psychotropic medications and falls vitamin d for fall and ... · psychotropic medications and falls...
TRANSCRIPT
Psychotropic Medications and falls
Vitamin D for fall and fracture
prevention
Leon Flicker
Western Australian Centre for Health & Ageing CMR,
School of Medicine and Pharmacology, UWA.
Department of Geriatric Medicine Royal Perth Hospital
Key concepts in age related
change • Contributing factors
– Impaired physiological function possibly only
due to disease and drugs
– Lifestyle and inactivity
• Intrinsic and Extrinsic Factors
• Multiple aetiology and multiple pathology
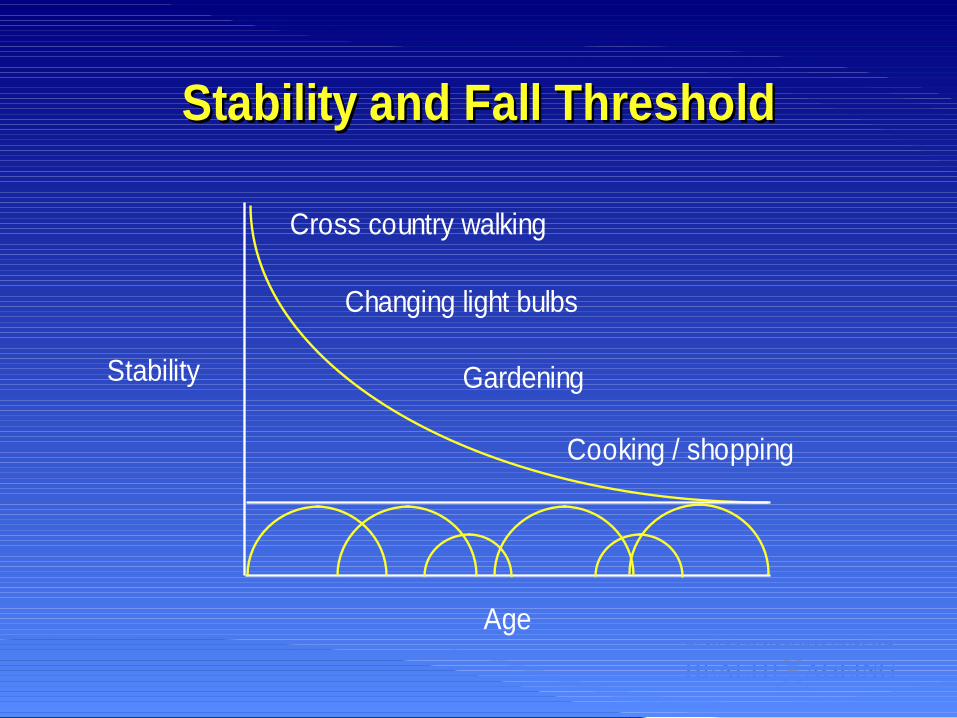
Stability and Fall ThresholdStability and Fall Threshold
Cross country walking
Changing light bulbs
Gardening
Cooking / shopping
Stability
Age
From being at risk to falling
• Not a linear relationship between
impaired function and disability
• Threshold effect: stability and daily
activities
• Instability is a key component of frailty
Risk factors RR/OR
•Medications associated with increased risk – ≥4 medications
– Psychotropic drugs (1.7)
– Includes SSRIs
– In women
– Class 1a antiarrhythmics (1.6)
•Why do these medications increase the risk
of falls?
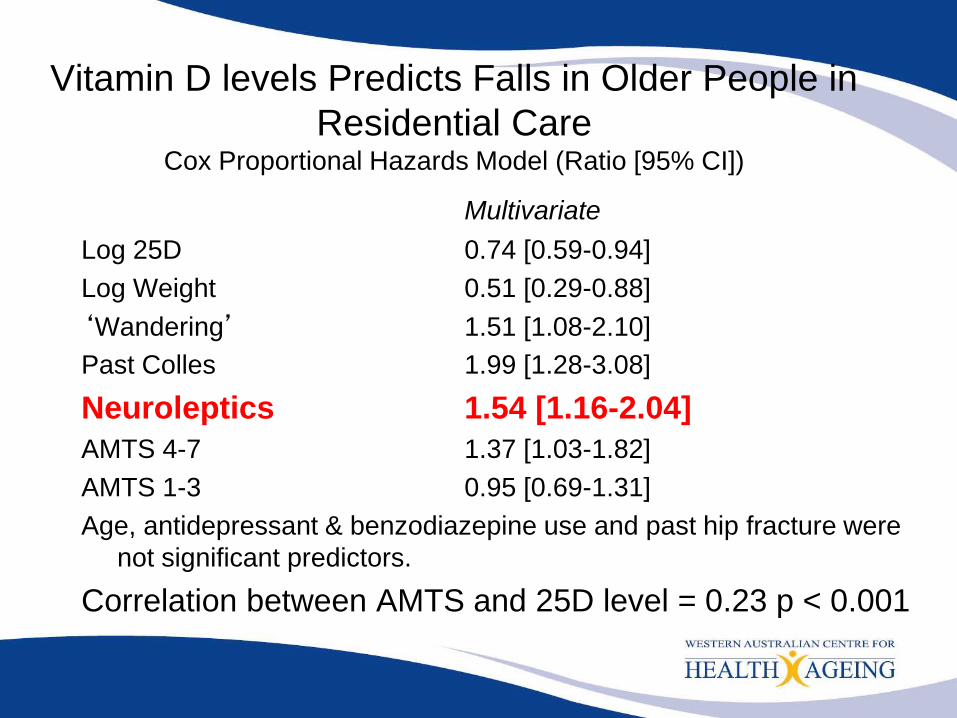
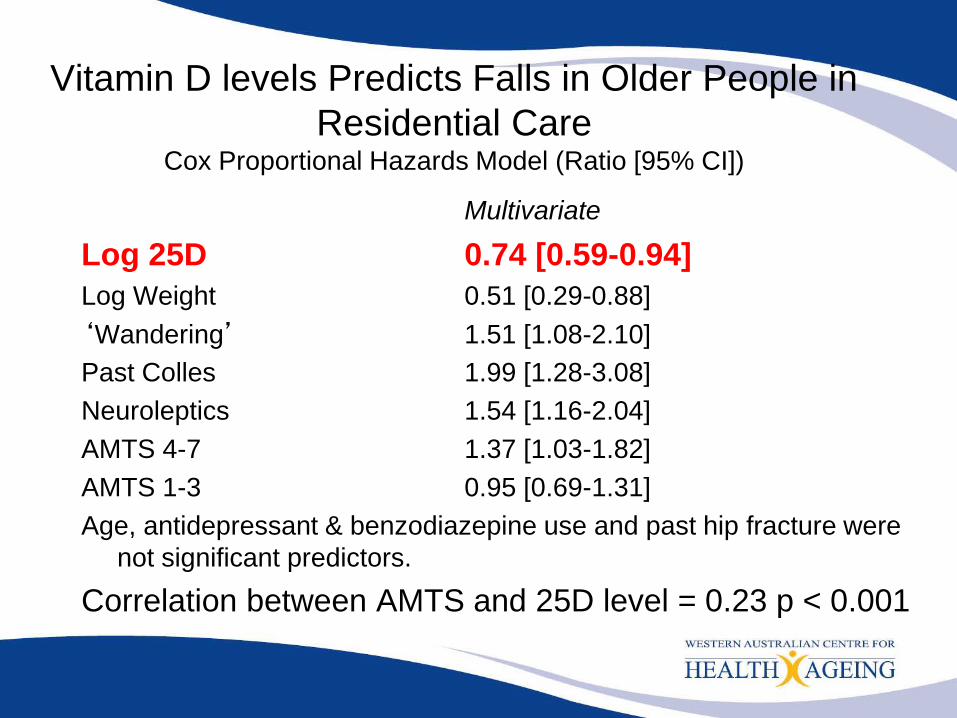
Vitamin D levels Predicts Falls in Older People in
Residential Care Cox Proportional Hazards Model (Ratio [95% CI])
Multivariate
Log 25D 0.74 [0.59-0.94]
Log Weight 0.51 [0.29-0.88]
‘Wandering’ 1.51 [1.08-2.10]
Past Colles 1.99 [1.28-3.08]
Neuroleptics 1.54 [1.16-2.04]
AMTS 4-7 1.37 [1.03-1.82]
AMTS 1-3 0.95 [0.69-1.31]
Age, antidepressant & benzodiazepine use and past hip fracture were
not significant predictors.
Correlation between AMTS and 25D level = 0.23 p < 0.001
2008
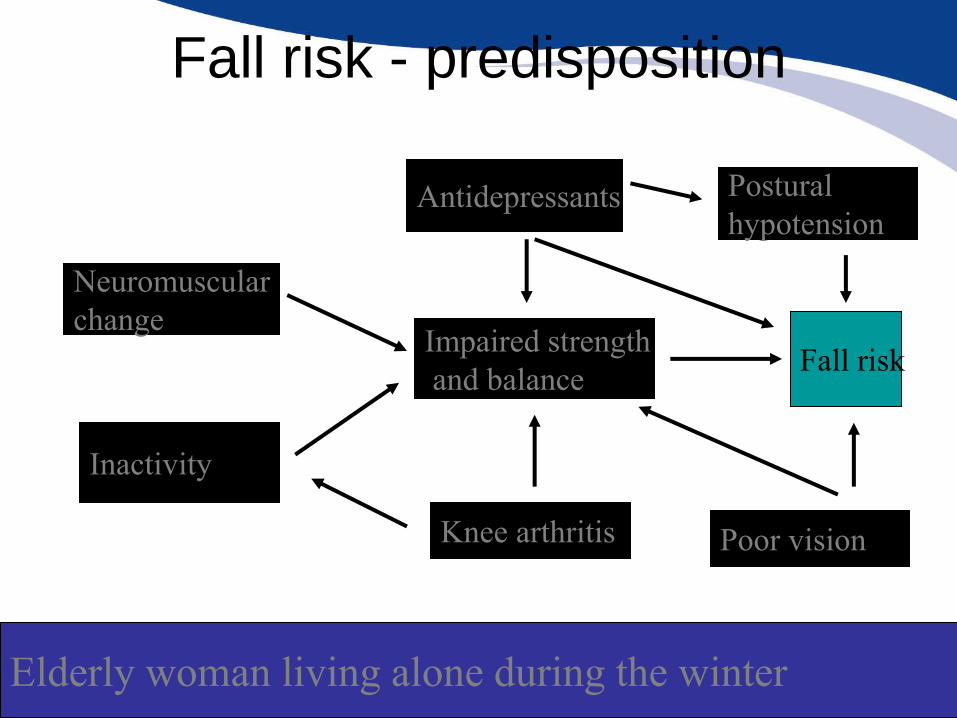
Fall risk - predisposition
Neuromuscular
change
Inactivity
Impaired strength
and balance Fall risk
Knee arthritis
Antidepressants Postural
hypotension
Poor vision
Elderly woman living alone during the winter
Fear and Gait performance
• Gait changes in old age are also an
adaptation to a range of factors
• Gait speed – predictor of falls and correlates with poor balance
– associated with
• decreased muscle strength
• fear of falling and “cautious gait” syndrome
• cardiorespiratory failure
Falls prevention - What works?
• Multidisciplinary assessment of high risk populations *
• Expedited cataract surgery *
• Strength and balance training in high risk populations *
• Group exercises with functional balance exercises *
• Withdrawal of centrally acting medications *
• Cardiovascular assessment and intervention of unexplained fallers *
• Comprehensive geriatric assessment in nursing homes
• Targeted interventions in hospitals
?? What works in RCFs and people with dementia *Community populations
Vitamin or Prehormone
• In most parts of the world the predominant
source of vitamin D3 is endogenous production
by the action of ultraviolet light on 7-dehydrochol
in the skin.
• Sunlight exposure cannot produce vitamin D
intoxication
• There is no biomarker that is more confounded
by general heath than circulating levels of
vitamin D as it represents general outdoor
activity
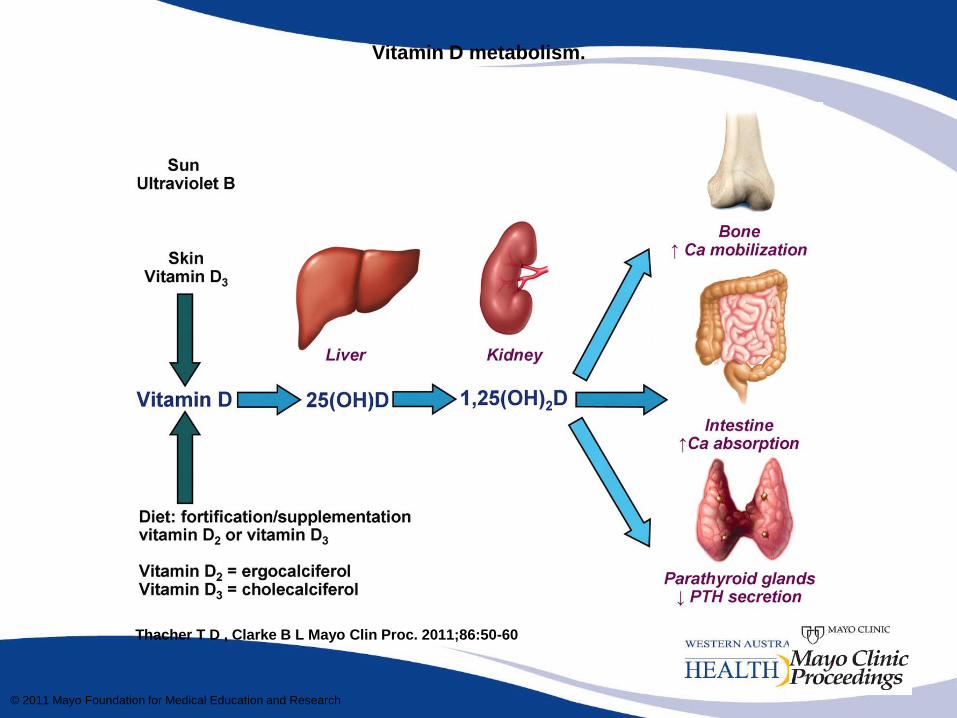
Vitamin D metabolism.
Thacher T D , Clarke B L Mayo Clin Proc. 2011;86:50-60
© 2011 Mayo Foundation for Medical Education and Research
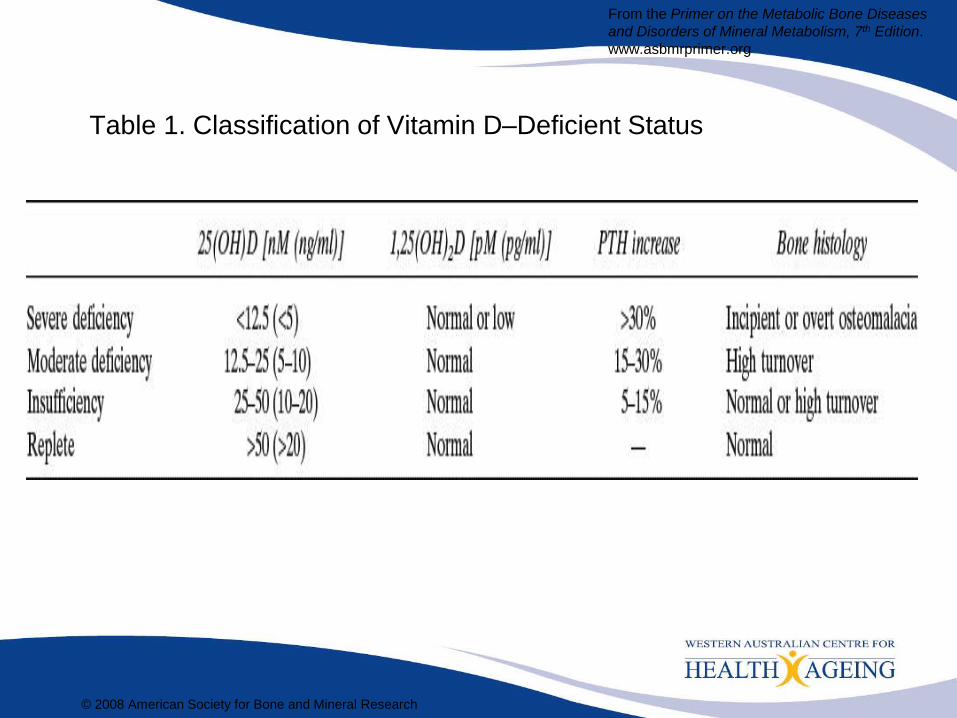
Table 1. Classification of Vitamin D–Deficient Status
© 2008 American Society for Bone and Mineral Research
From the Primer on the Metabolic Bone Diseases
and Disorders of Mineral Metabolism, 7th Edition.
www.asbmrprimer.org
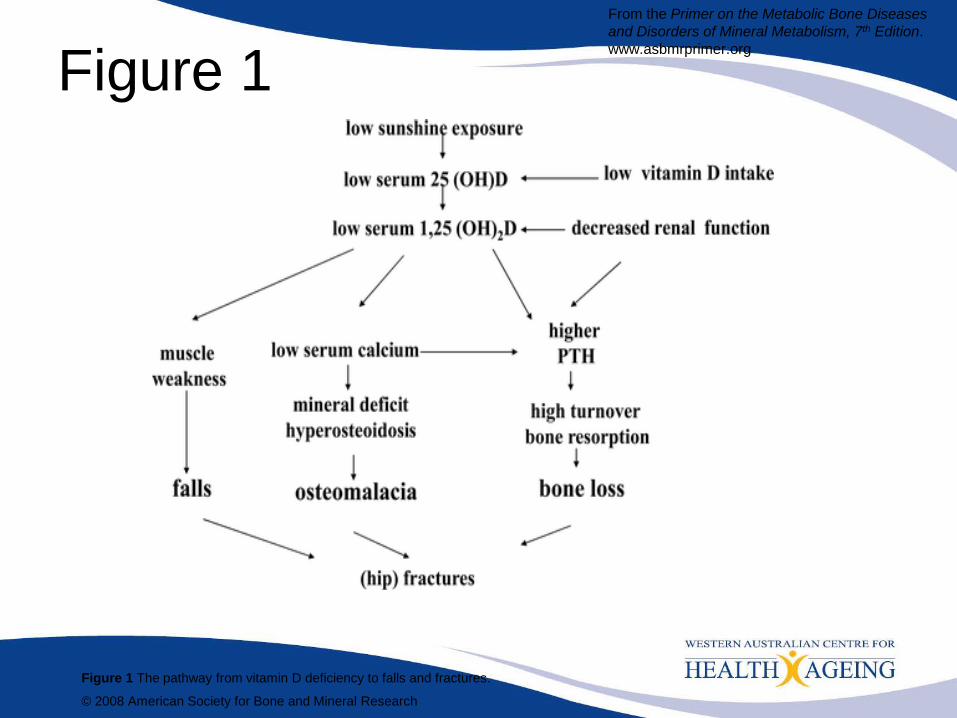
Figure 1
Figure 1 The pathway from vitamin D deficiency to falls and fractures. © 2008 American Society for Bone and Mineral Research
From the Primer on the Metabolic Bone Diseases
and Disorders of Mineral Metabolism, 7th Edition.
www.asbmrprimer.org


Vitamin D deficiency in older people
• Old people are more likely to have
relative vitamin D deficiency due to – Decreased production of D3 within the dermis
(MacLaughlin & Holick 1985),
– Inadequate exposure to sunlight (Reid et al. 1986),
and
– Decreased renal capacity for production of 1,25-
dihydroxyvitamin D (Tsai et al. 1984).
– Decrease in intestinal responsiveness to 1,25-
dihydroxyvitamin D occurring with age (Ebeling et
al. 1992), may potentiate the reduced availability of
1,25-dihydroxyvitamin D.
Vitamin D and Calcium to Prevent Hip Fractures in
Older Women The Best Evidence (Chapuy NEJM 1992)
3270 women - mean age 84
– Living in nursing homes and apartments for the elderly
– Treated group 1.2 g calcium and 800 IU of Vitamin D3
– Control group placebo
• Followed for 18 months
• In active group - 32% less non vertebral fractures
• 43% less hip fractures
• A subgroup of 142 women followed intensively
– mean PTH 6.0 to 3.3 pmol/l
– mean 25(OH) D 40 to 105 nmol/l (NR 38)
– Only a 1% difference in femoral neck BMD
• Community dwelling older people with
dementia have lower 25-hydroxyvitamin
(25-OHD) levels than age matched
controls (Kipen et al JAGS 1995;43:1088)
• Low concentration of 25-OHD have also
been associated with objective measures
of abnormal motor performance, proximal
muscle weakness, increased body sway
and impaired postural and dynamic
balance Glerup et al, Calc Tiss Int 2000;66:419; Pfeifer et al,
JBMR 2000;15:1113.; Dhesi et al JBMR 2002;17:891; Bischoff-
Ferrari et al, Arch Int Med 2006;166:424
Previous study of residential care in
Australia • The study spanned 3 states of
Australia - Victoria, NSW and
Western Australia.
• 60 hostels, 667 residents and
89 nursing homes, 953
residents participated in cohort
study for 6 months follow-up
• (JAGS 2003; 51:1533)
• Subsequently 625 subjects
participated in a RCT of
1000IU/day vitamin D
supplementation
• (JAGS 2005; 53:1881)
Vitamin D levels Predicts Falls in Older People in
Residential Care Cox Proportional Hazards Model (Ratio [95% CI])
Multivariate
Log 25D 0.74 [0.59-0.94]
Log Weight 0.51 [0.29-0.88]
‘Wandering’ 1.51 [1.08-2.10]
Past Colles 1.99 [1.28-3.08]
Neuroleptics 1.54 [1.16-2.04]
AMTS 4-7 1.37 [1.03-1.82]
AMTS 1-3 0.95 [0.69-1.31]
Age, antidepressant & benzodiazepine use and past hip fracture were
not significant predictors.
Correlation between AMTS and 25D level = 0.23 p < 0.001
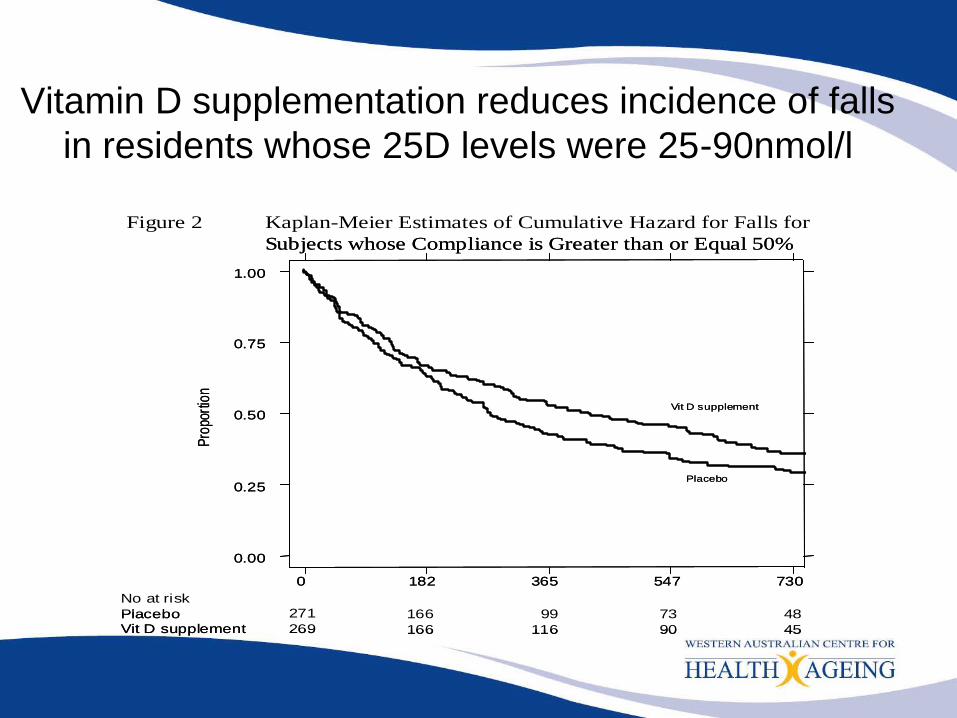
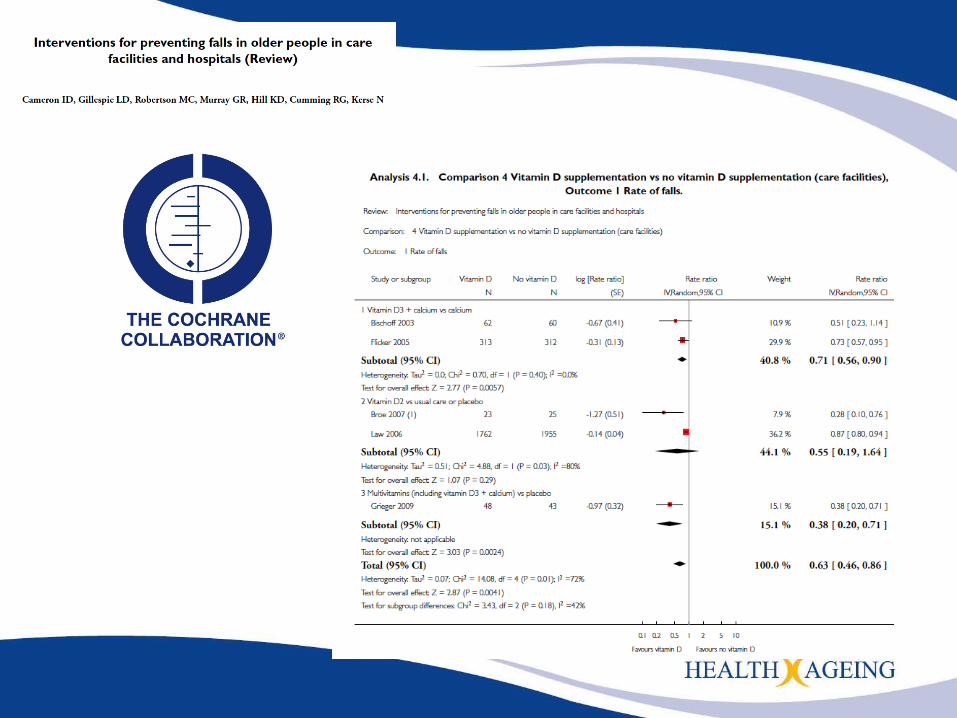
Vitamin D supplementation reduces incidence of falls
in residents whose 25D levels were 25-90nmol/l
0 182 365 547 730
0.00
0.25
0.50
0.75
1.00
Placebo
Vit D supplement
No at risk
Placebo
Vit D supplement
166
166
99
116
73
90
48
45
Pro
port
ion
271
269
Kaplan-Meier Estimates of Cumulative Hazard for Falls for
Subjects whose Compliance is Greater than or Equal 50%
Figure 2
0 182 365 547 730
0.00
0.25
0.50
0.75
1.00
Placebo
Vit D supplement
No at risk
Placebo
Vit D supplement
166
166
99
116
73
90
48
45
Pro
port
ion
271
269
Kaplan-Meier Estimates of Cumulative Hazard for Falls for
Subjects whose Compliance is Greater than or Equal 50%
Figure 2