oftransportation problems and thelimited amounts of blood obtained.All 433 blood samples were exam-ined microscopically for themicrofilariae, 265 blood sampleswere also tested for W. bancrofti-specific Og4C3 antigen and 178samples were tested by all 3 meth-ods.
Detection of W. bancrofti-specificOg4C3 antigen
The W. bancrofti-specificOg4C3 antigen was detected andmeasured by using a specificOg4C3monoclonal antibody-based sand-wich ELISA according to themanufacturer's instructions (Trop-Bio Pty Ltd, Townsville, Queen-sland, Australia). The results wereexpressed in arbitrary antigen unitsper milliliter. The antigen units werecalculated from a standard curvegenerat~d by using known concen-trations!of Onchocerca gibsoni an-tigen as standard. Positive sampleshad W. bancrofti-specific Og4C3antigen titers over 100 U/mI. Allsamples were performed in dupli-cate.
Detection of specific anti-filarialIgG4 antibodies
Detection and quantificationof the specific anti-filarial IgG4 anti-
182 NUCHPRAYOON. ET AL.
,-
Myanmar
t---ilOJan
-:-",
!I~,~~{ii~:,,{~.Myuunar ",."i"';'v:' ::-l'..I<;-,.,_.-'--+'-
~,.,~" . '- it .~
f?=c"U~:- ';';f--"'.,;-o
r-.: I' .-: J' , "I .r:.I"""r:~-"j/' t:-..' ;i'~"t:" l. -iJ~~I)""..,~~~~tt~iIna
\-'\';-~Ir.,; ,t' :.' ':,..1.."r-! :'::.-J ,='
\.' '...~,- "
,':1'',1 ':I':' ,
. ~~; ,J/;. .1,-
P W:}~,,::"huket ,~ '. ..:-- f;::,- ~~-....
(,!; ~Malaysia .-~--
N..ThaiJalldr---!13Jkm
Fig. 1 Location of the study areas at Mae Chan sub-district, Umphang district,Tak province, Thailand-
bodies were perfonned by ELISAas described previously5 with somemodifications. Briefly, 100 micro-liters of adult B. malayi extract incarbonate buffer (1 J.lg/ml) werecoated onto each well of microtiter
plates and incubated at 4°C over-night. One hundred microliters ofeach serum sample were added toeach well at a 1:100 dilution. Anti-human IgG4-horseradish peroxi-dases (HRP) conjugate (Zymed,South San Francisco, California,USA)( 1:2,000) was used as secondary
antibody. A substrate mixture (0-phenylenediamine; OPD) was addedto each well and left at room tem-
perature for 30 minutes. The reac-tion was stopped by adding 50 mi-croliters of 4 N H2SO4-The opticaldensity (O.D.) was read at the wave-length of 490 nrn. The O.D. for posi-tive cases was set above the mean +3 SD. of the control sera from healthyvolunteers. Specific anti-filarial IgG4antibody results were expressed inarbitrary units per milliliter. The anti-filarial IgG4 antibody units were cal-
culated from a standard curve gen-erated by using known concentra-tions of IgG4 antibodies as stand-ard. All samples were tested in du-plicate.
Data analysis
Data were recorded andanalyzed using Microsoft Excel 6.0program and SPSS for Windows.Unpaired Hest was used to com-pare log-transfonned Og4C3 anti-gen and anti-filarial IgG4 antibody
BANCROFTIAN FILARIASIS IN THAILAND 183
levels between amicrofilaremics and
microfilaremics with a p < 0.05taken as statistically significant. Thecorrelation between the specificanti-filarial IgG4 antibody units andthe W bancrojti-specific Og4C3 an-tigen units was determined by Pear-son's correlation test. Furthermore,Cohen's kappa coefficient .wascomputed to assess the agreementbetween the positive/negative re-sults from the W bancrojii-specificOg4C3 antigen assay and that fromthe specific anti-filarial IgG4 anti-body assay.
RESULTS
Prevalence of bancroftian filaria-sis assessed by microfilarial rate
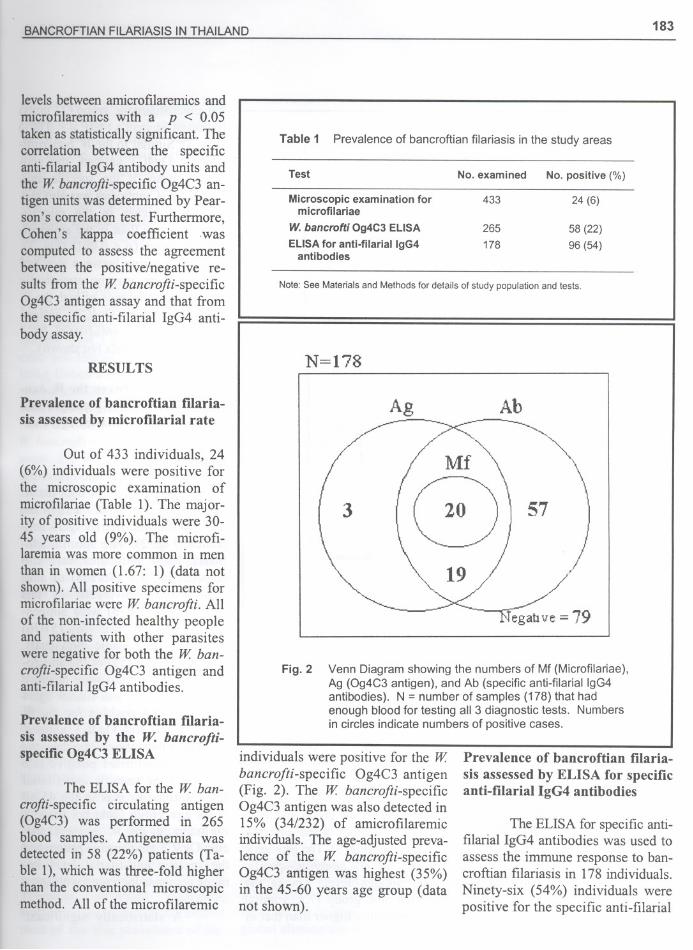
Out of 433 individuals, 24(6%) individuals were positive forthe microscopic examination ofmicrofilariae (Table 1). The major-ity of positive individuals were 30-45 years old (9%). The microfi-laremiawas more common in menthan in women (1.67: 1) (data notshown).All positive specimens formicrofilariaewere W bancrojii. Allof the non-infected healthy peopleand patients with other parasiteswere negative for both the W ban-crojii-specific Og4C3 antigen andanti-filarialIgG4 antibodies.
Prevalence of bancroftian filaria-sis assessed by the W. bancrofti-specificOg4C3 ELISA
The ELISA for the W ban-crojii-specific circulating antigen(Og4C3) was performed in 265blood samples. Antigenemia wasdetected in 58 (22%) patients (Ta-
. ble 1), which was three-fold higherthan the conventional microscopicmethod. All of the microfilaremic
Table 1 Prevalence of bancroftian filariasis in the study areas
Test
Microscopic examination formicrofilariae
W. bancrofti Og4C3 ELlSA
ELlSA for anti-filariallgG4antibodies
Note: See Materials and Methods for details of study population and tests.
N = 178
Ag
3 57
egahve = 79
Venn Diagram showing the numbers of Mf (Microfilariae),Ag (Og4C3 antigen), and Ab (specific anti-filariallgG4antibodies). N = number of samples (178) that hadenough blood for testing all 3 diagnostic tests. Numbersin circles indicate numbers of positive cases.
Fig. 2
individuals were positive for the Wbancrojii-specific Og4C3 antigen(Fig. 2). The W bancrojii-specificOg4C3 antigen was also detected in15% (34/232) of amicrofilaremiciridividuals.The age-adjustedpreva-lence of the W bancrojii-specificOg4C3 antigen was highest (35%)in the 45-60 years age group (datanot shown).
Prevalence of bancroftian filaria-sis assessed by ELISA for specificanti-filarial IgG4 antibodies
The ELISA for specific anti-filarial IgG4 antibodies was used toassess the immune response to ban-croftian filariasis in 178 individuals.Ninety-six (54%) individuals werepositive for the specific anti-filarial
No. examined No. positive (%)
433 24 (6)
265 58 (22)178 96 (54)
184NUCHPRAYOON, ET AL.
100000
----- ----
1::~~1-----~~---;~:3-ucits+"
~ 1000~'"bJ)
~ lOO
10
t
IGM-23ucits T
I
AmicrofIlaremics
I I
MicrofIlaremics
lOO
".~;=J
~ 100
~~
i+
GM-13ucits -I--
+
;f
GM-7units +
MicrofIlaremics AmicrofIlaremics
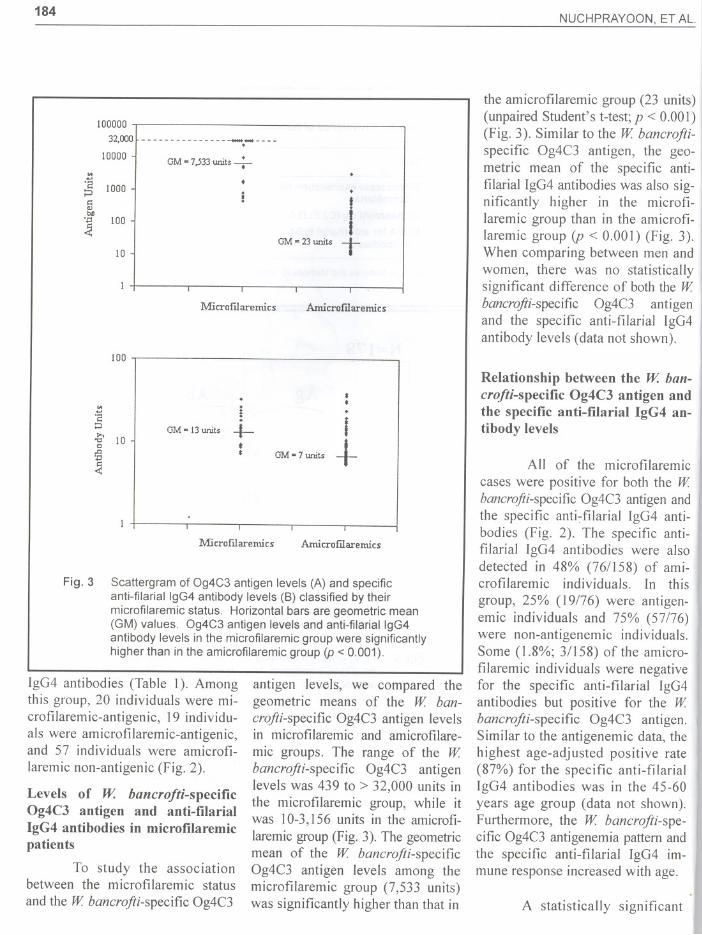
Fig. 3
I
Scattergram of Og4C3 antigen levels (A) and specificanti-filariallgG4 antibody levels (8) classified by theirmicrofilaremic status. Horizontal bars are geometric mean(GM) values. Og4C3 antigen levels and anti-filariallgG4antibody levels in the microfilaremic group were significantlyhigher than in the amicrofilaremic group (p < 0.001).
IgG4 antibodies (Table I). Amongthis group, 20 individuals were mi-crofilaremic-antigenic, 19 individu-als were amicrofilaremic-antigenic,and 57 individuals were amicrofi-
laremic non-anti genic (Fig. 2).
Levels of W. bancrojti-specificOg4C3 antigen and anti-filarialIgG4 antibodies in microfilaremicpatients
To study the associationbetween the microfilaremic status
and the W bancrojii-specific Og4C3
antigen levels, we compared thegeometric means of the W ban-crojii-specific Og4C3 antigen levelsin microfilaremic and amicrofilare-mic groups. The range of the Wbancrojii-specific Og4C3 antigenlevels was 439 to > 32,000 units inthe microfilaremic group, while itwas 10-3,156 units in the amicrofi-laremicgroup(Fig. 3). The geometricmean of the W bancrojii-specificOg4C3 antigen levels among themicrofilaremic group (7,533 units)was significantly higher than that in
the amicrofilaremic group (23 units)(unpaired Student's t-test;p < 0.001)(Fig. 3). Similar to the W bancrojii-specific Og4C3 antigen, the geo-metric mean of the specific anti-filarial IgG4 antibodies was also sig-nificantly higher in the microfi-laremic group than in the amicrofi-laremic group (p < 0.001) (Fig. 3).When comparing between men andwomen, there was no statisticallysignificant difference of both the Wbancrojii-specific Og4C3 antigenand the specific anti-filarial IgG4 Iantibody levels (data not shown).
Relationship between the W. ban-crofti-specific Og4C3 antigen andthe specific anti-filarial IgG4 an-tibody levels
All of the microfilaremiccases were positive for both the Wbancrojii-specificOg4C3 antigen andthe specific anti~filarial IgG4 anti-bodies (Fig. 2). The specific anti-filaria! IgG4 antibodies were alsodetected in 48% (76/158) of ami-crofilaremic individuals. In thisgroup, 25% (19/76) were antigen-emic individuals and 75% (57/76)were non-antigenemic individuals.Some (1.8%; 3/158) of the amicro-filaremic individuals were negativefor the specific anti-filaria! IgG4antibodies but positive for the Wbancrojii-specific Og4C3 antigen.Similar to the antigenemic data, thehighest age-adjusted positive rate(87%) for the specific anti-filaria!IgG4 antibodies was in the 45-60years age group (data not shown).Furthermore, the W bancrojii-spe-cific Og4C3 antigenemia pattern andthe specific anti-filarial IgG4 im-mune response increased with age.
A statistically significant
BANCROFTIAN FILARIASIS IN THAILAND 185
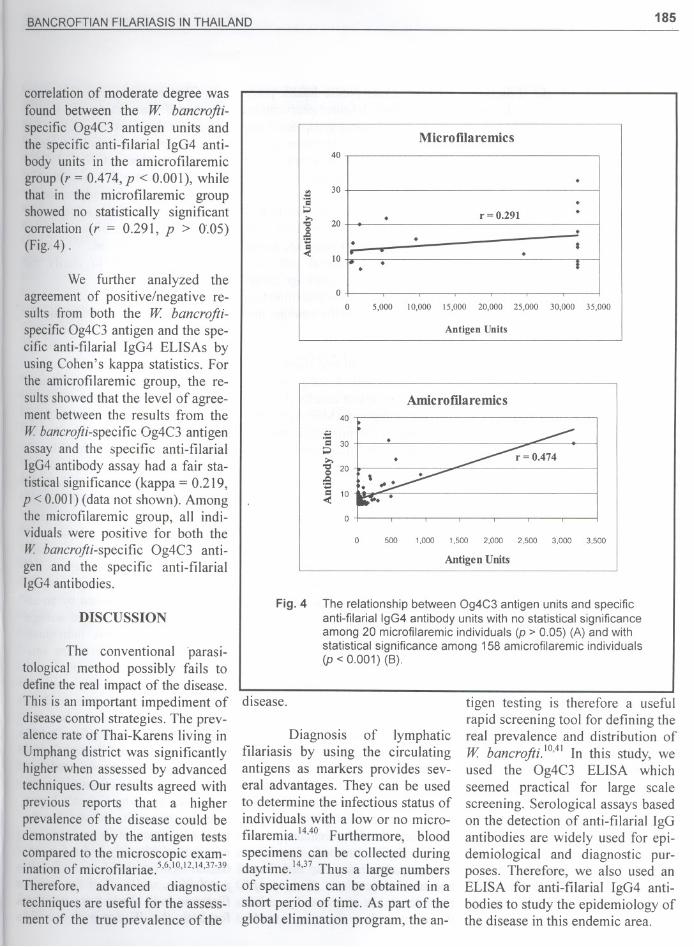
correlationof moderate degree wasfound between the W bancrojti-specific Og4C3 antigen units andthe specific anti-filarial IgG4 anti-body units in the amicrofilaremicgroup (r = 0.474,p < 0.001), whilethat in the microfilaremic groupshowed no statistically significantcorrelation(r = 0.291, P > 0.05)(Fig.4) .
We further analyzed theagreement of positive/negative re-sults from both the W bancrojti-specificOg4C3antigen and the spe-cific anti-filarial IgG4 ELISAs byusing Cohen's kappa statistics. Forthe amicrofilaremic group, the re-sultsshowedthat the level of agree-ment between the results from the
W bancrojti-specificOg4C3 antigenassay and the specific anti-filarialIgG4antibodyassay had a fair sta-tisticalsignificance(kappa = 0.219,p < 0.001)(data not shown). Amongthe microfilaremic group, all indi-viduals were positive for both theW bancrojti-specific Og4C3 anti-gen and the specific anti-filarialIgG4antibodies.
DISCUSSION
The conventionalparasi-tological method possibly fails todefine the real impact of the disease.This is an important impediment ofdisease control strategies. The prev-alence rate of Thai-Karens living inUmphang district was significantlyhigher when assessed by advancedtechniques. Our results agreed withprevious reports that a higherprevalence of the disease could bedemonstrated by the antigen testscompared to the microscopic exam-ination of microfilariae. 5,6,10,12,14,37-39
Therefore, advanced diagnostictechniques are useful for the assess-ment of the true prevalence of the
Microfilaremics
Fig. 4
00 5,000 10,000 15,000 20,000 25,000 30,000 35,000
Antigen Units
40
Amic ro fila re mic s
...'8 30;;.J....-g 20,.Q<=1:1 10-<
0
0 500 1,000 1,500 2,000 2,500 3,000 3,500
Antigen Units
The relationship between Og4C3 antigen units and specificanti-filariallgG4 antibody units with no statistical significanceamong 20 microfilaremic individuals (p > 0.05) (A) and withstatistical significance among 158 amicrofilaremic individuals(p < 0.001) (B).
disease.
Diagnosis of lymphaticfilariasis by using the circulatingantigens as markers provides sev-eral advantages, They can be usedto determine the infectious status ofindividuals with a Iow or no micro-filaremia.14,4OFurthermore, bloodspecimens can be collected duringdaytime.14,37Thus a large numbersof specimens can be obtained in ashort period of time. As part of theglobal elimination program, the an-
tigen testing is therefore a usefulrapid screening tool for defining thereal prevalence and distribution ofW bancrojti.10,41In this study, weused the Og4C3 ELISA whichseemed practical for large scalescreening. Serological assays basedon the detection of anti-filarial IgGantibodies are widely used for epi-demiological and diagnostic pur-poses. Therefore, we also used anELISA for anti-filarial IgG4 anti-bodies to study the epidemiology ofthe disease in this endemic area.
40
'" 30:!::1:1
;;J,.,
20"ClQ
1:1-<
10
.
.. r =0,291 .. . ." . 8
. .. !

186 NUCHPRAYOON, ET AL.
As part of the FilariasisControl Program in Thailand, DECmass treatment is performed every6 months in endemic areas, whileprevalence assessment is performedrandomly in some villages. Thestudy area selected is determined bythe prevalence of the disease duringthe past years. Sometimes the studyarea is expandedto cover more areas.However, the data collected overseveral years is used to determinethe overall situation of the disease in
each endemic area. The prevalenceof bancroftian filariasis in this en-demic area during the years 1992-1999 was 0.42-2.97%31 using theconventional microscopic method.
Very few studies on theprevalence of bancroftian filariasisin endemic areas of Thailand have
been reported.33We found that theprevalence of bancroftian filariasisin Mae Chan sub-district was 6%by the microscopic method, com-pared to 22% by the W bancrojti-specific Og4C3 antigen test, and to54% by the anti-filarial IgG4 anti-body assay. A previous study, usingthe microscopic method in com-parison to another antigen test (theICT Filariasis card test) showed asimilar pattern of disease burden.33Therefore, it is evident that the mi-croscopic method underestimatedthe prevalence of filariasis in thispopulation more than three-fold.Our data also indicated that one-fifth of the study population hadactive W bancrojti infection as as-sessed by the antigen assay. Fur-thermore, the 54% prevalence as-sessed by the specific IgG4 anti-body rate signified that more thanhalf of the population were eitheractively infected or had had a pastinfection of bancroftian filariasis.The high burden of the disease inthis endemic area should be consid-
ered a serious public health prob-lem needing definite intervention.The high-prevalencegroup accordingto our study was older than previ-ously reported.31The prevalence ofbancroftian filariasis determined bythe W bancrojti-specific Og4C3antigen and the specific anti-filarialIgG4 antibodies in our study washighest in the 45-60 years age group,while the microfilarial rate washighest in the 30-45 years age group.This seems to imply that infectionrates were lower in the younger agegroups.
Patients in our study couldbe classified into 4 subgroups ac-cording to the test results (Fig. 2).The first subgroup (Mf+/Ag+/Ab+)consisted of 20 microfilaremic in-dividuals with high levels of Wbancrojti-specific Og4C3 antigenand anti-filarial IgG4 antibodies.Obviously, this subgroup representsactive W bancrojti infections withhigh levels of microfilariae. Thesecond subgroup (Mf-/Ag+/Ab+)consisted of 19 amicrofilaremic in-dividuals with W bancrojti-specificOg4C3 antigenemia and anti-filarialIgG4 antibody responses. This sub-group may represent active W ban-crojti infections with adult wormsbut producing too few or no micro-filariae. The third subgroup (Mf-/Ag-/Ab+) consisted of 57 amicro-filaremic individuals with variablelevelsof anti-filarialIgG4 antibodies,without detectable Og4C3 antigenlevels. This subgroup possibly rep-resents past-infected individualswho had already eliminated the Wbancrojti-specific Og4C3 antigenfrom their blood, but remained anti-filarial IgG4 antibody positive.Alternatively, this group may havehad too Iow levels of W bancrojtiparasites to be detected by eitherthe microscopicor the antigen meth-
ods. The last subgroup (Mf-/Ag+/Ab-) had W bancrojti-specificOg4C3antigen in the blood circulation, buthad no detectable microfilaremia,nor a detectable anti-filarial IgG4I
antibody response. It is possible thatthis group was in the early period, orwindow period of the infection, or Ihad too low levels of antibody re-sponse to be detected.25,41Furtherstudies are needed to clarify theissues raised.
From Fig. 4, a statisticallysignificant correlation of moderatedegree was found between the Wbancrojti-specific Og4C3 antigenunits and the anti-filarial IgG4 anti-body units of the amicrofilaremicgroup (r = 0.474, P < 0.001). How-ever, there was no statistically sig-nificant correlation in the microfi-
laremic group (r = O.291,p > 0.05).Some microfilaremic individualshad very high levels of W bancrojti-specific Og4C3 antigen with Iowlevels of specific anti-filarial IgG4antibodies (Fig. 4). These resultswere similar to previous reports.25,42It has been proposed that this dis-crepancy is either caused by an as-sociation of the increased antigenload in microfilaremic individualswith a down-regulation of the anti-body production,42or simply by theearly infectious stage of the micro-filaremic individuals tested. How-ever, when the agreement betweenthe W bancrojti-specific Og4C3antigen and the specific anti-filarialIgG4 antibody results was analyzedin terms of number of positive/nega-tive cases by using Cohen's kappastatistic, the results showed that thelevel of agreement in amicrofilare-mic individuals only had a fair sta-tistical significance (kappa = 0.219,P < 0.001), while all of the micro-filaremic individuals were positivefor both the W bancrojti-specific
BANCROFTIAN FILARIASIS IN THAILAND 187
Og4C3antigenand the specificanti-filarial IgG4 antibodies (100%agreement).This data suggested thatthe W bancrofti-specific Og4C3antigenand the specific anti-filarialIgG4 antibodies were correlatedwithmicrofilaremicstatus.When thedata were analyzed in terms ofmagnitudeof W banerofti-specificOg4C3 antigen levels and specificanti-filarial IgG4 antibody levels,microfilaremicpatients had signifi-cantly higher W banerofti-specificOg4C3antigen levels than amicro-filaremicpatients (p < 0.001) (Fig.3). This could be explained by thatthe parasite burden in microfilare-mics was higher, therefore, moreantigens were released into thebloodcirculation.Similar to the W
bancrofti-specific Og4C3 antigenunits, the microfilaremic patientshad higher levels of specific anti-filarial IgG4 antibodies than ami-crofilaremicpatients with statisticalsignificance(p < 0.001) (Fig. 3).Moreover,we found that the spe-cific anti-filarial IgG4 antibodylevels increased with the W ban-erafti-specific Og4C3 antigen lev-els in both amicrofilaremic and mi-crofilaremic individuals. Our re-sults showed that both the W ban-erofti-specific Og4C3 antigenemiaand the specific anti-filarial IgG4antibodies correlated with the mi-crofilaremiastatus.Furthermore,ourdata supported that both the Wbanerofti-specific Og4C3 antigenlevels, and the specific anti-filarialIgG4 antibody levels correlatedwith active infection?5
Our data showed a highprevalence of bancroftian filariasisin the endemic area investigatedemphasizingthe importanceof closemonitoring of the disease in thisarea. To monitor and evaluate theelimination program of lymphatic
filariasis, the use of advanced tech-niques with a high sensitivity andspecificity is necessary. Further-more, the test method used shouldbe practical for a field study settingin that a lot of samples can be eas-ily tested and blood samples takenat any time of the day. Finally, it isalso necessary to improve theaccess for people to health careproviders, as well as the access forthe public health personnel to theremote villages in order to providemass treatment as well as educationfor disease control.
ACKN0 WLEDGMENTS
We are grateful for the sup-port from the Thailand ResearchFund (TRF) and the UNDP/WorldBank/WHO Special Program forResearch and Training in TropicalDiseases. Ms. Vivornpun Sanprasertand Ms. Chantima Porksakorn arePh.D. students in the Royal GoldenJubilee (RGJ) Ph.D. Program sup-ported by TRF. We would like tothank Professor Dr. Yong Poovora-wan (Faculty of Medicine, Chula-longkorn University), and Dr. Sara-vudh Suwanadabba (Ministry ofPublic Health) for their helpful ad-vice and field support.We are thank-ful to Ms. Kobkarn Karnjanopas forco-ordination in the field, to Ms.Songpun Sangprkan,Ms. Alisa Jun-pee, and Ms. Chantharat Krainarafor technical assistance. We alsothank Ms., Jiraporn Songtrus forhistorical data and all the healthpersonnel fTom the Vector-borneDiseases Center 18 and the Filaria-
sis Division, CDC Department,Ministry of Public Health, as wellas the staffs at the Department ofParasitology, Faculty of Medicine,Chulalongkorn University for theirskilled assistance in the field andlaboratorywork.
REFERENCES
1. Ottesen EA, Duke BO, Karam M,Behbehani K. Strategiesand tools for thecontrol/elimination of lymphatic filaria-sis. Bull WHO 1997; 75: 491-503.
2. Michael E, Bundy DA, Grenfell BT.Re-assessing the global prevalence anddistribution of lymphatic filariasis.Parasitology 1996; 112: 409-28,
3, Behbehani K. Candidate parasitic dis-eases, Bull WHO 1998; 76 (Suppl 2):64-7,
4, Turner P, Copeman B, Gerisi D,SpeareR. A comparison of the Og4C3 antigencapture ELISA, the Knott test, an IgG4assay and clinical signs, in the diagno-sis of bancroftian filariasis. Trop MedParasitol 1993;44: 45-8,
5. Triteeraprapab S, Nuchprayoon 1,Pork-sakorn C, Poovorawan Y, Scott AL,High prevalenceof Wuchereriabancroftiinfection among Myanmar migrants inThailand, Ann Trop Med Parasitol2001; 95: 535-8,
6, Triteeraprapab S, Songtrus J. Highprevalence of bancroftian filariasis inMyanmar-migrant workers: a study inMae Sot district, Tak province, Thai-land, J Med Assoc Thai 1999;82: 734-9.
7, Simonsen PE, Meyrowitsch DW Ban-croftian filariasis in Tanzania: specificantibody responses in relation to long-term observations on microfilaremia.Am J Trop Med Hyg 1998;59: 667-72.
8. Chanteau S, Plichart R, Spiegel A,Martin PM, Cartel JL Diagnostic valuesofELISA-lgG4 as compared to ELISA-IgG and indirect immunofluorescence,for the routine diagnosis of bancroftianfilariasis in the South Pacific, Applica-tion on capillary blood collected on fil-ter paper, Trop Med Parasitol 1991; 42:339-42,
9, Itoh M, Gunawardena NK, Qiu XG,Weerasooriya MV, Kimura E, The useof whole blood absorbed on filter paperto detect Wuchereria bancrofti circu-lating antigen, Trans R Soc Trop MedHyg 1998;92: 513-5,
IQ, Weil GJ, Lammie PJ, WeissN, The ICTFilariasis test: a rapid-format antigentest for diagnosis of bancroftian filaria-sis. Parasitol Today 1997; 13:401-4,
11, More SJ, Copeman DB, A highly spe-cific and sensitive monocIonal anti-body-based ELISA for the detection ofcirculating antigen in bancroftian fila-riasis. Trop Med Parasitol 1990; 41:403-6.
188NUCHPRAYOON, ET AL.
12.Simonsen PE, Dunyo SK. Comparativeevaluation of three new tools for diag-nosis of bancroftian filariasis based ondetection of specific circulating anti-gens. Trans R Soc Trop Med Hyg 1999;93: 278-82.
13. Nuchprayoon S, Yentakam S, Sangpra-karn S, Junpee A. Endemic bancroftianfilariasis in Thailand: detection byOg4C3 antigen capture ELISA an<ithepolymerase chain reaction. J Med As-soc Thai 2001; 84: 1300-7.
14. Lammie PJ, Hightower AW, EberhardML. Age-specific prevalence of antige-nemia in a Wuchereria bancrofti-exposed population. Am J Trop MedHyg 1994; 51: 348-55.
15. Njenga SM, Wamae CN. Evaluation ofICT filariasis card test using wholecapillary blood: comparison with Knott'sconcentration and counting chambermethods. J Parasitol2001; 87: 1140-3.
16. Freedman DO, de Almeida A, MirandaJ, Plier DA, Braga C. Field trial of arapid card test for Wuchereria ban-crofti. Lancet 1997; 350: 1681.
17. Bhumiratana A, Koyadun S, Rojana-premsuk J, Suvannadabba S. Diagnosisof Wuchereria bancrofti infection inendemic populations: diagnostic ap-proaches to control and elimination.Mahidol J 2000; 7: 101-7.
18. Nuchprayoon S, Porksakorn C, JunpeeA, Sanprasert V. Comparative assess-ment of the Og4C3 ELISA to ICT Fila-riasis test: a study in Myanmar migrantsof Thailand. Asian Pac J Allergy. 2003;[in press].
19. Chatterjee BP, Santra A, Karmakar PR,Mazumder ON. Evaluation of IgG4 re-sponse in ascariasis by ELISA for sero-diagnosis. Trop Med Int Health 1996;I: 633-9.
20. Grimm F, Maly FE, Lu J, Llano R.Analysis of specific immunoglobulin Gsubclass antibodies for serological di-agnosis of echinococcosisby a standardenzyme-linked immunosorbent assay.Clin Diagn Lab Immunol1998; 5: 613-6.
21. Anam K, Afrin F, Banerjee 0, Pra-manik N, Guha SK, Goswami RP,Gupta PN, Saha SK,Ali N. Immuno-globulin subclass distribution and diag-nostic value of LeishmaJia donovaniantigen-specific immunoglobulin G3 inIndian kala-azar patients. Clin DiagnLab Immunol1999; 6: 231-5.
22. Nuchprayoon S, Sanprasert V, Suntra-vat M, Kraivichian K, SaksirisampantW, Nuchprayoon I. Study of specific
IgG subclass antibodies for diagnosis ofGnathostoma spinigerum. Parasitol Res2003; 91: 137-43.
23. Ottesen EA, Skvaril F, Tripathy SP,Poindexter RW,Hussain R. Prominenceof IgG4 in the IgG antibody response tohuman filariasis. J Immunol 1985; 134:2707-12.
24. Lal RB, Ottesen EA. Enhanced diag-nostic specificity in human filariasis byIgG4 antibody assessment. J Infect Dis1988; 158: 1034-7.
25. Kwan-Lim GE, Forsyth KP, MaizelsRM. Filarial-specific IgG4 responsecorrelates with active Wuchereriabancrofti infection. J Immunol 1990;145: 4298-305.
26. Theodore JG, Kaliraj P, JayachandranS, Jayaraman K. Cloning, over-expres-sion and evaluation of a recombinantfusion protein of Wuchereria bancroftitowards its application as a diagnosticagent for bancroftian filariasis. Parasi-tology 1993; 106:413-20.
27. Triteeraprapab S, Thumpanyawat B,Sanprakarn S. Wuchereria bancrofti-specific circulating antigen for diagno-sis of bancroftian filariasis. Chula MedJ 1998;42: 267-77.
28. Triteeraprapab S, Karnjanopas K,Porksakorn C, Sai-Ngam A, YentakamS, Loymak S. Lymphatic filariasiscaused by Brugia malayi in an endemicarea of Narathiwat Province, Southernof Thailand. J Med Assoc Thai 2001; 84(Suppll): SI82-8.
29. Chanteau S, Glaziou P, Moulia-Pelat JP,Plichart C, Luquiaud P, Cartel JL. Lowpositive predictive value of anti-Brugiamalayi IgG and IgG4 serology for thediagnosisof Wuchereriabancrofti.TransR Soc Trop Med Hyg 1994;88: 661-2.
30. Kurniwan AA, Atkinson R, Sartono E,Partono F, Yazdanbakhsh M, MaizelsRM. Differential decline in filiria-specific IgGI, IgG4, and IgE antibodiesin Brugia malayi-infected patients afterdiethylcarbamazine chemotherapy.J In-fect Dis 1995; 172: 1567-72.
31. Filariasis Division. CDC Department,Ministry of Public Health, Thailand.Annual Report. 1992-2001(in Thai).
32. Filariasis Division. Elimination pro-gram for lymphatic filariasis. FilariasisDivision, CDC Department, Ministry ofPublic Health, Thailand 2000 (in Thai).
33. Bhumiratana A, Koyadun S, Suvannad-abba S, Karnjanopas K, RojanapremsukJ, Buddhirakkul P, Tantiwattanasup W.Field trial of the ICT filariasis for diag-
nosis of Wuchereriabancrofti infectionsin an endemic population of Thailand.Southeast Asian J Trop Med PublicHealth 1999;30: 562-8.
34. Triteeraprapab S, Kanjanopas K, Su-wannadabba S, Sangprakarn S, Poo-vorawan Y, Scott AL. Transmission ofthe nocturnal periodic strain of Wu-chereria bancrofti by Culex quinque-fasciatus: establishing the potential forurban filariasis in Thailand. EpidemiolInfect 2000; 125:207-12.
35. Triteeraprapab S, Nuchprayoon I. Eo-sinophilia, anemia and parasitism in arural region of northwest Thailand.Southeast Asian J Trop Med PublicHealth 1998;29: 584-90.
36. Nuchprayoon S, Siriyasatien P, Kraivi-chian K, Porksakorn C, Nuchprayoon I.Prevalence of parasitic infections amongThai patients at the King Chulalong-korn Memorial Hospital, Bangkok,Thailand. J Med Assoc Thai 2002; 85(SupplI): S415-23.
37. Weil GJ, Jain DC, Santhanam S, Mal-hotra A, Kumar H, Sethumadhavan KY.Liftis F,Ghosh TK. A monoclonal anti-body-based enzyme immunoassay fordetecting parasite antigenemia in ban-croftian filariasis. J Infect Dis 1987;156: 350-5.
38. Rocha A, Addiss 0, Ribeiro ME, No-roes J, Baliza M, Medeiros Z, DreyerG. Evaluation of the Og4C3 ELISA inWuchereriabancrofti infection: infectedpersons with undetectable or ultra-Iowmicrofilarial densities. Trop Med IntHealth 1996; I: 859-64.
39. Melrose W, Pisters P, Turner P, Kom-bati Z, Selve BP, Hii Jeffrey, Speare R.Prevalence of filarial antigenaemia inPapua New Guinea: results of surveysby the School of Public Health andTropical Medicine, James Cook Uni-versity, Townsville, Australia. P N GMedJ 2000;43: 161-5.
40. Faris R, Ramzy RM, Gad AM, WeilGJ, Buck AA. Community diagnosis ofBancroftian filariasis. Trans R Soc TropMed Hyg 1993;87: 659-61.
41. Karam M, Ottesen E. The control oflymphatic filariasis. Med Trop 2000;60: 291-6.
42. Marley SE, Lammie PJ, Eberhard ML,Hightower Aw. Reduced antifilarialIgG4 responsiveness in a subpopulationof microfilaremic persons. J Infect Dis1995; 172: 1630-3.