prostate biopsy 2018 - profdjavan.com biopsy 2018... · prostate biopsy in 2017 bob djavan, md, phd...
TRANSCRIPT
Prostate Biopsy in 2017
Bob Djavan, MD, PhD
Professor and Chairman, Department of Urology,
Rudolfinerhaus Foundation Hospital,Vienna, Austria Director Vienna Urology foundation
Board member Scientific Committee of the EAU and executive Board ESOU

Prostate Cancer 2017
▪ Over 1 million TRUS biopsies ! Most unnecessary
▪ PSA Screening: 20% reduction mortality ▪ Most men do not benefit from aggressive
treatment ▪ Identify the high risk (treat) & avoid
detection of low grade ▪ Push MR Imaging
EAU and AUA
• Adequate Detection of clinically significant prostate cancers (sensitivity) and if Index Cancers • Accuracy of negative sampling (negative predictive value) • Limited Detection of clinically insignificant cancers and, • Good Concordance with whole gland surgical pathology results to allow accurate risk stratification and • Aiding 3D Disease localization for (focal) treatment selection
Optimal prostate biopsy 2017
Djavan & Rocco, BMJ, 344:8201, 2011

Khauli 2015
FDA currently approved biomarkers for screening
▪ PSA ▪ PCA3 ▪ p2PSA ▪ PHI score (Derived from a combination of tPSA, fPSA, p2PSA)
1. More is better!
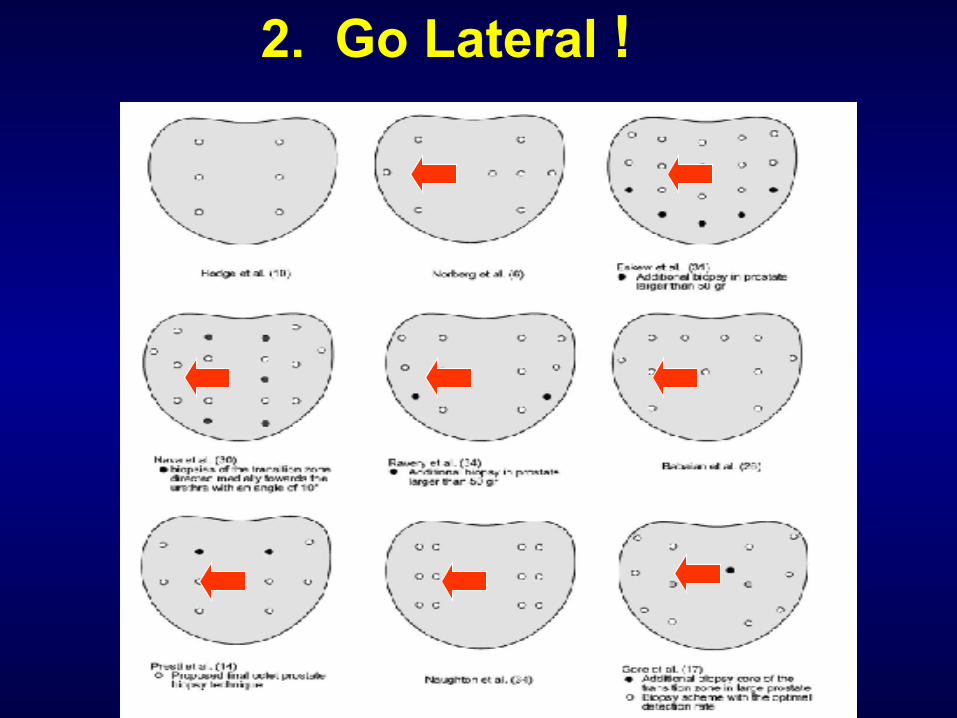
2. Go Lateral !

De La Taille Study
• 303 men with different indications for biopsy • 6 cores 22,7% • + 6 lateral cores 28.3% • + 6 TZ cores 30.7% • + 3 mid-line cores 31.3%
De la Taille et al. Urology, 61: 1181-86, 2003
+12%

Saturation Technique (24 cores) Does Not Improve Cancer Detection as an Initial Prostate Biopsy
Strategy
Men with PSA 2.5 to 9.9 ng/dl: cancer in 53 of 122 (43.4%) saturation biopsies
and 26 of 58 (44.8%) 10-core biopsies
Jones et al., J Urol ,February 2006
Jones Study

Chan et al, J Urol, 2181-84, 2001
and !...
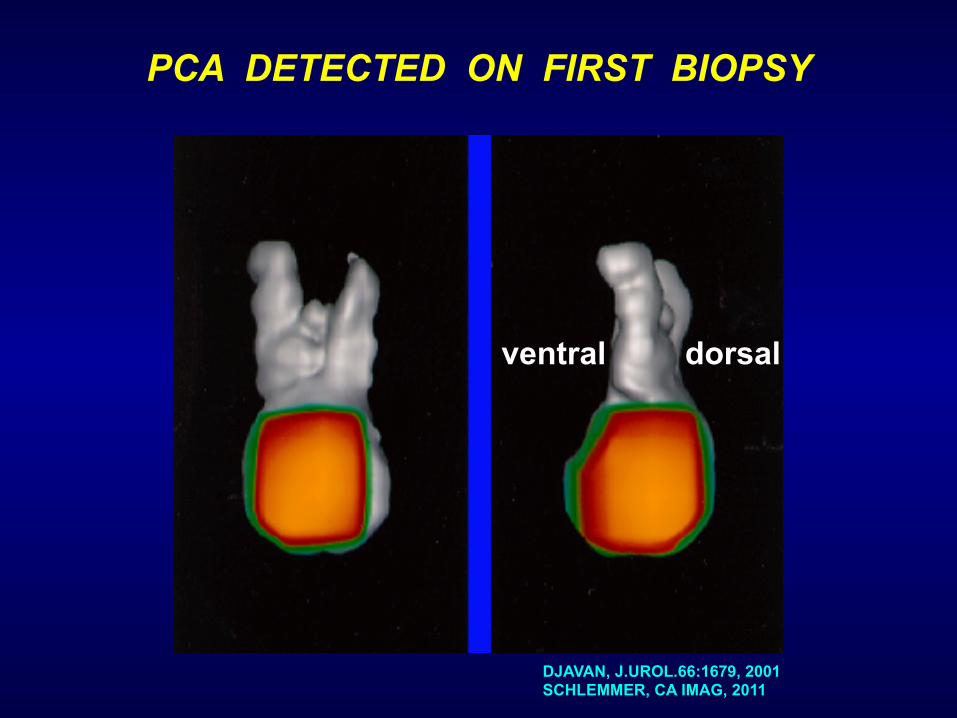
PCA DETECTED ON FIRST BIOPSY
dorsalventral
DJAVAN, J.UROL.66:1679, 2001 SCHLEMMER, CA IMAG, 2011
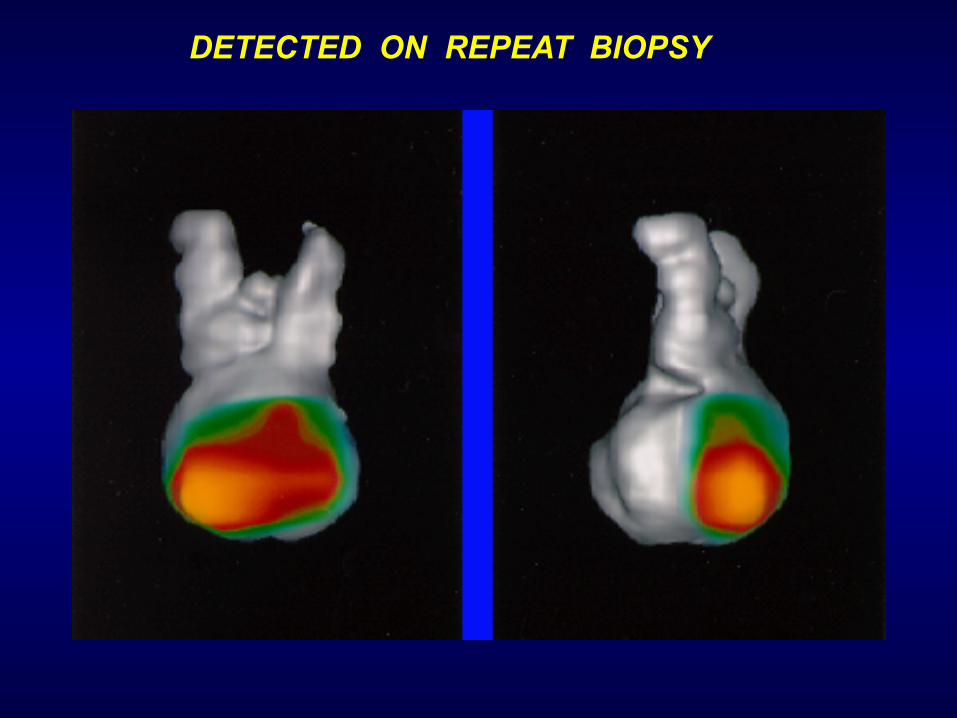
DETECTED ON REPEAT BIOPSY

WHERE DOES TRUS BIOPSY STAND IN 2017 ?
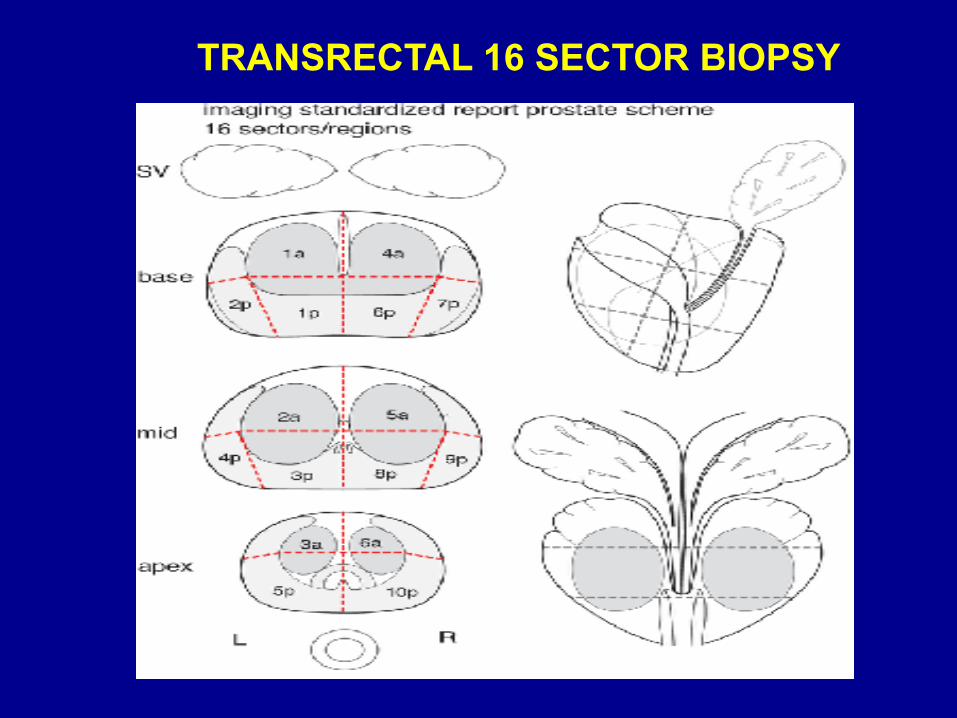
TRANSRECTAL 16 SECTOR BIOPSY
14
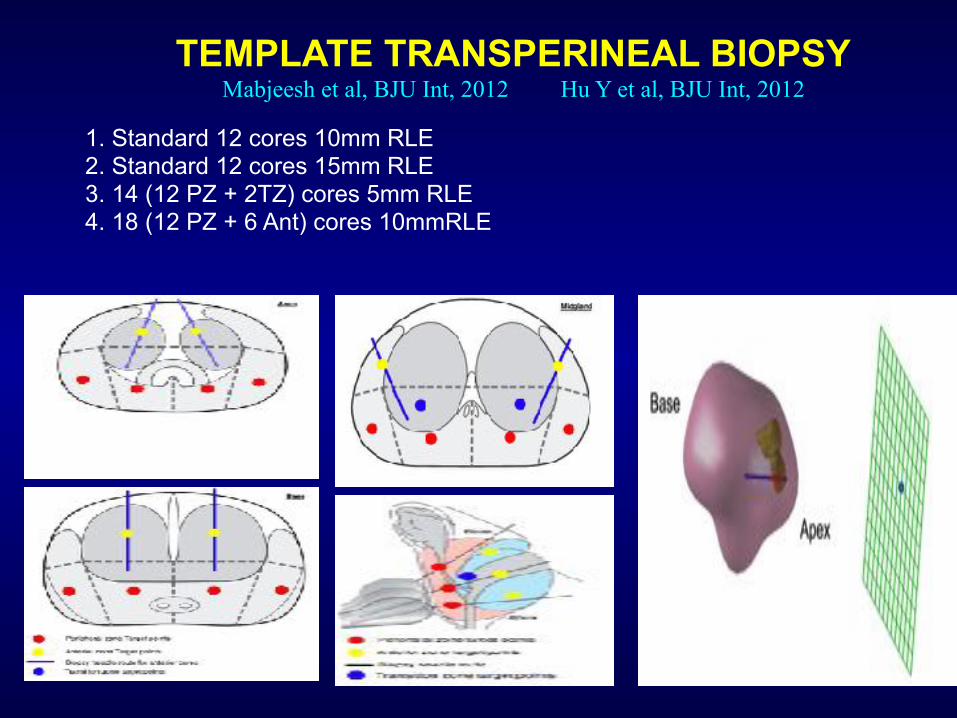
TEMPLATE TRANSPERINEAL BIOPSY Mabjeesh et al, BJU Int, 2012 Hu Y et al, BJU Int, 2012
1. Standard 12 cores 10mm RLE 2. Standard 12 cores 15mm RLE 3. 14 (12 PZ + 2TZ) cores 5mm RLE 4. 18 (12 PZ + 6 Ant) cores 10mmRLE


16
Accuracy of TRUS biopsy for PCa >/=0.5cc
Lecornet et al. BAUS ONC 2010 Mabjeesh et al., BJU Int, 2012
bibliographic search using PubMed® covering the period up to July 2012 yielded approximately 550 articles!
- 10/12 core schemes better than traditional sextant
- If cores > 12, then the increase in diagnostic yield is only marginal
- Only limited evidence supports the use of more than 12 cores or saturation on initial Bx
- Apical and laterally directed sampling increases cancer detection rate
1986-2010
Find ANY Cancer !

2010-2016
Find SIGNIFICANT Cancer

2017 ?
Find SIGNIFICANT Cancer &
Provide a cancer Grade Map
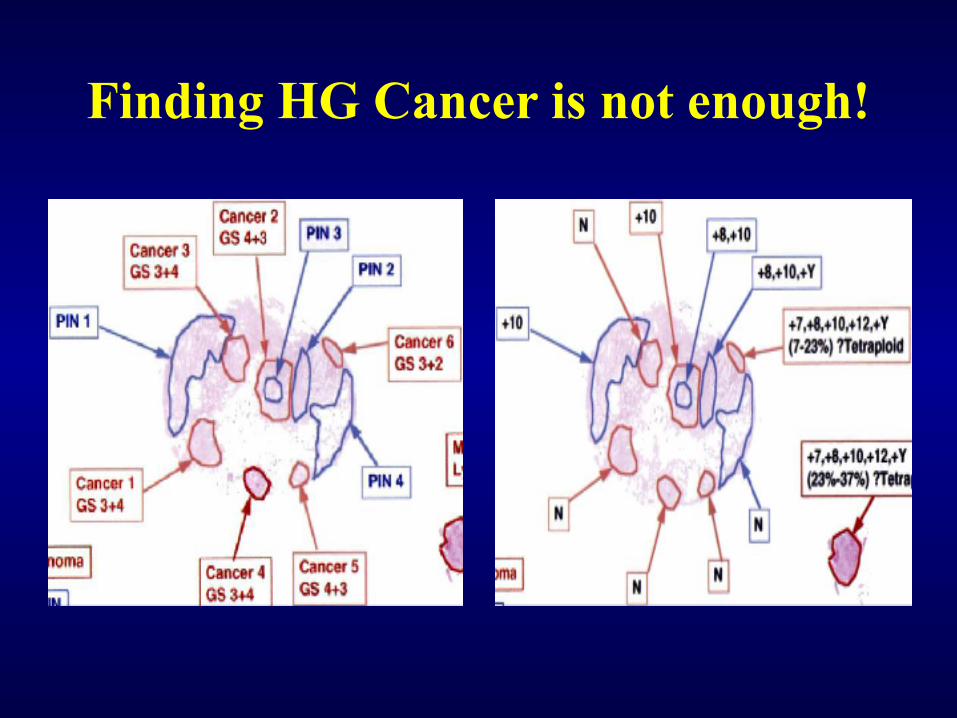
Finding HG Cancer is not enough!

How reliable are Standard TRUS prostate biopsies?
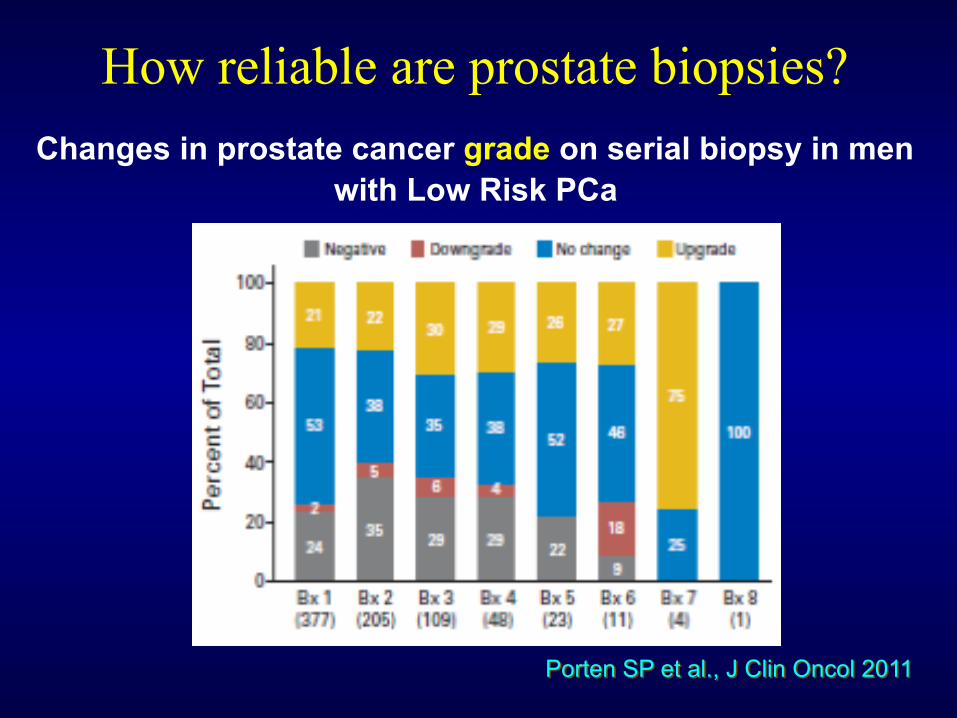
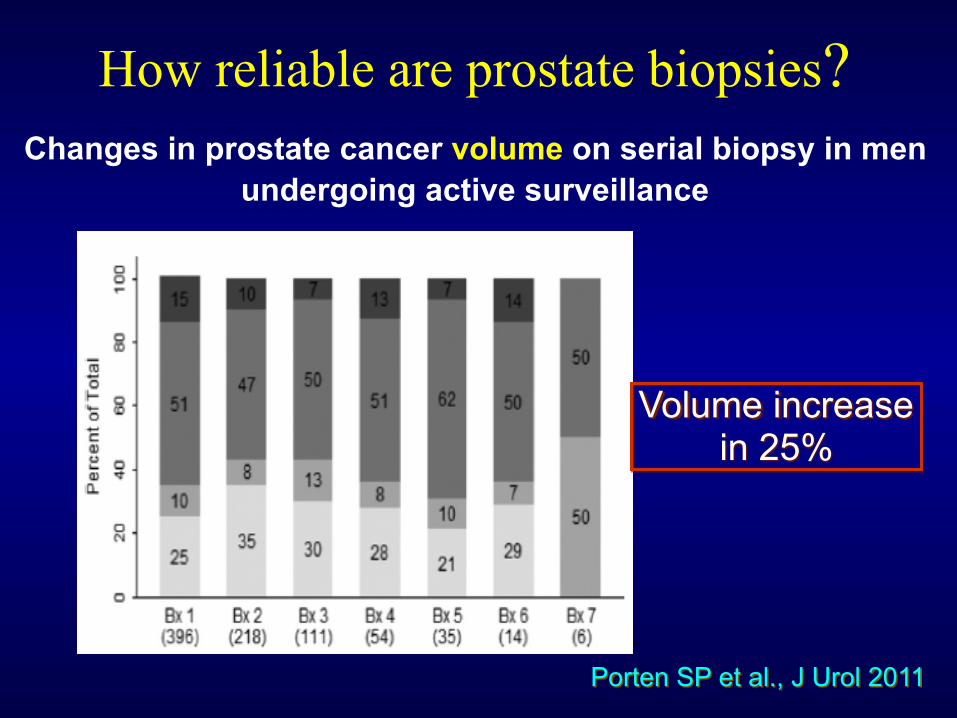
How reliable are prostate biopsies?
Porten SP et al., J Clin Oncol 2011
Changes in prostate cancer grade on serial biopsy in men with Low Risk PCa
How reliable are prostate biopsies?
Porten SP et al., J Urol 2011
Changes in prostate cancer volume on serial biopsy in men undergoing active surveillance
Volume increase in 25%
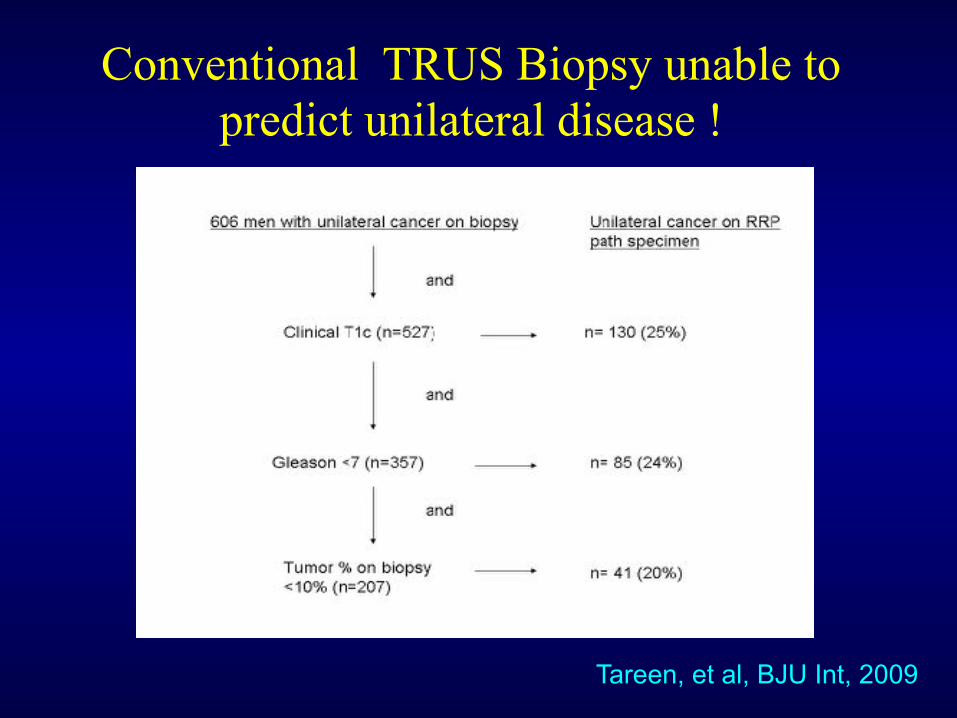
Conventional TRUS Biopsy unable to predict unilateral disease !
Tareen, et al, BJU Int, 2009
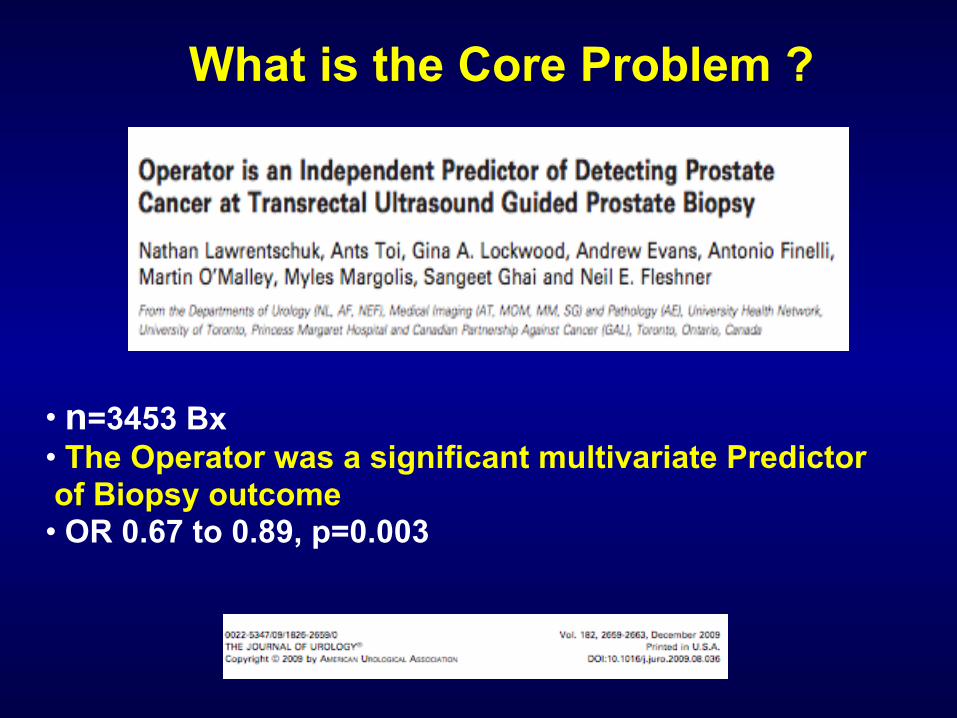
What is the Core Problem ?
• n=3453 Bx • The Operator was a significant multivariate Predictor of Biopsy outcome • OR 0.67 to 0.89, p=0.003
Multiparametric MRI
mpMRI: T2 + at least two functional (DWI / DCE / MRSI)
Barentsz JO, Richenberg J, Clements R, Choyke P, Verma S, Villeirs G, et al. ESUR prostate MR guidelines 2012. Eur Radiol 2012; 22(4):746–757
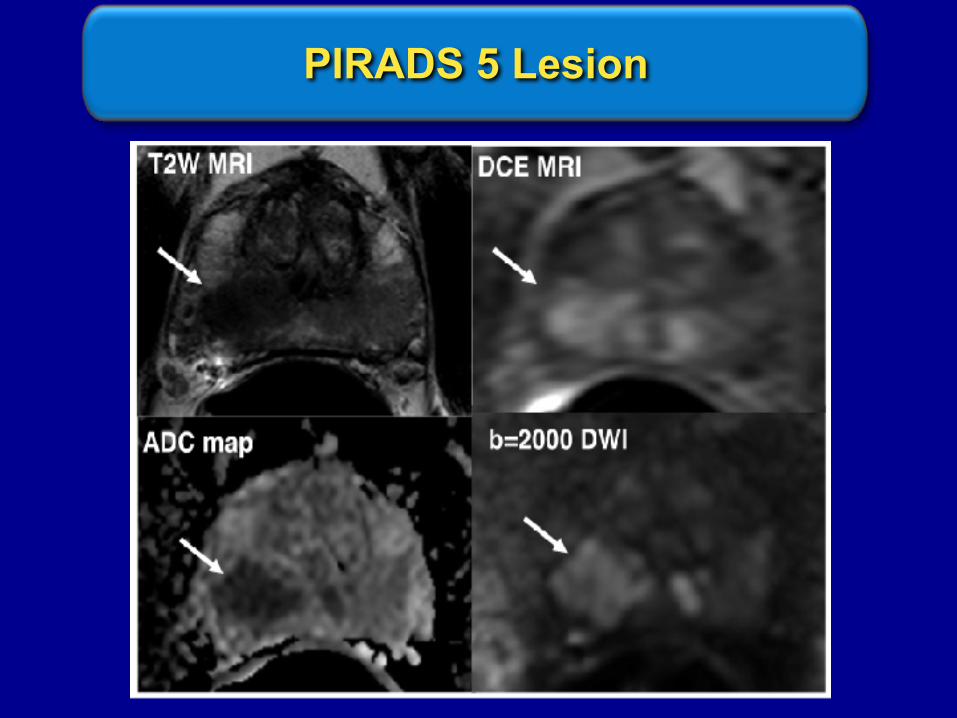
PIRADS 5 Lesion
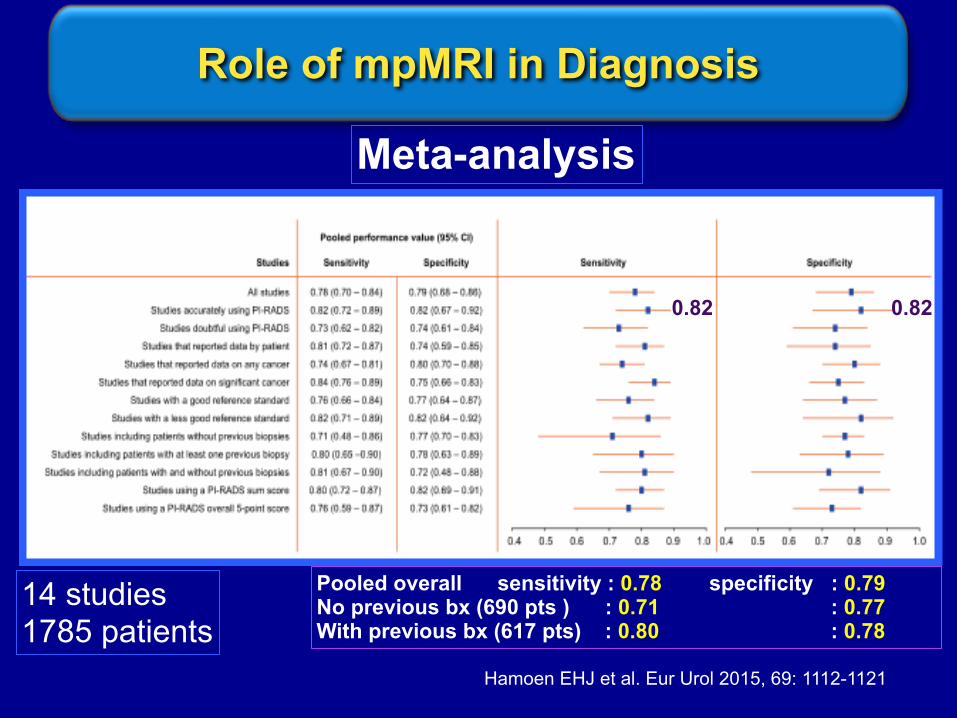
Pooled overall sensitivity : 0.78 specificity : 0.79 No previous bx (690 pts ) : 0.71 : 0.77 With previous bx (617 pts) : 0.80 : 0.78
Role of mpMRI in Diagnosis
Hamoen EHJ et al. Eur Urol 2015, 69: 1112-1121
14 studies 1785 patients
0.82 0.82
Meta-analysis
Fusion biopsy• MR-US fusion allows the information from MRI to be used to direct biopsy needles under TRUS guidance
• 2 Types: - Cognitive Fusion - Device Fusion
Sonn GA, Margolis DJ, Marks LS. Target detection: Magnetic resonance imaging-ultrasound fusion-guided prostate biopsy. Urol Oncol 2013;13:1–9.
CM, Kasivisvanathan V, Eggener S, et al. Standards of reporting for MRI-targeted biopsy studies (START) of the prostate: Recommendations from an international working group. Eur Urol 2013; 64:544–52.

31
Number of devices
No. of devices Devices
Koelis Trinity 1 Console including US
Ascendus 2 Console including US device + magnetic tracker
BiopSee 2 Console including US + holding arm including stepper and grid
Biojet 3 Console + US device + holding arm including stepper and grid
Artemis 2 Console including semi-robotic arm, stepper and grid + US device
IS robot (Biobot) 3 Console + US device + robotic unit
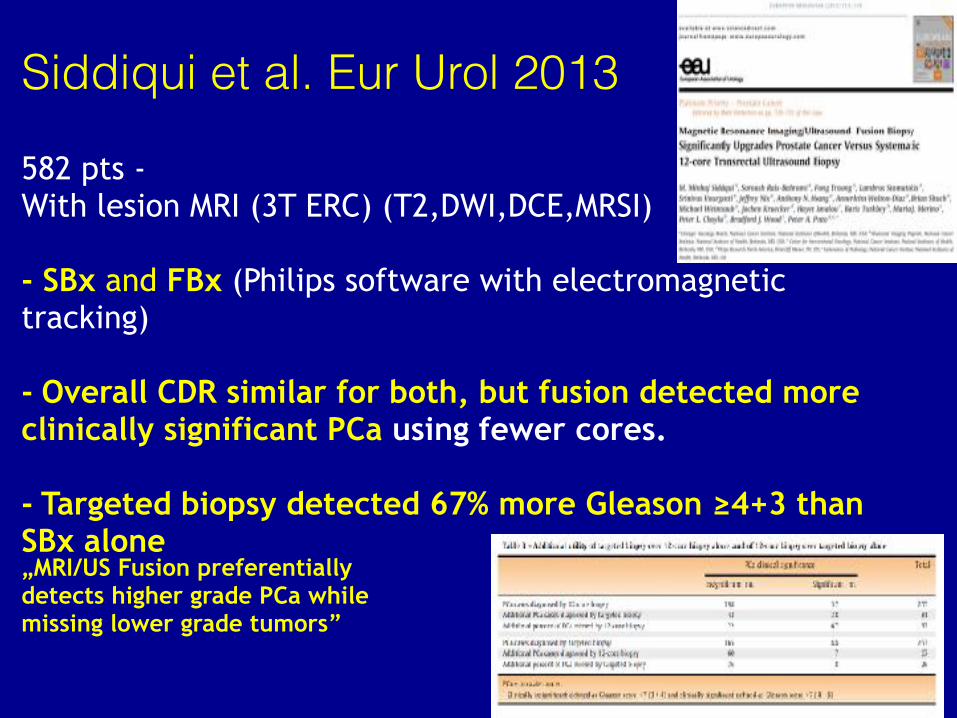
Siddiqui et al. Eur Urol 2013
582 pts - With lesion MRI (3T ERC) (T2,DWI,DCE,MRSI)
- SBx and FBx (Philips software with electromagnetic tracking)
- Overall CDR similar for both, but fusion detected more clinically significant PCa using fewer cores.
- Targeted biopsy detected 67% more Gleason ≥4+3 than SBx alone „MRI/US Fusion preferentially detects higher grade PCa while missing lower grade tumors”

BUT…
Does mp MRI solves the problem?

How Negative is a Negative mpMRI?
•Retrospective study of 101 RPE spec. with – mpMRI •68% T1c, mPSA 7.5ng/mL •11% had pT3a & 6%pT3b •2% had pN1 •13% had primary GG 4 •50% had secondary GG 4 or 5 •BUT with Expert Reading: No pT3, less primary GG 4 C: Negative mpMRI does NOT exclude significant PCa Need quality assurance
Branger, Eur Urol, 2016, A 501
• Prostate Health Index (PHI) • Repeat BX setting, N=168 • If mp MRI neg: 47% had cancer and 34% were GS >7 • At cut off >35, PHI predicted 86% of cancers if mpMRI was negative • Sens 86%, Spec 48% and NPV 80% • For GS>7: Sens 100%, Spec 48%, NPV 100%
Gnanapragasam, Eur Urol, 2016, A384
How Negative is a Negative mpMRI?
Where do we still need TRUS Bx?
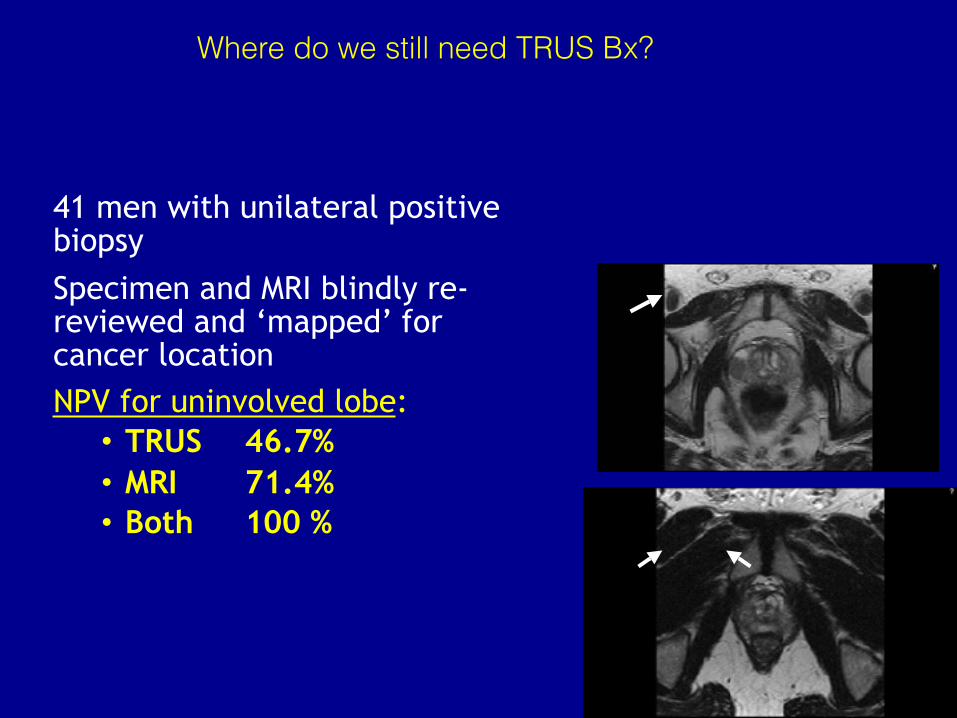
41 men with unilateral positive biopsy Specimen and MRI blindly re-reviewed and ‘mapped’ for cancer location NPV for uninvolved lobe:
• TRUS 46.7% • MRI 71.4% • Both 100 %
Do we need additional SysPBx with Fusion PBx?
•CDR was 40% for Fus-PBX (75% GS >7) •CDR 32% for Sys-PBX (69% GS>7) •15% of GS>7 detected by Sys PBx ALONE! •In MVA, max PI-RADs is the strongest predictor of GS>7 in Com-PBx !! •To detect High risk PCA, combine Fus-PBX with Sys-PBx
Borkowetz et al., Eur Urol, 2016, A503
Do we need additional SysPBx with Fusion PBx?
• Both Techniques miss apical lesions
• MR-Bx most often missed cancers in the dorsolateral part (58%)
• TRUS-Bx missed cancer in the anterior part (79%)
• We still need both targeted and systemic TRUS Bx
Schoutten et al., Eur Urol, 2016
Presentation Title Goes Here
AUA Consensus mp MRI and Biopsy
2017
use mp MRI in combination with sys TRUS biopsy…
39

use 18 G needle with a minimum 17 mm core length
improve grey scale TRUS capabilities
adequate sampling (16 sector biopsy)
correlate number of cores to volume
target pararectal, anterior and apical zones separately
How to get the best out of TRUS biopsy ?

mp MRI will increase cancer detection of HG prostete cancer
mpMRI: Less Biopsies Overall
mp MRI Bx Misses GS 6 Prostate cancer
Need to combine TRUS + mpMRI
Why we still need TRUS Bx
Summary
• Our notion of low risk is going to change
• The pathway will become dominated by imaging
• Location and focality (cancer mapping) will become essential

The Rudolfinerhaus Foundation Hospital
First oRPE by Theodor Billroth In 1867