prof. josaphine - diabetic upper limb
TRANSCRIPT

8/3/2019 Prof. Josaphine - Diabetic Upper Limb
http://slidepdf.com/reader/full/prof-josaphine-diabetic-upper-limb 1/35
Diabetic Limb ProblemDiabetic Limb Problem
* Upper Limb Presentation* Upper Limb PresentationDr. Josephine WingDr. Josephine Wing--yukyuk IpIp
Division Chief Division Chief
Division of Hand & Foot SurgeryDivision of Hand & Foot Surgery
Department of Department of OrthopaedicsOrthopaedics && TraumatologyTraumatology
Queen Mary HospitalQueen Mary Hospital
The University of Hong KongThe University of Hong Kong
8/3/2019 Prof. Josaphine - Diabetic Upper Limb
http://slidepdf.com/reader/full/prof-josaphine-diabetic-upper-limb 2/35
Diabetic hand infectionDiabetic hand infection
DM hand is currently not generallyDM hand is currently not generally
classified as common complicationclassified as common complicationof DM as in foot problemsof DM as in foot problems
Western literature: (1999) 10%Western literature: (1999) 10%
incidence of DM hand infection thatincidence of DM hand infection thatrequires hospital admission; which isrequires hospital admission; which iscomparable to foot infectioncomparable to foot infection
PathoPatho--mechanism similar to footmechanism similar to foot
8/3/2019 Prof. Josaphine - Diabetic Upper Limb
http://slidepdf.com/reader/full/prof-josaphine-diabetic-upper-limb 3/35
The HandThe Hand
Similar anatomy to foot, developSimilar anatomy to foot, develop
from limb budfrom limb bud
Different functional demand: ADL &Different functional demand: ADL &
workwork
Closer to the heart:Closer to the heart: vascularityvascularity isis
better, less extensive skin necrosisbetter, less extensive skin necrosis
Nerve cells with shorter axon: LessNerve cells with shorter axon: Less
prone to significant sensory deficit &prone to significant sensory deficit &
motor deficitmotor deficit

8/3/2019 Prof. Josaphine - Diabetic Upper Limb
http://slidepdf.com/reader/full/prof-josaphine-diabetic-upper-limb 4/35
Predisposition to infection inPredisposition to infection in
diabetic limbdiabetic limb High blood sugar levelHigh blood sugar level
Impaired immune responseImpaired immune response Loss of protective sensation, less so in handLoss of protective sensation, less so in hand – –
less chance of unaware bacterialess chance of unaware bacteria innoculationinnoculation &&tissue damagetissue damage
Motor deficit resulting in deformities, lessMotor deficit resulting in deformities, lesscommon in handcommon in hand
Rapid progression of infection along tendonsRapid progression of infection along tendons
Further tissue necrosis & infectionFurther tissue necrosis & infection
Septic thrombosis: digital, metatarsal moreSeptic thrombosis: digital, metatarsal morefrequent/ rarely metacarpalfrequent/ rarely metacarpal
Gangrene of tissueGangrene of tissue

8/3/2019 Prof. Josaphine - Diabetic Upper Limb
http://slidepdf.com/reader/full/prof-josaphine-diabetic-upper-limb 5/35
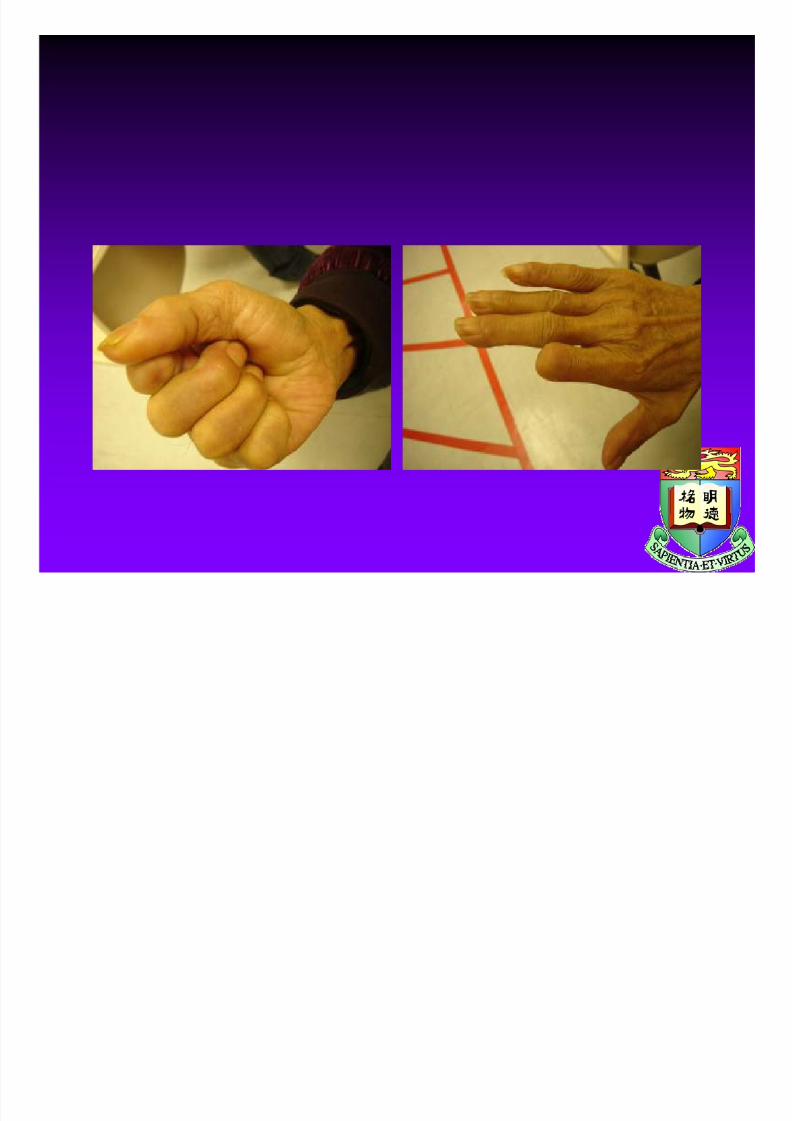
Diabetic hand with intrinsicDiabetic hand with intrinsic
minus deformitiesminus deformities

8/3/2019 Prof. Josaphine - Diabetic Upper Limb
http://slidepdf.com/reader/full/prof-josaphine-diabetic-upper-limb 6/35
The handThe hand Organ to contact outside worldOrgan to contact outside world
The most distal part is most prone to injuryThe most distal part is most prone to injuryi.e. the digiti.e. the digit
Special anatomy:Special anatomy: fascialfascial layers connectinglayers connecting
skin and underlying boneskin and underlying bone Many deep spaces ,multiple compartmentsMany deep spaces ,multiple compartments
in pulpin pulp
Infection raise compartment pressure, proneInfection raise compartment pressure, pronetoto ischaemiaischaemia & necrosis, underlying bone& necrosis, underlying bone
undergoesundergoes osteomyelitisosteomyelitis
8/3/2019 Prof. Josaphine - Diabetic Upper Limb
http://slidepdf.com/reader/full/prof-josaphine-diabetic-upper-limb 7/35
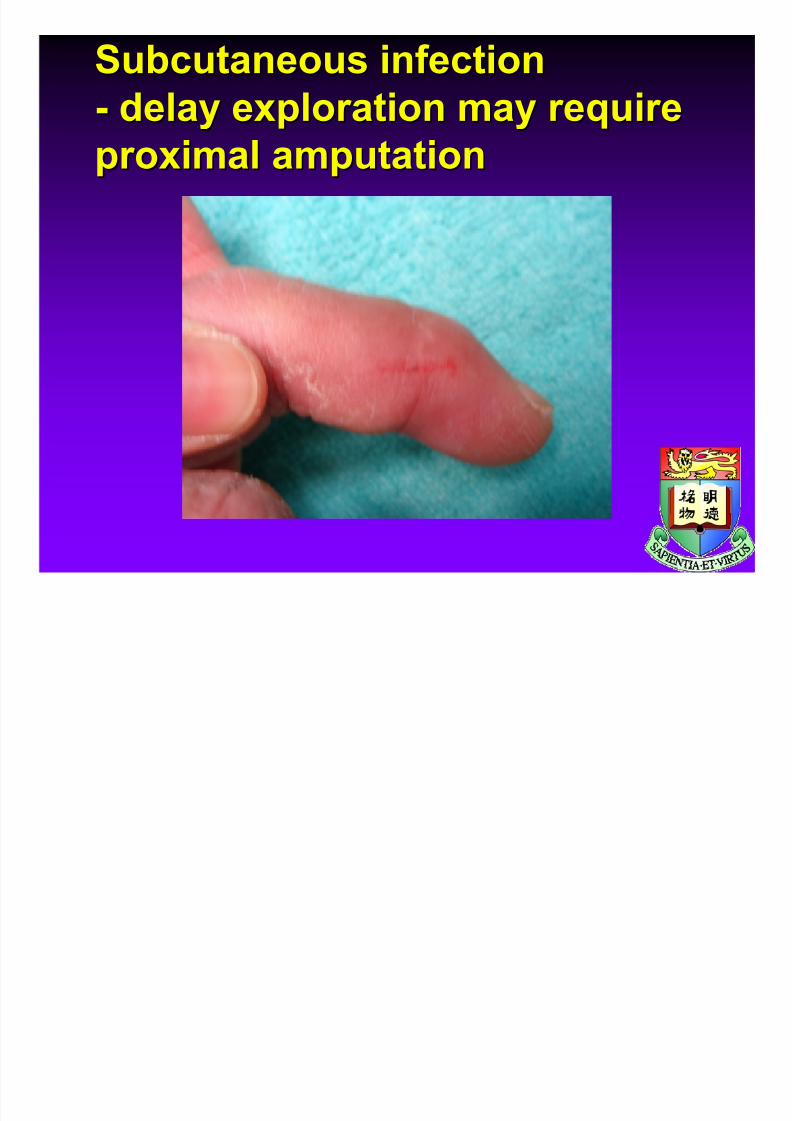
Subcutaneous infectionSubcutaneous infection
-- delay exploration may requiredelay exploration may requireproximal amputationproximal amputation

8/3/2019 Prof. Josaphine - Diabetic Upper Limb
http://slidepdf.com/reader/full/prof-josaphine-diabetic-upper-limb 8/35
Special demand of handSpecial demand of hand – –
motion, mo0tion, motionmotion, mo0tion, motion
The hand toleratesThe hand toleratesimmobilization poorlyimmobilization poorly
Adhesion between tissueAdhesion between tissue
layers develop easily: nolayers develop easily: nomanman’’s lands land
Stiff digit affects overallStiff digit affects overall
functionfunction
8/3/2019 Prof. Josaphine - Diabetic Upper Limb
http://slidepdf.com/reader/full/prof-josaphine-diabetic-upper-limb 9/35
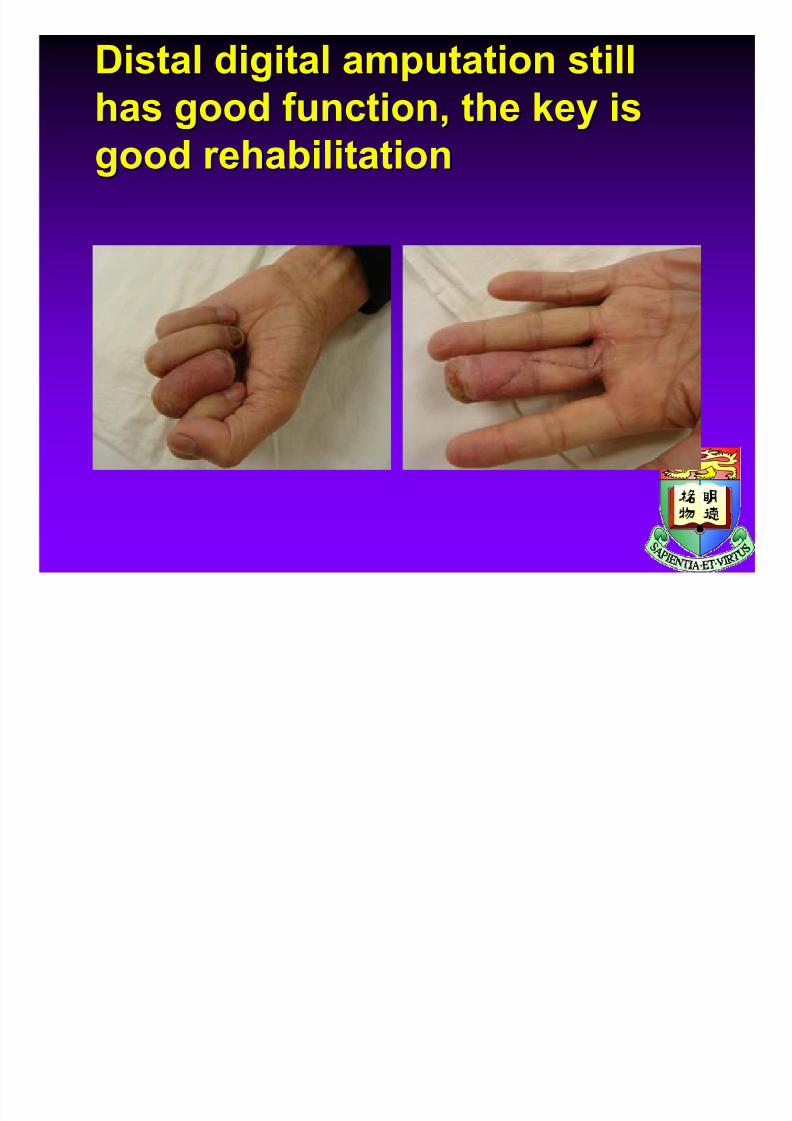
Distal digital amputation stillDistal digital amputation still
has good function, the key ishas good function, the key isgood rehabilitationgood rehabilitation
8/3/2019 Prof. Josaphine - Diabetic Upper Limb
http://slidepdf.com/reader/full/prof-josaphine-diabetic-upper-limb 10/35
Types of Infection inTypes of Infection in
diabetic limbdiabetic limb
CellulitisCellulitis
ParonychiaParonychia
PulpPulp
Web spaceWeb space
TenosynovitisTenosynovitis
Plantar Plantar spaces:medial,lateral,centralspaces:medial,lateral,central
Palmar Palmar
spaces:spaces:
thenar thenar
,,
hypothenar hypothenar
, mid, mid
--
palmar palmar
OsteomyelitisOsteomyelitis
Septic arthritisSeptic arthritis

8/3/2019 Prof. Josaphine - Diabetic Upper Limb
http://slidepdf.com/reader/full/prof-josaphine-diabetic-upper-limb 11/35
PParonychiaaronychia
common infectioncommon infection
8/3/2019 Prof. Josaphine - Diabetic Upper Limb
http://slidepdf.com/reader/full/prof-josaphine-diabetic-upper-limb 12/35
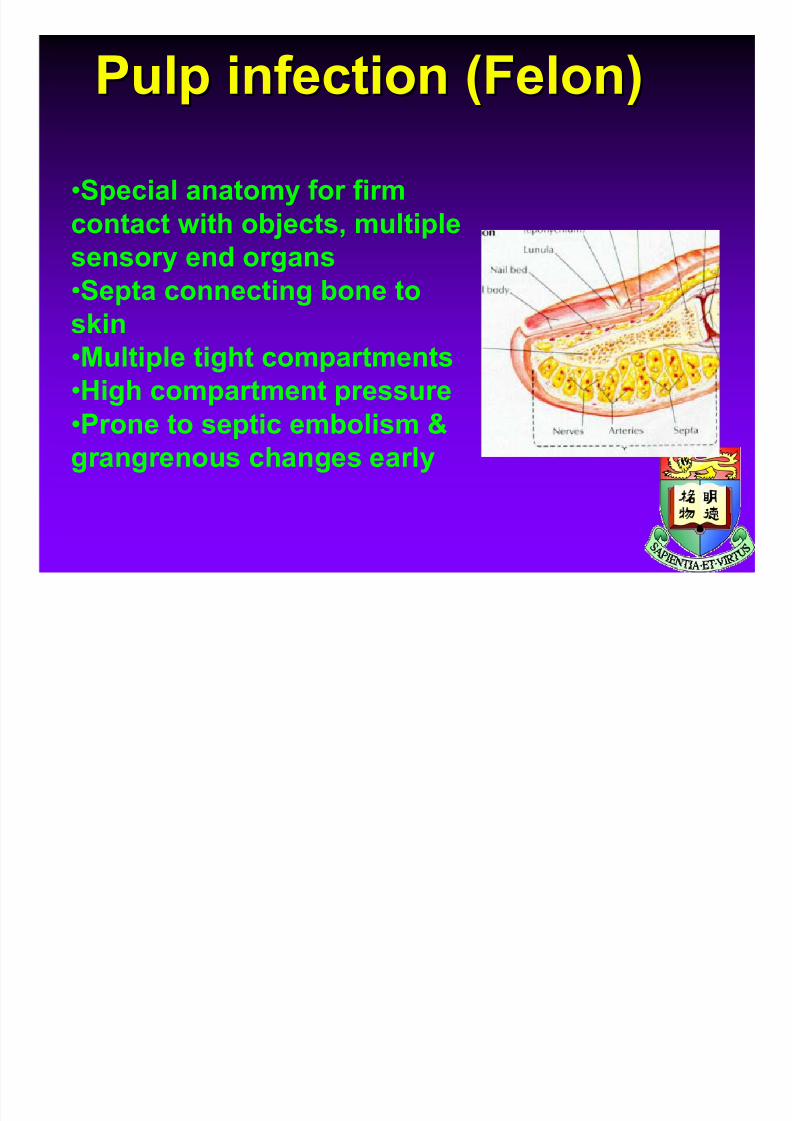
Pulp infection (Felon)Pulp infection (Felon)
•Special anatomy for firm
contact with objects, multiplesensory end organs
•Septa connecting bone to
skin•Multiple tight compartments
•High compartment pressure
•Prone to septic embolism &
grangrenous changes early

8/3/2019 Prof. Josaphine - Diabetic Upper Limb
http://slidepdf.com/reader/full/prof-josaphine-diabetic-upper-limb 13/35
Pulp infection resulting in pulpPulp infection resulting in pulp
gangrene, earlygangrene, early fasciotomyfasciotomy &&drainage may salvage itdrainage may salvage it

8/3/2019 Prof. Josaphine - Diabetic Upper Limb
http://slidepdf.com/reader/full/prof-josaphine-diabetic-upper-limb 14/35
Web space infectionWeb space infection
need volar & dorsal incision for need volar & dorsal incision for drainagedrainage
8/3/2019 Prof. Josaphine - Diabetic Upper Limb
http://slidepdf.com/reader/full/prof-josaphine-diabetic-upper-limb 15/35
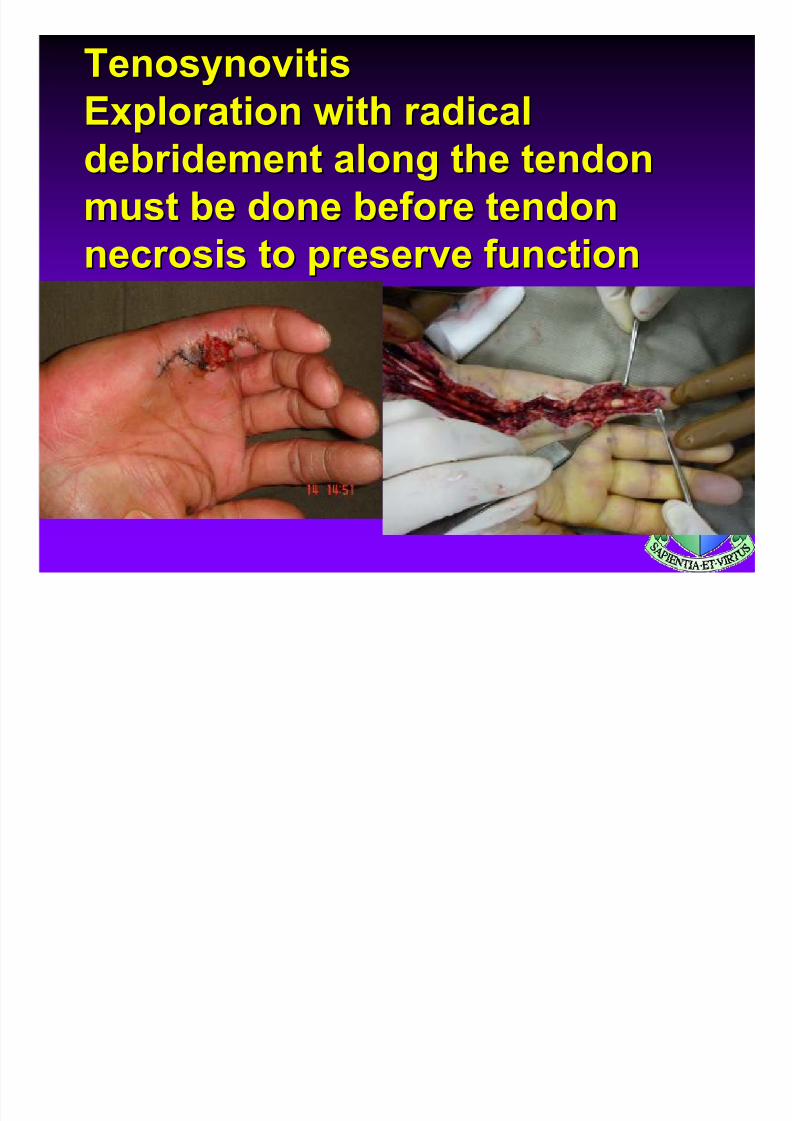
TenosynovitisTenosynovitis
Exploration with radicalExploration with radicaldebridement along the tendondebridement along the tendon
must be done before tendonmust be done before tendonnecrosis to preserve functionnecrosis to preserve function

8/3/2019 Prof. Josaphine - Diabetic Upper Limb
http://slidepdf.com/reader/full/prof-josaphine-diabetic-upper-limb 16/35
MidMid--palmar palmar space infectionspace infection
Late presentation as it startedLate presentation as it startedwith edematous hand onlywith edematous hand only
8/3/2019 Prof. Josaphine - Diabetic Upper Limb
http://slidepdf.com/reader/full/prof-josaphine-diabetic-upper-limb 17/35
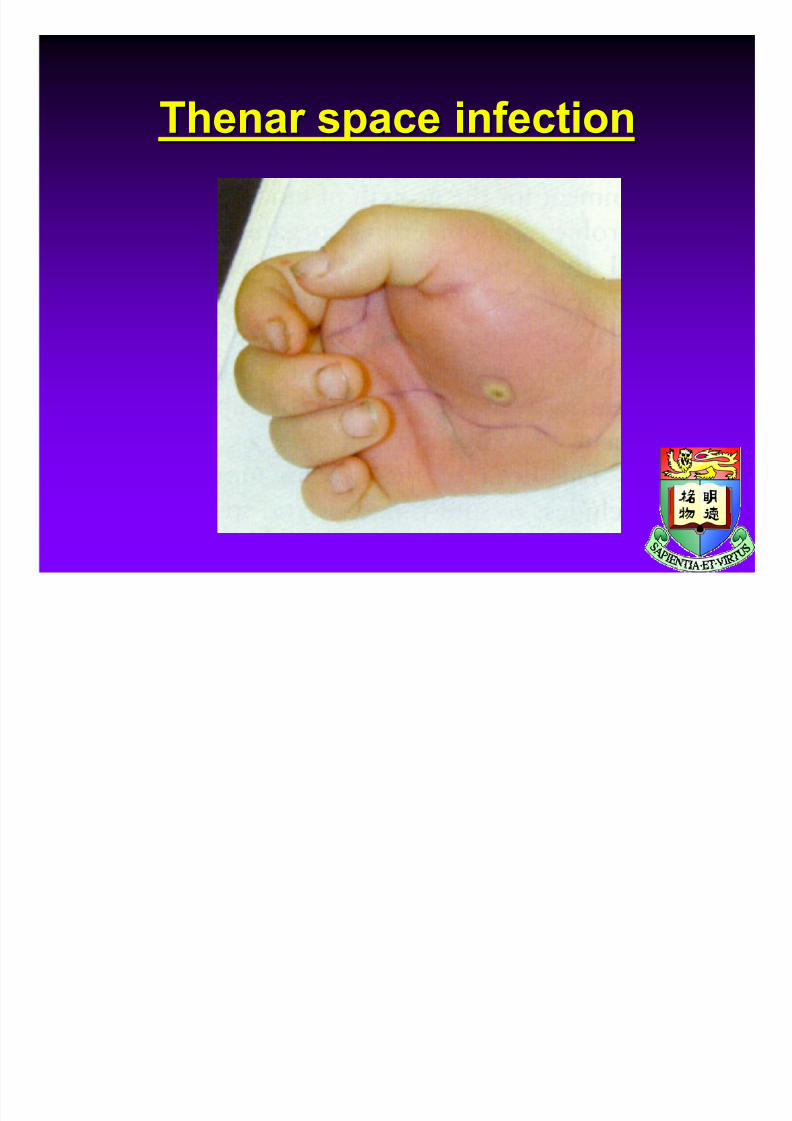
Thenar Thenar space infectionspace infection

8/3/2019 Prof. Josaphine - Diabetic Upper Limb
http://slidepdf.com/reader/full/prof-josaphine-diabetic-upper-limb 18/35
OsteomyelitisOsteomyelitis arising fromarising from
pulp infectionpulp infection

8/3/2019 Prof. Josaphine - Diabetic Upper Limb
http://slidepdf.com/reader/full/prof-josaphine-diabetic-upper-limb 19/35
Septic arthritisSeptic arthritis
8/3/2019 Prof. Josaphine - Diabetic Upper Limb
http://slidepdf.com/reader/full/prof-josaphine-diabetic-upper-limb 20/35
Hong Kong Chinese DiabetesHong Kong Chinese DiabetesPrevalencePrevalence
DM is 11%, around 700,000DM is 11%, around 700,000(700,000)(700,000)
DM hand: expect significant No.,DM hand: expect significant No.,
but no epidemiological data atbut no epidemiological data atpresentpresent
((KoKo GTC et al.GTC et al. TwoTwo- - hour post hour post - - glucose loading glucose loading plasma glucose is the main determinant for the plasma glucose is the main determinant for the progression from impaired glucose tolerance to progression from impaired glucose tolerance todiabetes mellitus in Hong Kong Chinese (letter)diabetes mellitus in Hong Kong Chinese (letter)..Diabetes Care 1999;22: 2096Diabetes Care 1999;22: 2096--2097.)2097.)

8/3/2019 Prof. Josaphine - Diabetic Upper Limb
http://slidepdf.com/reader/full/prof-josaphine-diabetic-upper-limb 21/35
Analysis of hand infectionAnalysis of hand infection
cases 2006cases 2006--20102010
Retrospective reviewRetrospective review Protocol:Protocol:
-- Rest in boxing glove, elevationRest in boxing glove, elevation
in hospitalin hospital

8/3/2019 Prof. Josaphine - Diabetic Upper Limb
http://slidepdf.com/reader/full/prof-josaphine-diabetic-upper-limb 22/35
-- Broad spectrum IV antibiotics coveringBroad spectrum IV antibiotics covering
gramgram-- and anaerobes : initiallyand anaerobes : initially AmpicillinAmpicillin++
CloxacillinCloxacillin ++ GentamycinGentamycin
-- Aggressive early debridement if there isAggressive early debridement if there is
pus collection or symptoms of infectionpus collection or symptoms of infection
not resolving within 24 hoursnot resolving within 24 hours
-- Liberal reLiberal re--exploration at intervals tillexploration at intervals till
clearance of infection, early decision onclearance of infection, early decision on
digital amputationdigital amputation
-- Early intervention by hand therapists toEarly intervention by hand therapists to
regain hand functionregain hand function

8/3/2019 Prof. Josaphine - Diabetic Upper Limb
http://slidepdf.com/reader/full/prof-josaphine-diabetic-upper-limb 23/35
Features of hand infection inFeatures of hand infection in
DM compared with nonDM compared with non--DMDM
More rapid in progressionMore rapid in progression More extensive involvementMore extensive involvement
More severe tissue involvementMore severe tissue involvement Frequently mixed organisms, gramFrequently mixed organisms, gram
negative organisms Vs gram positivenegative organisms Vs gram positive
organisms in nonorganisms in non--DMDM

8/3/2019 Prof. Josaphine - Diabetic Upper Limb
http://slidepdf.com/reader/full/prof-josaphine-diabetic-upper-limb 24/35
Epidemiological dataEpidemiological data
37 patients37 patients Average age 62(23Average age 62(23--87)87)
Male: 24 (64%), female: 13(36%)Male: 24 (64%), female: 13(36%)
Diagnosis of DM:Diagnosis of DM:--knownknown
-- previously unknown, diagnosed after 1previously unknown, diagnosed after 1stst
episode of hand infectionepisode of hand infection
Insulin injection:10Insulin injection:10 Oral medication 27, 5 need to switch toOral medication 27, 5 need to switch to
insulin injection during hospital stayinsulin injection during hospital stay
8/3/2019 Prof. Josaphine - Diabetic Upper Limb
http://slidepdf.com/reader/full/prof-josaphine-diabetic-upper-limb 25/35
AetiologyAetiology
Trauma 10(27%)Trauma 10(27%) Fish fin injury 8(22%)Fish fin injury 8(22%)
Animal bite 2(5.4%)Animal bite 2(5.4%) Acute on chronic nail infection 2(5.4%)Acute on chronic nail infection 2(5.4%)
CannulaCannula site infection 1(2.7%)site infection 1(2.7%)
PostPost--operation infection 1(2.7%)operation infection 1(2.7%)
Unknown 13(35%)Unknown 13(35%)

8/3/2019 Prof. Josaphine - Diabetic Upper Limb
http://slidepdf.com/reader/full/prof-josaphine-diabetic-upper-limb 26/35
Severity of infectionSeverity of infection
SuperficialSuperficial – – involving skin &involving skin &subcutaneous tissuesubcutaneous tissue
DeepDeep – – involving fascia, tendon,involving fascia, tendon,
muscle, bone & jointmuscle, bone & joint

8/3/2019 Prof. Josaphine - Diabetic Upper Limb
http://slidepdf.com/reader/full/prof-josaphine-diabetic-upper-limb 27/35
Pathological diagnosisPathological diagnosis
Subcutaneous abscess 15(40.5%)Subcutaneous abscess 15(40.5%) Felon 9(24.3%)Felon 9(24.3%)
TenosynovitisTenosynovitis 5(13.5%)5(13.5%) OsteomyelitisOsteomyelitis 2(5.4%)2(5.4%)
NecrotizingNecrotizing fasciitisfasciitis 2(5.4%)2(5.4%)
Septic arthritis 1(2.7%)Septic arthritis 1(2.7%)

8/3/2019 Prof. Josaphine - Diabetic Upper Limb
http://slidepdf.com/reader/full/prof-josaphine-diabetic-upper-limb 28/35
Length of hospital stayLength of hospital stay
Superficial: 9.6 daysSuperficial: 9.6 days Deep: 15.54 daysDeep: 15.54 days
P=0.002P=0.002
8/3/2019 Prof. Josaphine - Diabetic Upper Limb
http://slidepdf.com/reader/full/prof-josaphine-diabetic-upper-limb 29/35
MicroMicro--organismsorganisms
Mixed growth 15 (41%)Mixed growth 15 (41%) Gram positive 8 (22%)Gram positive 8 (22%)
Gram negative 4 (11%)Gram negative 4 (11%)
Fungus 2 (5%)Fungus 2 (5%)
No growth 8 (22%)No growth 8 (22%)
Most common organisms in mixed growth:Most common organisms in mixed growth:
StaphlcoccusStaphlcoccus,, KlebsiellaKlebsiella

8/3/2019 Prof. Josaphine - Diabetic Upper Limb
http://slidepdf.com/reader/full/prof-josaphine-diabetic-upper-limb 30/35
No. of operationNo. of operation
Single operation: 37.8%Single operation: 37.8% Multiple operations: 62.2%Multiple operations: 62.2%
Flap coverage of distal digit to preserveFlap coverage of distal digit to preserve
length was not always preferred as itlength was not always preferred as it
may delay rehabilitationmay delay rehabilitation

8/3/2019 Prof. Josaphine - Diabetic Upper Limb
http://slidepdf.com/reader/full/prof-josaphine-diabetic-upper-limb 31/35
Digital amputationDigital amputation
6/37 :16%6/37 :16% Early decision to hasten rehabilitationEarly decision to hasten rehabilitation
4 with mixed growth, 2 with single/no4 with mixed growth, 2 with single/no
identifiable organismidentifiable organism 5/6 started with pulp infection5/6 started with pulp infection
Reported amputation rate in literature:12Reported amputation rate in literature:12--38%; depends heavily on management38%; depends heavily on managementconceptconcept

8/3/2019 Prof. Josaphine - Diabetic Upper Limb
http://slidepdf.com/reader/full/prof-josaphine-diabetic-upper-limb 32/35
Digital amputation was performedDigital amputation was performed
after 1after 1stst debridement confirmeddebridement confirmedthat multiple procedures tothat multiple procedures to
preserve length will end up withpreserve length will end up with
poorer functionpoorer function

8/3/2019 Prof. Josaphine - Diabetic Upper Limb
http://slidepdf.com/reader/full/prof-josaphine-diabetic-upper-limb 33/35
Key points in managementKey points in management Proper Proper glycaemicglycaemic control to decreasecontrol to decrease
immunopathyimmunopathy
Immobilization during acute infection inImmobilization during acute infection inpressure dressing (boxing glove) to slowpressure dressing (boxing glove) to slowdown spread and control edemadown spread and control edema
Early aggressive antibiotic management toEarly aggressive antibiotic management to
cover mixed growthcover mixed growth Aggressive exploration & radical repeatedAggressive exploration & radical repeated
debridement to control infectiondebridement to control infection
Digital amputation should be consideredDigital amputation should be considered
early if the digit is not able to achieveearly if the digit is not able to achievereasonable functionreasonable function
start hand rehabilitation early: at day of start hand rehabilitation early: at day of
presentation, keep nonpresentation, keep non
--infected partsinfected parts
mobilemobile
8/3/2019 Prof. Josaphine - Diabetic Upper Limb
http://slidepdf.com/reader/full/prof-josaphine-diabetic-upper-limb 34/35

8/3/2019 Prof. Josaphine - Diabetic Upper Limb
http://slidepdf.com/reader/full/prof-josaphine-diabetic-upper-limb 35/35
Thank youThank youE mail:E mail:
[email protected]@hkucc.hku.hk