proposing a new indication for sporanox tm - in the treatment of cancer
TRANSCRIPT
Certificate in Clinical Pharmacology and SafetyAssessmentsPresented by: Carolina Hung HoResearch Director: Professor Peivand PirouziMay 05, 2016
Proposed New Indication forSporanox® in the Treatmentof Cancer

Outline Introduction
PharmacokineticsAbsorptionDistributionMetabolism Elimination
PharmacodynamicsCYP-450-dependent Inhibition
of Ergosterol SynthesisDrug and Drug InteractionsDrug and Food InteractionsAdverse Drug Reactions
Pharmacogenomics
Special Population
Proposed New Indication: Anti-Cancer Properties Proposed Mechanisms forAnti-cancer activityCyclodextrinsChallenges
Conclusions
Question Session
Introduction Itraconazole (ITZ) is used to treat many fungal
infections.
Invented in 1984.
Marketed under several brand names.
Janssen Pharmaceutica: Sporanox®
Available as a 100 mg capsule and 10 mg/mLoral suspension
Prescription only
IV form is not available in the USA or CAD.
DIN: 02047454(Canada, 1993)
DIN: 02231347(Canada, 1997)

Chemical Information Proper name: ItraconazoleA synthetic triazole derivative
Chemical name:(±)-cis-4-[4-[4-[4-[[2-(2,4-dichlorophenyl)-2-(1H-1,2,4-triazol-1- ylmethyl)-1,3-dioxolan-4-yl]methoxy]phenyl]-1-piperazinyl]phenyl]-2,4-dihydro-2-(1-methylpropyl)-3H-1,2,4-triazol-3-one
Structural formula:
Lipophilic molecule
pKa = 3.7
Log partition coefficient inoctanol/water =8.2
Figure 1: Chemical Structure of Itraconazole (Janssen, 2015)

Approved Indications SPORANOX® capsules (100 mg):
1. Invasive and non-invasive pulmonary aspergillosis.
2. Oral and/or esophageal candidiasis.
3. Chronic pulmonary histoplasmosis.
4. Cutaneous and lymphatic sporotrichosis.
5. Paracoccidioidomycosis.
6. Chromomycosis.
7. Blastomycosis.
8. Dermatomycosis
9. Onychomycosis.
Systemic fungalinfections
Topical fungalinfections
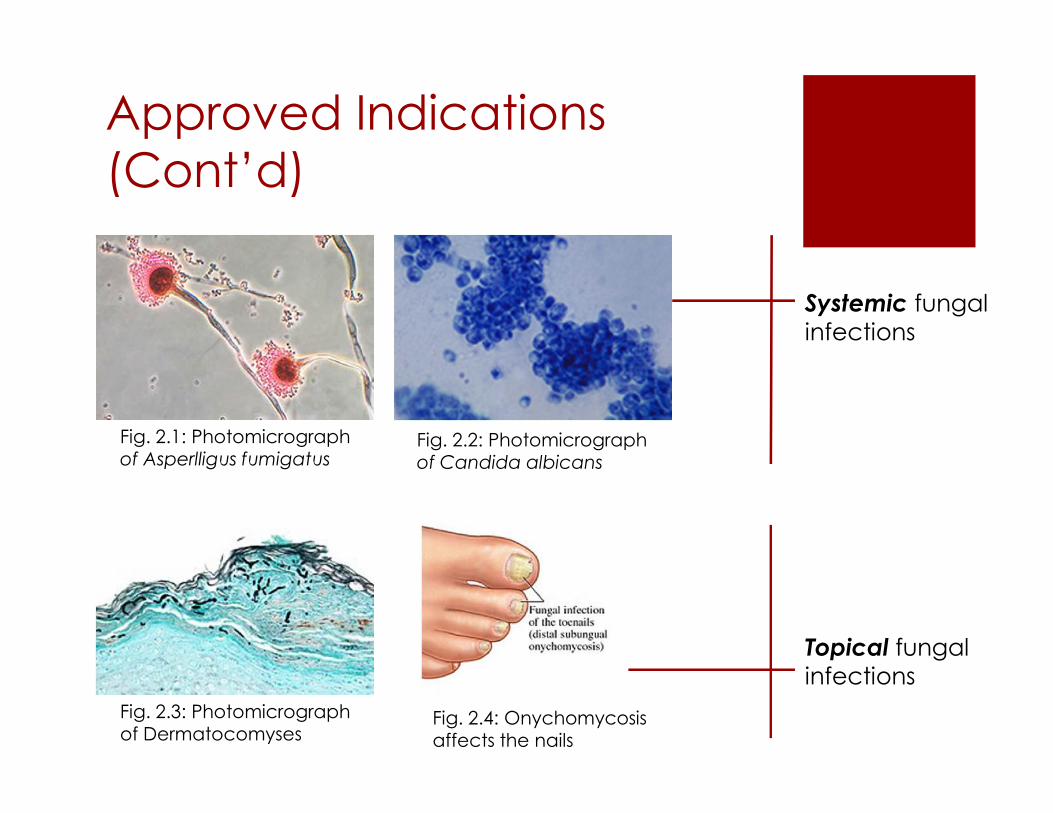
Approved Indications(Cont’d)
Systemic fungalinfections
Topical fungalinfections
Fig. 2.1: Photomicrographof Asperlligus fumigatus
Fig. 2.2: Photomicrographof Candida albicans
Fig. 2.3: Photomicrographof Dermatocomyses
Fig. 2.4: Onychomycosisaffects the nails

Approved Indications(Cont’d) SPORANOX® oral solution (10 mg/ mL):
1. Oral and/or esophageal candidiasis
• SPORANOX® is safe for use in normal, predisposed, orimmunocompromised adult patients (e.g. HIV-positive)
• SPORANOX® oral solution and SPORANOX® capsules should not beused interchangeably
• For use in special populations, see Special Populations

Pharmacokinetics
Absorption Oral bioavailability of SPORANOX® capsules is maximal
when taken immediately after a full meal. (Addedexcipient: sugar spheres)
Oral bioavailability of SPORANOX® oral solution is maximalwhen taken without food. (Added excipient:hydroxypropyl-β-cyclodextrin)
Table 1: Pharmacokinetic data on Itraconazole froma randomized, cross-over study on 7 healthy malesubjects following administration of an oral solutionPlasma clearance rate = 381 ± 95 mL/minVolume of distribution = 796 ± 185 LOral bioavailability = 33% - 55% (variable)
Pharmacokinetics
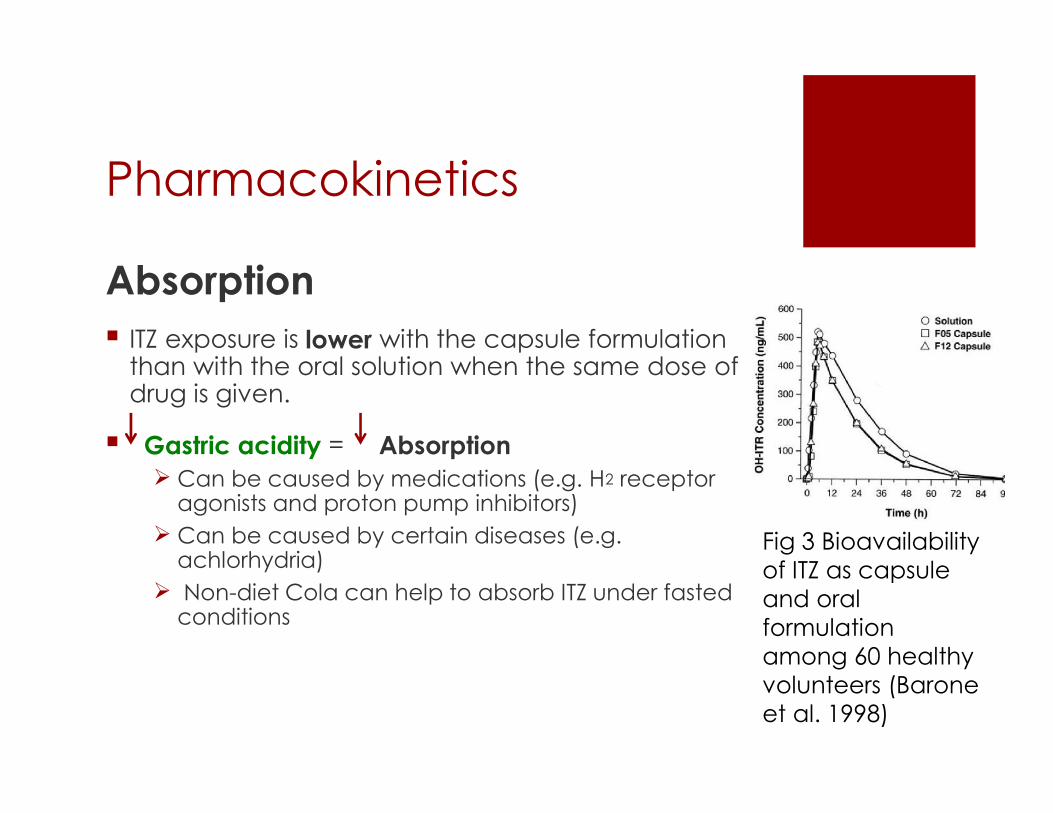
Absorption ITZ exposure is lower with the capsule formulation
than with the oral solution when the same dose ofdrug is given.
Gastric acidity = Absorption Can be caused by medications (e.g. H2 receptor
agonists and proton pump inhibitors) Can be caused by certain diseases (e.g.
achlorhydria) Non-diet Cola can help to absorb ITZ under fasted
conditions
Fig 3 Bioavailabilityof ITZ as capsuleand oralformulationamong 60 healthyvolunteers (Baroneet al. 1998)
Pharmacokinetics (Cont’d)
Distribution The plasma protein binding of ITZ is 99.8% and that
of hydroxy-ITZ is 99.5%
ITZ is extensively distributed into tissues which areprone to fungal infection: Lung Kidney Bones Stomach Spleen Muscle Skin Cskin is 5X higher than
Cplasma
Ctissues is 2X times than Cplasma

Pharmacokinetics (Cont’d)
Metabolism Extensive metabolism by the liver
Major enzyme: CYP 3A4
Main metabolite: Hydroxy-itraconazole (OH-ITZ) Same antifungal effect efficacy maintained Present 3x higher in the tissues (HPLC) Shorter T1/2 of elimination
> 30 other metabolic pathways involved.

Pharmacokinetics (Cont’d)
Hydroxylation – adding –OH
By CYP 3A4-body attempt to makecompound more polar forconjugation and subsequentelimination.
Pharmacokinetics (Cont’d)
Elimination The feces (18% as active drug, 54% as inactive
metabolites ) Active transport in the bile Using oral radiolabelled dose to track its fate.
The urine (< 0.03% active drug, 35% as inactivemetabolites)
Pharmacokinetics (Cont’d)
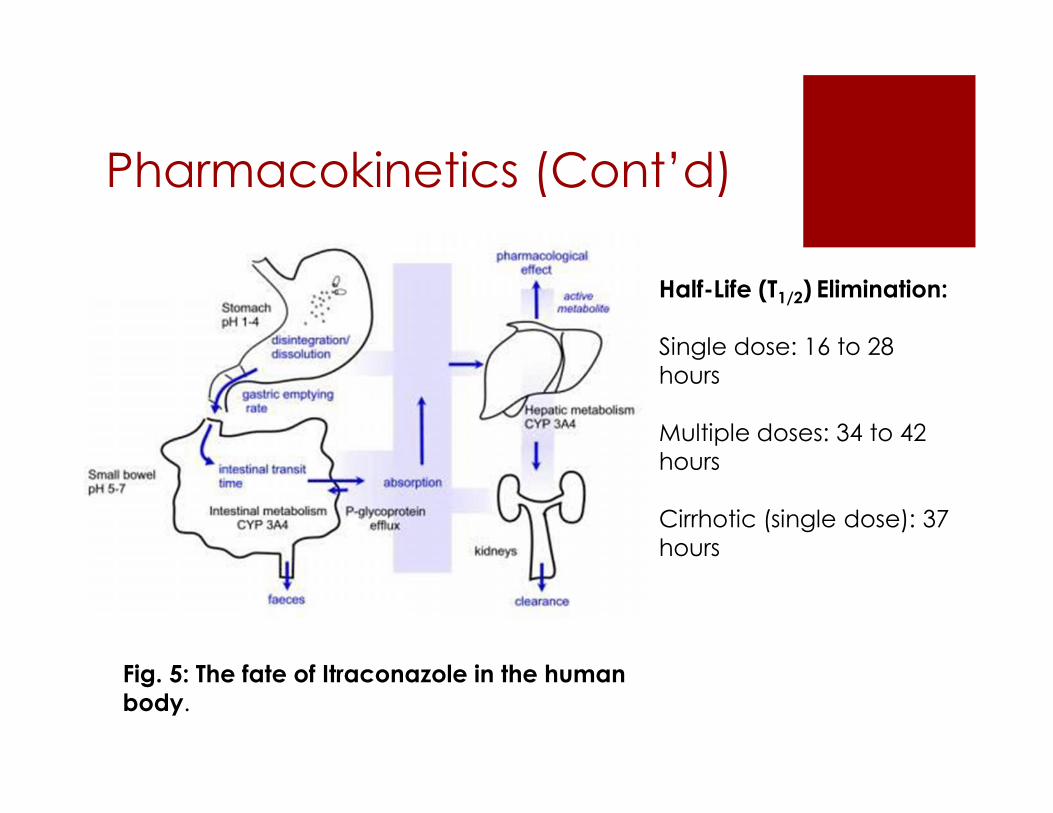
Fig. 5: The fate of Itraconazole in the humanbody.
Half-Life (T1/2) Elimination:
Single dose: 16 to 28hours
Multiple doses: 34 to 42hours
Cirrhotic (single dose): 37hours

Mode of Action
ITZ Inhibits P450 lanosterol 14-demethylase Enzyme responsible for
converting lanosterolergosterol
Ergosterol is needed for cellmembrane fluidity & stability.
Without ergosterol, cellmembrane is disrupted.
Fungi are unable to grow anddivide Fig 6: Structure of P450
lanosterol 14-demythalase(Podul et al.)

Mode of Action
Fig 7: Cell membrane and cell wall structure of a fungal cell

Drug-Drug Interactions ITZ (and its metabolites) are potent CYP 3A4 inhibitors By competing with other substrates for CYP 3A4 binding
sites in liver hepatocytes
ITZ is a potent P-glycoprotein (P-gp) inhibitor By competing with other substrates for P-g binding sites in
the liver, kidney, endothelium, and brain. Pg is responsible for active transport drugs back into the
gut lumen or into the bile.
RESULT: May alter Cp of other drugs or other drugs mayalter Cp of ITZ Prolonged therapeutic effects or overdose of these drugs Therefore, many drugs are contraindicated with
SPORANOX® a long list!
e.g. ITZ mayelevate morphineplasmaconcentrations,possibly byinhibiting P-gelimination ofmorphine into gutlumen
Drug Contraindications
Refer to Product Monograph for Itraconazole fora list of contraindicated medications
• CONTRAINDICATED (Table 1)• May increase risks of serious cardiovascular events
(e.g. QT prolongation, Torsade de pointes, bleeding,etc).
• NOT RECOMMENDED (Table 2)• If co-administration cannot be avoided, consider
monitoring signs, symptoms, plasma levels of ITZ, doseadjustment, etc.
• USE WITH CAUTION (Table 3)• Interaction is not well established.• Monitoring required• Special populations

Food-Drug Interactions Grapefruit juice is also a CYP 3A4
inhibitor
The culprit: furanocomarins
It may:1. May reduce or raise Cp of ITZ2.
Therefore, grapefruit juice is NOTrecommended when takingSPORANOX®
Fig. 8 Furanocomarinin Grapefruit juice

Adverse Reactions Rare and serious: Hepatotoxivity Acute liver
failure and death
Common ADRs: GI origin (dyspepsia, nausea,vomiting, diarrhea, abdominal pain, andconstipation).
Overdosage: No experience with overdosage If suspected, treated with activated charcoal. ITZ cannot be removed through hemodialysis
Other toxicity: Mutagenicity : NO Teratogenicity: NO

Pharmacodynamics In vitro studies (cultured cells):
[ITZ] = 4 x 10-7M 50% inhibition of cholesterol biosynthesis inhuman lymphocytes.
[ITZ] = 4 x 10-5M 50% inhibition of ergosterol in Candidaalbicans cells.
Point 1: ITZ is selectively toxic to fungal cells
Phase I (healthy volunteers):
100 mg ITZ o.d. for 1 month no difference in basal serumcholesterol levels between control and treatment groups.
50 - 400 mg ITZ o.d. for max. 2 years basal serumcholesterol were not significantly affected in 3 studies.
Point 2: Short and long-term exposure to ITZ does notsignificantly affect cholesterol levels in human
Note:Your Total Blood (orSerum) Cholesterol.Your total cholesterolscore is calculatedby the followingequation: HDL + LDL+ 20% of yourtriglyceride level. Atotal cholesterolscore of less than 180mg/dL is consideredoptimal.
Pharmacodynamics Phase I (healthy volunteers):
100 mg or 200 mg daily for 1 month no significant change in hormone levels: CNS (e.g. LH, FSH, prolactin) Reproductive organs (e.g. estrogen, testosterone) Adrenal gland (e.g. cortisol)
Point 3: ITZ does not cross BBB into cerebrospinal fluid. (cannot reachyour brain)
200 mg daily for 5 weeks no significant effect on the HR, BP, ECG-intervals inhealth volunteers
Point 4: ITZ does not affect the cardiovascular system
200 mg daily for 5 weeks no negative effect on immune functions. Values forOKT4 positive lymphocyte showed a significant shift from 42 ± 3.3% to 53 ±3.3%. This increase, as well as shifts in the other immunological parameters,remained within the normal ranges.
Point 5: ITZ does not affect immune system.

Pharmacodynamics
In summary:
Safe for human; does not affect cholesterol levels Does not adversely affect the brain, the heart or the immune
system directly. Exception: Rare cases of CHF. Precautions must be taken, however, when co-administered
with other medications and grapefruit juice.
But what about the kidney and the liver? See “Warnings and Precautions” See “Drug Interactions”

Special Population Geriatrics (> 65 years of age):
Use caution
Use only when potential benefit outweighs thepotential risks
Pediatrics (< 18 years of age):
The efficacy and safety of SPORANOX® have notyet been established.
Use caution
Special Population Pregnant Women and Lactating Mothers:
Should not be used if pregnant or planningpregnancy, except for life-threatening cases wherethe potential benefit to the mother outweighs thepotential harm to the fetus.
For women of childbearing age, SPORANOX®should not be prescribed unless effectivecontraception methods are used prior to the startof therapy.
Nursing Women:
Itraconazole is excreted in human milk; therefore,the patient should be advised to discontinuenursing while taking SPORANOX®.
Special Population Impaired renal function:
Limited data available. Exercise caution.
ITZ is mainly excreted through the feces, so BA isslightly increased if kidney function is impaired.
Impaired liver function:
Limited data available. Exercise caution
Cmax was reduced by 47% and resulted in atwofold increase in half-life (capsules).
ITZ is extensively metabolized by the liver, soimpaired liver function (e.g. cirrhosis, liver failure)elevate BA of other drugs overdose + toxicity

Pharmacodynamics(Cont’d) Efficacy & Safety
Large Vdist’n
Long T1/2
Main metabolite works just aswell as the parent drug
Precaution taken with: Concomitant medications Liver or kidney failure History of CHF Special populations
Fig. 9: Plasma concentrations ofItraconazole and its metabolite,hydroxyitraconazole.

Proposed New Indication forSporanox®
FungalInfections
Anti-CancerDrug
Current Indication: Proposed Indication:
Use as prophylacticagent and/or as part of
chemotherapy
Fights off infectionscaused by many fungal
species

Why Choose Sporanox® ?
Shown to have anti-neoplastic effects in vitro and invivo pre-clinical trials 2 Proposed Mechanisms
1 Block the angiogenesis pathway2 Block the Hedgehog signaling pathway
Types of cells studied: Basal cell carcinoma Non-small lung cancer cells Prostrate cancer cells Breast cancer cells
Long and well established safety profile
An affordable and accessible generic drug
Why Choose Sporanox® ?
Phase II Trial:A Randomized Phase II Clinical Trial of Two Dose-levels ofItraconazole in Patients With Metastatic Castration-resistantProstate Cancer
Identifier: NCT00887458
Sponsor: Johns Hopkins University
Collaborator: Memorial Sloan Kettering Cancer Center
Start date: July 2009
End date: December 2013

Phase II Study
Investigational drug: Itraconazole
Condition: Prostrate Cancer
Study type: Efficacy
Duration: 24 weeks (6 months)
N= 42 patients
Treatment:
Group Treatment Total dailydose
Low dose 200 mg by mouth, once daily 200 mgHigh dose 300 mg by mouth, twice daily 600 mg

Phase II Study (Cont’d) Results
1. Efficacy
*PSA – Prostrate Specific Antigen are secreted by prostratetumour cells; serve as tumour markers
*PSA progression is defined as a 25% increase in PSA over baselineor a 2 ng/ml increase when confirmed again 4 weeks later.
Conclusion: High dose ITZ (600mg/day) significant PSA responsesand delay in tumour progression.
Group Total daily dose Subjects No PSA Progression at24 weeks (95% CI)
Low dose 200 mg 17 11%High dose 600 mg 25 48%
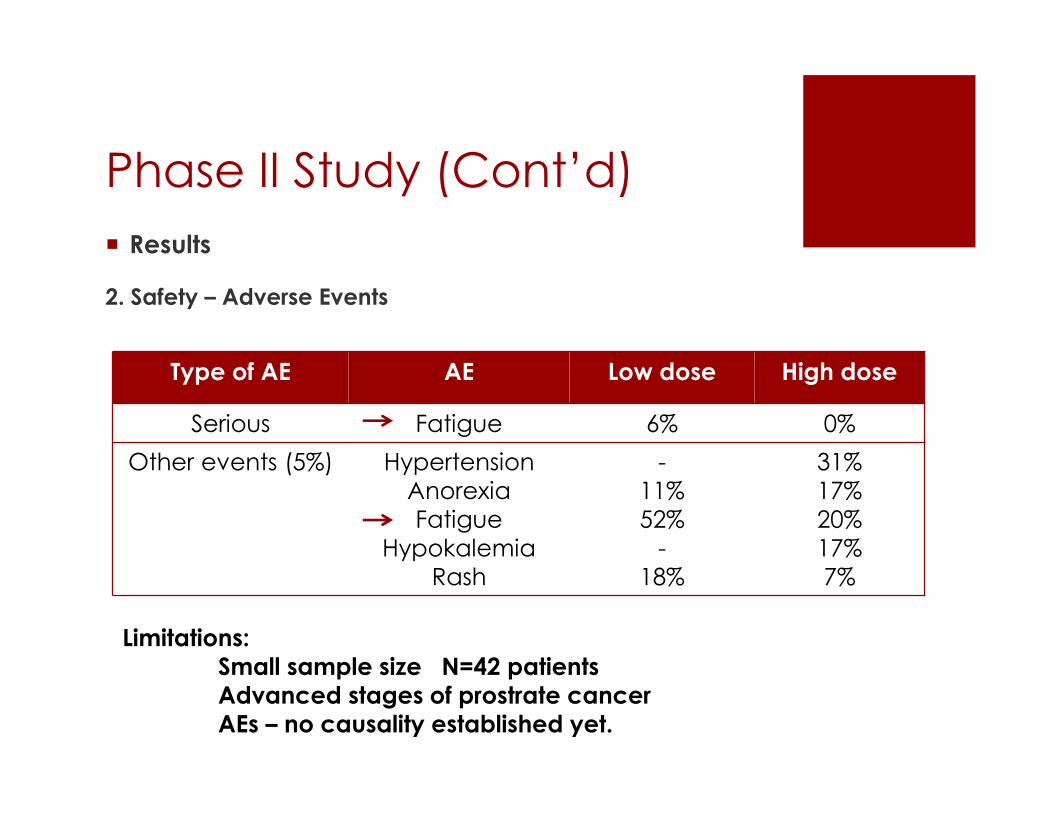
Phase II Study (Cont’d) Results
2. Safety – Adverse Events
Type of AE AE Low dose High dose
Serious Fatigue 6% 0%Other events (5%) Hypertension
AnorexiaFatigue
HypokalemiaRash
-11%52%
-18%
31%17%20%17%7%
Limitations:Small sample size N=42 patientsAdvanced stages of prostrate cancerAEs – no causality established yet.
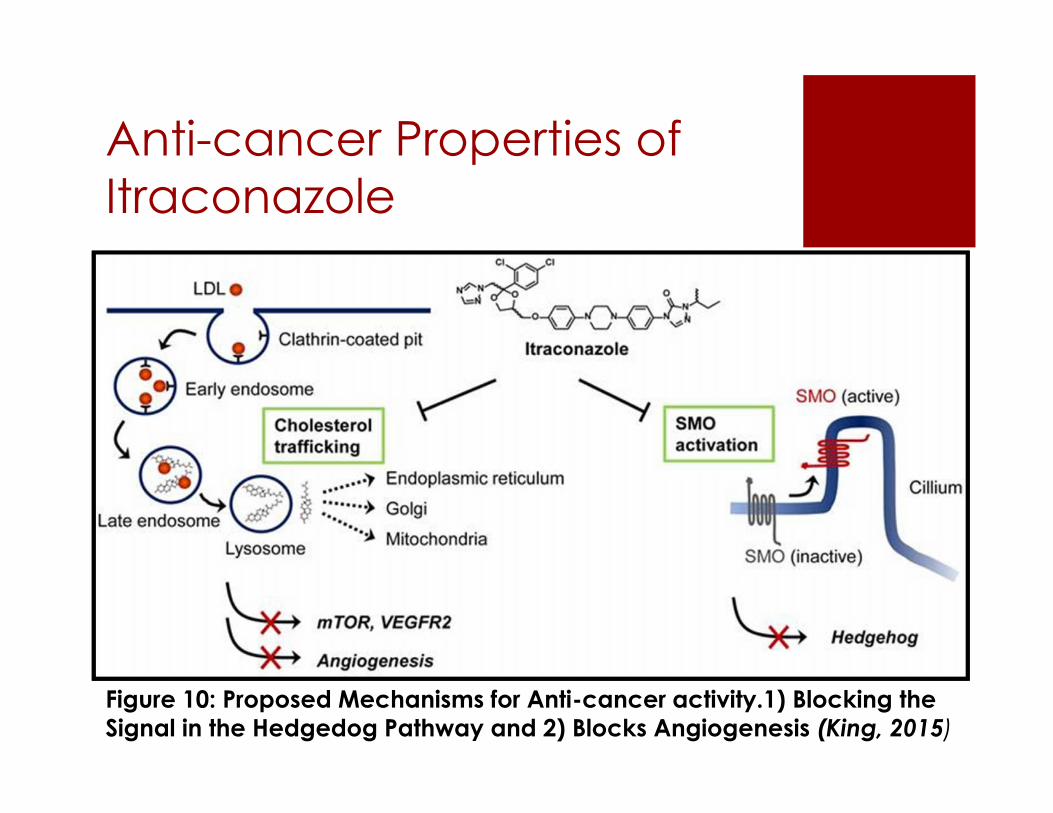
Anti-cancer Properties ofItraconazole
Figure 10: Proposed Mechanisms for Anti-cancer activity.1) Blocking theSignal in the Hedgedog Pathway and 2) Blocks Angiogenesis (King, 2015)

Blocking the AngiogenesisPathway: Sporanox®
Angiogenesis describes the processwhy which new blood vessels grow.
Cancer cells need blood vessels togrow and metastasize.
Cancer cells grow their vessels byreleasing angiogenic growth factorproteins (e.g. VEGH).
ITZ has been shown to block thispathway in cancer cell lines byinducing inhibitory factors
Hope to see that it can also stopcancer cells from growing vessels inhumans
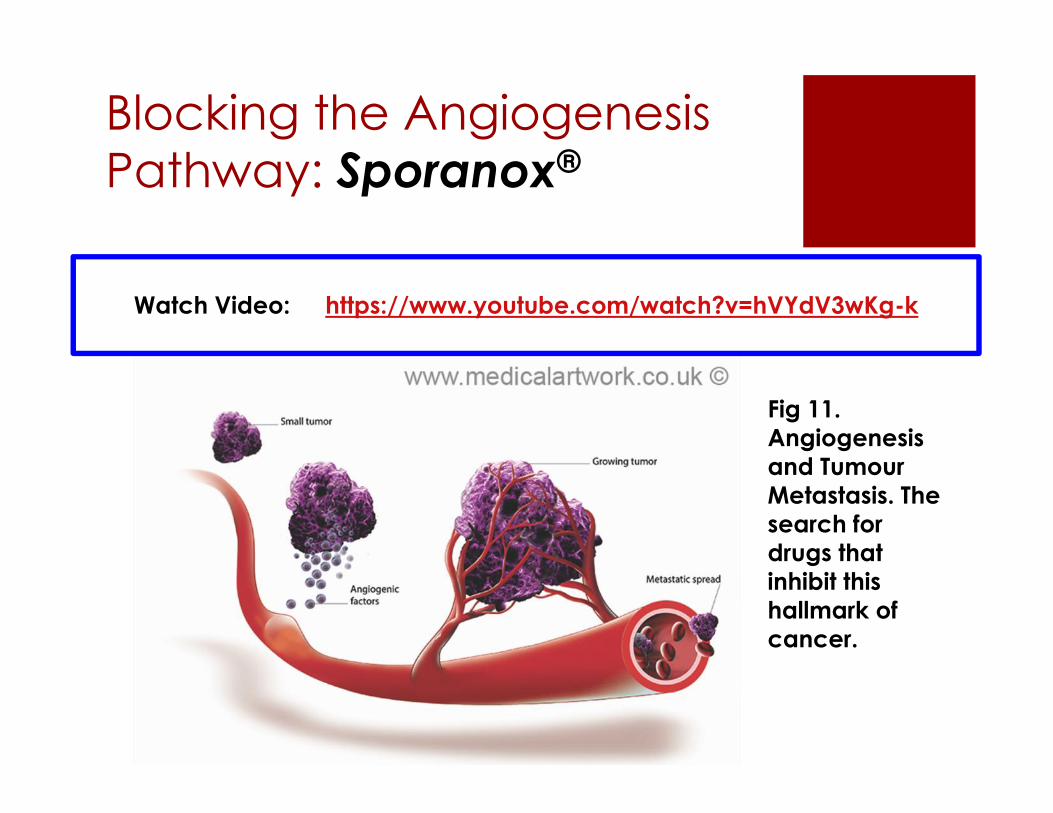
Blocking the AngiogenesisPathway: Sporanox®
Watch Video: https://www.youtube.com/watch?v=hVYdV3wKg-k
Fig 11.Angiogenesisand TumourMetastasis. Thesearch fordrugs thatinhibit thishallmark ofcancer.

Figure 12:Itraconazole andItraconazole plusCisplatin (anapprovedchemotherapeuticdrug) has shownsignificantreduction inendothelial cellproliferation,migration, andtube formation inresponse toangiogenicstimulation fromnon-small cellcancer lines(Afba, et al., 2011)
Blocking the HedgehogSignaling Pathway Sporanox®
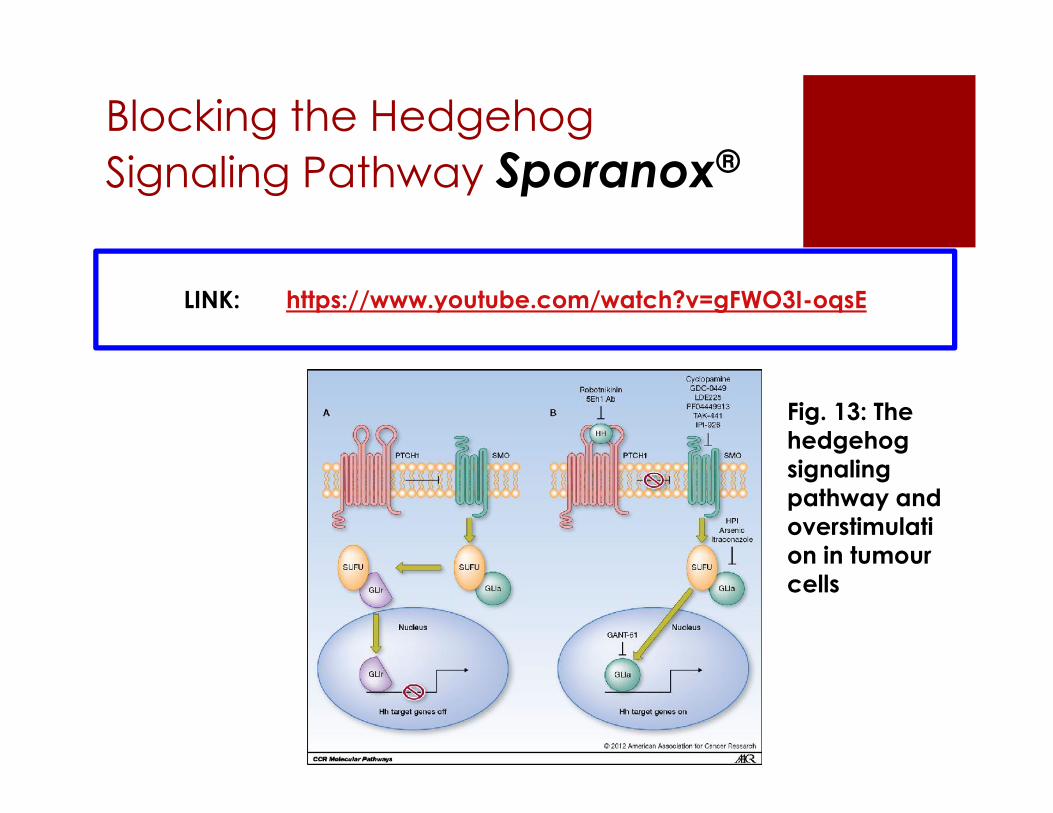
LINK: https://www.youtube.com/watch?v=gFWO3I-oqsE
Fig. 13: Thehedgehogsignalingpathway andoverstimulation in tumourcells
Blocking the HedgehogSignaling Pathway Sporanox®
Hedgehog signaling pathway is essential forembryonic development; remains active in adulttissues
Involve proteins that control cell proliferation,differentiation, and tissue patterning.
Over-stimulation of this pathway has been linkedto cancer of the brain, GI, lung, breast, andprostrate gland.
ITZ has shown to inhibit this signaling pathway;thus slowing cancer progression.

Challenges for Sporanox®:
Challenge 1: Varied bioavailability Capsule: 6%-20% Oral Solution: 20%-60%
2-(HYDROXYPROPYL)-BETA-CYCLODEXTRIN An excipient in oral solution and IV formulation Used to improve water solubility, rate of
dissolution, and hence, its bioavailability By forming a complex with drug molecule Lipophilic cavity – holds ITZ Hydrophobic exterior

Challenges for Sporanox®:
Excipient: 2-(HYDROXYPROPYL)-BETA-CYCLODEXTRIN
In the 1996, Horsky et al. From National Institute of Health (NIH)indicated that:
“HP-B-Cyclodextrin, when used in pharmaceutical formulations, haspotential to increase the absorption of carcinogens which enter theGI tract as food components or from air pollution.”
Note: The author cautions against the use of very large quantities ofthe substance, because if it can enhance BA of a therapeutic drug, itcan also provide the same service for harmful chemicals.

Challenges for Sporanox®:
SafetyFor oral, high doses (> 1000 mg/kg/day) : Diarrhea Enlargement of faeces seen only in animals
For IV, high doses nephrotoxicity in animal studies seen only in animals
At present, it is not required to add information on these excipients inthe package leaflet of medicinal products (European Union , 2015)
The presence of cyclodextrins should always be stated as a precaution because of limited information and possible interaction with
active substances.
Challenges for Sporanox®:
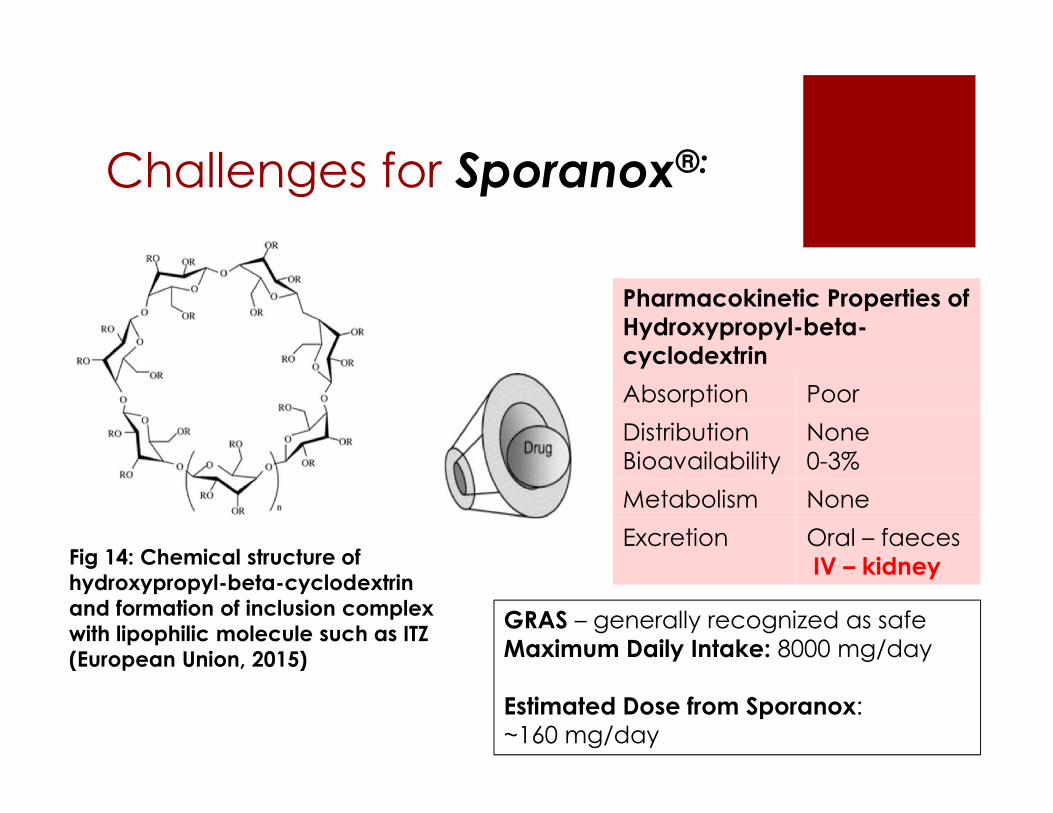
Fig 14: Chemical structure ofhydroxypropyl-beta-cyclodextrinand formation of inclusion complexwith lipophilic molecule such as ITZ(European Union, 2015)
Pharmacokinetic Properties ofHydroxypropyl-beta-cyclodextrinAbsorption PoorDistributionBioavailability
None0-3%
Metabolism NoneExcretion Oral – faeces
IV – kidney
GRAS – generally recognized as safeMaximum Daily Intake: 8000 mg/day
Estimated Dose from Sporanox:~160 mg/day

Improving its Bioavailability
Nanosizing - to reduce the particle size of the ITZ tosub-micron range, typically between 100-200nm, toenhance its oral bioavailability.
Mechanism: Maximizing surface area to improve itsdissolution rate, which in turn, enhances itsbioavailability.
Require the use of stabilizers (e.g. polymers)
Examples:
1. High Pressure Homogeneous
2. Supercritical Fluid Process

Improving its Bioavailability
Fig. 15: Scanning electronmicroscopy micrographsof coarse itraconazolepowders (top) andlyophilized intraconazolenanocrystals byhomogenized highpressure. (Sun, et al. (2011)

Nanosizing ITZ
Figure 16: By nanosizing ITZ with silica into flakes, it is going to increase the rate ofdissolution of ITZ in the stomach, thus increasing absorption rate in the intestine

Challenges for Sporanox®:
Challenge 2: Potential Drug to Drug Interactionswith Anti-neoplastic Drugs
AntineoplasticDrugs
Coadministrationwith Sporanox
Clinical Comments
irinotecan CONTRAINDICATED: The potential increase in plasma concentrations of irinotecanwhen coadministered with SPORANOX® may increase the risk of potentially fatal adverseevents.
axitinibdabrafenibdasatinibibrutinibnilotinibsunitinibtrabectedin
May increase plasmalevels of these drugs
NOT RECOMMENDED: It is recommended that the use of these drugs be avoidedduring and up to 2 weeks after discontinuation of treatment with itraconazole, unless thebenefits outweigh the potentially increased risks of side effects. If coadministration cannotbe avoided, clinical monitoring for signs or symptoms of increased or prolonged effects orside effects of the interacting drug is recommended, and its dosage be reduced orinterrupted as deemed necessary. When appropriate, it is recommended that plasmaconcentrations be measured.
bortezomib busulphandocetaxelerlotinibgefitinibimatinibixabepilonelapatinibponatanib trimetrexatevinca alkaloids
May increase plasmalevels of these drugs
USE WITH CAUTION: Careful monitoring is recommended when these drugs arecoadministered with itraconazole. Upon coadministration, it is recommended that patientsbe monitored closely for signs or symptoms of increased or prolonged effects or sideeffects of the interacting drug, and its dosage be reduced as deemed necessary. Whenappropriate, it is recommended that plasma concentrations be measured. See 3 above forfurther information.
Challenges for Sporanox®:
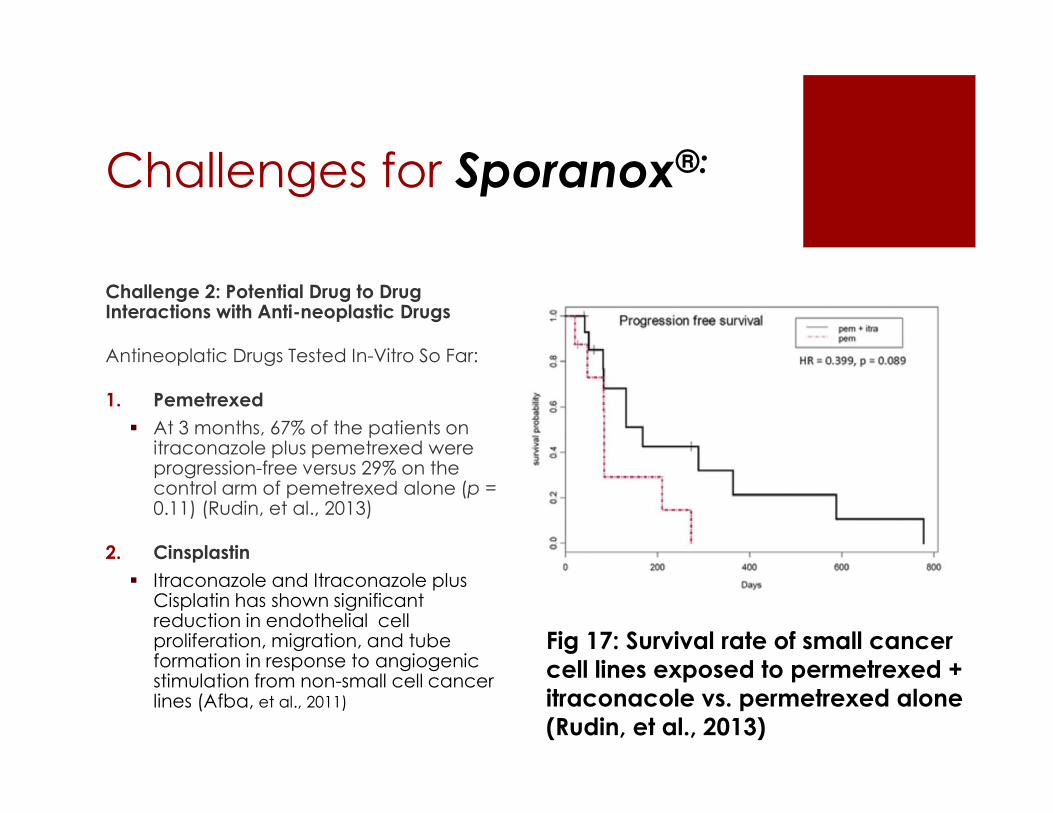
Challenge 2: Potential Drug to DrugInteractions with Anti-neoplastic Drugs
Antineoplatic Drugs Tested In-Vitro So Far:
1. Pemetrexed At 3 months, 67% of the patients on
itraconazole plus pemetrexed wereprogression-free versus 29% on thecontrol arm of pemetrexed alone (p =0.11) (Rudin, et al., 2013)
2. Cinsplastin Itraconazole and Itraconazole plus
Cisplatin has shown significantreduction in endothelial cellproliferation, migration, and tubeformation in response to angiogenicstimulation from non-small cell cancerlines (Afba, et al., 2011)
Fig 17: Survival rate of small cancercell lines exposed to permetrexed +itraconacole vs. permetrexed alone(Rudin, et al., 2013)

Conclusions ITZ should be further considered for its potential
anticancer effects Long record of safety. In-vitro and early phase clinical trials showcases
consistent anti-cancer effects. Oral capsules do not contain 2-(HYDROXYPROPYL)-BETA-
CYCLODEXTRIN, even if it is GRAS.
But must take into consideration: Limited applicability in clinical practice due to its wide
range of interactions with other drugs. Angiogenesis and Hedgehog signaling pathways are
not well understood – more research. Selecting a safe excipient or using biotechnology to
enhance its BA. How to incorporate this new drug into a chemotherapy
regime – Diarrhea is the common side effects.
References(2014). Background review for cyclodextrins used as excipients CPMP/463/00 Rev. 1 . European Medicines Agency.http://www.ema.europa.eu/docs/en_GB/document_library/Report/2014/12/WC500177936.pdf
Barone, J., Moskovitz, B., Guarnieri, B., Hassell, A., Colaizzi, J., Bierman, R., & Louis, J. (1998). Enhanced Bioavailability ofItraconazole in Hydroxypropylβ-Cyclodextrin Solution versus Capsules in Healthy Volunteers. American Society ofMicrobiology, 42 (7), 1862-1865.
Carducci, M. (2014). A Two-dose Level Clinical Trial of Itraconazole in Patients With Metastatic Prostate Cancer Who HaveHad Disease Progression While on Hormonal Therapy. National Institute of Health: Clinicaltrials.org. Identifier: NCT00887458.https://clinicaltrials.gov/ct2/show/results/NCT00887458?sect=X70156&term=sporanox&rank=27#outcome1
Diamond, R. (1999). Atlas of Fungal Infections. Introduction to Medical Mycology. Merck and Co.
Du, R., Lu, K. V., Petritsch, C., Liu, P., Ganss, R., Passegué, E., … Bergers, G. (2008). HIF1α Induces the Recruitment of BoneMarrow-Derived Vascular Modulatory Cells to Regulate Tumor Angiogenesis and Invasion. Cancer Cell, 13(3), 206–220.http://doi.org/10.1016/j.ccr.2008.01.034
Horsky, J., Pitha, J. (1996). Hydroxypropyl cyclodextrins: potential synergism with carcinogens. Journal of PharmaceuticalScience, 85(1), 96-100. http://www.ncbi.nlm.nih.gov/pubmed/8926593
McMillan, R., Matsui, W. (2012). Molecular Pathways: The Hedgehog Signaling Pathway in Cancer. American Associationfor Cancer Research, 18(18): 4883–4888. http://clincancerres.aacrjournals.org/content/18/18/4883.full.pdf+html

References (Cont’d)Nanonization of Itraconazole by High Pressure Homogenization: Stabilizer Optimization Podust LM, von Kries JP, EddineAN, Kim Y et al. "Small-Molecule Scaffolds for CYP51 Inhibitors Identified by High-Throughput Screening and Defined by X-ray Crystallography." Antimicrob Agents Chemother. 2007, 51(11): 3915-23.
Pantziarka, P., Sukhatme, V., Bouche, G., Meheus, L., & Sukhatme, V. P. (2015). Repurposing Drugs in Oncology (ReDO)—itraconazole as an anti-cancer agent. Ecancermedicalscience, 9, 521. http://doi.org/10.3332/ecancer.2015.521
Product Monograph: PrSPORANOX® itraconazoleoral solution 10 mg/mL Antifungal Agent. (2015). Janssen Inc.Extracted from Health Canada Drug Directorate. DIN number: 02047454.
Product Monograph: PrSPORANOX® itraconazolecapsules 100 mg Antifungal Agent. (2015). Janssen Inc. Extracted fromHealth Canada Drug Directorate. DIN number: 02231347.
Rudin, Charles M. et al. (2013). Phase 2 Study of Pemetrexed and Itraconazole as Second-Line Therapy for MetastaticNonsquamous Non–Small-Cell Lung Cancer. Journal of Thoracic Oncology , 8 (5) , 619 – 623http://www.jto.org/article/S1556-0864(15)32820-3/abstract
Stella, V. J., He, Q. (2008). Cyclodextrins. Toxicologic Pathology. 36(1), 30-42.
http://tpx.sagepub.com/content/36/1/30.long
Sun, W., Mao, S., Shi, Y., Li, L., Fang., L. (2011). Journal of Pharmaceutical Sciences, 100 (8), 3365-3373.http://jpharmsci.org/article/S0022-3549(15)32030-X/pdf
Types of Fungal Diseases. (2014, December 04). Retrieved April 04, 2016, fromhttp://www.cdc.gov/fungal/diseases/index.html

Thank You