pulsatility is overrated acute decompensated heart...
TRANSCRIPT

6/14/2017
1
Pulsatility is overrated: Acute Decompensated
Heart Failure in the ICU
Carolina Dimsdale DNP, ACNP-BC, AACC
No Disclosures
I have no current affiliation or financial
arrangement with any grantor or commercial interests that might have direct interest in the
subject matter of this CE Program.

6/14/2017
2
Objectives
1. Discuss clinical manifestations of acutely
decompensated heart failure.2. Describe management strategies including
medical and surgical options for therapy.
3. Review modern indications and usage of mechanical circulatory support.
What’s Acute Heart Failure?
• Ejection Fraction
• Symptoms
• End Organ Functiono Liver function
o Kidney function
o Neurologic status
Low Cardiac Output
Hypotension
Oliguria
Classifications• Framingham Heart Study classification
• ACC AHA
• Forrester
• Killip
• NYHA Yancy et al, 2013

6/14/2017
3
Acute Heart Failure
Case Study• 59F with PMH of ICM, VT s/p ICD placement. EF known to be
35%, mild AI, moderate TR.
• Admitted to ED complaining of lethargy, swelling, nausea x 1 week. Says she has been compliant with her diuretic regime, no dietary indiscretions
• Today’s echo: EF 20%, severe RV dysfunction, severe TR
• Objectively: dyspneic, nauseous, significant JVD, extremetiesare cool but dry
She is admitted to the Cardiac ICU for medical management.
ICU AssessmentNeuro: sedation, pain management, deliriumRespiratory: ETT, FiO2 and vent requirementCardiac: MCS sounds, arrhythmias, pacing device, swanGI: enteral access, nutrition, Renal: foleys, dialysis accessHeme: bleeding, clotting, anticoagulationInfectious: antibiotics, immunosuppressionLines: central lines, dialysis, chest tubesImaging: chest x-ray, echo, ultrasound, EKG
6/14/2017
4
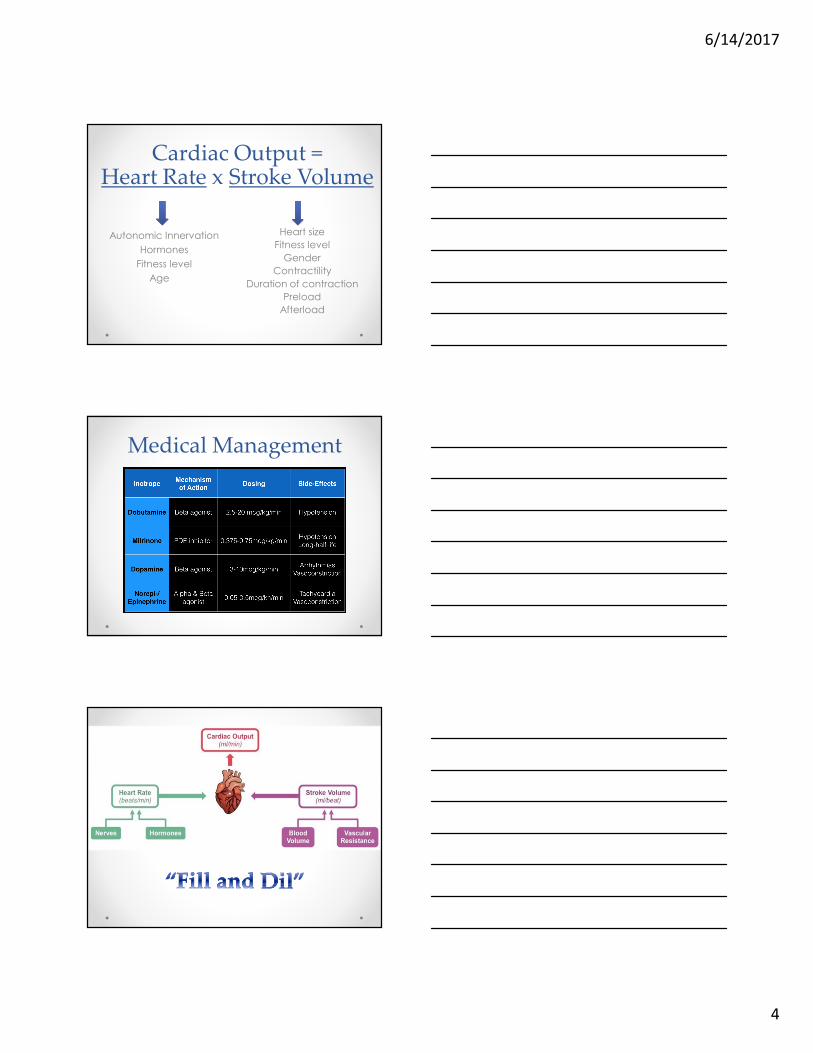
Cardiac Output =Heart Rate x Stroke Volume
Heart size
Fitness level
Gender
Contractility
Duration of contraction
Preload
Afterload
Autonomic Innervation
Hormones
Fitness level
Age
Medical Management

6/14/2017
5
Case StudyOur patient is being treated with Dopamine, Dobutamine, Lasix infusion. She was recently intubated for hypoxemia
r/t pulmonary edema. Epinephrine was added to support biVfunction.
Afternoon labs:
Lactate 6.2 (rising)
Creatinine 3.0
BUN 75
He soon experiences VT arrest refractory to antiarrhythmics.
VA ECMO is deployed.
Extracorporeal Membrane Oxygenation
• Indications:o refractory cardiac arrest
o refractory cardiogenic shock
• Contraindications:o Lack of neurological function
o Unrecoverable cardiac function
o Prolonged CPR without adequate tissue perfusion
Rescue, not a therapy
Gift of time
Decompression=recovery
Veno-Arterial (VA) ECMO• Cannulation Technique
o Open, surgical access (Cut down)
o Percutaneous (Seldinger)
o Surgical (open chest)
• Cannulation Strategieso Central (RA to Aorta)
o Peripheral (fem vein to descending aorta)
o Sites: Axillary, Femoral, Jugular
• Oxygenationo CO2 removal (sweep)
o Oxygenation 100% FiO2
Banfi et al., 2016

6/14/2017
6
Banfi et al, 2016
Percutaneous Femoral
Cannulation with Distal Perfusion
Catheter
Subclavian Artery Cannulation
Central Cannulation
ECMO Management• Preload dependent, afterload sensitive
• Anticoagulation: PTT goal 60-80
• Echocardiogram
• Modification of drug dosing
• Multidisciplinary
Complications
• Major bleeding (40.8%)
• Infection (30.4%)
• Stroke (6%)
• Neurologic complications (13.3%)
• Acute Kidney Injury (55.6%)
• Lower extremity ischemia (16.9%)
• End of Life Care
Cheng et al, 2014

6/14/2017
7
Case StudyOur patient’s end organ function improves on ECMO. On echo, the biventricular function is not improved.
The Heart Failure team deems her a candidate for durable LVAD.
She is taken to the OR for ECMO decannulation and VAD implantation.
Role of Echocardiography in the ICU
� volume status
� valvular abnormalities
� wall motion abnormalities
� rule out tamponade
� aids in weaning MCS/inotrope
image/video
Ventricular Assist Device
Temporaryo Bridge to recovery
o Bridge to durable device
Durableo Bridge to Transplant
o Destination
LEFT VENTRICLE
AORTA

6/14/2017
8
Aortic Valve Options
• Oversew
• Replace with bioprosthesis
Management Challenges
• Preload dependent
• Afterload sensitive
• Right ventricular support
• Optimize speed
• Preventing Thrombosis
• ICD settings
image

6/14/2017
9
Echocardiographic evidence of LVAD Suction Event
Griffin & Katz, 2014
LVAD Complications
BleedingStroke
ThrombosisHemolysis
Pump failureDriveline infection
RV Dysfunction

6/14/2017
10
Intraaortic Balloon Pump
1. Increases coronary perfusion2. Decreases afterload3. Augments cardiac output4. Modest increase in CI
ACSCardiogenic shock
Periop High Risk CABGBridge to transplant
IABP- SHOCK II Trial30 Day Mortality
Femoral Approach Subclavian Approach

6/14/2017
11
Total Artificial Heart (TAH)
Bridge to Survival
> 9 lpmTang, 2014
Copeland et al, 2004
Survival to Transplant
79%
Interagency Registry for Mechanically Assisted Circulatory Support
• > 15,000 patients from 158 hospitals
• patient survival
• adverse events
• cause of death over time
With current continuous-flow devices, survival at 1 and 2 years is 80% and 70% respectively
Kirklin, et al, 2015

6/14/2017
12
Heart Transplant• Indications
o End stage heart failure – ischemic heart disease and cardiomyopathy
o Congenital heart disease
• Absolute contraindicationso Recent malignancy
o Active infection
o Systemic disease which will affect life expectancy
o Significant pulmonary vascular resistance
3%
3%
35%
49%
3%
3%
3%1%
CHD
HCM
ICM
NICM
RCM
Retransplant
VCM
Other
2%2%
42%
46%2%
3%
4%0%
2016JHLT. 2016 Oct; 35(10): 1149-1205
Adult Heart TransplantsDiagnosis
0
10
20
30
40
50
60
2000 2001 2002 2003 2004 2005 2006 2007 2008 2009 2010 2011 2012 2013 2014
% o
f P
atie
nts
Year of Transplant
* LVAD, RVAD, TAH, ECMO
Adult Heart Transplants
% of Patients Bridged with Mechanical Circulatory Support*
2016JHLT. 2016 Oct; 35(10): 1149-1205
(Transplants: January 2000 – December 2014)

6/14/2017
13
2016JHLT. 2016 Oct; 35(10): 1149-1205
� Recipient age� Donor age
� Recipient creatinine� Ischemia time� Donor height� Recipient BSA
� Transplant center volume� Recipient total bilirubin
Risk Factors for 1 year Mortality
0
25
50
75
100
0 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22
Su
rviv
al (
%)
Years
1982-1991 (N=21,391)
1992-2001 (N=39,913)
2002-2008 (N=24,485)
2009-6/2014 (N=20,577)
Adult Heart TransplantsKaplan-Meier Survival by Era
2016JHLT. 2016 Oct; 35(10): 1149-1205
Median survival (years):1982-1991=8.5; 1992-2001=10.4; 2002-2008=11.9; 2009-6/2014=NA
All pair-wise comparisons were significant at p < 0.05.
(Transplants: January 1982 – June 2014)
New: Portable, warm perfusion and
monitoring system
Old: Cold Storage Heart
Preservation
� Increase transplantation
volume� Improve patient
outcomes� Reduce cost of
patient care
Transmedics.com
“Heart in a Box”

6/14/2017
14
Acute Heart Failure Prevention
• Same Day Access Clinics (SDAC)
• Implantable wireless hemodynamic monitoring� CHAMPION and IN-TIME trials
• Implantable intrathoracic impedence monitoring
ACC Expert Consensus Decision Pathways Task Force, 2017