program year 2014 stage 2 meaningful use for eps health... · program year 2014 stage 2 meaningful...
TRANSCRIPT

New Mexico Human Services Department
Medical Assistance Division
Valorie A. Vigil, Staff Manager
Idalia Lechuga-Tena, Communications Manager
Systems Bureau
NM Medicaid EHR Incentive Program
Program Year 2014
Stage 2 Meaningful Use for EPs
This Webinar will cover the Stage 2 Objectives and Measures
We will walk through the Objectives and Measures as they
will appear in the NM State Level Registry
Only providers who have attested to two years of Stage 1 MU
are eligible to attest to Stage 2 MU
Under the CMS 2014 CEHRT Flexibility Rule, providers will
only be able to attest to AIU if they have fully implemented
2014 Edition CEHRT
2

Before attesting in the NM State Level Registry, providers are
strongly encouraged to attend the webinar: Program Year
2014— CMS 2014 CEHRT Flexibility Rule & NM State Level
Registry Changes
Or view the webinar slides on the State EHR Website under
the General Information tab:
http://www.hsd.state.nm.us/providers/general-
information.aspx
3

4
NEW EHR FINAL RULE
It is critical that providers know the CEHRT Edition,
Vendor Name and Product Version they are using
for the 90-day EHR Reporting Period
Work with your Vendor and IT Staff to determine the
above
Go to the ONC website to get correct EHR CEHRT
number:
http://oncchpl.force.com/ehrcert/CHPLHome

2014 CEHRT FLEXIBILITY = NM SLR CHANGES
Log into PY 2014 Attestation in the NM SLR
Type in ONC CEHRT Number
Provider will get a Set of Attestation Options based
on the CERHT Edition associated with the number
• Choose from MU Options Available
Only 2014 CEHRT Edition will have the Option for AIU
or Stage 2 MU
5

2014 CEHRT FLEXIBILITY = NM SLR CHANGES
The NM SLR will Determine the Set of Measures
Based on the Following:
◦ 2014 CEHRT No.—Characters 3-5 are 14E
◦ Combo 2011/2014 CEHRT No.—Characters 3-5 are H13
◦ 2011 CEHRT No.—If Characters 3-5 are any Combination other
than 14E or H13
6

The CEHRT number you have entered results in an option for
MU Stage 2 Objectives and Measures
7
*Only
providers
that could
not fully
implement
2014
Edition
CEHRT for
the EHR
reporting
period in
2014 due to
delays in
2014
Edition
CEHRT
availability
8
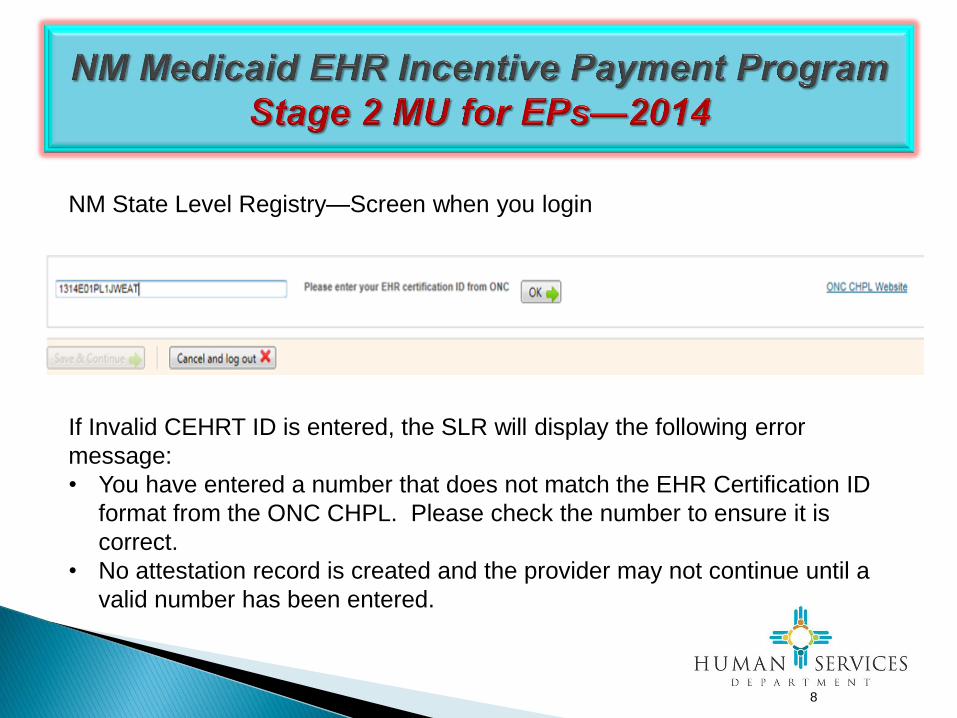
NM State Level Registry—Screen when you login
If Invalid CEHRT ID is entered, the SLR will display the following error
message:
• You have entered a number that does not match the EHR Certification ID
format from the ONC CHPL. Please check the number to ensure it is
correct.
• No attestation record is created and the provider may not continue until a
valid number has been entered.

9
NM State Level Registry—Screen when you login
Entering a 2014 CEHRT Edition Number allows 3 options;
• When Option 2 (second box) is selected, the SLR will create a set of
Stage 1 or Stage 2 objectives, measures and CQMs based on the
provider’s prior attestations.
10
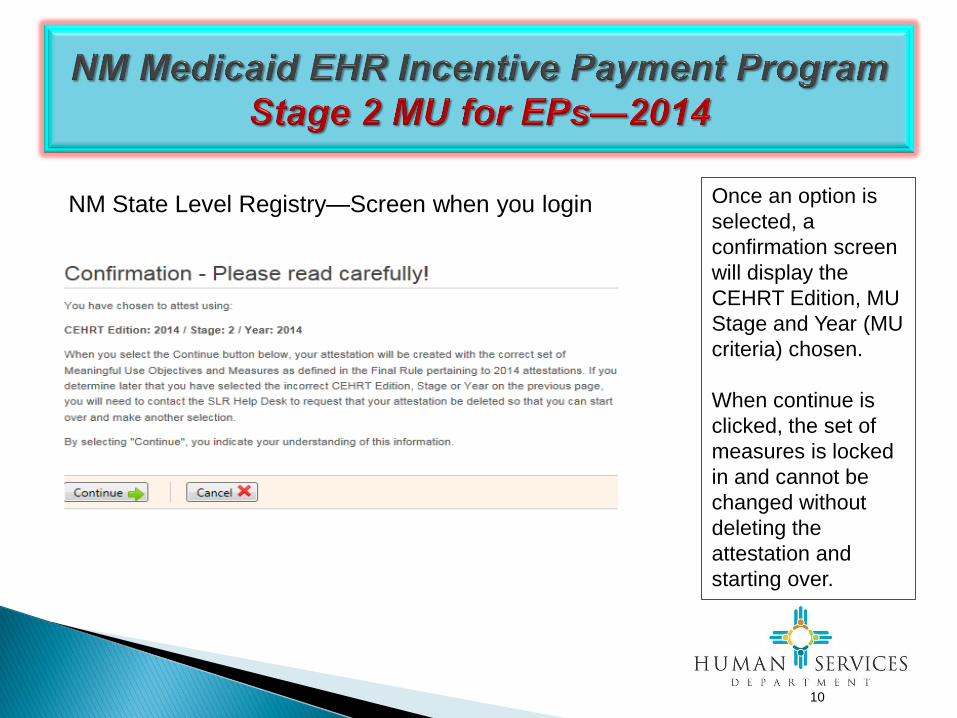
NM State Level Registry—Screen when you login Once an option is
selected, a
confirmation screen
will display the
CEHRT Edition, MU
Stage and Year (MU
criteria) chosen.
When continue is
clicked, the set of
measures is locked
in and cannot be
changed without
deleting the
attestation and
starting over.

Patient Volume Requirements
Step 2 in the State Level Registry
EPs need a minimum 30%
Medicaid PV for all patient
encounters over a continuous 90-
day Representative Period.
EPs may choose a 90-day
Representative Period from either:
the prior calendar year, OR
the preceding 12 months from date
of attestation
11

12
ONC CEHRT Number After login to PY 2014 Attestation
Step 3 in the SLR
Must have ONC CEHRT # each
Payment Year
First Payment Year: Attach
documentation—a vendor contract or
paid invoice on SLR Step 3
Subsequent Payment Years: If ONC
CEHRT # changes from prior year (new
version of EHR), attach vendor
documentation—a vendor contract or
paid invoice on SLR Step 3
PY 2014: Attach screenshot on SLR
Step 3
http://oncchpl.force.com/ehrcert/CHPLHome

13
IMPORTANT TO REMEMBER
The same product and version
may be listed under one or more
of the Edition tabs
However, the CEHRT number will
be different under each Edition
as shown on your left
Again, please verify with your
Vendor which CEHRT number
should be used
14
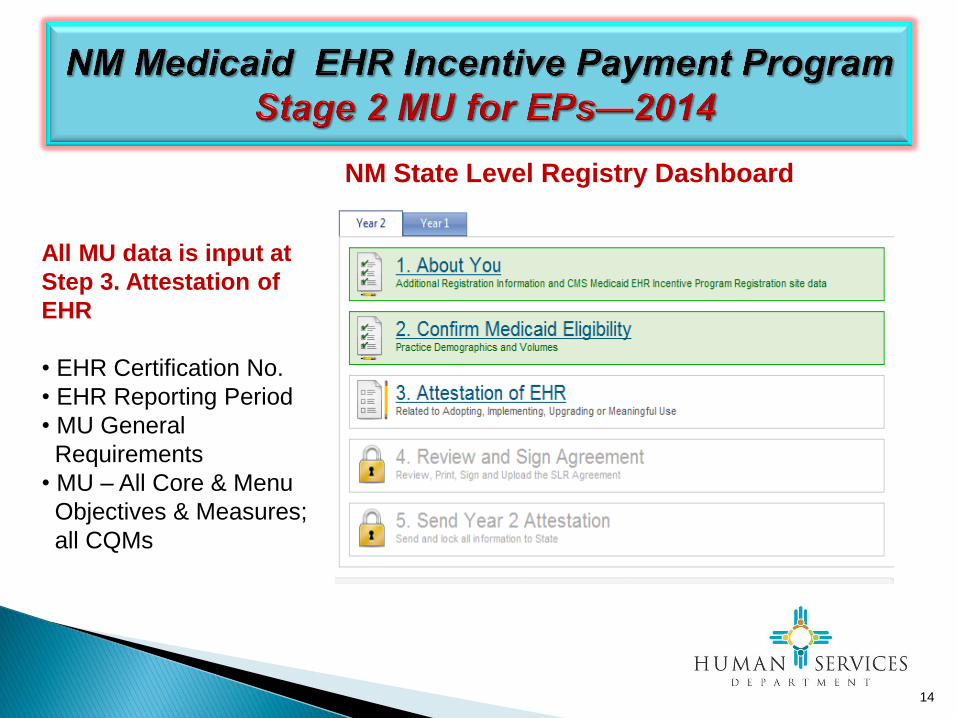
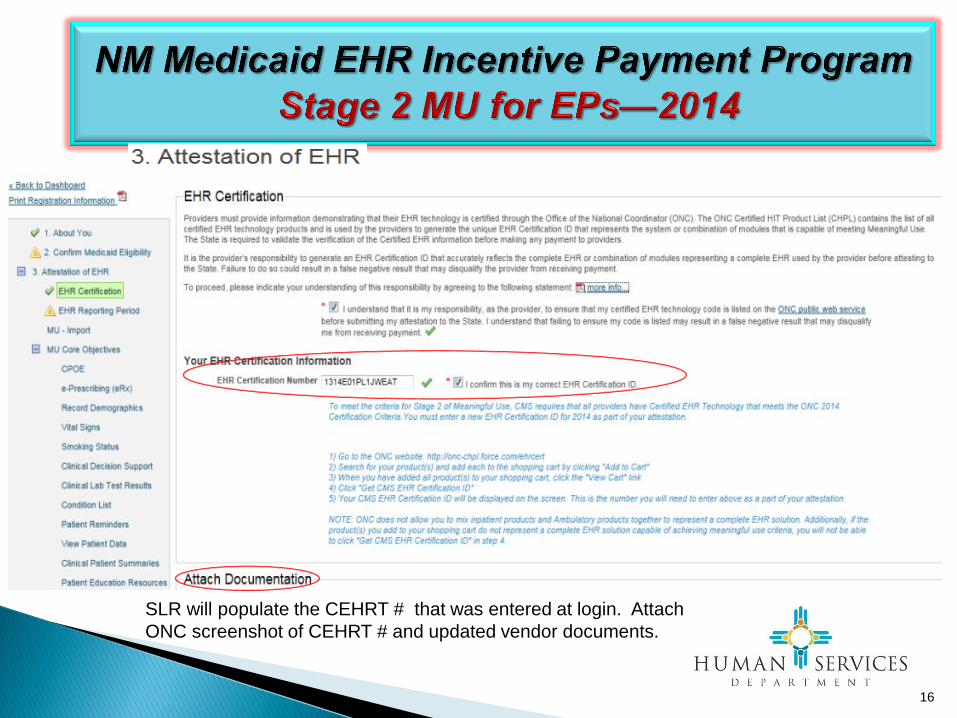
All MU data is input at
Step 3. Attestation of
EHR
• EHR Certification No.
• EHR Reporting Period
• MU General
Requirements
• MU – All Core & Menu
Objectives & Measures;
all CQMs
NM State Level Registry Dashboard

15
16
SLR will populate the CEHRT # that was entered at login. Attach
ONC screenshot of CEHRT # and updated vendor documents.

17
If the CEHRT # is changed on
Step 3 to a different CEHRT
Edition # that does not match the
CEHRT # entered at the
beginning of the attestation, you
will get an error message as
shown to the right.
NOTE: If the CEHRT Edition #
entered at login is incorrect, the
2014 attestation will have to be
deleted and the provider will
have to start over.

18
MU – Two General Requirements
At least 80% of unique patients must have their records
in a certified EHR during the EHR reporting period
Unique Patients = Number of patients seen in the EHR
reporting period. Patients seen more than once count only
once in the denominator.
For EPs who practice at multiple sites, at least 50% of
total patient encounters during the EHR reporting period
must be at location(s) with certified EHR technology
As long as an EP has certified EHR available for 50% or more
of their patient encounters during the EHR reporting period,
the EP only has to include those encounters where certified
EHR is available at the start of the EHR reporting period.

19

20
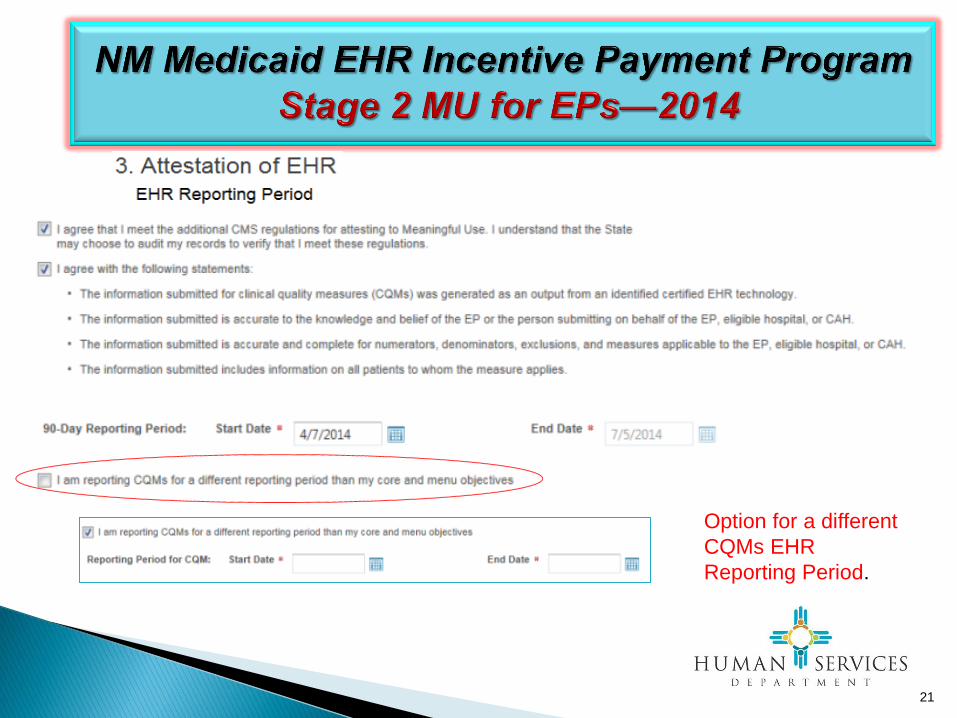
21
Option for a different
CQMs EHR
Reporting Period.

22
Reporting Requirements
Eligible Professionals
Meaningful Use 20 Objectives
CORE 17 Objectives
MENU 3 of 6
Objectives
Clinical Quality
Measures 9 Objectives
9 CQMs total out of 64
9 adult
9 pediatric
Any 9
2014– Stage 2

23
Stage 2 Objectives and Measures
2014 is the first year an EP can attest to Stage 2 MU if the EP
has already attested to two years of Stage 1 MU
Some Objectives have more than one Measure
Stage 2 Measures have higher thresholds than Stage 1
Immunization Measure moves to the Core set

24
2014
Stage 2 Core Set
Core Objectives: Must meet measures for all 17 Core Objectives or
meet an exclusion
•13 of the Core Objectives have percentage-based measures that require a
numerator and a denominator
• 4 of the Core Objectives have Y/N responses – did you perform the action
required in the measure?
• 4 of the Core Objectives have multiple measures
•14 of the Core Objectives have exclusion criteria

25
2014
Stage 2 Menu Set
Menu Measures: Must meet 3 out of 6 Menu Objectives without an
exclusion, or must attest to all 6 with some exclusions criteria.
•3 of the Menu Objectives have percentage-based measures that require a
numerator and a denominator
•3 of the Menu Objectives have Y/N responses – did you perform the action
required in the measure?
•6 of the Menu Objectives have exclusion criteria

26
2014—CQMs
Must report on 9 CQMs instead of 6 and choose from:
• 9 CQMs for adult populations; OR
• 9 CQMs for pediatric populations; OR
• 9 CQMs total from a list of 64
9 CQMs must be from 3 of 6 NQS key health care policy domains
1. Patient and Family Engagement
2. Patient Safety
3. Care Coordination
4. Population/Public Health
5. Efficient Use of Healthcare Resources
6. Clinical Process/Effectiveness
Data must be reported directly from information generated by CEHRT

Measure Types
Percentage-based Measures – Have a
Numerator and Denominator
Yes/No Measures
Some measures have exclusions
27

Exclusions
Based on all patients seen during the EHR reporting period – not
just those whose records are maintained in CEHRT
True even if the measure for the objective has the option to choose
only records maintained in the CEHRT
A “Yes” answer to a Core Measure exclusion meets the measure
A “No” answer to an exclusion means the EP has to meet the
required threshold for percentage-based measures or say “Yes” to
taking the required action on a “Yes/No” measure
If no exclusion criteria is offered, the EP must meet the measure
There are no exclusions based on provider type
28

Text Boxes in the NM SLR
• Require valid information be input
• Some are free text – must type something in
• Some are dropdown menus
• Some measures have more than one text box
29

Selection Pages & Detail Pages in the NM SLR
Each group of measures includes a Selection Page
which provides a place to access or select the
measures.
Each measure within a group also includes a Detail
Page where you input the data.
Use the Save & Continue button on each measure
Detail Page to move into the next measure requiring
input, or to the next Selection Page.
Navigation Menu is on left-hand side of each page.
30
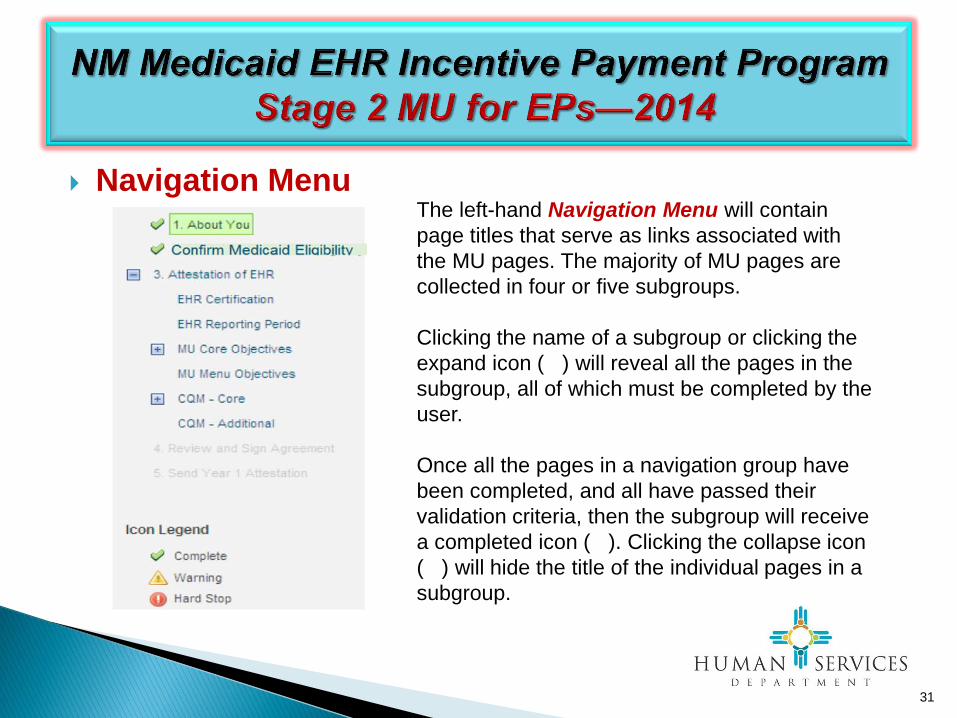
Navigation Menu
31
The left-hand Navigation Menu will contain
page titles that serve as links associated with
the MU pages. The majority of MU pages are
collected in four or five subgroups.
Clicking the name of a subgroup or clicking the
expand icon ( ) will reveal all the pages in the
subgroup, all of which must be completed by the
user.
Once all the pages in a navigation group have
been completed, and all have passed their
validation criteria, then the subgroup will receive
a completed icon ( ). Clicking the collapse icon
( ) will hide the title of the individual pages in a
subgroup.

32
NM Medicaid EHR Incentive Payment Program
Stage 2 MU for EPs—2014
Core Objectives
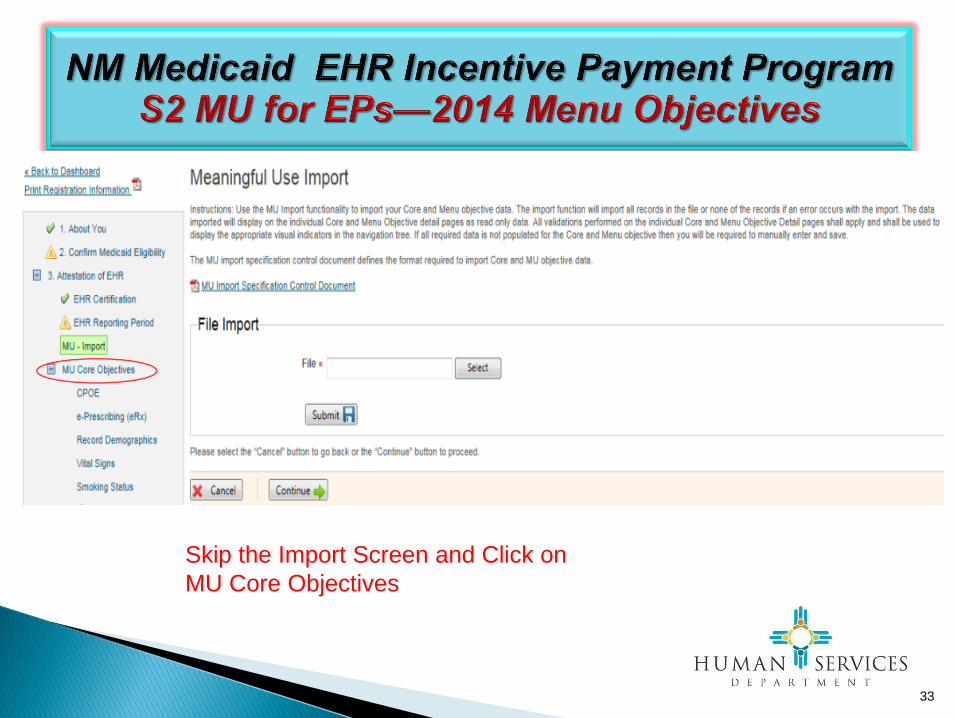
Skip the Import Screen and Click on
MU Core Objectives
33

34
NM Medicaid EHR Incentive Payment Program S2 MU for EPs—2014 Core Objectives

35

36
NM Medicaid EHR Incentive Payment Program S2 MU for EPs—2014 Core Objectives

37
Core Objective 1 – CPOE Definitions
Computerized Provider Order Entry (CPOE) – A provider's use of computer assistance to
directly enter medical orders (for example, medications, consultations with other providers,
laboratory services, imaging studies, and other auxiliary services) from a computer or mobile
device.
Laboratory and radiology orders are included as part of Stage 2 for CPOE:
Laboratory Order – Order for any service provided by a laboratory that could not be provided by
a non-laboratory.
Laboratory – A facility for the biological, microbiological, serological, chemical,
immunohematological, hematological, biophysical, cytological, pathological, or other examination
of from the human body for the purpose of providing information for the diagnosis, prevention, or
treatment of any disease or impairment of, or the assessment of the health of, human beings.
These examinations also include procedures to determine, measure, or otherwise describe the
presence or absence of various substances or organisms in the body. Facilities only collecting or
preparing specimens (or both) or only serving as a mailing service and not performing testing are
not considered laboratories.
Radiology Order – Order for any imaging services that uses electronic product radiation. The
EP can include orders for other types of imaging services that do not rely on electronic product
radiation in this definition as long the policy is consistent across all patient and for the entire EHR
reporting period.
38
Core Objective 1 – CPOE Definitions Continued
Electronic Product Radiation – Any ionizing or nonionizing electromagnetic or particulate
radiation, or [a]ny sonic, infrasonic, or ultrasonic wave that is emitted from an electronic product
as the result of the operation of an electronic circuit in such product.
Unique Patient – If a patient is seen by an EP more than once during the EHR reporting period,
then for purposes of measurement that patient is only counted once in the denominator for the
measure.
Objective: Use computerized provider order entry (CPOE) for medication, laboratory and radiology orders
directly entered by any licensed healthcare professional who can enter orders into the medical
record per state, local and professional guidelines.
Measure More than 60 percent of medication, 30 percent of laboratory, and 30 percent of radiology orders
created by the EP during the EHR reporting period are recorded using CPOE.
Exclusion Any EP who writes fewer than 100 medication, radiology, or laboratory orders during the EHR
reporting period.
39

Core Objective 1 – CPOE
Additional Information The provider is permitted, but not required, to limit the measure of this objective to those patients whose records are
maintained using certified EHR technology (CEHRT).
The CPOE function must be used to create the first record of the order that becomes part of the patient's medical record
and before any action can be taken on the order to count in the numerator.
However, in some situations it may be impossible or inadvisable to wait to initiate an intervention until a record of the order
has been created. For example, situations where an intervention is identified and immediately initiated by the provider, or
initiated immediately after a verbal order by the ordering provider to a licensed healthcare professional under his/her direct
supervision. Therefore in these situations, so long as the order is entered using CPOE by a licensed healthcare
professional or certified medical assistant to create the first record of that order as it becomes part of the patient’s medical
record, these orders would count in the numerator of the CPOE measure.
Any licensed healthcare professionals and credentialed medical assistants, can enter orders into the medical record for
purposes of including the order in the numerator for the objective of CPOE if they can originate the order per state, local
and professional guidelines. Credentialing for a medical assistant must come from an organization other than the
organization employing the medical assistant.
Electronic transmittal of the medication order is not a requirement for meeting the measure of this objective.
CPOE is the entry of the order into the patient's EHR that uses a specific function of CEHRT. It is not how that order is
filled or otherwise carried out.
In order to meet this objective and measure, an EP must use the capabilities and standards of CEHRT at 45 CFR
170.314(a)(1).
40

41

42

43
Core Objective 2 – e-Prescribing (eRx) Definitions:
Permissible Prescriptions – The concept of only permissible prescriptions refers to the current
restrictions established by the Department of Justice on electronic prescribing for controlled substances
in Schedule II-V. (The substances in Schedule II-V can be found at
http://www.deadiversion.usdoj.gov/schedules/orangebook/e_cs_sched.pdf ). Any prescription not subject
to these restrictions would be permissible.
Prescription – The authorization by an EP to a pharmacist to dispense a drug that the pharmacist would
not dispense to the patient without such authorization.
Objective:
Generate and transmit permissible prescriptions electronically (eRx).
Measure:
More than 50 percent of all permissible prescriptions, or all prescriptions, written by the EP are queried
for a drug formulary and transmitted electronically using CEHRT.
Exclusions:
Any EP who:
(1) Writes fewer than 100 permissible prescriptions during the EHR reporting period.
(2) Does not have a pharmacy within their organization and there are no pharmacies that accept
electronic prescriptions within 10 miles of the EP's practice location at the start of his/her EHR
reporting period.

44
45
Core Objective 3 – Record Demographics Definitions:
Preferred Language – The language by which the patient prefers to
communicate.
Unique Patient – If a patient is seen by an EP more than once during the EHR
reporting period, then for purposes of measurement that patient is only counted
once in the denominator for the measure. All the measures relying on the term
‘‘unique patient’’ relate to what is contained in the patient’s medical record. Not
all of this information will need to be updated or even be needed by the
provider at every patient encounter. This is especially true for patients whose
encounter frequency is such that they would see the same provider multiple
times in the same EHR reporting period.
Objective:
Record the following demographics: preferred language, sex, race, ethnicity,
date of birth.
Measure:
More than 80 percent of all unique patients seen by the EP have demographics
recorded as structured data.
Exclusion:
No exclusion.

46
Core Objective 3 – Record Demographics
Attestation Requirements:
DENOMINATOR: Number of unique patients seen by the EP during the EHR reporting period.
NUMERATOR: The number of patients in the denominator who have all the elements of demographics (or a
specific notation if the patient declined to provide one or more elements or if recording an element is contrary to
state law) recorded as structured data.
THRESHOLD: The resulting percentage must be more than 80 percent in order for an EP to meet this
measure.
Additional Information
If a patient declines to provide all or part of the demographic information, or if capturing a patient’s ethnicity or
race is prohibited by state law, such a notation entered as structured data would count as an entry for purposes
of meeting the measure. In regards to patients who do not know their ethnicity, EPs should treat these patients
the same way as patients who decline to provide race or ethnicity— identify in the patient record that the patient
declined to provide this information.
EPs are not required to communicate with the patient in his or her preferred language in order to meet the
measure of this objective.
The term “gender” in the Stage 1 objective is replaced with the term “sex” for Stage 2.

47

48

49
50

51

52
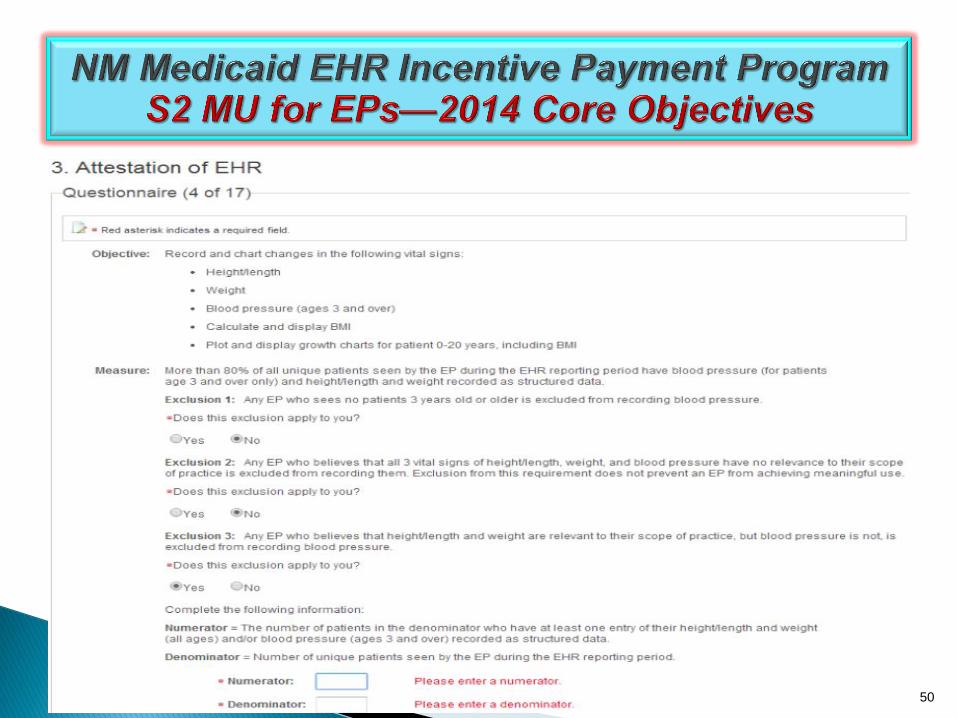
Core Objective 4 – Record Vital Signs
Definitions:
Unique Patient – If a patient is seen by an EP more than once during the EHR
reporting period, then for purposes of measurement that patient is only counted
once in the denominator for the measure. All the measures relying on the term
‘‘unique patient’’ relate to what is contained in the patient’s medical record. Not
all of this information will need to be updated or even be needed by the
provider at every patient encounter. This is especially true for patients whose
encounter frequency is such that they would see the same provider multiple
times in the same EHR reporting period.
Objective:
Record and chart changes in the following vital signs: height/length and weight
(no age limit); blood pressure (ages 3 and over); calculate and display body
mass index (BMI); and plot and display growth charts for patients 0-20 years,
including BMI.
53
Core Objective 4 – Record Vital Signs
Measure:
More than 80 percent of all unique patients seen by the EP have blood pressure (for patients age 3
and over only) and/or height and weight (for all ages) recorded as structured data.
Exclusion:
Any EP who:
(1) Sees no patients 3 years or older is excluded from recording blood pressure.
(2) Believes that all 3 vital signs of height/length, weight, and blood pressure have no relevance
to their scope of practice is excluded from recording them.
(3) Believes that height/length and weight are relevant to their scope of practice, but blood
pressure is not, is excluded from recording blood pressure.
(4) Believes that blood pressure is relevant to their scope of practice, but height/length and
weight are not, is excluded from recording height/length and weight.

54
55
56
Core Objective 5 – Record Smoking Status
Definitions:
Unique Patient – If a patient is seen by an EP more than once during the EHR
reporting period, then for purposes of measurement that patient is only counted once in
the denominator for the measure. All the measures relying on the term ‘‘unique patient’’
relate to what is contained in the patient’s medical record. Not all of this information will
need to be updated or even be needed by the provider at every patient encounter. This
is especially true for patients whose encounter frequency is such that they would see
the same provider multiple times in the same EHR reporting period.
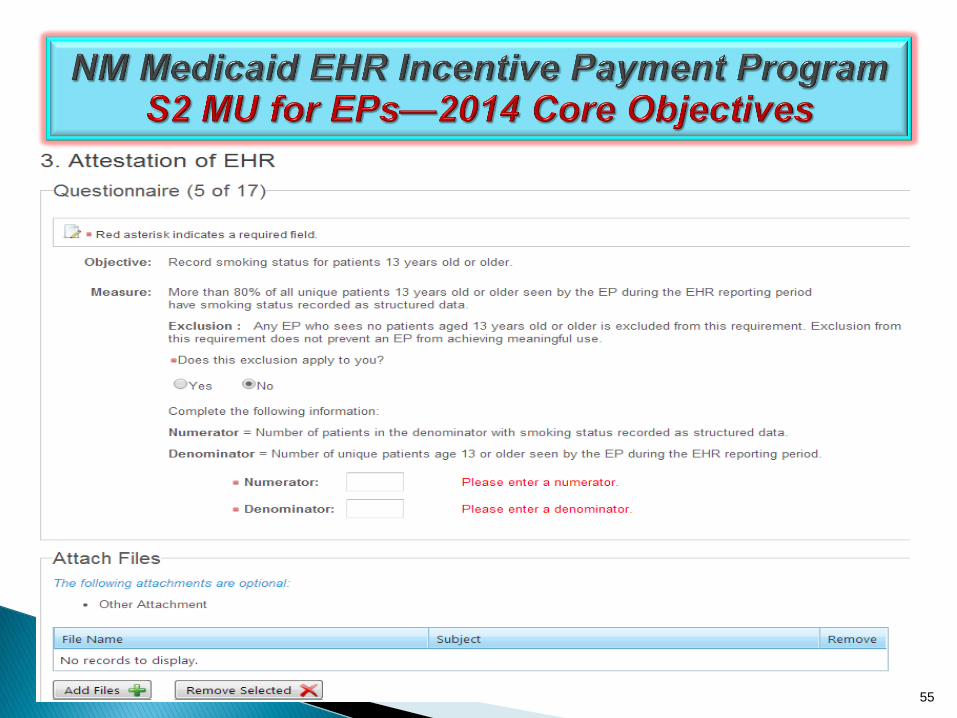
Objective:
Record smoking status for patients 13 years old or older.
Measure:
More than 80 percent of all unique patients 13 years old or older seen by the EP have
smoking status recorded as structured data.
Exclusion:
Any EP that neither sees nor admits any patients 13 years old or older.

57
NOTE: You must attest YES to meet the
attestation requirements

58
59

60
Core Objective 6 – Clinical Decision Support Rule
Definitions:
Clinical Decision Support – HIT functionality that builds upon the foundation of an EHR to
provide persons involved in care processes with general and person-specific information,
intelligently filtered and organized, at appropriate times, to enhance health and health care.
Objective:
Use clinical decision support to improve performance on high-priority health conditions.

61
Core Objective 6 – Clinical Decision Support Rule
Measure:
Measure 1: Implement five clinical decision support interventions related to four or more clinical
quality measures at a relevant point in patient care for the entire EHR reporting period. Absent four
clinical quality measures related to an EP’s scope of practice or patient population, the clinical
decision support interventions must be related to high-priority health conditions. Must attest YES
to this measure or EP will not meet Meaningful Use.
If none of the CQMs are applicable to an EP's scope of practice, the EP should implement
CDS interventions that he or she believes will drive improvements in the delivery of care for
the high-priority health conditions relevant to their patient population.
CMS will not issue additional guidance on the selection of appropriate clinical decision
support rules for Stage 2 Meaningful Use. This determination is best left to the EP taking into
account their workflow, patient population, and quality improvement efforts.
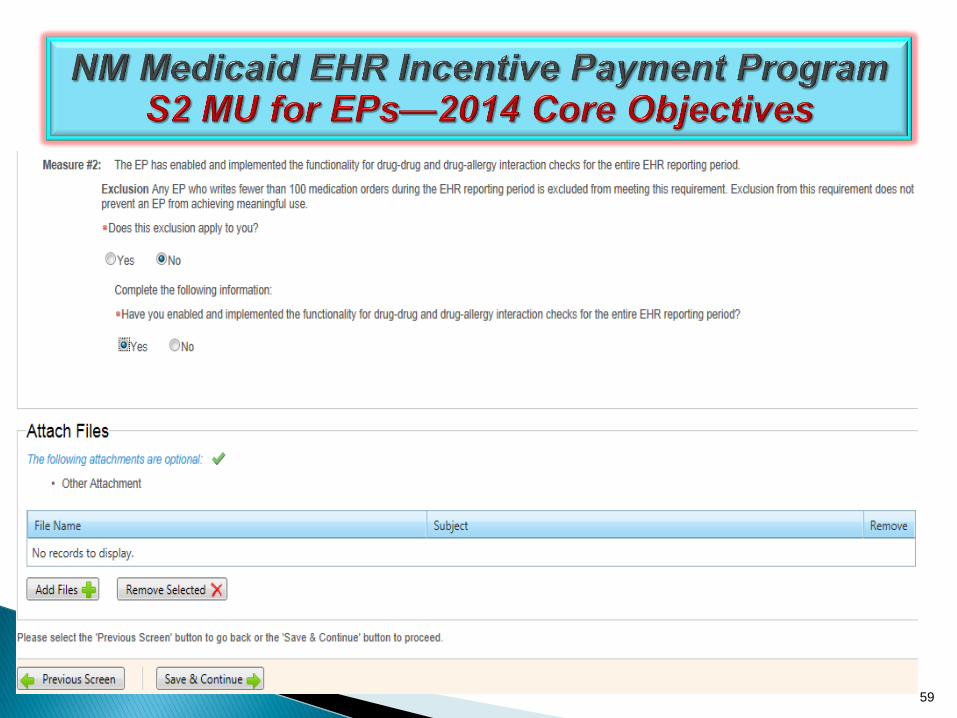
Measure 2: The EP has enabled and implemented the functionality for drug-drug and drug-allergy
interaction checks for the entire EHR reporting period.
Exclusion:
For the second measure, any EP who writes fewer than 100 medication orders during the EHR
reporting period.

62

63
64
Core Objective 7 – Clinical Lab-Test Results
Objective:
Incorporate clinical lab-test results into Certified EHR Technology
(CEHRT) as structured data
Measure:
More than 55 percent of all clinical lab tests results ordered by the EP
during the EHR reporting period whose results are either in a
positive/negative or numerical format are incorporated in Certified EHR
Technology as structured data
Exclusion:
Any EP who orders no lab tests where results are either in a
positive/negative affirmation or numeric format during the EHR
reporting period.

65
Core Objective 7 – Clinical Lab-Test Results Additional Information:
The structured data for the numeric/quantitative test results may include positive or negative affirmations
and/or numerical format that would include a reference range of numeric results and/or ratios.
Structured data does not need to be electronically exchanged in order to qualify for the measure of this
objective. The EP is not limited to only counting structured data received via electronic exchange, but may
count in the numerator all structured data entered through manual entry through typing, option selecting,
scanning, or other means.
Lab results are not limited to any specific type of laboratory or to any specific type of lab test.
The Medicare and Medicaid EHR Incentive Programs do not specify the use of code set standards in
meeting the measure for this objective. However, the Office of the National Coordinator for Health
Information Technology (ONC) has adopted Logical Observation Identifiers Names and Codes (LOINC®)
version 2.27, when such codes were received within an electronic transaction from a laboratory, for the
entry of structured data for this measure and made this a requirement for EHR technology to be certified.
Provided the lab result is recorded as structured data and uses the standards above, there does not need
to be an explicit linking between the lab result and the order placed by the physician in order to be
counted in the numerator.
In order to meet this objective and measure, an EP must use the capabilities and standards of CEHRT at
45 CFR 170.314(b)(5).

66
NOTE: You must attest YES to meet the
attestation requirements

67
Core Objective 8 – Patient Lists
Definitions:
Specific Conditions – Those conditions listed in the active patient problem
list.
Objective:
Generate lists of patients by specific conditions to use for quality
improvement, reduction of disparities, research, or outreach.
Measure:
Generate at least one report listing patients of the EP with a specific
condition.
Exclusion:
No exclusion.
Attestation Requirements:
Eligible professionals (EPs) must attest YES to having generated at least one
report listing patients of the EP with a specific condition to meet this measure.

68
69
70
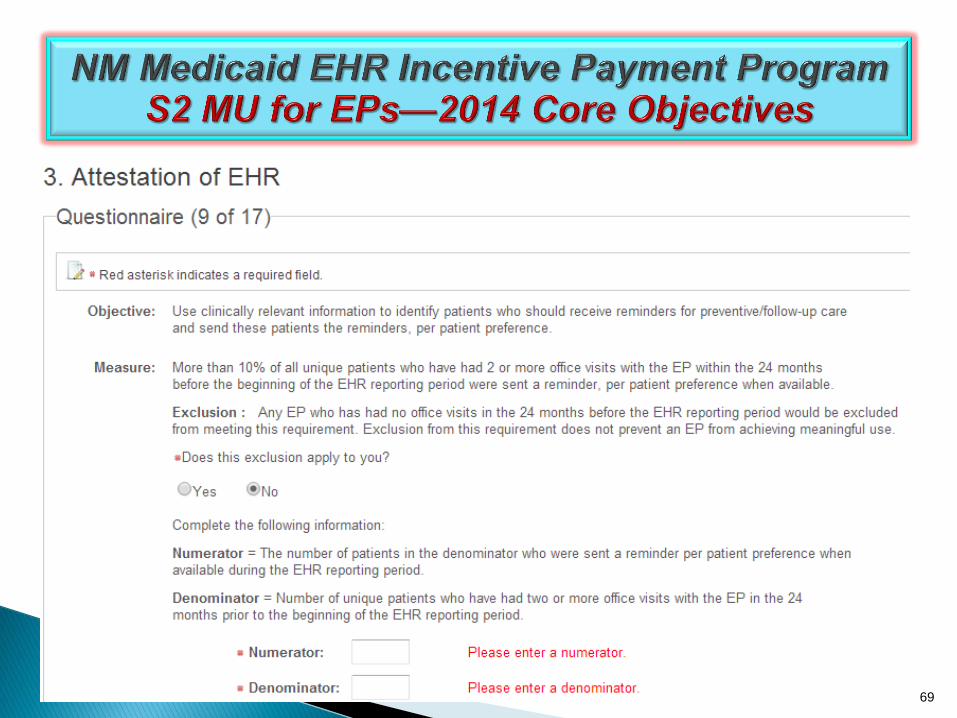
Core Objective 9 – Preventive Care
Definitions:
Patient Preference – The method of communication that patients prefer to
receive their reminders such as (but not limited to) by mail, by phone or by
secure messaging.
Active Patients – Patients with at least two office visits in the last 24 months.
Objective:
Use clinically relevant information to identify patients who should receive
reminders for preventive/follow-up care and send these patients the
reminders, per patient preference.
Measure:
More than 10 percent of all unique patients who have had 2 or more office
visits with the EP within the 24 months before the beginning of the EHR
reporting period were sent a reminder, per patient preference when available.
Exclusion:
Any EP who has had no office visits in the 24 months before the EHR
reporting period.

71

72

73
OR

74
Core Objective 10 – Patient Electronic Access Definitions:
Access – When a patient possesses all of the necessary information needed to view,
download, or transmit their information. This could include providing patients with instructions
on how to access their health information, the website address they must visit for online
access, a unique and registered username or password, instructions on how to create a
login, or any other instructions, tools, or materials that patients need in order to view,
download, or transmit their information.
View – The patient (or authorized representative) accessing their health information online.
Transmission – Any means of electronic transmission according to any transport
standard(s) (SMTP, FTP, REST, SOAP, etc.). However, the relocation of physical electronic
media (for example, USB, CD) does not qualify as transmission although the movement of
the information from online to the physical electronic media will be a download.
Business Days – Business days are defined as Monday through Friday excluding federal or
state holidays on which the EP or their respective administrative staffs are unavailable.
Diagnostic Test Results – All data needed to diagnose and treat disease. Examples
include, but are not limited to, blood tests, microbiology, urinalysis, pathology tests, radiology,
cardiac imaging, nuclear medicine tests, and pulmonary function tests.

75
Core Objective 10 – Patient Electronic Access Objective:
Provide patients the ability to view online, download and transmit their health information within four
business days of the information being available to the EP.
Measure:
Measure 1: More than 50 percent of all unique patients seen by the EP during the EHR reporting period
are provided timely (available to the patient within 4 business days after the information is available to the
EP) online access to their health information, with the ability to view, download, and transmit to a third
party.
Measure 2: More than 5 percent of all unique patients seen by the EP during the EHR reporting period
(or their authorized representatives) view, download, or transmit to a third party their health information.
Exclusion:
Any EP who:
(1) Neither orders nor creates any of the information listed for inclusion as part of both measures,
except for "Patient name" and "Provider's name and office contact information,” may exclude both
measures.
(2) Conducts 50 percent or more of his or her patient encounters in a county that does not have 50
percent or more of its housing units with 3Mbps broadband availability according to the latest
information available from the FCC on the first day of the EHR reporting period may exclude only the
second measure.
76
Core Objective 10 – Patient Electronic Access Additional Information:
The following information must be made available online: Patient name, provider's name and office
contact information, current and past problem list, procedures. laboratory test results, current
medication list and medication history, current medication allergy list and medication allergy
history, vital signs (height, weight, blood pressure, BMI, growth charts), smoking status,
demographic information (preferred language, sex, race, ethnicity, date of birth), care plan field(s),
including goals and instructions, and any known care team members including the primary care
provider (PCP) of record unless the information is not available in certified EHR technology
(CEHRT), is restricted from disclosure due to any federal, state or local law regarding the privacy
of a person’s health information, including variations due to the age of the patient or the provider
believes that substantial harm may arise from disclosing particular health information in this
manner.
Replaces the Stage 1 core objective for EPs of "Provide patients with an electronic copy of their
health information (including diagnostic test results, problem list, medication lists, medication
allergies) upon request" and the Stage 1 menu objective for EPs of "Provide patients with timely
electronic access to their health information (including lab results, problem list, medication lists,
and allergies) within 4 business days of the information being available to the EP."
Both of the measures for this objective must be met using CEHRT.

77

78

79
Core Objective 11 – Clinical Summaries Definitions:
Clinical Summary – An after-visit summary that provides a patient with relevant and actionable
information and instructions containing in no particular order:
• Patient name. • Provider's name and office contact information.
• Date and location of the visit. • Reason for the office visit.
• Current problem list. • Current medication list.
• Current medication allergy list. • Procedures performed during the visit.
• Laboratory test results. • List of diagnostic tests pending.
• Clinical instructions. • Future appointments.
• Referrals to other providers. • Future scheduled tests.
• Smoking status. • Care plan field(s), including goals and instructions.
• Recommended patient decision aids (if applicable to the visit).
• Demographic information maintained within certified electronic health record technology (CEHRT)
(sex, race, ethnicity, date of birth, preferred language).
• Immunizations or medications administered during the visit.
•Vital signs taken during the visit (or other recent vital signs).

80
Core Objective 11 – Clinical Summaries
Definitions Continued:
Office Visit – Office visits include separate, billable encounters that result from evaluation and
management services provided to the patient and include:
(1) Concurrent care or transfer of care visits,
(2) Consultant visits, or
(3) Prolonged Physician Service without Direct (Face-To-Face) Patient Contact (tele-health). A
consultant visit occurs when a provider is asked to render an expert opinion/service for a specific
condition or problem by a referring provider.
Objective:
Provide clinical summaries for patients for each office visit.
Measure:
Clinical summaries provided to patients or patient-authorized representatives within one business day for
more than 50 percent of office visits.
Exclusion:
Any EP who has no office visits during the EHR reporting period.

81
Core Objective 11 – Clinical Summaries
Additional Information:
The provision of the clinical summary is limited to the information contained within CEHRT.
The clinical summary can be provided through a PHR, patient portal on the web site, secure e-mail,
electronic media such as CD or USB fob, or printed copy. If the EP chooses an electronic media, they
would be required to provide the patient a paper copy upon request. They may also default to providing
paper copies, in which case an electronic form of the EP’s choice would need to be provided upon
request.
Providers may not charge patients a fee to provide this information.
When a patient visit lasts several days or a patient is seen by multiple EPs, a single clinical summary at
the end of the visit should be counted only once in both the numerator and denominator.
In the event that a clinical summary is offered to and subsequently declined by the patient, that patient
may still be included in the numerator of the measure.
In circumstances where there is no information available to populate one or more of the fields
previously listed, either because the EP can be excluded from recording such information (for example,
vital signs) or because there is no information to record (for example, no medication allergies or
laboratory tests), an indication that the information is not available in the clinical summary would meet
the measure of this objective.
82

83

Core Objective 12 – Patient-Specific Education Resources Definitions:
Patient-Specific Education Resources identified by Certified EHR Technology – Resources
or a topic area of resources identified through logic built into certified EHR technology which
evaluates information about the patient and suggests education resources that would be of
value to the patient.
Unique Patient – If a patient is seen by an EP more than once during the EHR reporting period,
then for purposes of measurement that patient is only counted once in the denominator for the
measure. All the measures relying on the term ‘‘unique patient’’ relate to what is contained in the
patient’s medical record. Not all of this information will need to be updated or even be needed by
the provider at every patient encounter. This is especially true for patients whose encounter
frequency is such that they would see the same provider multiple times in the same EHR
reporting period.
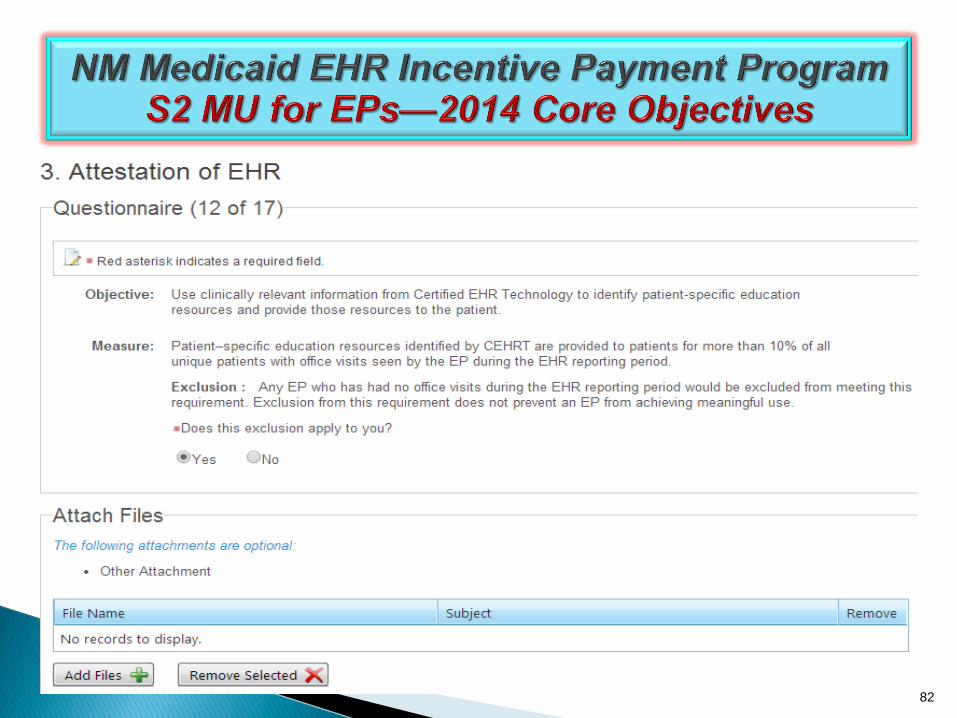
Objective:
Use clinically relevant information from Certified EHR Technology to identify patient-specific
education resources and provide those resources to the patient.
Measure:
Patient-specific education resources identified by Certified EHR Technology are provided to
patients for more than 10 percent of all unique patients with office visits seen by the EP during
the EHR reporting period.
Exclusion:
Any EP who has no office visits during the EHR reporting period.
84
Core Objective 12 – Patient-Specific Education Resources Additional Information:
Unique patients with office visits means that to count in the denominator a patient must be seen by the EP for
one or more office visits during the EHR reporting period, but if a patient seen by the EP more than once
during the EHR reporting period, the patient only counts once in the denominator.
Education resources or materials do not have to be stored within or generated by the certified EHR. However,
the provider should utilize certified EHR technology (CEHRT) in a manner where the technology suggests
patient-specific educational resources based on the information stored in the CEHRT. The provider can make
a final decision on whether the education resource is useful and relevant to a specific patient.
While CEHRT must be used to identify patient-specific education resources, these resources or materials do
not have to be stored within or generated by the CEHRT.
Certified EHR technology is certified to use the patient's problem list, medication list, or laboratory test results
to identify the patient-specific educational resources.
The EP may use these elements or additional elements within CEHRT to identify educational resources
specific to patients' needs. The EP can then provide these educational resources to patients in a useful format
for the patient (such as, electronic copy, printed copy, electronic link to source materials, through a patient
portal or PHR).
If resources or topic area of resources are not identified by CEHRT and provided to the patient then it will not
count in the numerator.
The education resources will need to be provided prior to the calculation and subsequent attestation to
meaningful use.
85

86

87

88
Core Objective 13 – Use Secure Electronic Messaging
Definitions:
Secure Message – Any electronic communication between a provider and patient that ensures
only those parties can access the communication. This electronic message could be email or the
electronic messaging function of a PHR, an online patient portal, or any other electronic means.
Objective:
Use secure electronic messaging to communicate with patients on relevant health information.
Measure:
A secure message was sent using the electronic messaging function of CEHRT by more than 5
percent of unique patients (or their authorized representatives) seen by the EP during the EHR
reporting period.
Exclusion:
Any EP who has no office visits during the EHR reporting period, or any EP who conducts 50
percent or more of his or her patient encounters in a county that does not have 50 percent or more
of its housing units with 3Mbps broadband availability according to the latest information available
from the FCC on the first day of the EHR reporting period.

89
Core Objective 13 – Use Secure Electronic Messaging
Attestation Requirements:
DENOMINATOR: Number of unique patients seen by the EP during the EHR
reporting period.
NUMERATOR: The number of patients or patient-authorized representatives in
the denominator who send a secure electronic message to the EP that is
received using the electronic messaging function of CEHRT during the EHR
reporting period.
THRESHOLD: The resulting percentage must be more than 5 percent in order for
an EP to meet this measure.
EXCLUSION: Any EP who has no office visits during the EHR reporting period, or
any EP who conducts 50 percent or more of his or her patient encounters in a
county that does not have 50 percent or more of its housing units with 3Mbps
broadband availability according to the latest information available from the FCC
on the first day of the EHR reporting period.
Additional Information:
There is not an expectation that the EP must personally respond to electronic
messages to the patient.

90
91

92
Core Objective 14 – Medication Reconciliation
Definitions:
Medication Reconciliation – The process of identifying the most accurate list of all medications that the
patient is taking, including name, dosage, frequency, and route, by comparing the medical record to an
external list of medications obtained from a patient, hospital, or other provider.
Relevant Encounter – An encounter during which the EP performs a medication reconciliation due to
new medication or long gaps in time between patient encounters or for other reasons determined
appropriate by the EP. Essentially an encounter is relevant if the EP judges it to be so. (Note: Relevant
encounters are not included in the numerator and denominator of the measure for this objective.)
Transition of Care – The movement of a patient from one clinical setting (inpatient, outpatient, physician
office, home health, rehab, long-term care facility, etc.) to another or from one EP to another. At a
minimum, transitions of care include first encounters with a new patient and encounters with existing
patients where a summary of care record (of any type) is provided to the receiving provider. The summary
of care record can be provided either by the patient or by the referring/transiting provider or institution.
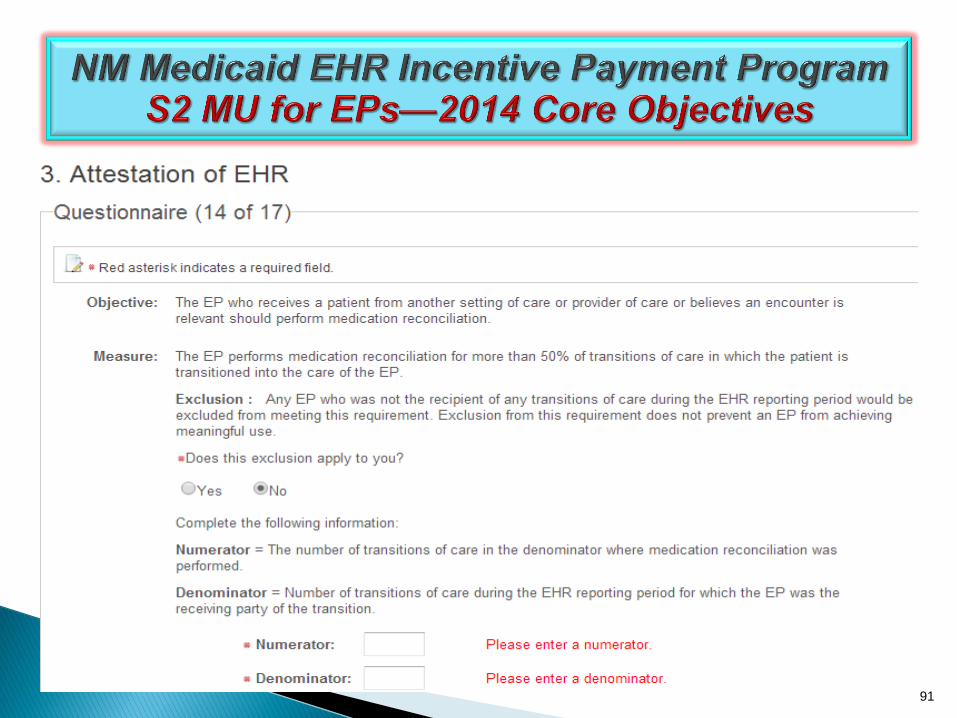
Objective: The EP who receives a patient from another setting of care or provider of care or believes an
encounter is relevant should perform medication reconciliation.
Measure: The EP who performs medication reconciliation for more than 50 percent of transitions of care in
which the patient is transitioned into the care of the EP.
Exclusion: Any EP who was not the recipient of any transitions of care during the EHR reporting period.

93
Core Objective 14 – Medication Reconciliation
Additional Information:
Only patients whose records are maintained using certified
EHR technology must be included in the denominator for
transitions of care.
In the case of reconciliation following transition of care, the
receiving EP should conduct the medication reconciliation.
The electronic exchange of information is not a requirement for
medication reconciliation.
The measure of this objective does not dictate what information
must be included in medication reconciliation. Information
included in the process of medication reconciliation is
appropriately determined by the provider and patient.
94

95

96
97
98
http://www.cms.gov/Regulations-and-Guidance/Legislation/EHRIncentivePrograms/Stage_2.html

99
Core Objective 15 – Summary of Care
Definitions:
Transition of Care – The movement of a patient from one setting of care (hospital, ambulatory primary care
practice, ambulatory, specialty care practice, long-term care, home health, rehabilitation facility) to another.
At a minimum this includes all transitions of care and referrals that are ordered by the EP.
Summary of Care Record – A summary of care record must include the following elements:
•Patient name •Smoking status • Reason for referral
• Procedures •Encounter diagnosis • Current medication list
• Immunizations •Laboratory test results • Current medication allergy list
• Vital signs (height, weight, blood pressure, BMI).
• Functional status, including activities of daily living, cognitive and disability status
• Demographic information (preferred language, sex, race, ethnicity, date of birth).
• Care plan field, including goals and instructions.
• Care team including the primary care provider of record and any additional known
care team members beyond the referring or transitioning provider and the receiving provider.
• Referring or transitioning provider's name and office contact information (EP only).
• Current problem list (EPs may also include historical problems at their discretion).

100
Core Objective 15 – Summary of Care
Definitions Continued:
Problem List – At a minimum a list of current, active and historical diagnoses. We
do not limit the EP to just including diagnoses on the problem list.
Active/current medication list – A list of medications that a given patient is
currently taking.
Active/current medication allergy list – A list of medications to which a given
patient has known allergies.
Allergy – An exaggerated immune response or reaction to substances that are
generally not harmful.
Care Plan – The structure used to define the management actions for the various
conditions, problems, or issues. A care plan must include at a minimum the
following components: problem (the focus of the care plan), goal (the target
outcome) and any instructions that the provider has given to the patient. A goal is
a defined target or measure to be achieved in the process of patient care (an
expected outcome).

101
Core Objective 15 – Summary of Care
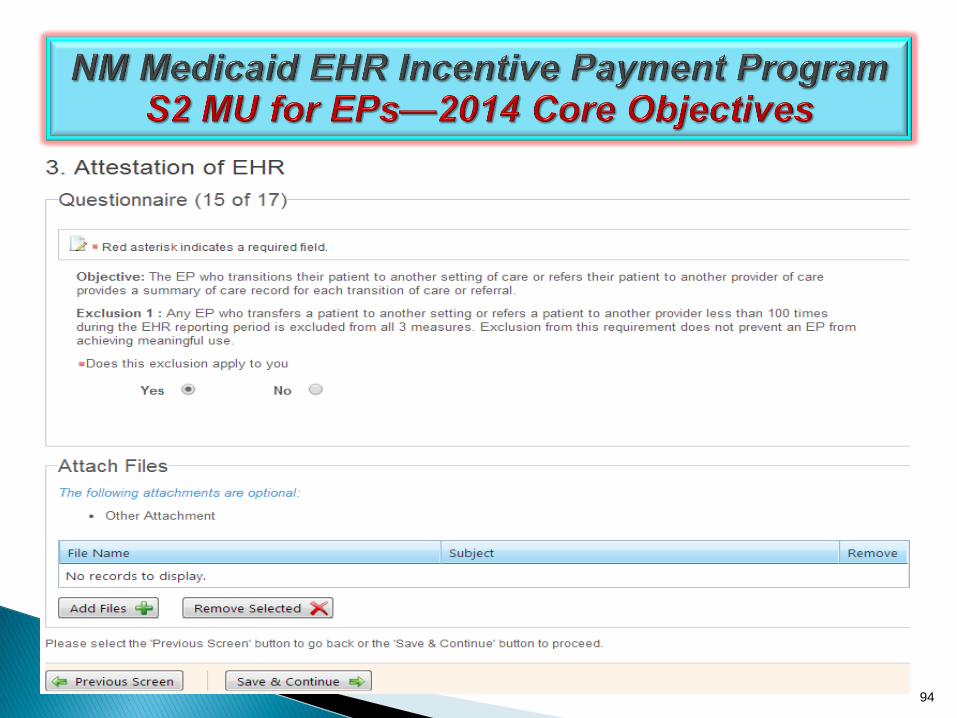
Objective: The EP who transitions their patient to another setting of care or provider of care or refers their patient to
another provider of care should provide summary care record for each transition of care or referral.
Measure:
EPs must satisfy both of the following measures in order to meet the objective:
Measure 1: The EP who transitions or refers their patient to another setting of care or provider of care provides
a summary of care record for more than 50 percent of transitions of care and referrals.
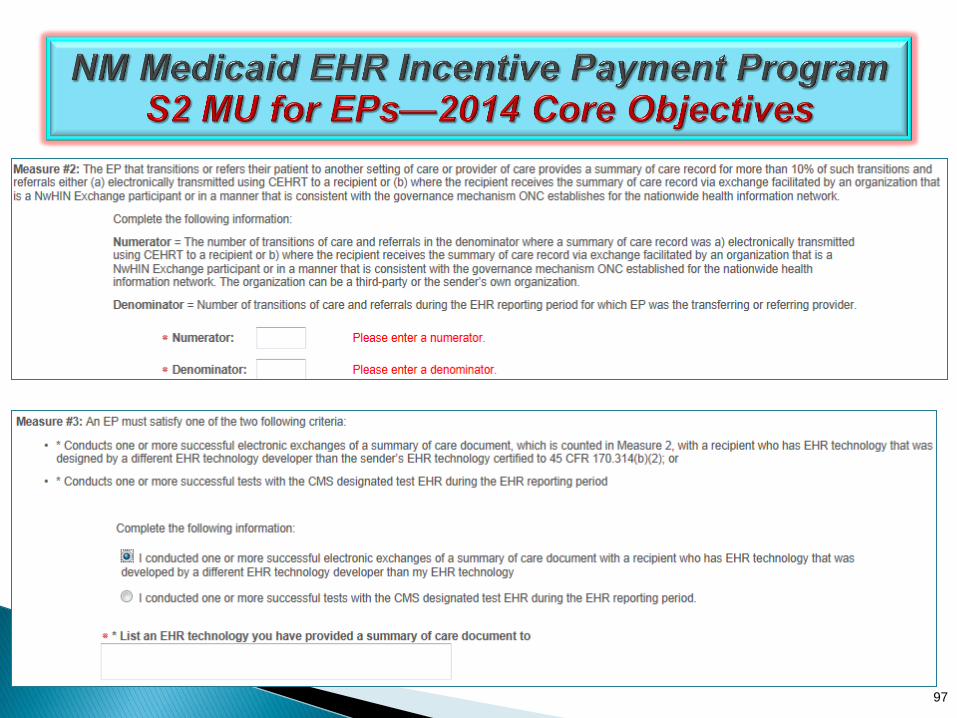
Measure 2: The EP who transitions or refers their patient to another setting of care or provider of care provides
a summary of care record for more than 10 percent of such transitions and referrals either (a) electronically
transmitted using CEHRT to a recipient or (b) where the recipient receives the summary of care record via
exchange facilitated by an organization that is a NwHIN Exchange participant or in a manner that is consistent
with the governance mechanism ONC establishes for the NwHIN.
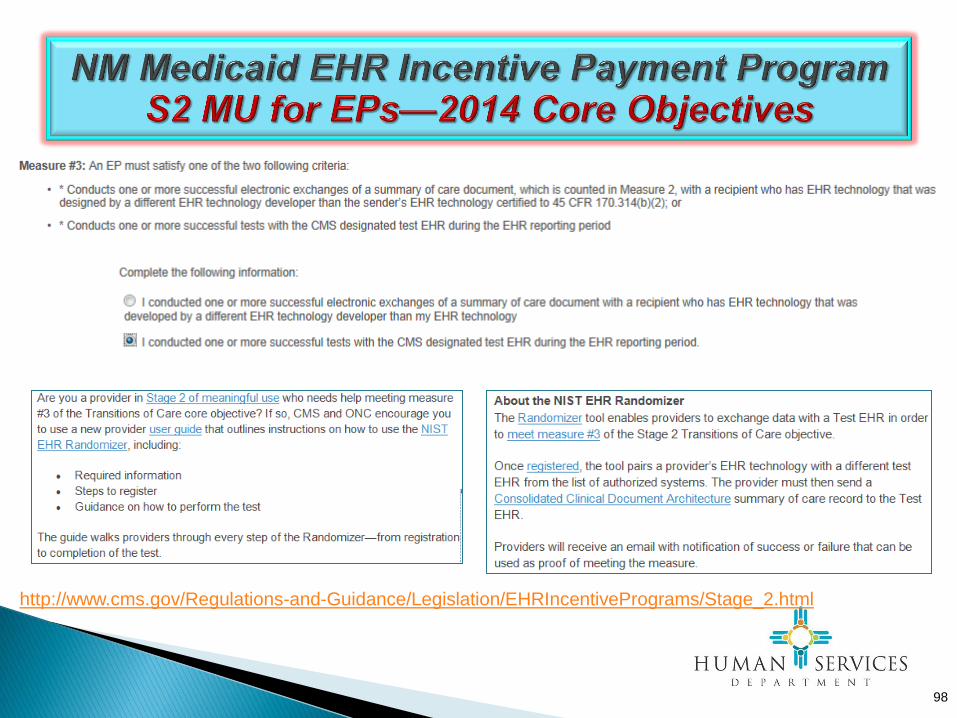
Measure 3: An EP must satisfy one of the following criteria:
Conducts one or more successful electronic exchanges of a summary of care document, as part of which is
counted in "measure 2" (for EPs the measure at §495.6(j)(14)(ii)(B) with a recipient who has EHR
technology that was developed designed by a different EHR technology developer than the sender's EHR
technology certified to 45 CFR 170.314(b)(2).
Conducts one or more successful tests with the CMS designated test EHR during the EHR reporting period.
Exclusion: Any EP who transfers a patient to another setting or refers a patient to another provider less than 100
times during the EHR reporting period is excluded from all three measures.
102
Core Objective 15 – Summary of Care
Additional Information:
Only patients whose records are maintained using certified EHR technology must be included in
the denominator for transitions of care.
The EP that transfers or refers the patient to another setting of care or provider should provide
the summary of care document. It is for this provider that has the most recent information on the
patient that may be crucial to the provider to whom the patient is transferred or referred.
The EP can send an electronic or paper copy of the summary care record directly to the next
provider or can provide it to the patient to deliver to the next provider, if the patient can
reasonably expected to do so and meet Measure 1.
If the provider to whom the referral is made or to whom the patient is transitioned to has access
to the medical record maintained by the referring provider then the summary of care record
would not need to be provided, and that patient must not be included in the denominator for
transitions of care.
To count in the numerator of any measure, the EP must verify these three fields for current
problem list, current medication list, and current medication allergy list are not blank and include
the most recent information known by the EP or hospital as of the time of generating the
summary of care document.
To count in the numerator of measure 2, the summary of care record must be received by the
provider to whom the sending provider is referring or transferring the patient.

103
Core Objective 15 – Summary of Care
Additional Information:
To count in the numerator of measure 2, one of the following three transmission approaches must be used:
• Use of the transport standard capability required for certification. As required by ONC to meet the CEHRT
definition, every EP, eligible hospital, and CAH, must have EHR technology that is capable of electronically
transmitting a summary care record for transitions of care and referrals according to the primary Direct Project
specification (the Applicability Statement for Secure Health Transport). Thus, EPs, eligible hospitals, or CAHs
that electronically transmit summary care records using their CEHRT’s “Direct” capability (natively or combined
with an intermediary) would be able to count all such electronic transmissions in their numerator.
• Use of the SOAP-based optional transport standard capability permitted for certification. As part of certification,
ONC permits EHR technology developers to voluntarily seek certification for their EHR technology’s capability
to perform SOAP-based electronic transmissions. EHR technology developers who take this approach would
enable their customers to also use this approach to meet the measure. Thus, EPs, eligible hospitals, or CAHs
that electronically transmit summary care records using their CEHRT’s “SOAP-based” capability (natively or
combined with an intermediary) would be able to count all of those transmissions in their numerator.
• Use of CEHRT to create a summary care record in accordance with the required standard (i.e., Consolidated
CDA as specified in 45 CFR 170.314(b)(2)), and the electronic transmission is accomplished through the use of
an eHealth Exchange participant who enables the electronic transmission of the summary care record to its
intended recipient. Thus, EPs, eligible hospitals, or CAHs who create standardized summary care records using
their CEHRT and then use an eHealth Exchange participant to electronically transmit the summary care record
would be able to count all of those transmissions in their numerator.
104
Core Objective 15 – Summary of Care
CMS 2014 Flexibility Rule—Limited Exception:
The Flexibility Rule allows providers who cannot meet the Stage 2 Summary of Care
measures to attest to Stage 1 Meaningful Use using the 2014 Edition criteria if the following
applies.
• Provider cannot meet the Stage 2 Summary of Care Measures due to the recipient
Summary of Care transmittal being impacted by a 2014 CEHRT issue. The sending
provider may experience significant difficulty meeting the 10% threshold for electronic
transmissions, despite the referring provider’s ability to send the electronic document if
the intermediary or recipient of the transmission or referral is experiencing delays in the
ability to fully implement 2014 Edition CEHRT.
• The Referring Provider under this circumstance may attest to the 2014 Stage 1
Objectives and Measures for the EHR Reporting Period in 2014.
• The Referring Provider must retain documentation demonstrating that s/he was unable
to meet the 10% threshold to Provide and Electronic Summary of Care document for a
Transition or Referral because the Intermediary or Recipient of the Transmission or Referral is experiencing delays in the ability to Fully Implement 2014 Edition CEHRT.

105
https://www.nmhit.org/Registration/
106

107
On-Boarding Status
Attach NM DOH
https://www.nmhit.org/
screenshot OR DOH email
dated within 60 days of the
start of EHR Reporting
Period

108

109
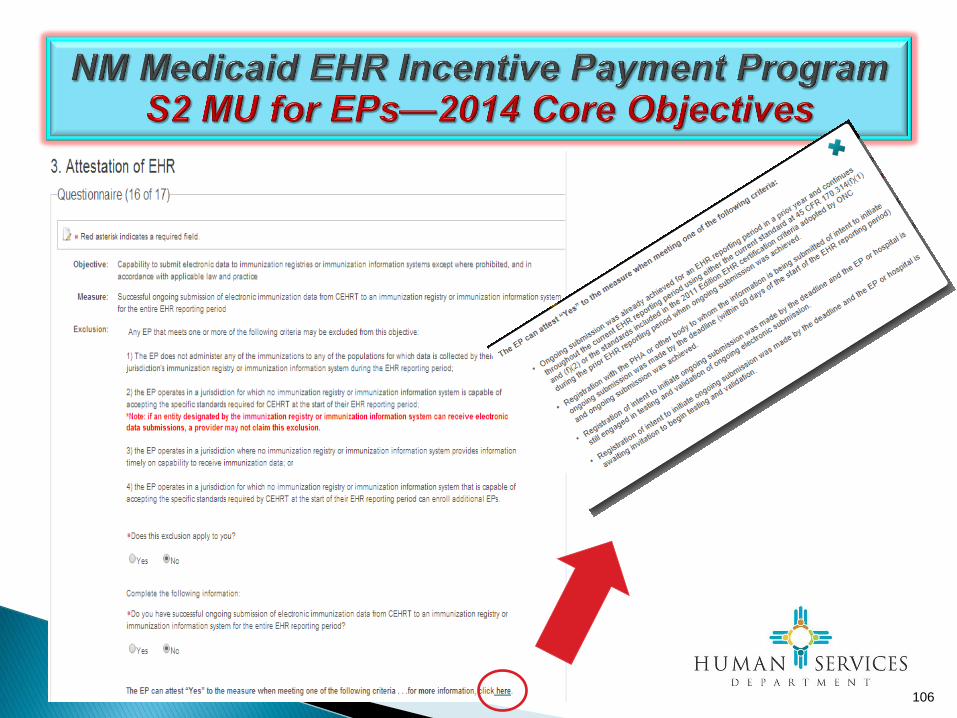
Core Objective 16 – Immunization Registries Data Submission
Objective: Capability to submit electronic data to immunization registries or immunization information
systems except where prohibited, and in accordance with applicable law and practice.
Measure: Successful ongoing submission of electronic immunization data from CEHRT to an
immunization registry or immunization information system for the entire EHR reporting period.
Exclusions:
Any EP that meets one or more of the following criteria may be excluded from this objective:
(1) the EP does not administer any of the immunizations to any of the populations for which data
is collected by their jurisdiction's immunization registry or immunization information system
during the EHR reporting period;
(2) the EP operates in a jurisdiction for which no immunization registry or immunization
information system is capable of accepting the specific standards required for CEHRT at the
start of their EHR reporting period;
(3) the EP operates in a jurisdiction where no immunization registry or immunization information
system provides information timely on capability to receive immunization data; or
(4) the EP operates in a jurisdiction for which no immunization registry or immunization
information system that is capable of accepting the specific standards required by CEHRT at the
start of their EHR reporting period can enroll additional EPs.
110
Core Objective 16 – Immunization Registries Data Submission
Additional Information: The second exclusion does not apply if an entity designated
by the immunization registry or immunization information system can receive electronic
immunization data submissions. For example, if the immunization registry cannot
accept the data directly or in the standards required by CEHRT, but if it has designated
a Health Information Exchange to do so on their behalf and the Health Information
Exchange is capable of accepting the information in the standards required by CEHRT,
the provider could not claim the second exclusion.
In order to meet this objective and measure, an EP must use the capabilities and
standards of CEHRT at 45 CFR 170.314(f)(1) and (f)(2). However, if EPs prior to CY
2014 have achieved successful ongoing submission using EHR technology certified to
the 2011 Edition EHR certification criteria (HL7 2.3.1 only), it is acceptable to continue
this ongoing submission and meet the Stage 2 measure for as long as HL7 2.3.1
continues to be accepted by the immunizations information system or immunization
registry.
111
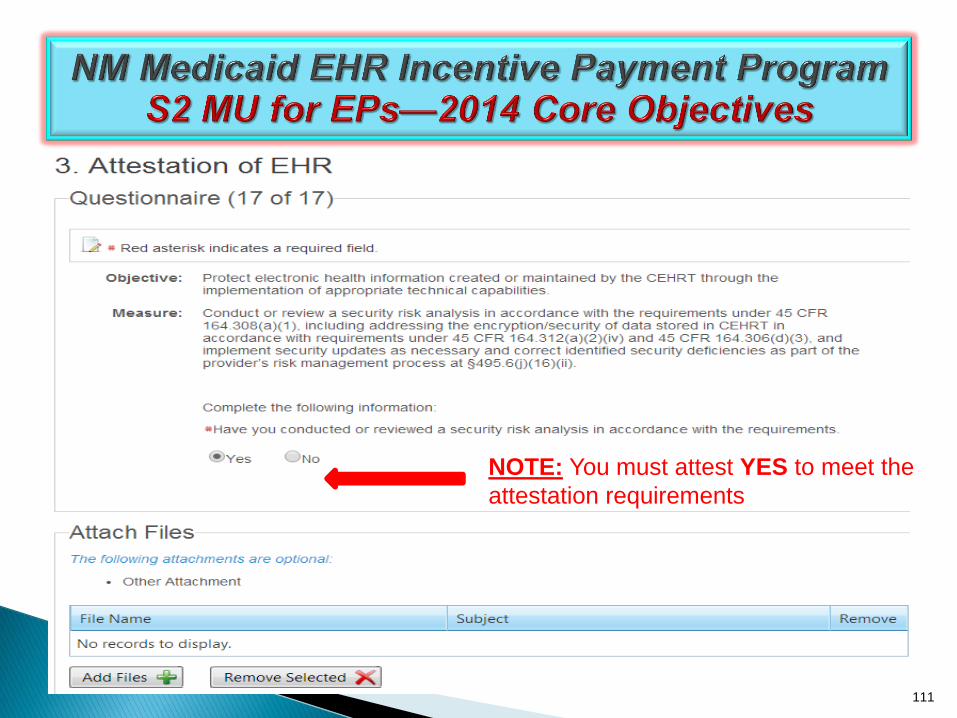
NOTE: You must attest YES to meet the
attestation requirements
112
Core Objective 17 – Protect Electronic Health Information
Objective:
Protect electronic health information created or maintained by the certified
EHR technology (CEHRT) through the implementation of appropriate
technical capabilities.
Measure:
Conduct or review a security risk analysis in accordance with the
requirements under 45 CFR 164.308(a) (1), including addressing the
encryption/security of data stored in CEHRT in accordance with
requirements under 45 CFR 164.312 (a)(2)(iv) and 45 CFR 164.306(d)(3),
and implement security updates as necessary and correct identified
security deficiencies as part of the provider's risk management process for
EPs.
Exclusion:
No exclusion.

113
Core Objective 17 – Protect Electronic Health Information
Additional Information:
EPs must conduct or review a security risk analysis of CEHRT including addressing
encryption/security of data, and implement updates as necessary at least once prior
to the end of the EHR reporting period and attest to that conduct or review. The
testing could occur prior to the beginning of the first EHR reporting period. However,
a new review would have to occur for each subsequent reporting period.
The parameters of the security risk analysis are defined 45 CFR 164.308(a)(1) which
was created by the HIPAA Security Rule. Meaningful use does not impose new or
expanded requirements on the HIPAA Security Rule nor does it require specific use
of every certification and standard that is included in certification of EHR technology.
More information on the HIPAA Security Rule can be found at
http://www.hhs.gov/ocr/privacy/hipaa/administrative/securityrule/
114
Core Objective 17 – Protect Electronic Health Information
Additional Information:
An EP who is reporting for a 90-day EHR Reporting Period in 2014 may complete the
security risk analysis requirements outside of the this 90-day period as long as it is
completed between January 1st of the EHR reporting year and no later than the date
the eligible professional submits the attestation for that reporting period. If the EP
attests in the grace period, the security analysis must be performed by December 31,
2014.
For more information, read the updated FAQ 10754 at https://questions.cms.gov/

115
Core Objective 17 – Protect Electronic Health Information
Attestation—Attach Supporting Documentation
Providers should attach supporting documentation in the NM State Level
Registry at the time of Attestation, including any of the following:
Copy of the security risk analysis or subsequent review
Letter from provider/practice summarizing results of security risk analysis or
subsequent review; note any actions that were taken or will be taken to address
any security issues identified
Letter from contractor who performed the security risk analysis or subsequent
review—summarizing results; note any actions that were taken or will be taken to
address any security issues identified

New Mexico Human Services Department
Reporting Requirements
Eligible Professionals
Meaningful Use 20 Objectives
CORE 17 Objectives
MENU 3 of 6
Objectives
Clinical Quality
Measures 9 Objectives
9 CQMs total out of 64
9 adult
9 pediatric
Any 9
2014
116

117
NM Medicaid EHR Incentive Payment Program
S2 MU for EPs—2014 Menu Objectives
118

Don’t click here…ask Xerox
119

Don’t click here…ask Xerox
120

121
https://www.nmhit.org/Registration/
121
122

On-Boarding Status
Attach NM DOH
https://www.nmhit.org/
screenshot OR DOH
email dated within 60
days prior to start of
EHR Reporting Period
123

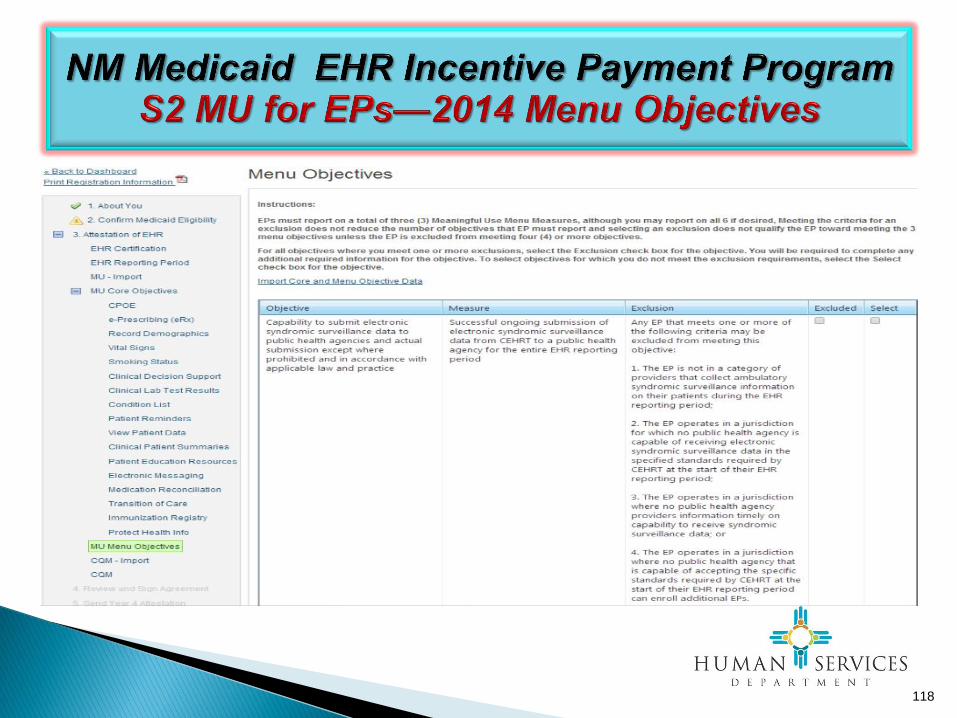
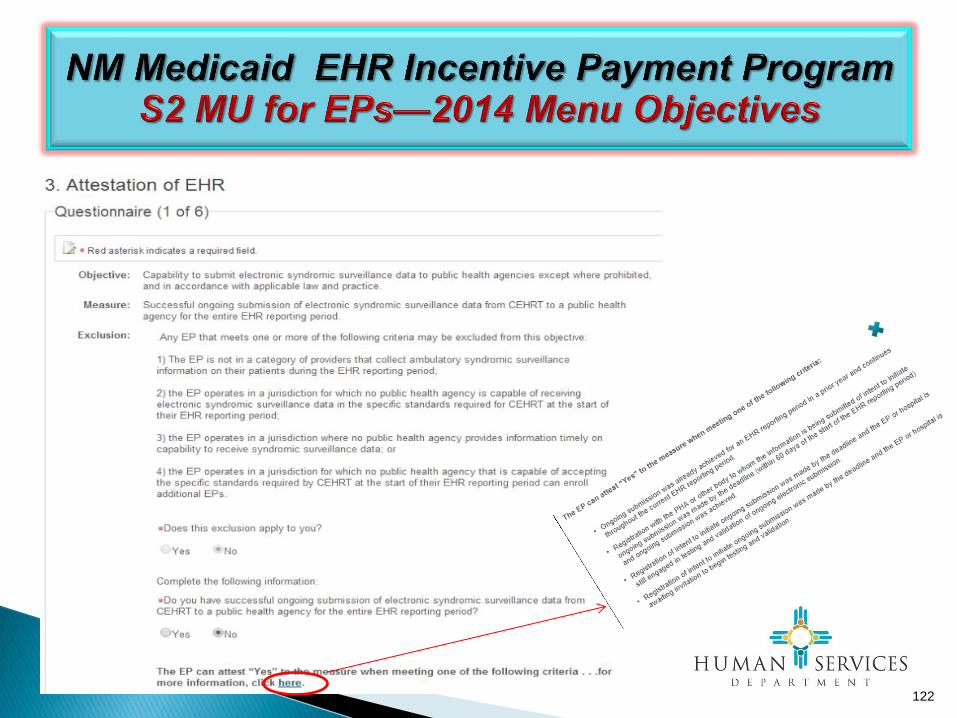
Menu Objective 1 – Syndromic Surveillance Data Submission Definition:
Public Health Agency – An entity under the jurisdiction of the U.S. Department of Health and
Human Services, tribal organization, State level and/or city/county level administration that
serves a public health function.
Objective: Capability to submit electronic syndromic surveillance data to public health agencies
except where prohibited, and in accordance with applicable law and practice.
Measure: Successful ongoing submission of electronic syndromic surveillance data from CEHRT
to a public health agency for the entire EHR reporting period.
Exclusion:
Any EP that meets one or more of the following criteria may be excluded from this objective:
(1) the EP is not in a category of providers that collect ambulatory syndromic surveillance
information on their patients during the EHR reporting period;
(2) the EP operates in a jurisdiction for which no public health agency is capable of receiving
electronic syndromic surveillance data in the specific standards required by CEHRT at the start
of their EHR reporting period;
(3) the EP operates in a jurisdiction where no public health agency provides information timely
on capability to receive syndromic surveillance data; or
(4) the EP operates in a jurisdiction for which no public health agency that is capable of
accepting the specific standards required by CEHRT at the start of their EHR
reporting period can enroll additional EPs.
124
125

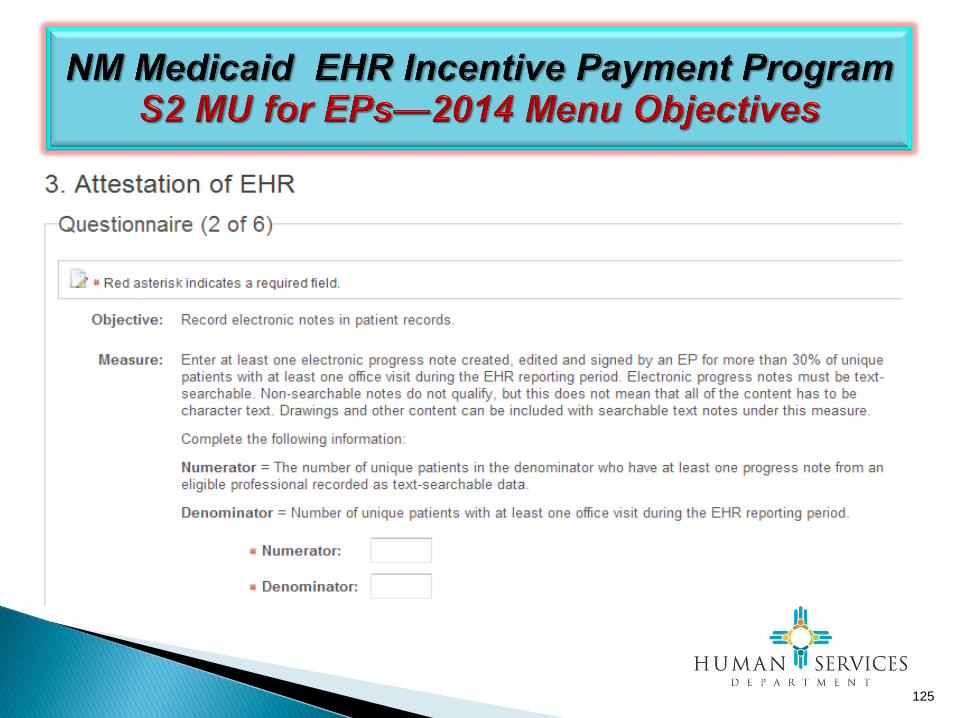
Menu Objective 2 – Electronic Notes
Definition:
Electronic Notes – Defined as electronic progress notes. CMS will rely on
providers own determinations and guidelines defining when progress notes are
necessary to communicate individual patient circumstances and for coordination
with previous documentation of patient observations, treatments and/or results in
the electronic health record.
Objective:
Record electronic notes in patient records.
Measure:.
Enter at least one electronic progress note created, edited and signed by an EP
for more than 30 percent of unique patients with at least one office visit during the
EHR reporting period. The text of the electronic note must be text searchable and
may contain drawings and other content
Exclusion:
Any EP who has no office visits during the EHR reporting period.
126

127

Menu Objective 3 – Imaging Results
Definition:
Imaging – The description of radiology services from the Stage 2 CPOE objective is the minimum
description of imaging. We describe radiologic services as any imaging service that uses electronic product
radiation. Electronic product radiation is defined at 21 CFR 1000.3 as: "any ionizing or nonionizing
electromagnetic or particulate radiation, or [a]ny sonic, infrasonic, or ultrasonic wave that is emitted from
an electronic product as the result of the operation of an electronic circuit in such product." If the provider
desires to include other types of imaging services that do not rely on electronic product radiation they may
do so as long as the policy is consistent across all patients and for the entire EHR reporting period.
Accessible through – Either incorporation of the image and accompanying information into CEHRT or an
indication in CEHRT that the image and accompanying information are available for a giving patient in
another technology and a link to that image and accompanying information.
Incorporation of the Image – The image and accompanying information is stored by the CEHRT.
A Link to the Image and Accompanying Information – A link to where the image and accompanying
information is stored is available in CEHRT. This link must conform to the certification requirements
associated with this objective in the ONC final rule published elsewhere in this issue of the Federal
Register.
No Access – None of the imaging providers used by the EP provide electronic images and any
explanation or other accompanying information that are accessible through their CEHRT at the start of the
EHR reporting period.
128

Menu Objective 3 – Imaging Results
Objective:
Imaging results consisting of the image itself and any explanation or other
accompanying information are accessible through CEHRT.
Measure:
More than 10 percent of all tests whose result is one or more images ordered
by the EP during the EHR reporting period are accessible through CEHRT.
Exclusion:
Any EP who orders less than 100 tests whose result is an image during the
EHR reporting period; or any EP who has no access to electronic imaging
results at the start of the EHR reporting period.
129

130

Menu Objective 4 – Family Health History
Definition:
First Degree Relative – A family member who shares about 50 percent of
their genes with a particular individual in a family. First degree relatives include
parents, offspring, and siblings.
Objective:
Record patient family health history as structured data.
Measure:.
More than 20 percent of all unique patients seen by the EP during the EHR
reporting period have a structured data entry for one or more first-degree
relatives.
Exclusion:
Any EP who has no office visits during the EHR reporting period.
131
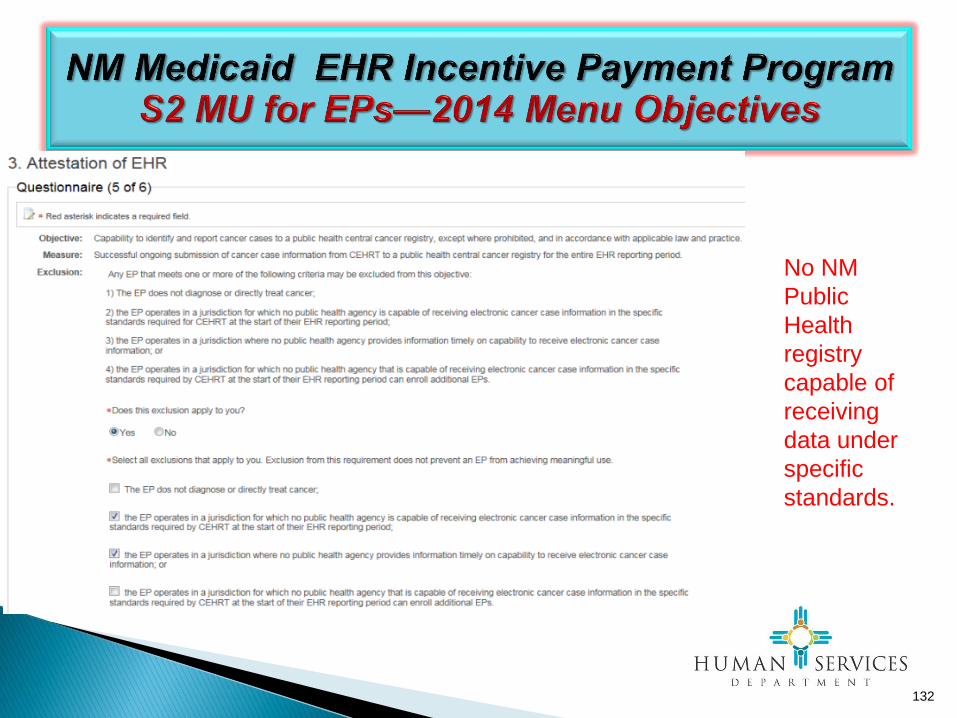
No NM
Public
Health
registry
capable of
receiving
data under
specific
standards.
132

133

Cont’d
134

Menu Objective 5—Report Cancer Cases
Objective: Capability to identify and report cancer cases to a public health central cancer
registry, except where prohibited, and in accordance with applicable law and practice.
Measure: Successful ongoing submission of cancer case information from CEHRT to a public
health central cancer registry for the entire EHR reporting period.
Exclusion:
Any EP that meets at least 1 of the following criteria may be excluded from this objective:
(1) The EP does not diagnose or directly treat cancer;
(2) The EP operates in a jurisdiction for which no public health agency is capable of
receiving electronic cancer case information in the specific standards required for
CEHRT at the beginning of their EHR reporting period;
(3) The EP operates in a jurisdiction where no PHA provides information timely on
capability to receive electronic cancer case information; or
(4) The EP operates in a jurisdiction for which no public health agency that is capable of
receiving electronic cancer case information in the specific standards required for
CEHRT at the beginning of their EHR reporting period can enroll additional EPs.
135

No NM
Public
Health
registry
capable of
receiving
data under
specific
standards.
136

137

Cont’d
138

Menu Objective 6—Specialized Registry
Objective: Capability to identify and report specific cases to a specialized registry (other than a
cancer registry), except where prohibited, and in accordance with applicable law and practice.
Measure: Successful ongoing submission of specific case information from CEHRT to a specialized
registry for the entire EHR reporting period.
EPs must attest YES to successfully submitting specific case information from CEHRT to a
specialized registry for the entire reporting period to meet this measure.
Ongoing submission was already achieved for an EHR reporting period in a prior year and
continues throughout the current EHR reporting period.
Registration with the PHA or other body to whom the information is being submitted of intent to
initiate ongoing submission was made by the deadline (within 60 days of the start of the EHR
reporting period) and ongoing submission was achieved.
Registration of intent to initiate ongoing submission was made by the deadline and the EP or
hospital is still engaged in testing and validation of ongoing electronic submission.
Registration of intent to initiate ongoing submission was made by the deadline and the EP or
hospital is awaiting invitation to begin testing and validation.
139
Menu Objective 6—Specialized Registry
Exclusions:
Any EP that meets at least 1 of the following criteria may be excluded from this objective:
(1) The EP does not diagnose or directly treat any disease associated with a specialized registry sponsored by a
national specialty society for which the EP is eligible, or the public health agencies in their jurisdiction;
(2) The EP operates in a jurisdiction for which no specialized registry sponsored by a public health agency or by a
national specialty society for which the EP is eligible is capable of receiving electronic specific case information in
the specific standards required by CEHRT at the beginning of their EHR reporting period;
(3) The EP operates in a jurisdiction where no public health agency or national specialty society for which the EP is
eligible provides information timely on capability to receive information into their specialized registries; or
(4) The EP operates in a jurisdiction for which no specialized registry sponsored by a public health agency or by a
national specialty society for which the EP is eligible that is capable of receiving electronic specific case information
in the specific standards required by CEHRT at the beginning of their EHR reporting period can enroll additional EPs.
140
Menu Objective 6—Specialized Registry
Definition of Terms
Specialized Registry – Sponsored by national specialty societies and specialized registries maintained by public health agencies.
Additional Information:
The specialized registry cannot be duplicative of any of the other registries included in other
meaningful use objectives and measures. This means that an EP cannot meet the immunization,
syndromic surveillance or cancer objectives and this objective by reporting to the same registry.
In determining whether an EP meets the first exclusion, the registries in question are those
sponsored by the public health agencies with jurisdiction over the area where the EP practices and
national medical societies covering the EP’s scope of practice.
Attestation: Attach Supporting Documentation:
If attesting to a specialized registry sponsored by a national specialty society, attach a letter from
the specialty society stating that the data was received by them, that the data was transmitted from
the provider’s/practice’s CEHRT, and on what date the transmission occurred.
141

142
Reporting Requirements
Eligible Professionals
Meaningful Use 20 Objectives
CORE 17 Objectives
MENU 3 of 6
Objectives
Clinical Quality
Measures 9 Objectives
9 CQMs total out of 64
9 adult
9 pediatric
Any 9
2014 — Stage 2

143
NM Medicaid EHR Incentive Payment Program
S2 MU for EPs—2014 CQMs
144
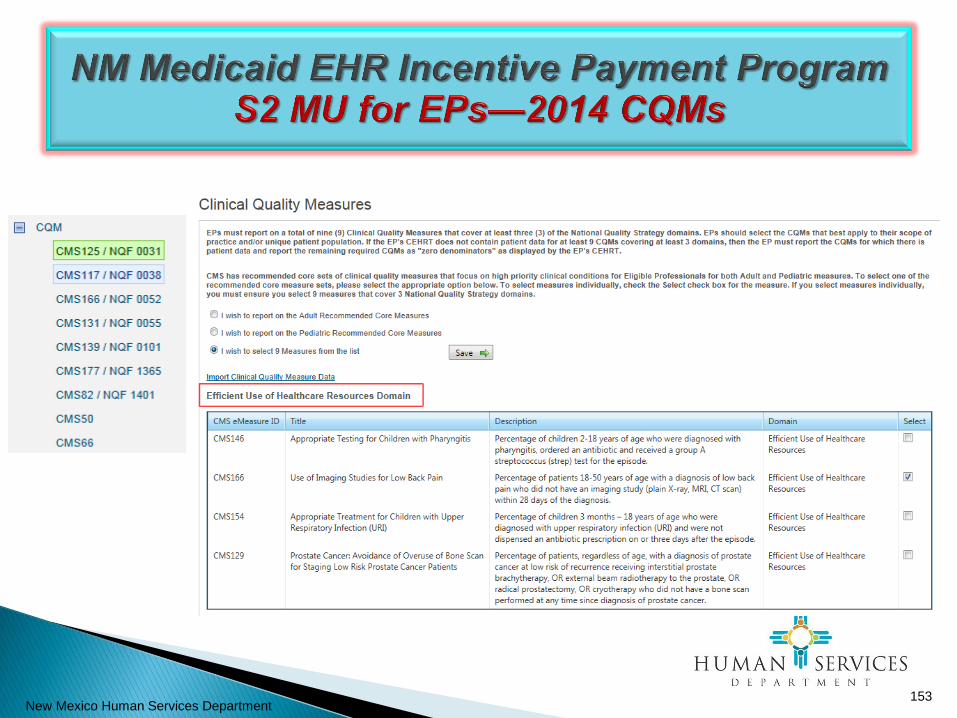
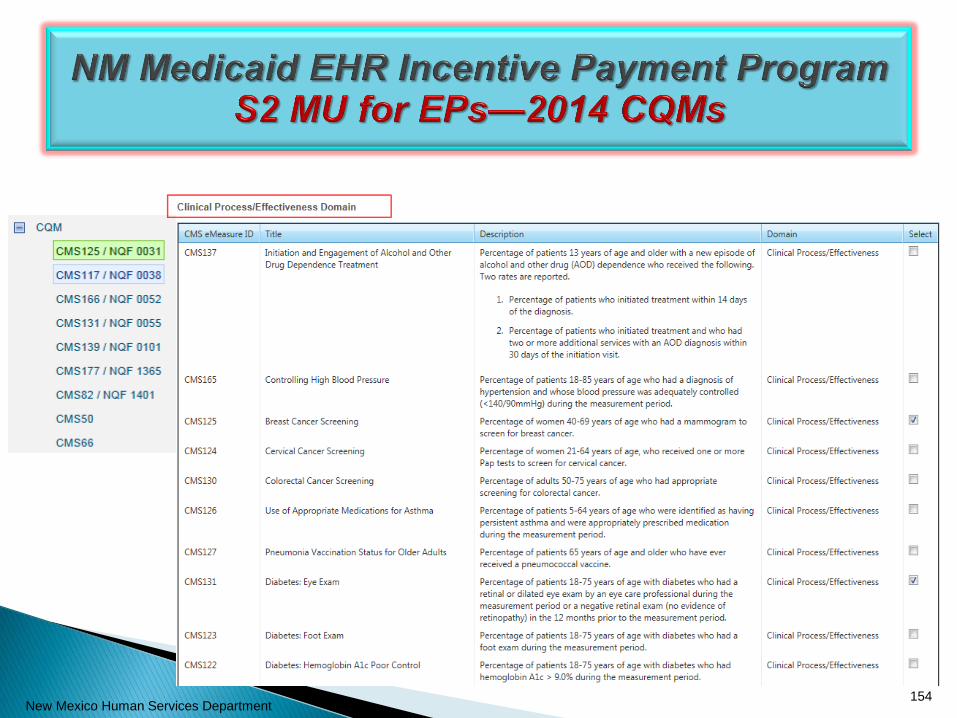
Clinical Quality Measures
• Specific to Medical
Conditions
• Help evaluate how a
particular medical
condition is treated

4 Components of CQMs
• Initial Patient Population: The group of patients the performance
measure is designed to address. Example: All patients 65 years and
older.
• Denominator: A subset of the initial patient population; in some
measures the denominator may be the same as the initial patient
population. Example: All patients 65 years and older with diabetes.
• Numerator: A subset of the denominator for whom a process or
outcome of care occurs. Example: Patients who had a diabetic foot
exam.
• Exclusions: The mechanism used to exclude patients from the
denominator of a performance measure when a therapy or service
would not be appropriate in instances for which the patient otherwise
meets the denominator criteria. Example: A patient with bilateral
lower extremity amputation is excluded from a measure of foot
exams.
145

146
May choose from:
• 9 CQMs for adult populations; OR
• 9 CQMs for pediatric populations; OR
• 9 CQMs total from a list of 64
Data must be reported directly from
information generated by CEHRT
9 CQMs should be individually certified by
the ONC
Report on 9 CQMs with a denominator
greater than zero; attach a copy of CEHRT
report including CQM data
9 CQMs must be from 3 of 6 NQS key health
care policy domains
1. Patient and Family Engagement
2. Patient Safety
3. Care Coordination
4. Population/Public Health
5. Efficient Use of Healthcare
Resources
6. Clinical Process/Effectiveness
Report on 9 out of 64 CQMs

147
Electronic CQMs are optional for 2014
Skip Import Screen and Click on CQMs

148
Electronic CQMs are optional for 2014
Skip Import

2014 Edition Stage 1 Only 9 Adult Core CQMs 1. Questionnaire (1 of 9): Controlling High Blood Pressure
2. Questionnaire (2 of 9): Use of High-Risk Medications in the Elderly
3. Questionnaire (3 of 9): Preventive Care and Screening: Tobacco Use: Screening and
Cessation Intervention
4. Questionnaire (4 of 9): Use of Imaging Studies for Low Back Pain
5. Questionnaire (5 of 9): Preventive Care and Screening: Screening for Clinical
Depression and Follow-Up Plan
6. Questionnaire (6 of 9): Documentation of Current Medications in the Medical Record
7. Questionnaire (7 of 9): Preventive Care and Screening: Body Mass Index (BMI)
Screening and Follow-Up
8. Questionnaire (8 of 9): Closing the referral loop: receipt of specialist report
9. Questionnaire (9 of 9): Functional status assessment for complex chronic conditions
https://www.cms.gov/Regulations-and-Guidance/Legislation/EHRIncentivePrograms/2014_ClinicalQualityMeasures.html
149

New Mexico Human Services Department
150

2014 Edition Stage 1 Only 9 Pediatric Core CQMs
1. Questionnaire (1 of 9): Appropriate Testing for Children with Pharyngitis
2. Questionnaire (2 of 9): Weight Assessment and Counseling for Nutrition and
Physical Activity for Children and Adolescents
3. Questionnaire (3 of 9): Chlamydia Screening for Women
4. Questionnaire (4 of 9): Use of Appropriate Medications for Asthma
5. Questionnaire (5 of 9): Childhood Immunization Status
6. Questionnaire (6 of 9): Appropriate Treatment for Children with Upper Respiratory
Infection (URI)
7. Questionnaire (7 of 9): ADHD: Follow-Up Care for Children Prescribed Attention-
Deficit/Hyperactivity Disorder (ADHD) Medication
8. Questionnaire (8 of 9): Preventive Care and Screening: Screening for Clinical
Depression and Follow-Up Plan
9. Questionnaire (9 of 9): Children who have dental decay or cavities
https://www.cms.gov/Regulations-and-Guidance/Legislation/EHRIncentivePrograms/2014_ClinicalQualityMeasures.html
151

2014 Edition Stage 1 Only SELECTION ERROR MESSAGES
• If you select less than 9 CQMs, when you hit Save & Continue, you will get the following error
message at the bottom of the selection page:
• If you select less than 3 domains, when you hit Save & Continue, you will get the following error
message at the bottom of the selection page:
152
New Mexico Human Services Department 153
New Mexico Human Services Department 154

New Mexico Human Services Department 155

New Mexico Human Services Department 156

New Mexico Human Services Department 157

New Mexico Human Services Department 158

New Mexico Human Services Department 159

New Mexico Human Services Department 160

New Mexico Human Services Department 161

CMS Links—Stage 2 MU
Stage 2 MU — https://www.cms.gov/Regulations-and-
Guidance/Legislation/EHRIncentivePrograms/Stage_2.html
Table: Core & Menu Set Objectives
http://www.cms.gov/Regulations-and-
Guidance/Legislation/EHRIncentivePrograms/Downloads/Stage2_Mean
ingfulUseSpecSheet_TableContents_EPs.pdf
Core and Menu Set—Zip File: at bottom of Stage 2 MU Page
2014 Clinical Quality Measures Page
http://www.cms.gov/Regulations-and-
Guidance/Legislation/EHRIncentivePrograms/2014_ClinicalQualityMeas
ures.html
162

CMS EHR Final Rules Links
EHR Final Rule 2010
http://www.gpo.gov/fdsys/pkg/FR-2010-07-28/pdf/2010-17207.pdf
EHR Stage 2 Final Rule 2012
http://www.gpo.gov/fdsys/pkg/FR-2012-09-04/pdf/2012-21050.pdf
CMS 2014 CEHRT Flexibility Rule - September 2014
http://www.gpo.gov/fdsys/pkg/FR-2014-09-04/pdf/2014-21021.pdf
163


Attestation
• Step 4 in the SLR: Print the attestation agreement.
• Attestation must be signed and dated by the Eligible Professional (EP). A practice
representative or MU/EHR coordinator cannot sign on behalf of the EP.
• Upload the signed and dated attestation agreement on Step 4.
• Step 5 in the SLR : Submit the signed and dated agreement electronically.
• Make a copy of the original agreement for your records for audit purposes.
• Mail the original signed and dated attestation to the address on the agreement.
• The Prepayment review process will begin upon receipt of the agreement..
165

Save All Documentation for 6 Years
• You will be asked to attach during attestation, or later submit,
documentation supporting the data from any of the sources
used in the Meaningful Use attestation process.
• It is the responsibility of the individual eligible professional to
retain all supporting documents, reports and other
information used in the attestation process for a period of
six years. This is true even if EPs enrolled in the EHR
program through the Group Administrator function or if EPs
change practice locations.
• Work with your EHR vendor to fully understand the capabilities
of your certified EHR technology. For example, if you were
randomly audited eight months after Meaningful Use
attestation, could your certified EHR produce the identical
report for the 90-day EHR reporting period you used for
Meaningful Use attestation? If not, keep an electronic file copy
or a hard copy of the report used for your attestation.
166
Group Administrator Webinar
Group Administrator is a “must use” function for any practice or clinic:
• whose EPs choose to use Group Patient Volume as proxy for the EPs
in the group; and/or
• will have one representative entering data in the NM SLR on behalf of
two or more EPs.
Group Administrator is the only approved method by the NM Medicaid EHR
Incentive Program for someone other than the eligible professional to enter
the data for attestation.
Contact [email protected] to schedule a webinar
demonstration customized to your practice or clinic; 505-827-1342.
167

New Mexico Program Contacts
Program Registration: Call 1-800-299-7304
Option 6, then 2
Email [email protected]
Policy Questions: Staff Manager
EHR Incentives Program
Phone: 505-827-1321
168

169
QUESTIONS???

170
THANK YOU!