primary cutaneous cd30+ t-cell lymphoproliferative disorders cutaneau… · aggressive...
TRANSCRIPT

PRIMARY CUTANEOUS CD30+ T-CELL LYMPHOPROLIFERATIVE DISORDERS
Marshall E. Kadin, M.D.Marshall E. Kadin, M.D.Boston University and Roger Williams Medical Center Boston University and Roger Williams Medical Center
Society for Hematopathology Workshop on Cutaneous Lymphomas
1
Primary cutaneous CD30+ T-cell lymphoproliferative disorders
30% of CTCL.
Includes primary cutaneous ALCL (C-ALCL), lymphomatoid papulosis (LyP) and borderline cases.
Clinicopathologic correlation is essential for proper diagnosis and management.
Incorrect diagnosis can result in overly aggressive therapy.
3

Spectrum of CD30+ cutaneous lymphoproliferative disorders
Lymphomatoid papulosis (LyP) Primary cutaneous ALCL Borderline lesions
4

5
Histopathology of Lymphomatoid Papulosis
Early perivascular lesion
Mature wedge-shaped lesion
Neutrophils within and around blood vessels are characteristic
Advanced ulcerated lesion
This slide illustrates the varied histologic picture of LyP. Early lesions have a perivascular lymphoid infiltrate. Mature lesions have a wedge-shaped appearance. The most common type A lesions have large RS like cells and frequent mitoses in an inflammatory background. Type B lesions resemble MF and may be a papular variant of MF. Whittaker and colleagues in London emphasized the significance of an indeterminant cell type as candidate for the clonal T cell in LyP. Type C lesions demonstrate a relatively monotonous population of large CD30+ cells with minimum inflammatory cells.

Four histologic types of LyP
Type A- Most common. Large atypical cells often resembling RS-like cells surrounded by inflammatory cells.
Type B- Epidermotropic lymphocytes with irregular sometimes cerebriform nuclei simulating MF. Distinguished from MF by papular self-healing lesions.
Type C- Clusters or sheets of CD30+ cells with relatively few inflammatory cells confined to the upper dermis.
Type D- CD8+ variant with intra-epidermal atypical medium-sized lymphocytes. Large anaplastic cells are rarely seen.

LyP Type A
Type A is the most common type. Large atypical cells sometimes resembling RS cells surrounded by inflammatory cells..
7

LyP type B
Epidermotropic lymphocytes with irregular sometimes cerebriform nuclei simulating MF. Distinguished from MF by papular self‐healing lesions.
8

LyP A/B
Some lesions have overlapping features of type A and B with a spectrum of epidermotropic lymphocytes and large atypical cells and have been classified by us as type A/B
9

LyP type C
Type C lesions have large clusters or sheets of CD30+ cells with relatively few inflammatory cells confined to the upper dermis. This lesion shows early regression.
10

LyP type D, CD8+
Courtesy of LorenzoCerroni,Graz, Austria
Am J Surg Pathol. 2010, 34:1168-75.
CD8
Recently proposed by Cerroni and colleagues as an LyP subtype that can be confused with an aggressive epidermotropic CD8+ lymphoma. However, erythematous papules or small nodules with scale crust or ulceration resolve spontaneously within some weeks. Intra‐epiderdermal lymphocytes are atypical, pleomorphic, medium‐sized cells. Large anaplastic cells are rarely seen.
9 patients (M:F=6:3, median age: 29; mean age 27,2; age range 10 to 38) who presented with clinical features typical of LyP but with histopathologic aspects that resembled primary cutaneous aggressive epidermotropic CD8+cytotoxic T‐cell lymphoma. In all but 1 case atypical lymphoid cells showed expression of CD30, and in 8 of 9 cases a T‐cell cytotoxic phenotype could be observed (betaF1+, CD3+, CD4‐, CD8+). Expression of at least 1 cytotoxic marker (TIA‐1, granzyme B) was observed in all cases. Polymerase chain reaction analysis of the T‐cell receptor genes revealed a monoclonal rearrangement in 2 of 5 cases tested. Follow‐up data available for 8 patients (mean follow‐up time: 84 mo, median: 32.5 mo; range: 1 to 303 mo) revealed that none of them developed systemic involvement or signs of other cutaneous lymphomas
11

12
LyP- Immunophenotype
CD30
TIA-1
CD4
LyP cells in most cases are activated T helper-cells (CD4+, CD30+)
Kadin, Am J Path, 119:315, 1985; Kummer J Invest Dermatol 109:636, 1997
CD25
The large atypical cells in most cases have a phenotype of activated helper T cells, CD4+, CD30+, CD25+ and contain cytotoxic proteins in ½ of cases.
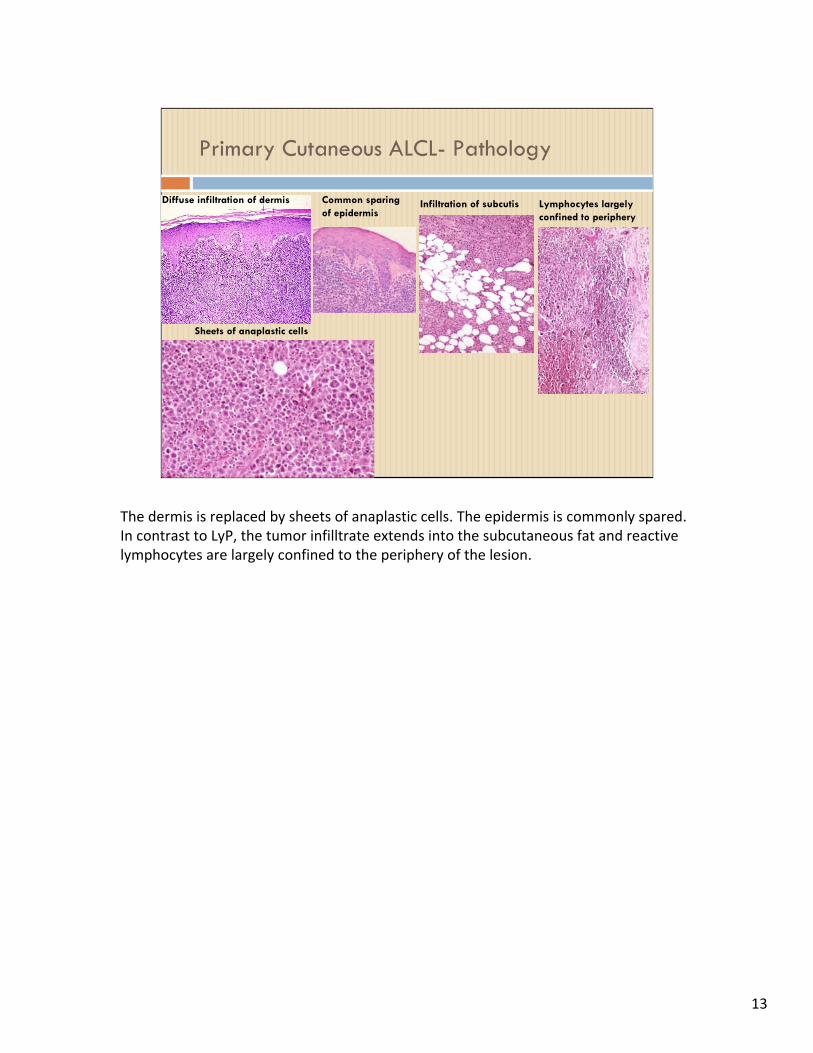
Primary Cutaneous ALCL- Pathology
Infiltration of subcutis Lymphocytes largely confined to periphery
Sheets of anaplastic cells
Common sparing of epidermis
Diffuse infiltration of dermis
The dermis is replaced by sheets of anaplastic cells. The epidermis is commonly spared. In contrast to LyP, the tumor infilltrate extends into the subcutaneous fat and reactive lymphocytes are largely confined to the periphery of the lesion.
13

Pseudoepitheliomatous hyperplasia and neutrophil-rich ALCL
This slides shows PEH also nicely illustrated in case 146 and neutrophil‐rich ALCL as in case 103. These may be examples of ALCL derived from Th17 cells as I will describe later.
14

Borderline/ALCL
CD30
BAP-FISH: IRF4
Courtesy of Andrew Feldman

16
IRF4 testing by FISH and IHC in cutaneous CD30+ T-cell lymphoproliferative disorders (Skin biopsies only)
0102030405060708090
100
c-ALCL
LYP s-ALCL
PTCL-U
FISHIHC
% o
f ca
ses
posi
tive
FISH
IHC
CALCL LyP sALCL PTCLCourtesy of Andrew Feldman, MD, Mayo Clinic
This slide from Dr. Feldman compares FISH and IHC data in skin biopsies, showing that while IRF4 protein expression can be detected by IHC in LyP, sALCL and PTCL, IRF4 translocations were detected only in primary cutaneous ALCL. IRF4 protects CD4+ T cells against pro‐apoptotic stimuli and activation induced cell death.

17
Differential diagnosis of Primary Cutaneous ALCL-Secondary skin lesions in systemic ALCL
Sinus infiltrate of CD30+ cells in lymph node
Reniform “hallmark” cells
Nuclear-cytoplasmic ALK
Primary cutaneous ALCL must be distinguished from secondary skin lesions of systemic ALCL which requires aggressive chemotherapy. Skin lesions may be present at clinical presentation in up to 40% of systemic ALCL. A positive ALK stain with nuclear/cytoplasmic staining favors systemic ALCL.

Large cell transformation in mycosis fungoides
CD30
Background of patch and plaque lesions
Epidermal involvement Anaplastic cells
A diagnosis of large cell transformation of MF is usually made when co‐existent plaques or patches are present. An exception to this general rule may be illustrated by remarkable cases 238 and 288 in which patients developed an ALK+ ALCL in the context of prior lesions of MF.
18
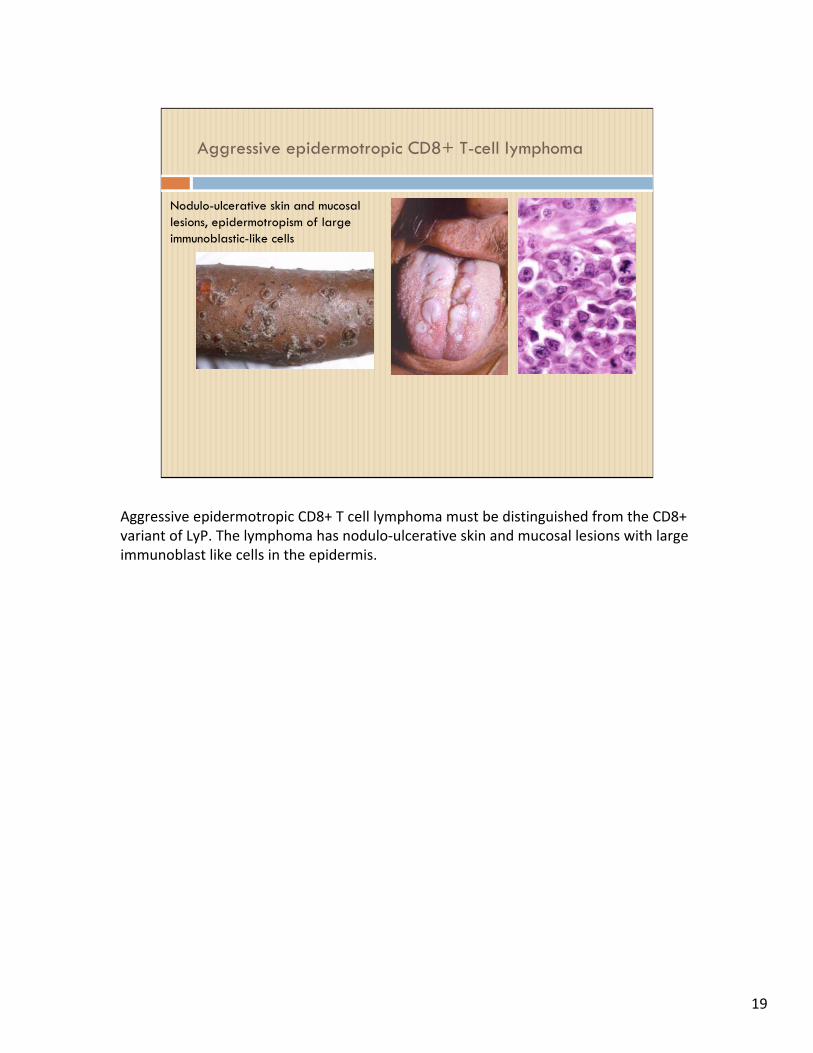
Aggressive epidermotropic CD8+ T-cell lymphoma
Nodulo-ulcerative skin and mucosallesions, epidermotropism of largeimmunoblastic-like cells
Aggressive epidermotropic CD8+ T cell lymphoma must be distinguished from the CD8+ variant of LyP. The lymphoma has nodulo‐ulcerative skin and mucosal lesions with large immunoblast like cells in the epidermis.
19

PLEVA- necrotic keratinocytes, CD8+
Pityriasis lichenoides acuta or PLEVA represents a more difficult differential diagnosis with LyP. PLEVA also presents with erythematous papulonecrotic lesions. In contrast to LyP, the histology is that of an interface dermatiits with necrotic keratinocytes and extravasated erythrocytes; atypical CD30+ cells are rare or absent and CD8+ cells predominate. Necrotic keratinocytes are absent in CD8+ LyP. PLEVA patients are usually young males in contrast to a generally older population of female predominance in LyP.
20

Pityriasis lichenoides chronica (PLC)
Parakeratosis and necrotic keratinocytes
Interface pattern, intra-epidermal lymphocytes
Vacuolization of basal layerextravasated erythrocytes and hemosiderin
Colloid bodies
The distinction between LyP and PLC can be more difficult because of chronic recurrent lesions. The interface pattern with parakeratosis, necrotic keratinocytes and extravasated erythrocytes in absence of LAC favors PLC.
21

Pityriasis lichenoides chronica (PLC) vs. LyP type B
CD30CD4
12 year old boy with 3 year history of recurrent papules on trunk and extremities.
This case illustrates a difficult differential diagnosis from LyP. CD4+ cells may predominate in PLC and in this case, numerous CD30+ cells were found within the epidermis. These cells were gamma‐delta positive and may identify a newly recognized variant of PLC.
22

23
Nodular scabies mimics LyP
CD30mite
CD30+ cells are not specific for LyP and some inflammatory conditions such as Scabies can be mistaken for LyP.
Other cutaneous disorders with frequent CD30+ cells
Atopic dermatitis
Lymphomatoid drug eruption
Herpes simplex
Herpes varicella-zoster
Syphilis
Milker’s nodules
Molluscum contagiosum
Hydroa-like lymphoma
CD30+ cells may be found in a variety of other cutaneous disorders which must be considered in the differential diagnosis of LyP.
24
Pathways of pathogenesis of CD30+ CLPD
Translocations involving IRF4 in ~25%.
Feldman et al, Leukemia 2009, 23:574.
ALK variants (cytoplasmic)- see case 42.
Kadin et al, Am J Surg Pathol, 2008
Deregulation of genes (FRA2, Id2, CSFR1) around the t(2;5) breakpoint in ALK negative C-ALCL.
Mathas et al, PNAS, 2009, 106:5831.
Notch signaling
Kamstrup et al, Br J Dermatol 2008, 2010
I will not further address IRF4 translocations which will be discussed by Dr. Feldman. We reported a case of ALK+ cutaneous ALCL with no extra‐cutaneous disease for more than 10 years. Dr. Gascoyne will present a simiiar case #42. In collaboration with Dr. Stephan Mathas in Berlin, we found increased expression of several oncogenes adjacent ALK and NPM on chromosomes 2 and 5. Finally, I will present new data that links the pathogenesis of Notch signaling to cutaneous ALCL.
25
26
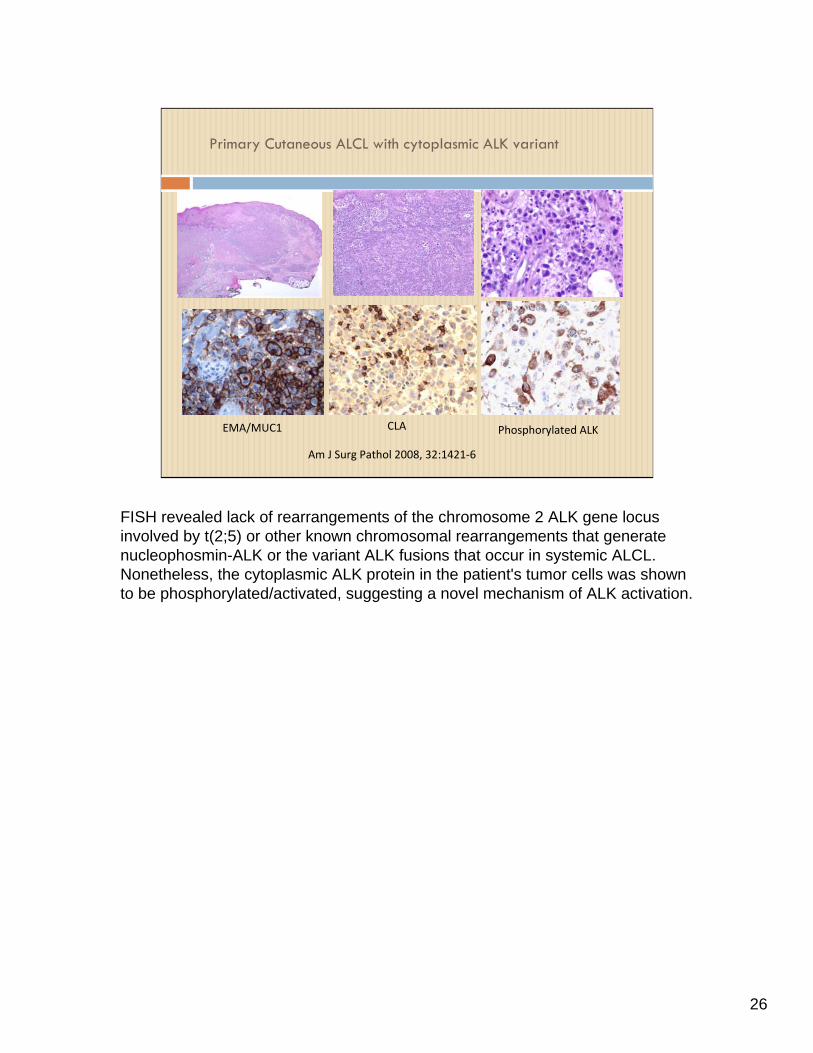
Primary Cutaneous ALCL with cytoplasmic ALK variant
EMA/MUC1 CLA Phosphorylated ALK
Am J Surg Pathol 2008, 32:1421‐6
FISH revealed lack of rearrangements of the chromosome 2 ALK gene locus involved by t(2;5) or other known chromosomal rearrangements that generate nucleophosmin-ALK or the variant ALK fusions that occur in systemic ALCL. Nonetheless, the cytoplasmic ALK protein in the patient's tumor cells was shown to be phosphorylated/activated, suggesting a novel mechanism of ALK activation.
CD30+ lymphoma cells resemble Th17 cells
Patients’ serum lack elevated Th2 cytokines IL-4 and IL-5.
Some patient sera contain Th17 cytokines IL-17A, IL-17F and/or IL-22.
CD30+ cutaneous ALCL lines secrete Th17 cytokines.
We hypothesize that CD30+ lymphoma cells of some patients are derived from Th17 cells.
In support of our hypothesis, CD30+ lymphoma cells lack FoxP3 transcription factor, characteristic of regulatory T-cells, but express transcription factors ROR, IRF4 and pSTAT3 which are critical for Th17 differentiation.
In a study of sera from 116 patients with CD30+ CLPD collected at clinical presentation, we found a lack of Th2 cytokines IL‐4 and IL‐5. Instead many but not all patient sera contained Th17 cytokines IL‐17A, IL‐17F and/or IL‐22. These same cytokines were detected in cell culture supernatants of CD30+ cutaneous ALCL cells.
27

What are Th17 cells?
Th17 cells represent a recently recognized subset of CD4+ effector T cells that regulate autoimmune inflammation.
Immunity mediated by Th17 cells is particularly important at epithelial and mucosal surfaces, e.g. skin and GI tract.
Th17 cells are prominent in psoriasis, contact dermatitis and scleroderma.

Hypothesis
CD4+ is the dominant phenotype of tumor cells in CD30+ ALK(-) cutaneous T-cell lymphomas. The precise nature of the CD4+ T-cell in these lymphomas is not yet defined and is the subject of our current research.
We hypothesize that CD30+ tumor cells in some CTCL derive from Th17 or recently discovered Th22 cells. Alternatively, Th17/Th22 differentiation occurs during tumor progression.
Confirmation of this hypothesis could lead to new prognostic markers and cytokine targeted therapies for CD30+ cutaneous T-cell lymphoproliferative disorders.
This slide depicts pathways of effector T cell differentiation from naïve T cells. Differentiation of Th17 cells requires TGFb and induction of nuclear receptor RORgt. Th17 cells secrete IL‐21, IL17a, IL17f, IL‐22 and IL‐10.
29

CD30+ cutaneous ALCL cell lines secrete Th17 cytokines
Courtesy of Roderick McLeod, Ph.D.
This slide demonstrates secretion of abundant IL‐22 by both Mac‐1 and Mac‐2A cell lines, while Mac‐1 secretes IL‐17A and TGF‐beta and Mac‐2A secretes mainly IL‐17F, TGF‐b, IL‐6, IL‐13 and thymus and activation regulated chemokine TARC.
30

IL-17F immunohistochemistry in CD30+ CLPD
IL-17F
Control without primary Ab H&E section
IL-17F
Patient had 10 pg/ml circulating IL-17F at time of biopsy
We confirm that tumor cells from some patients with CD30+ cutaneous lymphoma produce IL‐17F as shown here.
31
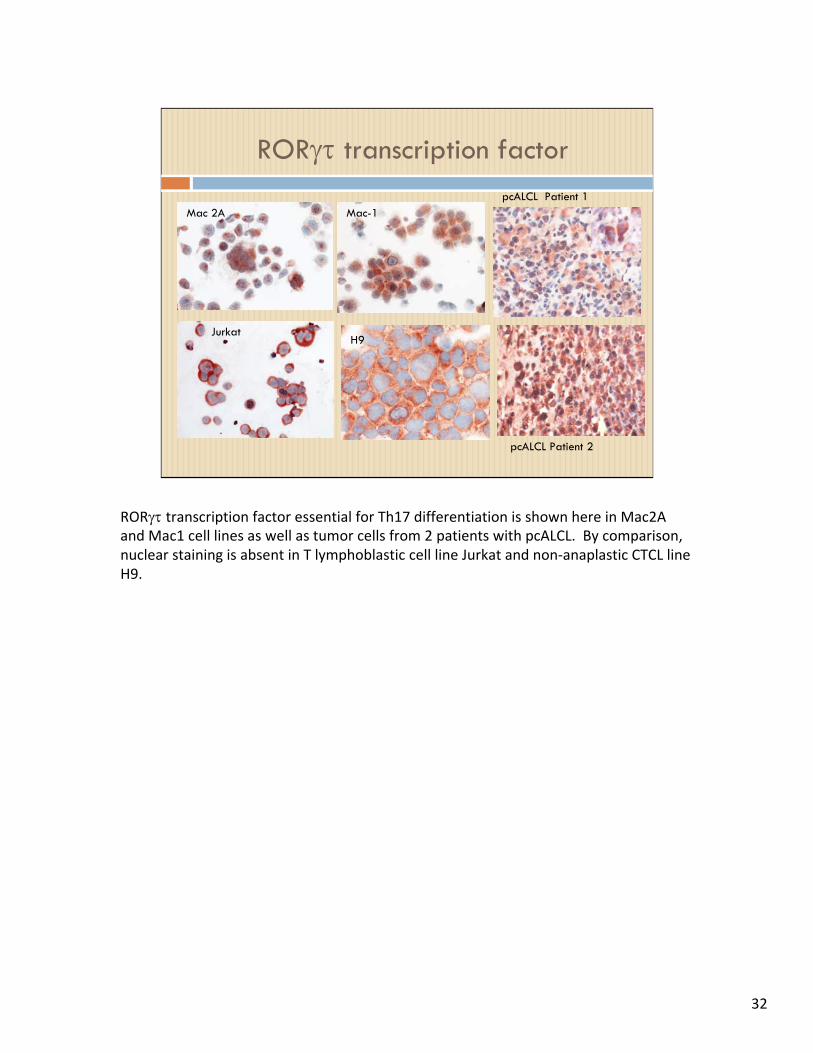
ROR transcription factor
Mac 2A
JurkatH9
Mac-1pcALCL Patient 1
pcALCL Patient 2
RORtranscription factor essential for Th17 differentiation is shown here in Mac2A and Mac1 cell lines as well as tumor cells from 2 patients with pcALCL. By comparison, nuclear staining is absent in T lymphoblastic cell line Jurkat and non‐anaplastic CTCL line H9.
32

Phosphorylated STAT3 in CD30+ CLPD
LyP
pcALCL
Mac2A cell line
Phosphorylated or activated STAT3 essential for Th17 differentiation is shown here in nuclei of Mac2A cells and tumor cells of LyP and pcALCL.
33

Large atypical CD30+ cells lack FoxP3
FoxP3
In contrast, the large atypical CD30+ cells lack FoxP3, the transcription factor for induced T regulatory cells which are seen as small reactive lymphocytes.
34

AhR
-actin
JB-6 Mac-2B Mac-2A Mac-1
ALCL cells express Aryl Hydrocarbon Receptor (AhR): A mediator of responses to toxic aromatic hydrocarbons
Mac-1 cells express activated AhR
AhR activation results in expansion of Th17 cells and is essential for production of IL-22.
Western blot
This slide demonstrates the AhR in ALCL lines and biopsy of a patient with pcALCL. The AhR is a mediator of toxic responses to aromatic hydrocarbons potentially linking the pathogenesis of some CD30+ CLPD to environmental toxins. The AhR is a cytosolic sensor of small synthetic compounds and natural chemicals which act as ligands. Ligand binding induces a conformational change of cytosolic AhR resulting in nuclear translocation. AhR expression is extremely low in Tregs.
35

Notch signaling in CD30+ CLPD
Kamstrup and co-workers found cells expressing Notch-1 and its ligand Jagged-1 in LyP and pcALCL. (Br J Dermatol, 2008)
CD30+ ALCL lines (Mac-1, Mac-2A and JK) express Notch-1 (Br J Dermatol, 2010).
Gamma secretase inhibitors of the Notch signaling pathway triggered apoptosis preceded by accumulation of CD30+ lymphoma cells in G2/M of the cell cycle.

Notch signaling drives IL-22 secretion in CD4+ T-cells by stimulating the Aryl hydrocarbon receptor
Innate immunityin skin, GI and respiratory epithelium
IL-17F
IL-17A
IL-22
Keratinocyte hyperplasia
Acute inflammation, defensins
ALCL
IL-22R1IL-10R2
pSTAT3
CD4/LyPAhR
Alam et al, PNAS, 2010, 107: 5943; Bard et al, Leukemia 2008, 22:1595 Kamstrup et al , Br J Dermatol 2010 June epub
LyP lesion
Notch
IL‐22 acts as an autocrine growth factor for ALK+ ALCL lines signaling through IL‐22R1 which is not expressed on normal lymphocytes but is aberrantly expressed on ALCL lines including cutaneous ALCL line Mac‐2A. IL‐22 normally synergizes with IL‐17A and IL‐17F to regulate innate immunity in the skin, GI and respiratory tracts. IL22 induces keratinocyte hyperplasia, dermal inflammation and synthesis of anti‐microbial peptides potentially explaining characteristic features in the pathology of CD30+ CLPD.
37

High soluble CD30, CD25 and IL-6 may identify patients with worse survival in CD30+ cutaneous lymphomas
We measured soluble CD30 (sCD30), soluble CD25 (sCD25), TGF-, IL-8, IL-6, and other Th2 cytokines in sera of 116 patients with CD30CLPD followed up to 20 years (median 11 years).
Significantly worse disease-related survival was found for patients with high sCD30, sCD25, and IL-6. (J Invest Dermatol, in press)
38

Survival of patients with primary cutaneous CD30-positive lymphoproliferative disease according to IL-6 levels
B- Disease related deathA- All causes of death

Survival of patients with CD30+ primary cutaneous T-cell lymphoproliferative disease according to sCD30 levels
A- all causes of death B- disease-related death
A possible mechanism for the adverse prognostic signifiance of CD30 is that cross‐linking of cell surface CD30 causes up‐regulation of NF‐kB, (Levi et al., 2000) which activates anti‐apoptotic C‐FLICE in cutaneous ALCL cells (Braun et al., 2010). A similar mechanism may be operative in MF in which NF‐kB, a pro‐survival transcription factor, is constitutively expressed (Izban et al., 2000).
40

Mac1 Mac2A Mac2B0.00
0.01
0.02
0.03
0.04
RatioCD30:B-actin
Increased CD30 expression in progression Of LyP derived lymphoma cell lines
Real Time PCR amplification of CD30 in Mac cell lines
The mechanism of decreased survival may be linked to the increased expression of CD30 with tumor progression as illustrated here by real time PCR amplification of CD30 in cell line Mac1 from early disease compared to cell lines Mac2A and 2B from advanced disease.
41

CD30 ligation activates NF-B
EMSASpecific inhibition of NF-kB binding by SN50
CD30 was cross-linked by HeFi-1 antibody
Levi et al, J Invest Dermatol 2000
CD30 ligation by monoclonal antibody HeFi‐1 activates CD30 as shown in this electrophorectic mobility shift assay. Specificity is shown with a specific inhibitor SN50.
42

How cytokines may contribute to the pathogenesis of pc-ALCL
Jagged 1-NotchAhR
ALCLCD30L NF-kB C-FLIP
TGF-R
X
TGF-Immune responsesuppressed
IL-22 IL-22R1
CD30Neut
Eos
Levi et al, J Invest Dermatol 2000, Braun et al, J Invest Dermatol 2010
This cartoon illustrates how cytokines may contribute to the pathogenesis of pc‐ALCL. CD30 cross‐linking activates NF‐kB which promotes cell survival in part through up regulation of C‐FLIP an inhibitor of death‐receptor signaling. TGF‐beta secreted by tumor cells suppresses the immune response but can no longer inhibit tumor cell growth because of receptor mutations. As discussed earlier, the Notch signaling pathway promotes IL‐22 autocrine growth.
43

Conclusions
Primary cutaneous CD30+ T-cell LPD have characteristic morphology, immunophenotype, genetics, and clinical behavior which allow distinction from other CTCL and benign dermatoses in nearly all cases.
Pathways of pathogenesis involve rearrangements of IRF4, ALK andNotch signaling.
CD30+ T-cell LPD do not closely resemble Th2 cells but in some patients have characteristics of Th17 cells.
Elevated serum levels of cytokine receptors (CD30, CD25) and cytokines (IL-6, IL-8) identify patients with potential poor outcome to be monitored for disease progression.
Deregulated cytokines contribute to the pathogenesis of pcALCL.

Acknowledgements
Eric Vonderheid, M.D.- Clinical co-investigator Igor Pavlov, Ph.D Roderick McLeod, Ph.D Cytokine measurements Edi Levi, M.D., Ph.D. Joan Massague, Ph.D. Harvey Lodish, Ph.D. Juergen Eberle, Ph.D. Xiao-Feng Lin, Ph.D. Deb Greer Haiying Xu
Grant support
NIH- P20RR018757 Allergan, Inc.
Cytokine functional studies
IHC, molecular studies

THANKS FOR YOUR ATTENTION
THANKS FOR YOUR ATTENTION

47
Deregulated genes in ALK negative ALCL
21 M
Mathas et al, PNAS, 2009, 106:5831-6.
Although the t(2;5) characteristic of systemic ALCL is pcALCL, a recent study has shown deregulation of genes surrounding the t(2;5) breakpoints. Deregulated genes near the ALK locus are the oncogenic AP1 transcription factor FRA2, and ID2, a helix loop helix inhibitor of cellular differentiation which may explain silencing of T cell differentiation antigens seen in ALCL. CSF1 receptor is an oncogenic tyrosine kinase at 5q33.1 near NPM.

48
Fra2 and Id2 are expressed together with CD30 in LyP
Fra2 and Id2 are also over‐expressed by CD30+ cells in LyP showing a pathogenetic link to ALK negative ALCL.

Comparison of histologic types of lymphomatoid papulosis
Type A Type B Type C Type D
Cytology Immunoblasts, large anaplastic cells, RS-like cells, apoptotic bodies
Cerebriform cells (CMC)
Immunoblasts; large anaplastic cells
Pagetoid pattern with epidermotropism of mid-sized atypical pleomorphic lymphocytes.Absence of necrotic keratinocytes.
Inflammatory cells Numerous Infrequent Few to moderate Not prominent
Mitoses Frequent Infrequent Frequent
Regression 4-6 weeks 8-12 weeks Slow and incomplete Resolve in some weeks

Cytokine expression in Mac cell lines
Control No Primary Ab
IL-17F in Mac-2A cells IL-22 Mac 2B
Western blot-IL-22
20kd
C 2B 2A Mac1
IL-22 Mac-1
actin
IL-22 Mac 2A
We confirmed the expression of IL‐17F and IL‐22 in Mac cell lines by IF, IHC and Western blot as shown here.
50
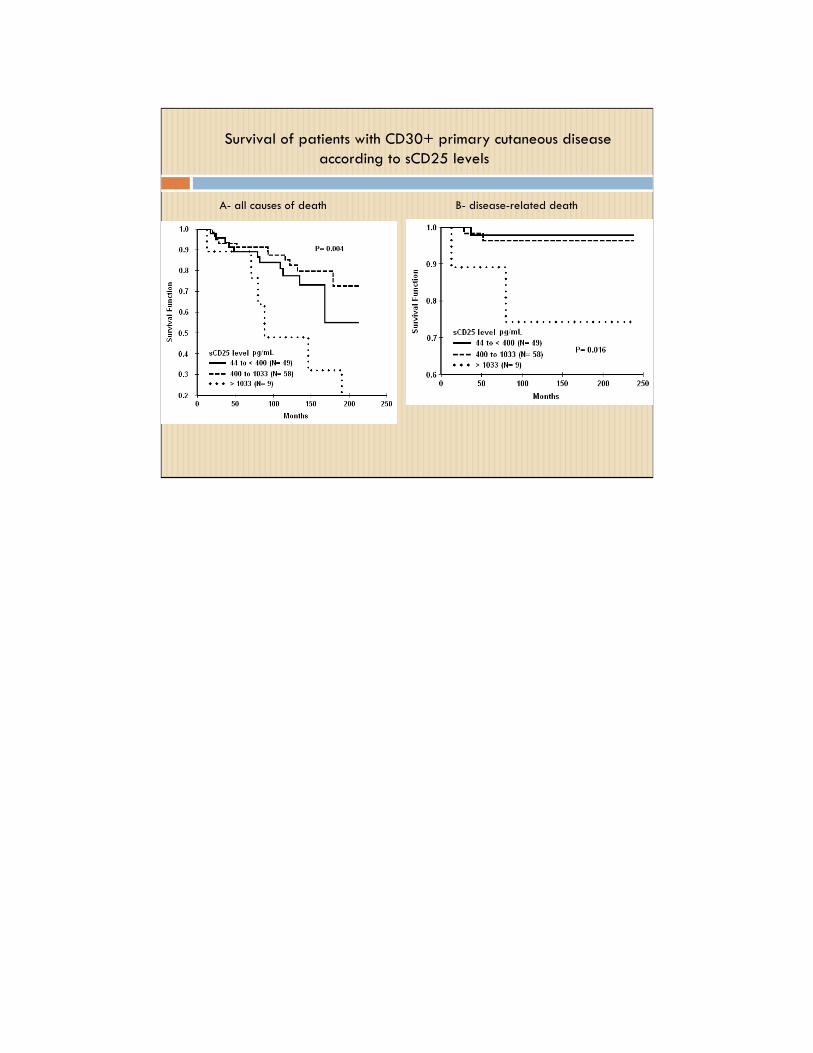
Survival of patients with CD30+ primary cutaneous disease according to sCD25 levels
A- all causes of death B- disease-related death
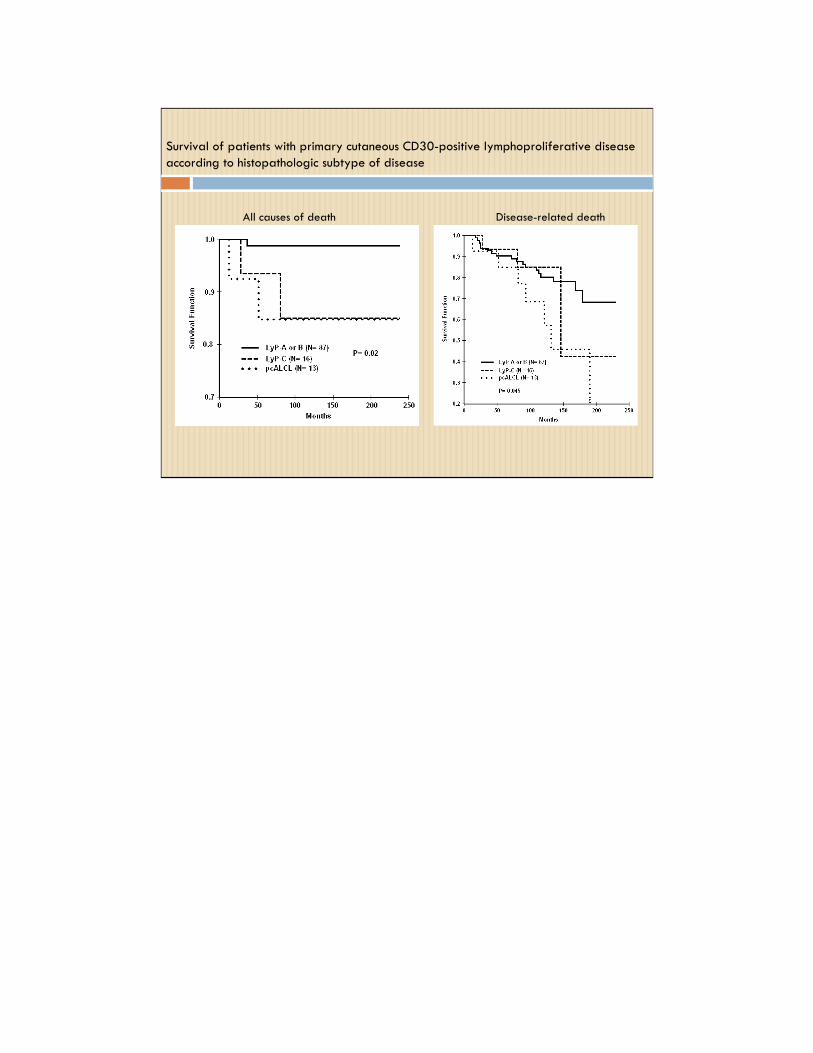
Survival of patients with primary cutaneous CD30-positive lymphoproliferative disease according to histopathologic subtype of disease
All causes of death Disease-related death

Systemic ALCL Mycosis fungoides
Pityriasis Lichenoides
Arthropod bite
Scabies
Clinical Frequent skin lesions, generalized lymphadenopathyB symptoms
Scaling erythematous patches, plaques, tumors, +/- lymph-adenopathy
Scaling erythematous hemorrhagic lesions
Exposure history Itchy lesions.Responds well to Kwell
HistologyImmuno-phenotype
Lack of epidermotropic cerebriform cellsALK+, EMA+Often ALK neg. in patients over 30
Epidermotropism of cerebriform cellsCD30+ with large cell transformation
Interface dermatitis, extravasated RBCsCD8+ > CD4+, few CD30+ cells in acute form (PLEVA). CD4>CD8, CD30+ cells in chronic form (PLC)
Punctum, insect parts.PolymorphousInflammation CD30+ cells may be present
Presence of mite. CD30+ cells and B cells present
Genetics t(2;5) often presentNo IRF4 rearrangementClonal TCR-GR
Lack of t(2;5)Complex karyotype,TCR clonal or oligoclonal
Clonal TCR in 50% No abnormalities No abnormalities
Differential diagnostic features of CD30+ primary cutaneous lympDifferential diagnostic features of CD30+ primary cutaneous lymphoproliferative disordershoproliferative disorders

L yP ALCL Borderline
Clinical Crops of papules/nodules with central necrosis; spontaneous regression occurs in 4-6 weeks
One to several ulcerating nodules or tumors, regression occurs in 25%
Intermediate size nodules (1-2 cm); slow regression
Histology Early lesions have upper dermal perivascular lymphocytes. Neutrophils in blood vesselsScattered large atypical cells surrounded by reactive/ inflammatory cells“Mature” lesions are wedge-shaped. Late lesions develop crust and may ulcerate.
Deep dermal infiltrate, often sparing epidermisExtensive tumor cell infiltration of dermis and subcutis.Reactive small lymphocytes largely confined to periphery.Neutrophil-rich variant with rare tumor cells
Clusters of large atypical cells largely confined to dermis.Variable numbers of inflammatory cells.Spectrum of cerebriform mononuclear cells to large RS-like cells may be found.
Immunophen-otype, genetics
CD30+, CD4+, LCA+, TIA-1/Granzyme B+Diploid to aneuploidPoly-, oligo-, or monoclonal TCR gene rearrangement (60%)
CD30+, CD4+, LCA+, TIA1/Granzyme B+Absence of t(2;5) except in rare pediatric cases.IRF4 translocation in 25%Aneuploidy, clonal TCR (>90%)
CD30+, CD4+, LCA+, TIA-1+ No data on cytogeneticsClonal by TCR gene analysis
Major distinguishing features of CD30+ cutaneous lymphoproliferative disorders
54

Survival of patients with primary cutaneous CD30-positive lymphoproliferative disease according to IL-6 levels
B- Disease related deathA- All causes of death

Survival according to serum IL-8 levels- all causes of death

Increased serum CD30 and CD25 at clinical presentation are associated with poor outcome