professor soo downe
TRANSCRIPT

‘Which horses for which courses? The EBM Problem in studies of
pharmacological substances in maternity care
Soo Downe University of Belfast September 10th 2015 Alcohol & Medica-ons in Pregnancy: Sharing Research Evidence on Recrea-onal and Prescribed Substances.
Penthouse Suite, Europa Hotel Belfast. With thanks to all who gave permission for their images to be used

CreaGng formal acceptable knowledge

• Theory-‐pracGce gap
• ‘Ivory towers’ and real life…

On the high ground, manageable problems lend themselves to soluGon through the applicaGon of research method and theory…

‘In the swampy lowland, messy confusing problems defy technical soluGon.. [these are]…the problems of greatest human concern’ Schon 1983 The Reflec1ve Prac11oner: How professionals think in ac1on. London: Temple Smith, p14

Impact of medicaGons during pregnancy on the fetus
…A 2011 study of medica1ons approved by the Food and Drug Administra1on (FDA) from 1980 through 2010 found that 91% of the medica1ons approved for use in adults lacked sufficient data to determine the risk of birth defects due to use of [those] medica1ons during pregnancy….

Why this maSers… DiethylsGlbestrol (DES)
• Oestrogen mimic
• Used from the 1940s to the 1970s to prevent miscarriage.
Impact on 1st genera1on
• Increased risk of breast cancer (approximately doubled in exposed women).

US
NaGonal Cancer InsGtute DES
follow-‐up study: 1992
onwards (Hoover et al
2011)

How did we know this?
“Our study…documents elevated risk for DES-‐exposed daughters for a host of medical problems—many of them also quite common in the general populaGon…Without the senGnel finding of a very rare cancer in young women, and without the sustained follow-‐up of those who were exposed, we would not know the full extent of harm caused by DES exposure in the womb.”
Robert N. Hoover, M.D., director of the Epidemiology and Biosta1s1cs Program in NCI’s Division of Cancer Epidemiology and Gene1cs.

Impact on future generaGons… ? EpigeneGc influence?
Impact on 3rd genera1on
• QuesGonnaire to 793 women whose mothers had documented in-‐utero DES exposure.
• Mean age of menstruaGon the same
• Daughters of exposed women regularized menstruaGon later
(mean 16.2 years vs. 15.8 years; p = 0.05), • More likely to report irregular menstrual periods
( OR = 1.54 (95% CI 1.02-‐2.32))
• Daughters of exposed women had fewer live births (1.6) than the unexposed (1.9) (P = 0.005).

The current situaGon in terms of drugs and pregnancy (USA)
(Adam et al 2011)
• Majority of women: at least one medicaGon during pregnancy
• Review of safety of 172 drugs approved by FDA from 2000 to 2010, and 468 drugs approved 1980-‐2000
• TERIS risk raGng system • Teratogenic risk in human pregnancy "undetermined" for 168 (97.7%) of drug treatments approved between 2000 and 2010.
• No data regarding safety available for 126 (73.3%) of these drugs.

We are doing beSer now…? (Adam et al 2011 cont)
Drugs approved between 1980 and 2000: only 23 (5%) changed a full risk category or more in the past 10 years.
Revised risks were derived from:
exposure cohort studies/record linkage studies, teratogen informaGon services,
large populaGon-‐based case-‐control studies pregnancy registries
(animal studies?)
The mean Gme for a treatment to move from an "undetermined" risk to be assigned a more precise risk was 27 years (95% confidence interval 26-‐28 years)

Unknown unknowns…

Pregnant women who need medicaGon.. Women with epilepsy (+/-‐ anG-‐epilepGcs) vs no
epilepsy
.
outcome OR 95% CI for OR
miscarriage 1.54 1·∙02-‐2·∙32
APH 1.49 1·∙01-‐2·∙20
PPH 1.29 1·∙13-‐1·∙49
Hypertension 1.37 1·∙21-‐1·∙55
InducGon 1.67 1·∙31-‐2·∙11
CS 1.40 1·∙23-‐1·∙58
Preterm birth 1.16 1·∙01-‐1·∙34
Fetal growth restricGon
1.26 1·∙20-‐1·∙33


RouGne use of medicaGon for all/most: and what about labour?
• Short term benefits/long term risks?
• Why are drugs our default posiGon?
• AlternaGves with less risks? – InducGon of labour to reduce CS
in healthy women and babies (: OR
– RelaGonship based conGnuity of care/out of hospital birth (added benefits for preterm birth)

‘AlternaGve’ sesngs (Cochrane review) Hodnett ED, Downe S, Walsh D, Weston J 2010"
• for the care of pregnant women who prefer and require liSle or no medical intervenGon.
• The sesngs may offer care throughout pregnancy and birth, or only during labour;
• they may be part of hospitals or freestanding enGGes.
AlternaGve sesngs: findings
10 trials; n = 11795
-‐ reduced likelihood of medical intervenGons
-‐ increased likelihood of : -‐ spontaneous vaginal birth, -‐ maternal saGsfacGon
-‐ conGnued breasueeding at 1-‐2 months postpartum
-‐ no risks to mother or baby.

Birthplace UK
•
• Birth is generally very safe (4.3/1000 adverse events). • MLU’s (alongside or freestanding: safe for the baby, benefits for the mother
• significantly fewer intervenGons, (fewer intrapartum caesarean secGons, and more ‘normal births’) than planned birth in an obstetric unit.
• Mul-parous women: home births and midwifery unit births safe for the baby, benefits for the mother

Midwife led care: evidence Sandall et al 2013
• 13 trials involving 16,242 women
• Women who had midwife-‐led conGnuity models of care were less likely to experience: – regional analgesia (RR 0.83, 95% CI 0.76 to 0.90)
– episiotomy ( RR 0.84, 95% CI 0.76 to 0.92), – instrumental birth (RR 0.88, 95% CI 0.81 to 0.96)
– preterm birth ( RR 0.77, 95% CI 0.62 to 0.94) – fetal loss before 24 weeks' gestaGon RR
0.81, 95% CI 0.66 to 0.99),

Sweden oxytocin outcomes: neonate Effects of induc1on and augmenta1on
• Oxytocin use and Apgar score < 7 at 5 min – OR 2.3; 95% CI 1.8-‐2.9
• Need for neonatal intensive care – OR 1.6; 95% CI 1.5-‐1.7)
• OperaGve birth – OR 4.0; 95% CI 3.7-‐4.2).

Longer term risks of the use of oxytocin? Induced foals up to 10 days postnatal
(Holdstock et al 2012)
• Differences in pancreaGc endocrine cell funcGon with delivery method were associated with 2-‐3 fold higher corGsol levels in the induced foals and with differences in the absolute and age-‐related changes in basal concentraGons of glucose, alpha-‐amino nitrogen and insulin.
• Induced delivery leads to changes in pancreaGc beta cell sensiGvity to glucose and/or Gssue insulin resistance in associaGon with persistent neonatal hypercorGsolaemia.

…pregnancy and birth intervenGons and non-‐communicable disease…?
• ?Feedback loops between the hormonal/physiological effects of pregnancy and birth and outcomes for the baby in later life:
• Type 1 diabetes
• Eczema
• Asthma
• MulGple sclerosis
• Some cancers (esp acute lymphoblasGc leukemia)
• Obesity
• Etc….
• …changes in white blood cell DNA-‐methylaGon in cord blood

Complex interplay between genes, epigeneGcs, life experiences, and our ‘Old Friends’?

What the World Health OrganisaGon says:
• ….Generally, between 70 and 80% of all pregnant women may be considered as low-‐risk at the start of labour.
• ….The uncriGcal adopGon of a range of unhelpful, unGmely, inappropriate and/or unnecessary intervenGons, all too frequently poorly evaluated, is a risk run by many who try to improve the maternity services…..
WHO hSp://www.who.int/reproducGvehealth/publicaGons/MSM_96_24/MSM_96_24_Chapter1.en.html

Taking account of the mother baby dyad: InverGng the evidence hierarchy for
pharmacological research…?
• Cohort studies • Case-‐control studies • PragmaGc RCT’s…
• (mulGmethod)
systemaGc reviews..
SystemaGc reviews with individual level data

N of one (?two?) studies

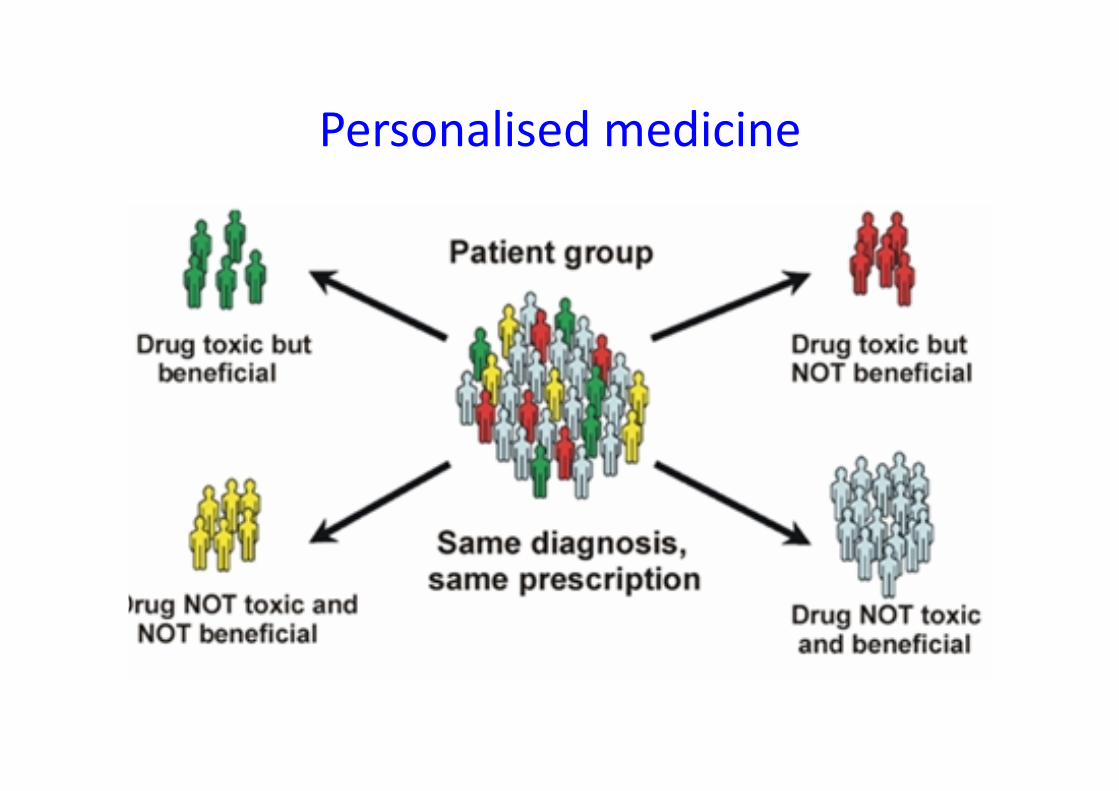
Personalised medicine

Taking account of placebo… Studies of doctors and diabeGc paGents
Hojat et al 2013
• Study one: 29 family physicians. 891 paGents (USA) – physicians’ higher scores on the Jefferson Scale of Empathy significantly
associated with indicators of diabeGc control
• Study two: 242 general pracGGoners, 20 961 paGents (Italy) – associaGon between higher physician empathy and lower incidence of
acute metabolic complicaGons that required hospitalisaGon

The real effect of placebo even in randomised trials
(issues of generalisibility of size of effect?)
• Pain relief scores. • 5 placebo-‐controlled single-‐dose parallel-‐group RCTs in acute postoperaGve pain
• 130/525 had a placebo. • Scores varied from 0 to 100% maximum possible pain relief.
• > 50% maximum possible pain relief across trials: – 7% to 37% with placebo – 5 to 63% with acGve drugs

Untangling to Gordian knot: Finding out what works…beyond RCT’s
• Full range of standard quanGtaGve methods
• QualitaGve research
• Realist research
• Mixed methods…
• Views of stakeholders, including service users

Gesng the balance right..

From knowledge hierarchies to a knowledge matrix
Pescrew M Roberts H 2003 Evidence, hierarchies, and typologies: horses for courses J Epidemiol Community Health 2003;57:527-‐529

Horses for courses: squaring the circle

Adam MP1, Poli~a JE, Friedman JM. Evolving knowledge of the teratogenicity of medicaGons in human pregnancy. Am J Med Genet C Semin Med Genet. 2011 Aug 15;157C(3):175-‐82. doi: 10.1002/ajmg.c.30313. Epub 2011 Jul 15. Hojat M, Louis DZ, Maio V, Gonnella JS. Empathy and health care quality. Am J Med Qual. 2013 (1):6-‐7. doi: 10.1177/1062860612464731. Holdstock NB, Allen VL, Fowden AL. PancreaGc endocrine funcGon in newborn pony foals a�er induced or spontaneous delivery at term. Equine Vet J Suppl. 2012 Feb;(41):30-‐7. Hoover RN, Hyer M, Pfeiffer RM, Adam E, Bond B, Cheville AL, Colton T, Hartge P, et al. Adverse Health Outcomes in Women Exposed In Utero to DiethylsGbestrol. NEJM. Oct. 6, 2011. 6,500 women (4,600 exposed and 1,900 unexposed), Lillie EO1, Patay B, Diamant J, Issell B, Topol EJ, Schork NJ The n-‐of-‐1 clinical trial: the ulGmate strategy for individualizing medicine? Per Med. 2011 Mar;8(2):161-‐173. McQuay H Carroll D Moore A VariaGon in the placebo effect in randomised controlled trials of analgesics: all is as blind as it seems Pain 64 ( 2) 331–335

Oscarsson ME, Amer-‐Wåhlin I, Rydhstroem H, Källén K. Outcome in obstetric care related to oxytocin use. A populaGon-‐based study. Acta Obstet Gynecol Scand. 2006;85(9):1094-‐8. Reed CE, Fenton SE. Exposure to diethylsGlbestrol during sensiGve life stages: a legacy of heritable health effects. Birth Defects Res C Embryo Today. 2013 Jun;99(2):134-‐46. doi: 10.1002/bdrc.21035. Schlinzig T, Johansson S, Gunnar A, Ekstr TJ, Norman M EpigeneGc modulaGon at birth -‐ altered DNA-‐methylaGon in white blood cells a�er Caesarean SecGon. Acta Paediatr. 2009 Jul;98(7):1096-‐9. Schon 1983 The ReflecGve PracGGoner: How professionals think in acGon. London: Temple Smith, p14 Titus-‐Ernstoff L, Troisi R, Hatch EE, Wise LA, Palmer J, Hyer M, Kaufman R, Adam E, et al Menstrual and reproducGve characterisGcs of women whose mothers were exposed in utero to diethylsGlbestrol (DES).”. Interna1onal Journal of Epidemiology 2006 35 (4): 862–8.
Viale L1, Allotey J2, Cheong-‐See F2, Arroyo-‐Manzano D3, Mccorry D4, Bagary M5, Mignini, Khan KS6, Zamora J7, ThangaraGnam S6; EBM CONNECT CollaboraGon. Epilepsy in pregnancy and reproducGve outcomes: a systemaGc review and meta-‐analysis. Lancet. 2015 Aug 25. pii: S0140-‐6736(15)00045-‐8. doi: 10.1016/S0140-‐6736(15)00045-‐8. [Epub ahead of print]