procedural sedation keir swisher, d.o. may 13, 2010
TRANSCRIPT

Procedural SedationKeir Swisher, D.O.
May 13, 2010

2011 Superbowl ChampionsKansas City Chiefs

Objectives
• State the definitions of sedation according to JCAHO
• List pre-procedural patient assessments
• Understand common sedation complications and their management
• Post-procedural patient care
• Sedation medications and appropriate reversal agents


Sedation is a continuum moving from one state of conscious to another and is dose-related depending on the individual patient
response

Levels of Sedation and Anesthesia
Levels of Sedation and Anesthesia
• Level 0: No Sedation
• Level 1: Light/Minimal sedation (anxiolysis)
• Level II: Moderate sedation
• Level III: Deep sedation
• Level IV: General Anesthesia

Level 0: No Sedation
• Patients undergoing diagnostic procedures without sedation
• Arousal: No alteration in level of consciousness
• These patients should be able to lie still and are anxiety/pain free throughout procedure
Level I: Light or minimal sedation
• Administration of medications to reduce potential anxiety
• Arousal: Patient responds normally to verbal commands although cognitive function and coordination may be impaired
• Respiratory function: unaffected

Level II: Moderate Sedation/Procedural sedation
• Arousal: Respond purposefully to verbal commands, either alone or accompanied by light tactile stimulation
• Respiratory function: No interventions required to maintain a patent airway, spontaneous ventilation is adequate

Level III: Deep sedation
• Arousal: Cannot be easily aroused but responds purposefully after repeated or painful stimulation
• Respiratory function: may require assistance in maintaining a patent airway and spontaneous ventilation may be inadequate
Level IV: Anesthesia
• Arousal: Loss of consciousness during which patients are not arousable, even by painful stimulations
• Respiratory function: Ability to independently maintain ventilatory function impaired, requires assistance to maintain patent airway and often requires positive pressure ventilation

Pre-Procedural Evaluation
• History and Physical exam• Airway assessment• Review current medications, prior sedation
history, allergies, pregnancy status, history of substance abuse, pain assessment, laboratory results, vital signs, Aldrete score and current level of consciousness
• NPO status• ASA classification

Fasting Guidelines
Intake Category Fasting Period for Low Risk Patients
Fasting Period for High Risk Patients
Clear Liquids 2 hours 8 hours
Breast Milk 4 hours 8 hours
Infant Formula 6 hours 8 hours
Non-human Milk 6 hours 8 hours
Regular Meal 8 hours 8 hours

Airway Assessment: Mallampati
• Class 1: soft palate, fauces, uvula, pillars
• Class 2: soft palate, fauces, portion of uvula
• Class 3: soft palate, base of uvula
• Class 4: hard palate only


ASA Classification
• Class I: Normal healthy patient• Class II: Patient with mild systemic disease• Class III: Patient with severe systemic disease• Class IV: Patient with severe systemic disease
that is a constant threat to life• Class V: Moribund patient not expected to
survive without operation
*E can be added for emergency procedures

Class II: Patient with mild systemic disease
• No functional limitations
• Well-controlled disease of one body system
• Controlled hypertension or diabetes without systemic effects
• Cigarette smoking without chronic obstructive pulmonary disease (COPD)
• Mild obesity
• Pregnancy

Class III: Patient with severe systemic disease
• Some functional limitation• Controlled disease of more than one body
system or one major system• No immediate danger of death• Controlled congestive heart failure (CHF),
stable angina, old heart attack, poorly controlled hypertension, morbid obesity, chronic renal failure; bronchospastic disease with intermittent symptoms

Class IV: Patient with severe systemic disease that is a constant threat to life
• Has at least one severe disease that is poorly controlled or at end stage
• Possible risk of death
• Heart disease showing marked signs of cardiac insufficiency, unstable angina
• Advanced degrees of pulmonary, hepatic, renal, or endocrine insufficiency


Informed Consent
• Physician is to review the objectives, risks benefits, and alternatives to the procedure with the patient

Pre-Procedure Time Out
• Completed before the first dose of sedation
• All participants including patient must agree
• Verify– Correct patient– Correct procedure– Correct site– Correct/Special equipment

Intra-Procedural Monitoring
• Documentation must include vital signs (BP, pulse, respirations, pulse oximetry) and level of consciousness prior to, during and post-procedure
• Vital signs must be monitored every 5 minutes and documented every 15 minutes if vitals remain stable
• Oxygen may be administered throughout the procedure and recovery period

In case of emergency…..
• Emergency equipment– Oxygen with nasal
cannula/mask– Ambu bag with mask– Suction– Crash cart– Airway box– Reversal agents
Intra-Procedural Cardio-Respiratory Monitoring
• Cardiac monitoring must be available for all patients
• Pediatric patients (birth to 18 years) continuous SpO2 monitoring must be used regardless of sedation level
• Adult patients continuous SpO2 monitoring is based on:– patient clinical assessment– invasiveness and length of planned procedure– medication and degree of sedation used

Potential Complications• Usually related to medications/patient response• Most common is respiratory depression
– Patient stimulation often successful– Consider use of emergency equipment such as bag-valve mask
and oxygen
• Aspiration– Suction– May have silent aspiration. Monitor skin color and SpO2.
• Hemodynamic instability– Consider fluid bolus.
• Consider ACLS guidelines for any complication• If significant respiratory depression and/or
hemodynamic instability occurs, consider use of reversal agents.
Choosing appropriate medications
• Agents should be chosen based on the desired pharmacological response (anxiolysis, analgesia, amnesia).
• Adverse effects: the potential side effects of any medication in a particular patient must be considered.
• Pharmacokinetic considerations: – Onset and duration– Elimination route– Accumulation– Drug interactions/potentiations– Cross-tolerance

PharmacokineticsDrug Onset time (min) Duration
Ketamine 0.3 5-10 mins
Midazolam (Versed®)
3-5 1-2 hours
Lorazepam
(Ativan®)
10-20 4-6 hours
Fentanyl 1-2 0.5-1 hours
Morphine 5-10 2-4 hours
Propofol
(Diprivan®)
0.5-2 10-15 mins

Route of elimination
Hepatic Renal
Ketamine Diazepam metabolites
Midazolam (Versed®) Midazolam metabolites
Lorazepam (Ativan®) Morphine metabolites
Fentanyl
Morphine
Propofol (Diprivan®)
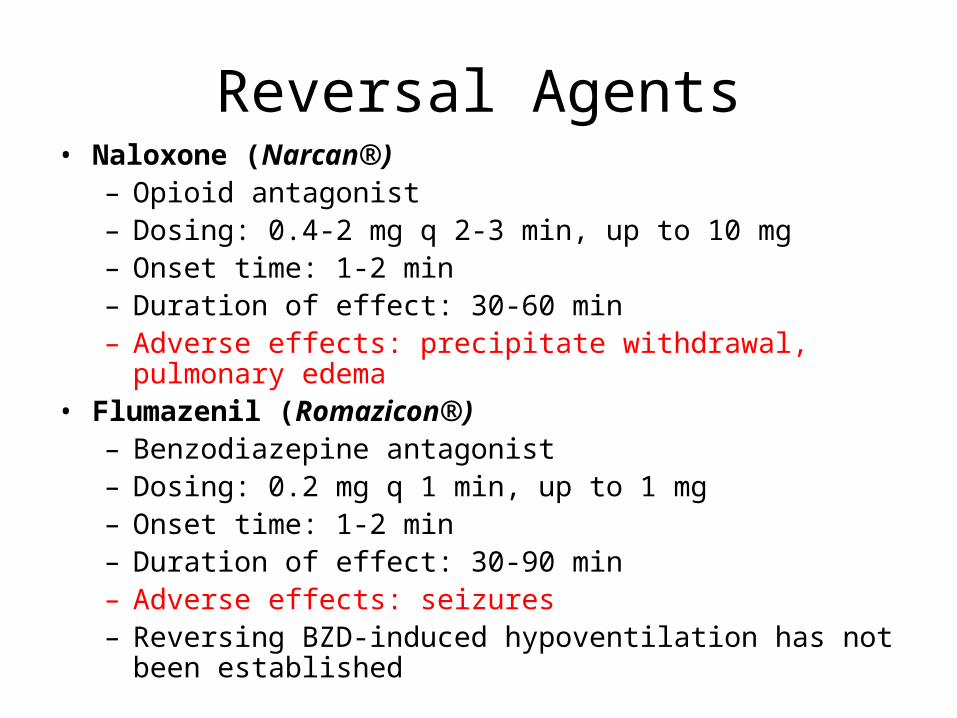
Reversal Agents• Naloxone (Narcan®)
– Opioid antagonist– Dosing: 0.4-2 mg q 2-3 min, up to 10 mg– Onset time: 1-2 min– Duration of effect: 30-60 min– Adverse effects: precipitate withdrawal, pulmonary edema
• Flumazenil (Romazicon®)– Benzodiazepine antagonist– Dosing: 0.2 mg q 1 min, up to 1 mg– Onset time: 1-2 min– Duration of effect: 30-90 min– Adverse effects: seizures– Reversing BZD-induced hypoventilation has not been
established

Post-procedure Monitoring
• Patients will be assessed immediately post-procedure and a minimum of every 15 minutes x 2.
• If a reversal agent has been used, monitor at least every 15 minutes x 4.
• Patients will be monitored every 5 minutes if still moderately or deeply sedated.
Recovery Criteria:Inpatient
• Aldrete score of 8 or equal to their pre-procedure score.
• Cardiovascular function and airway patency are satisfactory and stable.
• Patient is easily aroused, protective reflexes (gag and cough) are intact.
• Patient can communicate at pre-sedation level.• Patient can tolerate food and fluids.• Pain is at an acceptable level.

Discharge criteria:Outpatient
• In addition to the recovery criteria:– Department-specific discharge criteria must be met.– Stable vital signs.– Patient must have a responsible person drive him/her
home and assume responsibilities for the patient after discharge.
– Pain is at an acceptable level.– Adequate discharge instructions (avoid driving for 24
hours, avoid alcoholic beverages for 24 hours, etc.)– Patient can sit up without support and/or walk at pre-
sedation level.

Aldrete ScoreAldrete Score Pre Post
Able to move 4 extremities voluntarily or on command = 2
Able to move 2 extremities voluntarily or on command = 1
Able to move 0 extremities voluntarily or on command = 0
ACTIVITY
Able to deep breathe and cough freely = 2
Dyspnea or limited breathing = 1
Apneic = 0
RESPIRATION
BP +/- 20% of Pre-anesthesia level = 2
BP +/- 20-50% of Pre-anesthesia level = 1
BP +/- 50% of Pre-anesthesia level = 0
CIRCULATION
Fully awake = 2
Arousable on calling = 1
Not responding = 0
CONSCIOUSNESS
Pink = 2
Pale, dusky, blotchy, jaundiced, other = 1
Cyanotic = 0
COLOR

Documentation
• Should reflect evidence of baseline and continued assessment, patient response, and intervention.– Informed consent– Relevant history and physical assessment– ASA and Mallampati classification– Medication, dosage, route– Location and number of attempts to establish IV
access– All fluids administered– Physiologic data (BP, HR, RR, O2 saturation, pain
score), Aldrete score

Question I
• Documentation of vital signs should occur how often during procedural sedation?
• A. Every minute
• B. Every 5 minutes if they stay stable
• C. Every 15 minutes if they remain stable, yet monitored every 5 minutes
• D. Beginning and end of procedure
Question 2
• A 30 year old male dislocates his shoulder playing basketball. During his procedural sedation he is arousable only to painful stimuli, has normal oxygen saturation and chest wall excursion. What level of sedation is he in?
• A. Level 0• B. Level I• C. Level II• D. Level III• E. Level IV

Question 3
• 8 year old male requires procedural sedation for a complex laceration repair. During the sedation the patient has an acute decrease in end tidal CO2, with desaturation to 88%. He does not respond to painful stimulus and has shallow respirations. What level of sedation does he fall under?
• A. Level 0• B. Level I• C. Level II• D. Level III• E. Level IV

Question 4
• A 42 year old male inpatient is receiving procedural sedation for a paracentesis. He responds to verbal stimuli, has normal vital signs. What level of sedation has been achieved?
• A. Level 0• B. Level I• C. Level II• D. Level III• E. Level IV
Question 5
• You are sedating a 16 year old female for PICC line placement. During sedation she has oxygen desaturations to 91%, with painful stimulus she improves her saturations to 99%. What level of sedation was she in?
• A. Level 0• B. Level I• C. Level II• D. Level III• E. Level IV
Question 6
• You are providing procedural sedation for a 72 year old female with a dislocated hip. During sedation, she has desaturations to 85%, does not respond to painful stimuli, and requires bagging for 3 minutes before she resumes appropriate ventilation. What level of sedation was she in?
• A. Level 0• B. Level I• C. Level II• D. Level III• E. Level IV

Question 7
• The appropriate minimum fasting time for a healthy patient undergoing elective moderate sedation on a clear liquid diet is?
• A. 1 hour
• B. 2 hours
• C. 4 hours
• D. 6 hours
• E. 8 hours

Question 8
• During the pre-procedural evaluation the soft palate, fauces and a portion of the uvula are visible. Which Mallampati airway classification should be assigned?
• A. Class 1
• B. Class 2
• C. Class 3
• E. Class 4

Question 9
• A 60 year-old female with a history of diabetes and hypertension controlled with medications is scheduled for colonoscopy. What ASA classification should be assigned?
• A. ASA I• B. ASA II• C. ASA III• D. ASA IV• E. ASA V

Question 10
• A 65 year-old male with a history of COPD requiring home oxygen and chronic renal insufficiency is in the ICU for upper gastrointestinal bleeding. She is currently hypotensive and being transfused for acute blood loss anemia. The patient is scheduled for emergent endoscopy. What ASA classification should be assigned?
• A. ASA III E• B. ASA IV• C. ASA IV E• D. ASA V• E. ASA V E
Question 11
• Which is not required for the pre-procedural time out?
• A. Correct patient
• B. Correct time
• C. Correct procedure
• D. Correct site

Question 12• During a moderate sedation procedure, the patient
begins to have increased oxygen requirements and desaturations. He is only intermittently responding to noxious stimuli and experiencing periods of apnea. What is the next appropriate step in this patients management?
• A. Nothing, continue with procedure• B. Immediate intubation• C. Administer naloxone• D. Airway support with oral airway and bag-mask
ventilation

Question 13
• Joe Brown is a 60-year-old otherwise healthy male who is to have a closed reduction of a distal radial fracture under moderate sedation. Pre-procedural vitals include BP 140/80, P78, R18, SpO2 98%. After administration of the medications, Mr. Brown’s BP drops to 106/60 and his pulse rises to 98. What should be the first intervention provided?
• A. Fluid bolus• B. Flumazenil 0.2 mg IVP• C. Narcan 0.4 mg IVP• D. Immediately cancel the procedure.

Question 14
• During a hip reduction, you order Morphine 6 mg IV. Within a few minutes, the patient’s oxygen saturation drops to 92%. You should immediately:
• A. Insert an oropharyngeal airway• B. Stimulate the patient• C. Begin bagging the patient with a bag-
valve mask• D. Give a fluid bolus

Question 15
• What is the usual Midazolam onset time and what is the time interval that should elapse before a second dose should be administered?
• A. 30 seconds, 5 minutes
• B. 1 minute, 1 minute
• C. 3-5 minutes, 5 minutes
• D. 10 minutes, 20 minutes

Question 16
• What is the expected duration of effect of a single bolus of Morphine?
• A. 1-2 hours
• B. 4-6 hours
• C. 0.5-1 hour
• D. 2-4 hours

Question 17
• What is the duration of effect of Naloxone and what is the minimum amount of time after the dose that the patient should be monitored?
• A. 30 min to 1 hour, 30 minutes
• B. 30 min to 1 hour, 1 hour
• C. 1 to 2 hours, 1 hour
• D. 1 to 2 hours, 2 hours
Question 18
• After procedural sedation to reduce a distal radial fracture, your patient states that she is ready to go home. Which of the following would indicate that she is not ready to be discharged?
• A. Dizziness when first standing• B. Systolic BP 120-136 for the past hour• C. Wrist pain, reported 3/10• D. Aldrete score 2 below pre-procedural
score.

Question 19
• Your patient’s mother has not arrived to drive her daughter home after procedural sedation. The patient states that she feels fine and would really like to leave now. What should the nurse do?
• A. Send the patient home in a cab.• B. Wait another 30 minutes, then allow the patient to
take a bus home.• C. Release the patient only after a responsible
person is present to drive.• D. Allow the patient to drive herself home.

Question 20
• Which of the following information should be included in the discharge information when a patient is discharged within 24 hours of receiving procedural sedation?
• A. Return to your normal activities• B. Do not drive for 24 hours• C. Avoid alcoholic beverages for the next 2
hours• D. Clear liquid diet for 24 hours
Answers• 1: C 15: C• 2: D 16: D• 3: E 17. B• 4: B 18. D• 5: D 19. C• 6: E 20. B • 7: B• 8: B• 9: A • 10: E • 11: B• 12: D• 13: A• 14: B

References
• ASA (2002) Practice Guidelines for Sedation and Analgesia by Non-Anesthesiologists. Anesthesiology, 96:1004-17.
• JCAHO Standards, Comprehensive Accreditation Manual for Hospitals: The Official Handbook, Jan 2007:PC42-44.
• OSF Saint Francis Medical Center ORGANIZATIONAL POLICY: PROVISION OF CARE, Procedural Sedation/Analgesia by Non-Anesthesiologists, 12/08.
• Procedural Sedation for Clinicians, Teaching Module for Initial Appointment, Barnes-Jewish Hospital, 5/08.
• Sedation by Non-Anesthesia Personnel for Procedures. (2007) BJH Policy/Procedure/Guideline.
• www.medscape.com
