prolonged diabetes reversal after intraportal xenotransplantation of wild-type porcine islets in...
TRANSCRIPT

Prolonged Diabetes Reversal after intraportal xenotransplantation of wild-type porcine islets in
immunosuppressed nonhuman primates Hering et al, Nature Medicine 12:301-303, 2006
• Reversal Diabetes > 100 days Porcine islet transplants into streptozotocin diabetic cynomolgus macaques
• Required Rx with toxic regimen including anti-CD154, leflunomide, basiliximab, FTY720 and everolimus
• No Gal-specific antibody mediated hyperacute rejection

Five-Year Follow-Up After Clinical Islet Transplantation
Ryan et al, Diabetes 54:2060-2069, 2005.
0
20
40
60
80
100
0 12 24 36 48 60
% Cpep Positive % Insulin Independent
Months of Follow-up
Percent derived from life Table

Issues in Islet Graft Issues in Islet Graft TransplantationTransplantation
•Allograft immunity
•Xenograft immunity
•Autoimmunity

TransplantImmunity Autoimmunity
Islets

00
100000
100000
200000
200000
300000
300000
400000
400000
500000
500000
600000
600000
Number of transplantsNumber of transplants
IsletIslet
PancreasPancreas
HeartHeart
KidneyKidney
World Experience in Organ / Tissue World Experience in Organ / Tissue TransplantationTransplantation
>500,000>500,000
>50,000>50,000
>13>13,000,000
<500<500

Autografts:Autografts: islets obtained islets obtained from the recipientfrom the recipient to toprevent pancreatectomy-induced diabetes prevent pancreatectomy-induced diabetes Autografts:Autografts: islets obtained islets obtained from the recipientfrom the recipient to toprevent pancreatectomy-induced diabetes prevent pancreatectomy-induced diabetes
Allografts: Allografts: islets obtained from an islets obtained from an unrelatedunrelateddonordonor to prevent pancreatectomy-induced diabetes to prevent pancreatectomy-induced diabetes
Allografts + IDDM: Allografts + IDDM: islets obtained from an islets obtained from an unrelated donor after or at the same time as unrelated donor after or at the same time as kidney transplantationkidney transplantation
Clinical Experience in Islet TransplantationClinical Experience in Islet Transplantation

Islet Transplantation Registry Islet Transplantation Registry
10090
80
70
60
5040
30
0
2010
0 1 2 3 4 5 76 8 9 1210 11
Autografts (n=50, 50%)Autografts (n=50, 50%)
Allografts (n=15, 40%)Allografts (n=15, 40%)
Allografts + IDDM (n=200, 8%)Allografts + IDDM (n=200, 8%)
Months post-Months post-transplantationtransplantation
1990 - 19971990 - 1997%
In
suli
n-I
nd
epen
den
ce%
In
suli
n-I
nd
epen
den
ce

IsletsIslets
Possible Reasons for Islet Graft Possible Reasons for Islet Graft FailureFailure
Allograft rejectionAllograft rejectionDisease recurrenceDisease recurrence
Insufficient islet massInsufficient islet mass Poor quality of isletsPoor quality of islets
Toxicity of anti-Toxicity of anti-rejection drugsrejection drugs
Failure to engraftFailure to engraft
Insulin resistanceInsulin resistance

`Edmonton’ Protocol`Edmonton’ Protocol`Edmonton’ Protocol`Edmonton’ Protocol
• Islet-alone transplantation trialIslet-alone transplantation trial
• Standard immunosuppressive therapy was Standard immunosuppressive therapy was replaced with a steroid-free protocol: replaced with a steroid-free protocol:
• Type 1 diabetic patients received two Type 1 diabetic patients received two transplantstransplants of large numbers of high quality islets.of large numbers of high quality islets.
University of Alberta, Edmonton, AlbertaUniversity of Alberta, Edmonton, AlbertaUniversity of Alberta, Edmonton, AlbertaUniversity of Alberta, Edmonton, AlbertaJ. Shapiro, M.D.J. Shapiro, M.D. R. Rajotte, Ph.D.R. Rajotte, Ph.D.
DaclizumabDaclizumab (DZB) (anti-IL2 receptor antibody) (DZB) (anti-IL2 receptor antibody)Daily doses of Daily doses of sirolimussirolimus and low-dose and low-dose tacrolimustacrolimus

Eligibility CriteriaEligibility CriteriaEligibility CriteriaEligibility Criteria
• Evidence of early diabetic nephropathy or other Evidence of early diabetic nephropathy or other secondary complicationssecondary complications
• Hypoglycemia unawareness requiring medical Hypoglycemia unawareness requiring medical assistanceassistance
• Uncontrolled blood sugars despite intensive Uncontrolled blood sugars despite intensive insulin therapy (“ brittle diabetes”).insulin therapy (“ brittle diabetes”).
• 18-55 years of age, have had IDDM for >5 18-55 years of age, have had IDDM for >5 yearsyears

Exclusion CriteriaExclusion CriteriaExclusion CriteriaExclusion Criteria
• cardiac disease or psychiatric illnesscardiac disease or psychiatric illness
• active alcohol or substance active alcohol or substance abuseabuse• previous transplantprevious transplant
• a history of malignancy or abnormal liver a history of malignancy or abnormal liver functionfunction• an active infection (HIV, Hepatitis B or C, an active infection (HIV, Hepatitis B or C, TB)TB)
• 13 consecutive cases of insulin-13 consecutive cases of insulin-independence with a duration of (longest > independence with a duration of (longest > 2.5 years) 2.5 years)
• no episodes of acute rejection and no episodes of acute rejection and minimal toxicity from anti-rejection drug minimal toxicity from anti-rejection drug therapytherapy
`Edmonton Protocol’`Edmonton Protocol’`Edmonton Protocol’`Edmonton Protocol’ResultsResults
• no episodes of hypoglycemiano episodes of hypoglycemia
• normalization of HbA1C values (mean normalization of HbA1C values (mean of 5.7% at 3 and 6 months post-of 5.7% at 3 and 6 months post-transplantation)transplantation)

600
500
400
300
200
100
0
2 4 6 8 10 12 2 4 6 8 10
600
500
400
300
200
100
012
a.m. p.m.
Post-transplantPost-transplant
Pre-transplantPre-transplant
Time of dayTime of day
Blo
od
glu
cose (
mg
/dl)
Blo
od
glu
cose (
mg
/dl) B
lood
glu
cose (
mg
/dl)
Blo
od
glu
cose (
mg
/dl)
Shapiro et al. Shapiro et al. N Engl J Med N Engl J Med 2000; 343:230-2000; 343:230-238238

Islet Transplantation: The NIH ExperienceDiabetes Care 2003: 26:3288-95
• Major Procedure ComplicationsPartial portal vein thrombosisIntra-abdominal hemorrhage
• Immunosupression ComplicationsKidney ToxicitySirolimun-induced Pneumonitis
• Three Patients Discontinued Immunotherapy
½ Patients insulin-independent at one year
Decreased Hypoglycemia and less severe Hypoglycemia
0
10
20
30
40
50
60
70
80
90
100
Panc Alone Panc after Kidney Combined Panc Kidney
Transplanted Waiting List
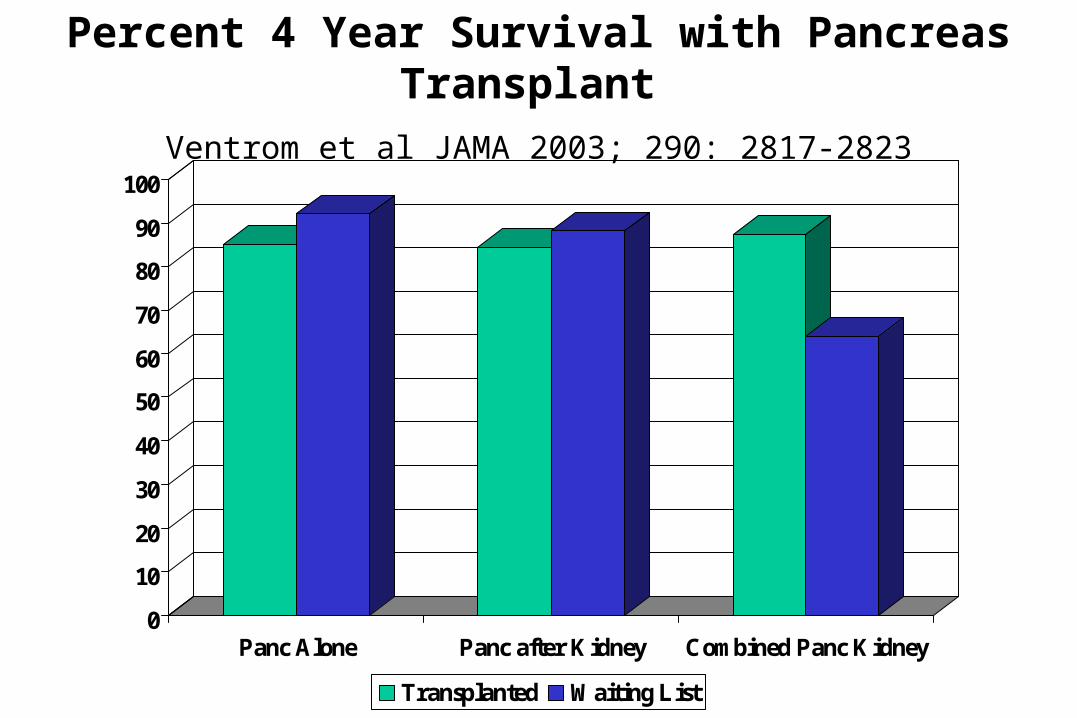
Percent 4 Year Survival with Pancreas Transplant
Ventrom et al JAMA 2003; 290: 2817-2823

Future DirectionsFuture DirectionsFuture DirectionsFuture Directions
• Reduce requirement to single pancreas / Reduce requirement to single pancreas / recipientrecipient
• Interventions to reduce peri-transplant Interventions to reduce peri-transplant inflammationinflammation
• Progress towards ‘tolerizing’ Progress towards ‘tolerizing’ strategiesstrategies

Alternative sources of tissueAlternative sources of tissueAlternative sources of tissueAlternative sources of tissue
• insulin-producing cell insulin-producing cell lineslines
• xenografts (other xenografts (other species)species)
• stem cellsstem cells

Experimental Islet Experimental Islet TransplantationTransplantation
C57Bl/6 mouse (H-2b)Remove pancreas
Isolate islets
Transplant islets under kidney capsule
Streptozotocin-induced diabetic BALB/c mouse (H-2d)

Key Components to Islet Key Components to Islet Allograft Cellular RejectionAllograft Cellular RejectionKey Components to Islet Key Components to Islet
Allograft Cellular RejectionAllograft Cellular Rejection
• DonorDonor-derived APCs -derived APCs
• Host CD8 T cells Host CD8 T cells
• DonorDonor MHC class I MHC class I expressionexpression
• Variable requirement for Variable requirement for CD4 T CD4 T cell help cell help

Key Components to Islet Key Components to Islet Xenograft Cellular RejectionXenograft Cellular Rejection
Key Components to Islet Key Components to Islet Xenograft Cellular RejectionXenograft Cellular Rejection
• HostHost-derived APCs -derived APCs
• Host CD4 T cells Host CD4 T cells
• HostHost MHC class II MHC class II expressionexpression
Conclusion / Hypothesis Conclusion / Hypothesis Conclusion / Hypothesis Conclusion / Hypothesis
• Xenograft Rejection and Xenograft Rejection and Autoimmune Autoimmune pathogenesispathogenesis --> --> Predominant CD4-Predominant CD4- dependent dependent ‘indirect’ recognition‘indirect’ recognition
• Allograft RejectionAllograft Rejection --> Predominant --> Predominant CD8-CD8- dependent ‘direct’ dependent ‘direct’ recognitionrecognition
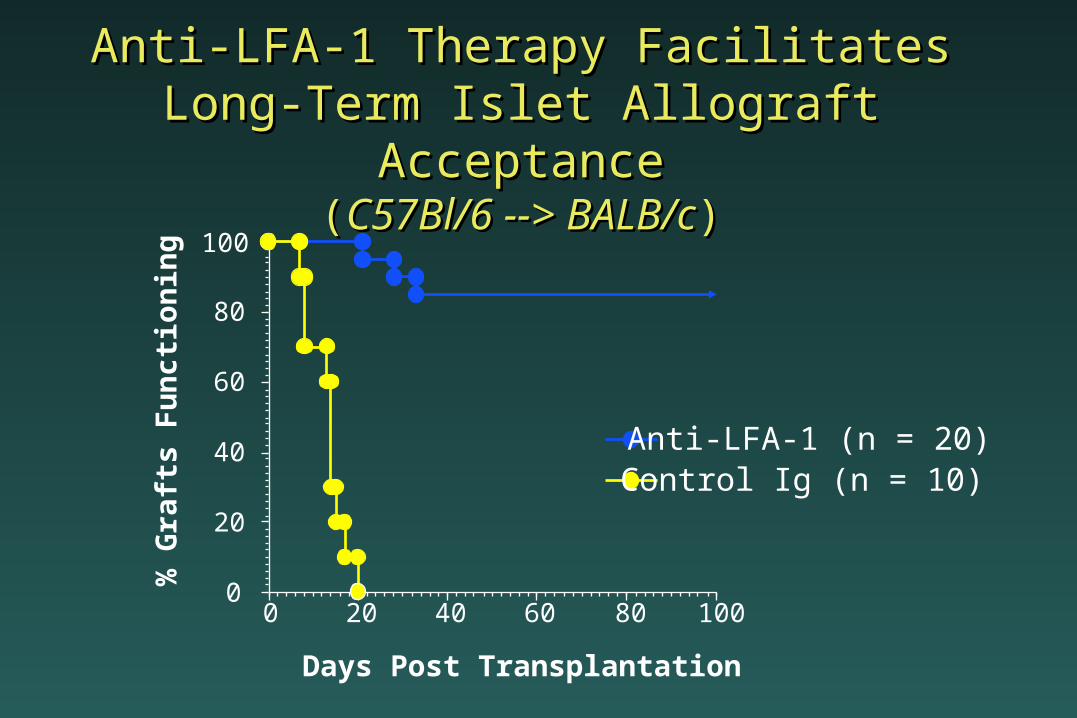
Anti-LFA-1 Therapy Facilitates Long-Anti-LFA-1 Therapy Facilitates Long-Term Islet Allograft AcceptanceTerm Islet Allograft Acceptance
((C57Bl/6 --> BALB/cC57Bl/6 --> BALB/c))
0
20
40
60
80
100
0 20 40 60 80 100
% G
raft
s F
un
ctio
nin
g
Days Post Transplantation
Anti-LFA-1 (n = 20)Control Ig (n = 10)

Failure of Anti-LFA-1 to Prevent Disease Failure of Anti-LFA-1 to Prevent Disease RecurrenceRecurrence
((NOD --> NODNOD --> NOD))
0
20
40
60
80
100
0 20 40 60 80 100
% G
raft
s F
unct
ioni
ng
Days Post Transplantation
Untreated (n = 10)
Anti-LFA-1 (n = 8)
Young SZ-NOD (n = 3)

11000088006600440022000000
2200
4400
6600
8800
110000
Anti-CD4 but not anti-CD8 therapy preventsAnti-CD4 but not anti-CD8 therapy preventsAnti-CD4 but not anti-CD8 therapy preventsAnti-CD4 but not anti-CD8 therapy prevents
acute disease recurrence in NOD miceacute disease recurrence in NOD mice acute disease recurrence in NOD miceacute disease recurrence in NOD mice
Days Post-transplantationDays Post-transplantation Days Post-transplantationDays Post-transplantation
Untreated (n=8)Untreated (n=8)
Anti-CD8 (116-13.1; n=10)Anti-CD8 (116-13.1; n=10)
Anti-CD4 (GK1.5; n=9)Anti-CD4 (GK1.5; n=9)
% G
raft
s F
un
ctio
nin
g%
Gra
fts
Fu
nct
ion
ing
% G
raft
s F
un
ctio
nin
g%
Gra
fts
Fu
nct
ion
ing
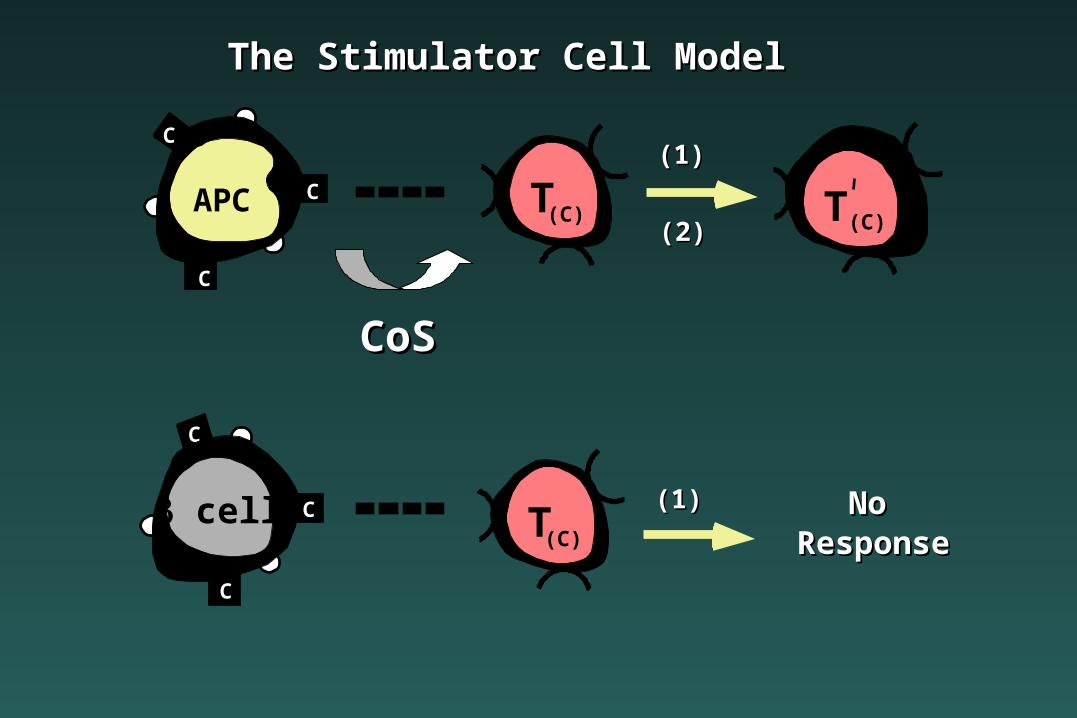
C
C
CAPC T(C) T (C)
T(C)
CoSCoS
(1)(1)
(1)(1)
(2)(2)
NoNoResponseResponse
C
C
C cell
The Stimulator Cell ModelThe Stimulator Cell Model

DIRECTDIRECT
T(B.X) T(B.X)
INDIRECTINDIRECT
(1)(1)
(2)(2)T(A) T (A)
(1)(1)
(2)(2)
A
A
AAPC
DONOR
Shed GraftShed Graft AntigensAntigens
(X)(X)
B
B
APCHOST
Bx
x
x

GRAFT
Delayed-Type Hypersensitivity
CD4 T Cell
B Cell Help
CD8 T CellHelp

No direct
CD4II (x )
'INDIRECT'
Shed graftantigen (X)
II
II
APCHOST
IIx
x
x
CD8IAPC-depleted
islet allograftresponse

DIRECT
CD4 II (X)
INDIRECT
CD8I
IIAPCHOST
x
x
x
II
II
( )
APCDONOR I
I
I
Shed graftantigen (X)
APC-depletedislet allograft
TOLERANCETOLERANCE