qis: where regulation meets quality - ohca - ohio health ... · qis: where regulation meets quality...
TRANSCRIPT

4/28/2014
1
QIS: Where Regulation Meets Quality
Kenneth DailyElder Care Systems Group
2014 OHCA
Annual Convention
Quality Care or Compliance?
CMS Approach to Change
Value
5 Star Rating
SurveyStaffing
QMs
QAPIData
LeadershipProcess
Culture Change
SatisfactionEnvironment
MDS 3.0
InterviewsRelevant
data
Fiscal Policy
VBPBundling
Hospitalizations
4/28/2014
2
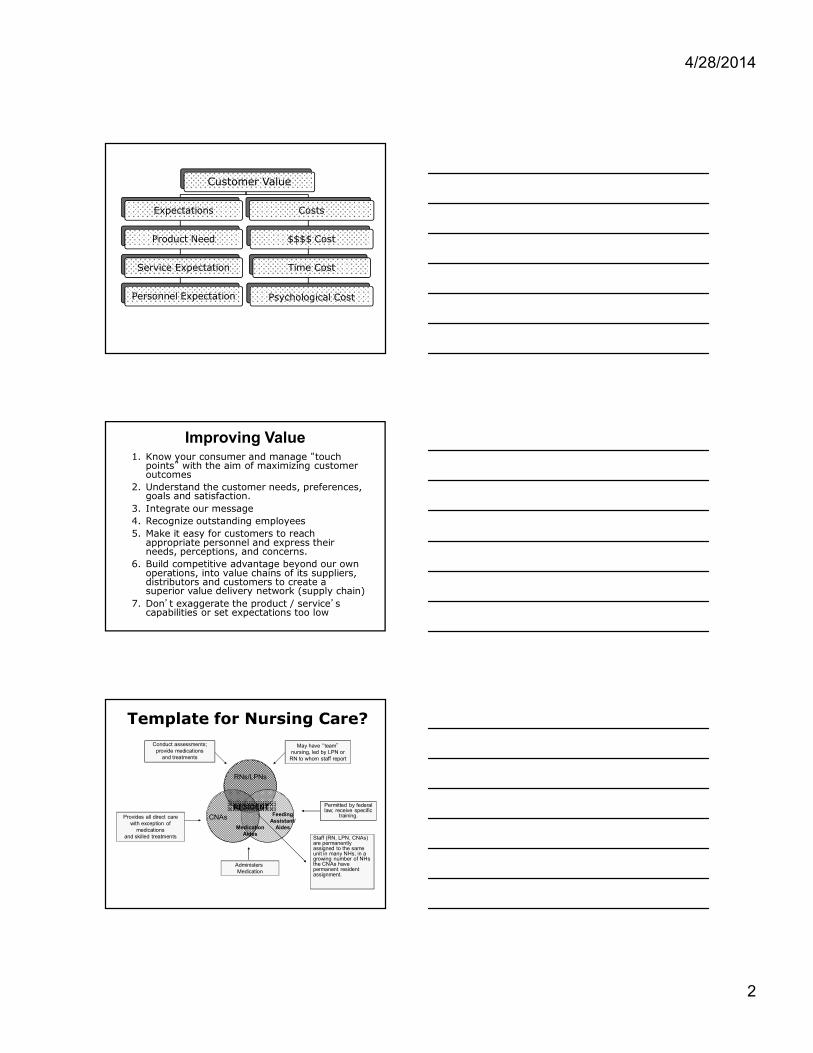
Customer Value
Expectations
Product Need
Service Expectation
Personnel Expectation
Costs
$$$$ Cost
Time Cost
Psychological Cost
Improving Value1. Know your consumer and manage “touch
points” with the aim of maximizing customer outcomes
2. Understand the customer needs, preferences, goals and satisfaction.
3. Integrate our message
4. Recognize outstanding employees
5. Make it easy for customers to reach appropriate personnel and express their needs, perceptions, and concerns.
6. Build competitive advantage beyond our own operations, into value chains of its suppliers, distributors and customers to create a superior value delivery network (supply chain)
7. Don’t exaggerate the product / service’s capabilities or set expectations too low
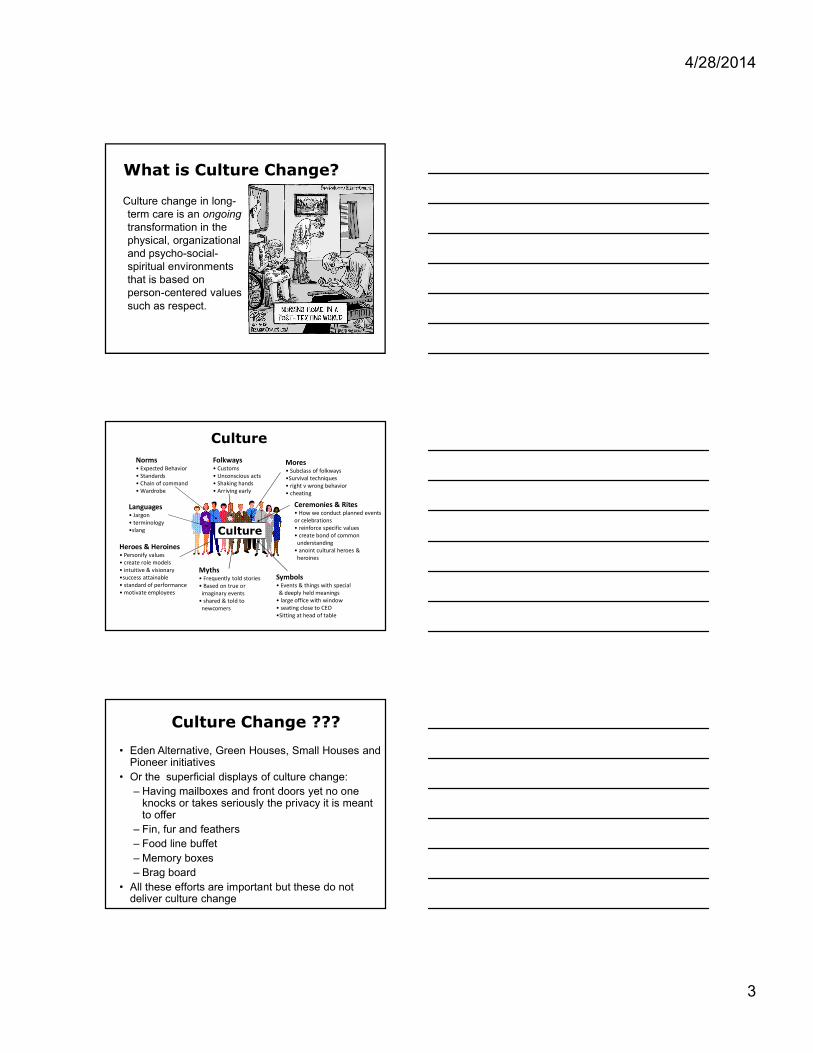
Template for Nursing Care?
.. Staff (RN, LPN, CNAs) are permanently assigned to the same unit in many NHs; in a growing number of NHs the CNAs have permanent resident assignment.
MedicationAides
Feeding Assistant/
Aides
RNs/LPNs
CNAs
RESIDENT
Administers Medication
Provides all direct care with exception of
medications and skilled treatments
Conduct assessments; provide medications
and treatments
May have “team”nursing, led by LPN or
RN to whom staff report
Permitted by federal law; receive specific
training.
4/28/2014
3
What is Culture Change?
Culture change in long-term care is an ongoing transformation in the physical, organizational and psycho-social-spiritual environments that is based on person-centered values such as respect.
Culture
Culture
Norms• Expected Behavior• Standards• Chain of command• Wardrobe
Folkways• Customs• Unconscious acts• Shaking hands• Arriving early
Mores• Subclass of folkways•Survival techniques• right v wrong behavior• cheating
Languages• Jargon • terminology•slang
Symbols• Events & things with special & deeply held meanings
• large office with window• seating close to CEO•Sitting at head of table
Ceremonies & Rites• How we conduct planned events or celebrations • reinforce specific values• create bond of common understanding
• anoint cultural heroes & heroines
Myths• Frequently told stories• Based on true or imaginary events
• shared & told to newcomers
Heroes & Heroines• Personify values• create role models• intuitive & visionary•success attainable• standard of performance• motivate employees
Culture Change ???
• Eden Alternative, Green Houses, Small Houses and Pioneer initiatives
• Or the superficial displays of culture change:
– Having mailboxes and front doors yet no one knocks or takes seriously the privacy it is meant to offer
– Fin, fur and feathers
– Food line buffet
– Memory boxes
– Brag board
• All these efforts are important but these do not deliver culture change

4/28/2014
4
Team Discussion
1. Describe the artifacts of culture change developed by CMS
2. What are the underlying values and culture that these artifacts represent?
3. What are the strengths and weaknesses of this culture?
4. Is there a gap between where the organization is and where it would like to be?
5. If you were to attempt culture change, how would you go about it?
Quality Is…
• Product or service meets its specifications
• This can be problematic for long term health care systems– Natural tension between business
needs, everyone's expectations, and government quality requirements (safety, efficiency, reliability, etc.)
– Some quality requirements are difficult to specify in an unambiguous way – quality of life
– Often the specifications for care are incomplete and inconsistent because of human nature.
• 1987 Nursing Home Reform Amendments (OBRA ’87)
• State licensure
• State Medicaid standards
• Medicare 5 Star rating
• Professional standards
• Risk group or preferred provider group
• Facility policy and procedures
• Your personal standards or code of ethics
4/28/2014
5
Quality Improvement
Variations on those themes…
• Quality assurance
• Quality improvement
• Risk management
• Quality assurance/ performance improvement
• Compliance and quality improvement
• Total quality management
Assessment of
causative factors
Determination of where you want to be
Implementation consistently with eye
on evolving issues
Evaluation and measurement of
success
NURSING HOME QUALITY
Care Planning/ interventions undertaken
Quality Assurance and Performance Improvement (QAPI)
• Significantly expands the level and scope of required Quality activities
– Ensure that facilities continuously identify and correct quality deficiencies as well as sustain performance improvement”
• QA: QUALITY ASSESSMENT
– How are we doing compared to our industry?
• PI: PROCESS IMPROVEMENT
– Making it better
4/28/2014
6
QAPI
• Design and Scope – Ongoing and comprehensive
– Includes all departments and functions
• Governance and Leadership – Administration leads with input from facility staff, as well
as from residents and their families
• Feedback, Data Systems and Monitoring – Systems to monitor care and services
• Performance Improvement Projects (PIPs)– Performance Improvement Projects
• Systematic Analysis and Systemic Action – Data driven
– Systematic approach to determine problem, its causes, and implications of a change.
Uses of Data
1. Uncover problems that might otherwise remain invisible.
2. Convince the need for change.
3. Can confirm or discredit assumptions
4. Prioritize vulnerabilities
5. Can help evaluate program effectiveness
6. Can prevent one-size-fits-all and quick solutions.
7. Give the ability to respond to accountability questions.
8. Can build a culture of inquiry and continuous improvement.
Facility Quality Measure Report
Falls w/injury
4/28/2014
7
Resident Level QM Report
Root Cause Analysis• Finding the real cause of the problem and dealing with it
rather than simply continuing to deal with the symptoms
• Asks why, why, why at each level
• Interdisciplinary- involves those closest to the situation
• Identifies changes that need to be made
• Identifies risks and how they contributed
• Leads the team to potential process improvements
• Move beyond a culture of blame
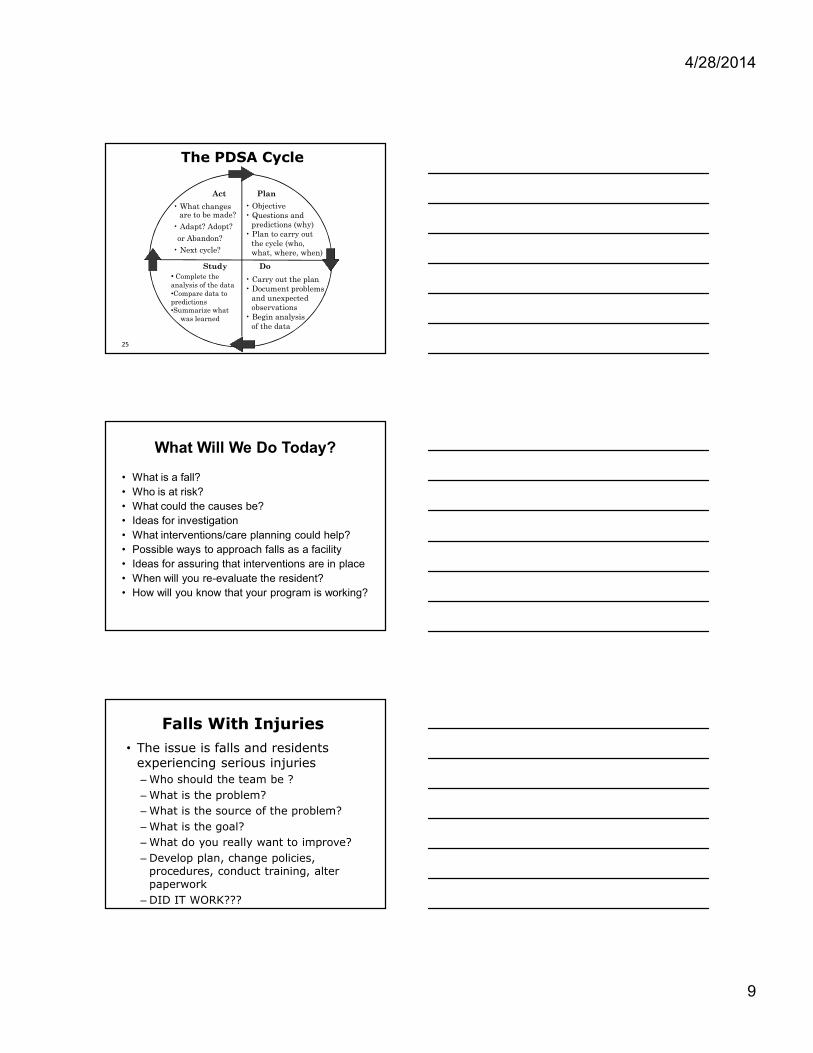
Tools for RCA
4/28/2014
8
Brainstorming Rules
• Non-judgmental communications
• Encourage wild and exaggerated ideas.
• Quantity counts at this
stage, not quality.
• Build on the ideas put
forward by others.
• Every person and every
idea has equal worth.
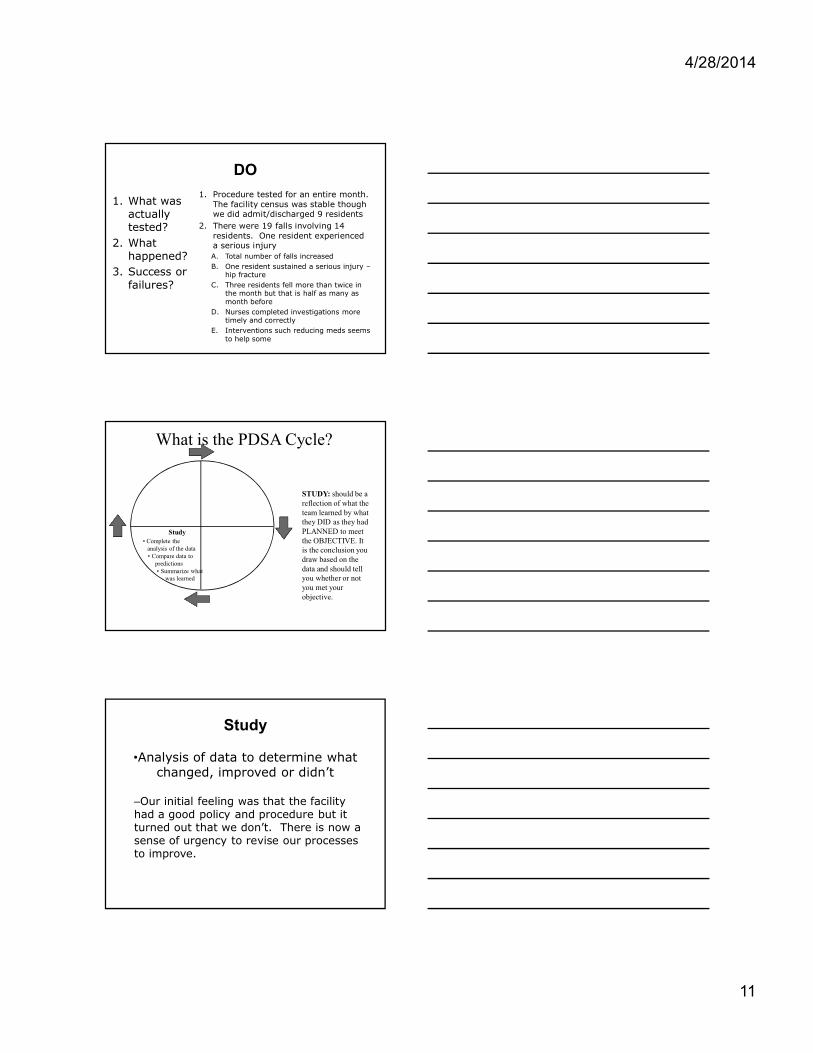
Resident fell last night
Resident pushed called light and no one came to help
Resident always just gets up even though not steady
Therapist told resident to be more independent
It was dark and tripped going to bathroom
Needs to go to bathroom every night
1. Dark bathroom2. Strength training3. Toileting and staff response
WHY ???
Now What???
• Have active and effective QAPI program
• Auditing, rounding and accountability
• William Deming
– Plan, Do, Study and Act
• Planning is the identifying of hazards and risk
• Do is the implementing of interventions to reduce risks and hazards
• Study is the monitoring of effectiveness
• Act is the effectiveness and modifying as necessary
4/28/2014
9
Act
• What changesare to be made?
• Adapt? Adopt?
or Abandon?
• Next cycle?
Plan
• Objective• Questions and
predictions (why)• Plan to carry out
the cycle (who,what, where, when)
Study
• Complete the analysis of the data•Compare data to predictions•Summarize what
was learned
Do
• Carry out the plan• Document problems
and unexpectedobservations
• Begin analysisof the data
The PDSA Cycle
25
What Will We Do Today?
• What is a fall?
• Who is at risk?
• What could the causes be?
• Ideas for investigation
• What interventions/care planning could help?
• Possible ways to approach falls as a facility
• Ideas for assuring that interventions are in place
• When will you re-evaluate the resident?
• How will you know that your program is working?
Falls With Injuries
• The issue is falls and residents experiencing serious injuries
– Who should the team be ?
– What is the problem?
– What is the source of the problem?
– What is the goal?
– What do you really want to improve?
– Develop plan, change policies, procedures, conduct training, alter paperwork
– DID IT WORK???

4/28/2014
10
What is the PDSA Cycle?
Plan
• Objective• Questions and
predictions (why)• Plan to carry out
the cycle (who,what, where, when)
Your PLAN and should answer WHO; WHAT;
WHEN; WHERE; HOW
PLAN
1. What are we testing?
2. On whom are we testing the change?
3. When are we testing?
4. Where are we testing?
• Data - What data do we need to collect?
1. NF’s falls mgt. policy and procedure
2. Nursing home residents
3. At all times
4. Throughout the facility to see if facility procedures reduce falls.
• Falls numbers, days of the week, time of day, location, possible reasons, contributing factors, etc.
What is the PDSA Cycle?
Do• Carry out the plan• Document problems
and unexpectedobservations
• Begin analysisof the data
DO (WRITTEN IN PAST TENSE): The reader should be able to read exactly what your team DID.
4/28/2014
11
DO
1. What was actually tested?
2. What happened?
3. Success or failures?
1. Procedure tested for an entire month. The facility census was stable though we did admit/discharged 9 residents
2. There were 19 falls involving 14 residents. One resident experienced a serious injury
A. Total number of falls increased
B. One resident sustained a serious injury –hip fracture
C. Three residents fell more than twice in the month but that is half as many as month before
D. Nurses completed investigations more timely and correctly
E. Interventions such reducing meds seems to help some
What is the PDSA Cycle?
Study• Complete the
analysis of the data• Compare data to
predictions• Summarize what
was learned
STUDY: should be a reflection of what the team learned by what they DID as they had PLANNED to meet the OBJECTIVE. It is the conclusion you draw based on the data and should tell you whether or not you met your objective.
Study
•Analysis of data to determine what changed, improved or didn’t
–Our initial feeling was that the facility had a good policy and procedure but it turned out that we don’t. There is now a sense of urgency to revise our processes to improve.

4/28/2014
12
What is the PDSA Cycle?
Act
• What changesare to be
made?• Next cycle?
ACT (WRITTEN IN FUTURE TENSE): should describe what your next steps will be to meet the objective based on what you learned from what you did according to the plan to meet the objective.
ACT
1. What adjustments to the change or method of testing should we make before the next cycle?
– Team will redraft policy and procedures, risk assessment, investigation tools, QA review tool
1. Are we ready to implement the change we tested?
– Total facility reeducation
2. What will the next test cycle be?
– Next months data related to falls will begin test our ability to successively revise policy and procedure.
The QIS Process
• The Quality Indicator Survey process is a revised survey process that changes how surveyors determine a facility's compliance
• Phase I – Collected comprehensive set of resident
sampling data consisting of standardized questionnaires, specific observations and record reviews which is used to determine a facilities Quality Indicators
• Phase II
– Once the quality indicators are determined surveyors investigate items which exceed CMS thresholds
• Goes beyond previous traditional survey process by measuring quantified quality of life aspects of care
4/28/2014
13
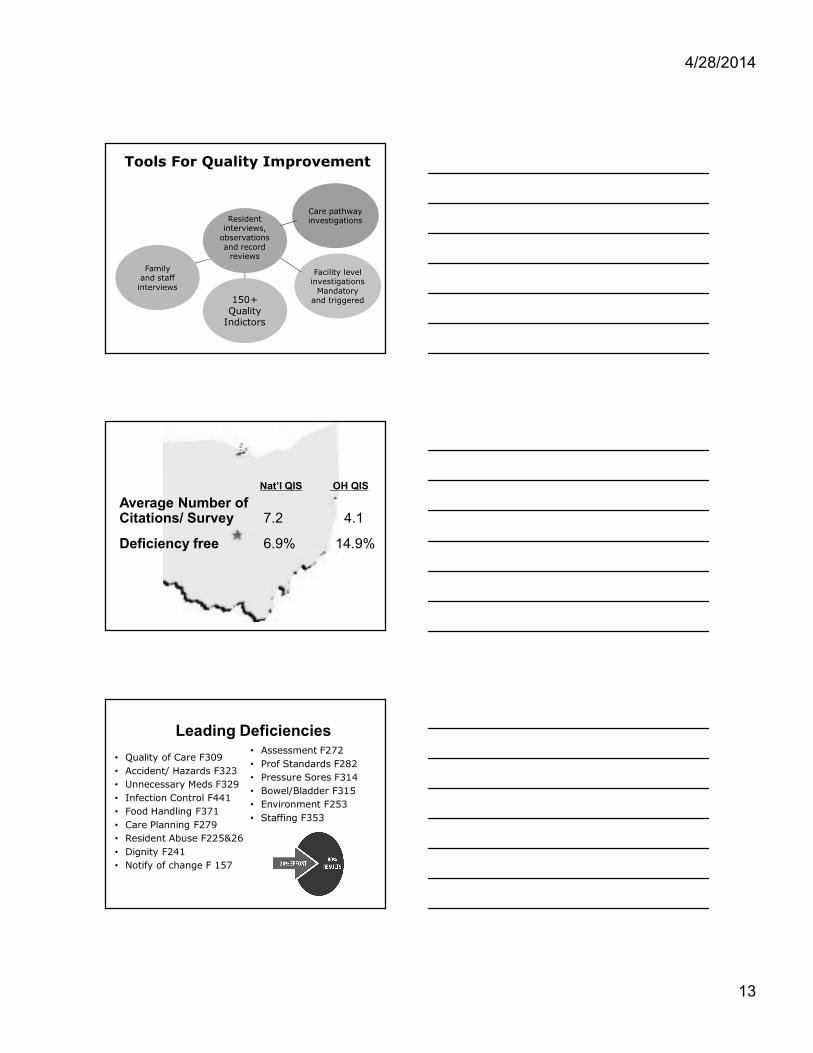
Tools For Quality Improvement
Resident interviews,
observations and record
reviews
Facility level investigations
Mandatory and triggered 150+
Quality Indictors
Family and staff interviews
Care pathway investigations
Nat’l QIS OH QIS
Average Number of Citations/ Survey 7.2 4.1
Deficiency free 6.9% 14.9%
Leading Deficiencies
• Quality of Care F309
• Accident/ Hazards F323
• Unnecessary Meds F329
• Infection Control F441
• Food Handling F371
• Care Planning F279
• Resident Abuse F225&26
• Dignity F241
• Notify of change F 157
• Assessment F272
• Prof Standards F282
• Pressure Sores F314
• Bowel/Bladder F315
• Environment F253
• Staffing F353

4/28/2014
14
“Trigger” Responses and Stage II Investigations
QIS rates for:
• Family Interview 19.6%
• Resident Interview 19.4%
• Staff Interview 18.6%
• Admission Clinical Record 17.8%
• Resident Observation 16.6%
• Census Clinical Record 15.2%
Triggered vs. Deficiency
Care Area Trigger % Citation %
Accidents 99% 27%
Pressure Ulcers 77% 21%
Community Discharge 77% 11%
ADLs 60% 11%
Nutrition 58% 16%
Rehabilitation 58% 2%
Urinary Incontinence 56% 0%
Dental 55% 23%
ROM 46% 15%
Abuse 43% 22%
Admis/ Transfer 41% 11%
Environment Observations 41% 63%
Triggered vs. Deficiency
Care Area Trigger% Citation %
Dignity 40% 15%
Choices 40% 17%
Activities 40% 27%
Personal Funds 38% 17%
Staffing 36% 6%
Personal Property 35% 8%
Hydration 26% 8%
Catheter Use 21% 12%
Participation in Care Planning 17% 16%
Hospitalization 15% 0%
Restraints 15% 35%
Skin Conditions 15% 32%

4/28/2014
15
Triggered vs. Deficiency
Care Area Trigger % Citation %
Food Quality 12% 6%
Pain Management 11% 18%
Privacy 9% 9%
Notification of Change 8% 22%
Positioning 1% 38%
Social Services 1% 100%
Behavior Emotion Status - 2%
Infections - 25%
Vision - 27%
UTIs - 0%
Stage II Investigations
Task Triggered Task Triggered
Extended Surveys 62% Personal Funds 18%
Environment 58% Dining 17%
Unnecessary Med 40% Med. Admin 11%
Infection Control 33% Liability Notices 5%
Kitchen 26% Staffing 5%
Abuse Prohibition 24% QA & A 4%
Med Storage 23% Resident Council 4%
Average number of tasks triggered = 12.1
Survey is Survey • Facility appearance & what surveyors see, hear,
feel and smell is important• Residents with obvious unmet needs• Resident interactions • Activities • Dining experience • Personal items stored & labeled• Data
– Weights– Skin – Behavior – Falls
• Splints and restorative care• Wheelchairs and lifts• Therapy gym
Remember: survey is about the basics

4/28/2014
16
Off-site to Entrance• Review facility history is reviewed including the
CASPER, past survey history and patterns of repeat deficiencies
• Contact ombudsman • Conduct entrance conference with
Administrator/designee– 1 surveyor meets with administrator– 2 surveyors begin tour plus the kitchen– 1 surveyor completes reconciliation
• Provide resident census • Medicare beneficiaries of last six months sampled
from MDS data for review of Liability Notice and Beneficiary Appeal Rights review
Entrance Activities
• QIS brochure is provided
• Given the CMS 671 and CMS 672
• Resident lists:– PASRR II Services
– Ventilator
– Dialysis • Unit, Peritoneal, Home
– Certified Medicare Hospice– Comfort/ End of Life care
• One Resident will be chosen from each care area during stage II
This is where 5 Star staffing comes from…
Initial Tour
• Characteristics of the facility, special care areas, staff – resident interactions, response to resident requests, behaviors
• Ask nursing assistants questions, such as
– How many residents are under your care today?
– Who determines the assignment?
– Is there enough time to complete your assignment?
– What happens if you do not get your assignment completed?
– What steps do you take when the fire alarm sounds?
– What is RACE?

4/28/2014
17
Entrance Notebook
• Alphabetical Resident Census• New Admission Information (last 30 days)• Facility floor plan• Staffing schedules for survey period• List of key employees• Resident Council President• Meal times and locations• Medication times• Whether facility utilizes paid feeding
assistants• Influenza/ Pneumococcal Immunization policy
and procedure
Entrance Notebook
• List of rooms that would require a variance– Less than required square footage– More than 4 residents– Below ground level– No window to the outside– No access to an exit corridor
• Quality Assessment and Assurance (contact, members, frequency)
• Experimental research• Contact person for Abuse policies and
procedures • Whether or not DON is full time• Emergency water policy/ contact
Additional Information
• CLIA certificate• Surety Bond• Fire drills past year• Activity calendar• Resident council minutes
(3-6 months)• Abuse policy and self
reported incidents• STNA Registry update• Criminal background logs• Medical Director reports• Grievance committee
minutes/ policy
• Resident Council minutes• Smoking policy• Infection control policy• Nurse aides less than 4
months• Employee files (Mantoux,
H/P, in-servicing)• Department heads less than
1 year• Resident account balances• Medical director information

4/28/2014
18
Census and Admission Sample
• Census and Admission sample drawn from MDS sample plus census reconciliation
• Thresholds are broken into categories ‘small’and ‘not small’. Small would be when there are 35 or fewer residents
• Census sample – random sample current residents
– Resident interviews and observations
– Staff and family interviews
– Record reviews
• Admission sample – random sample of up to 30 discharged residents
– Record review
Census Sample Update
• The Census Sample (affecting 50% of facilities) was altered to speed up process
• If facility census is:
– > 100 residents = sample size of 40
– 61-100 residents = sample size of 35
– 33-60 residents = sample size of 30
– 1-32 residents = the sample will automatically be set to 90% of the total
Sentinel QIs
1. Abuse2. Dangerous device use3. Fall/Fracture4. Activities 5. ADL Assist6. Admission process7. Exercise Rights8. Death9. Dehydration 10.Hydration 11.Notification of family12.Personal Funds13.Privacy14.Medicaid costs 15.Range of Motion
16.Oral health status
17.Comfortable Temperatures
18.Pest control
19.Electric cords & outlets
20.Ambulation, therapy equip.
21.Bathing safety
22.Call light
23.Chemical-Hazard
24.Unsafe hot water
25.Sufficient staff
26.Participate in care plan
27.PU @ stage 3 or 4
28.Presence - incontinence
QIS indicators set at 0-1% threshold
4/28/2014
19
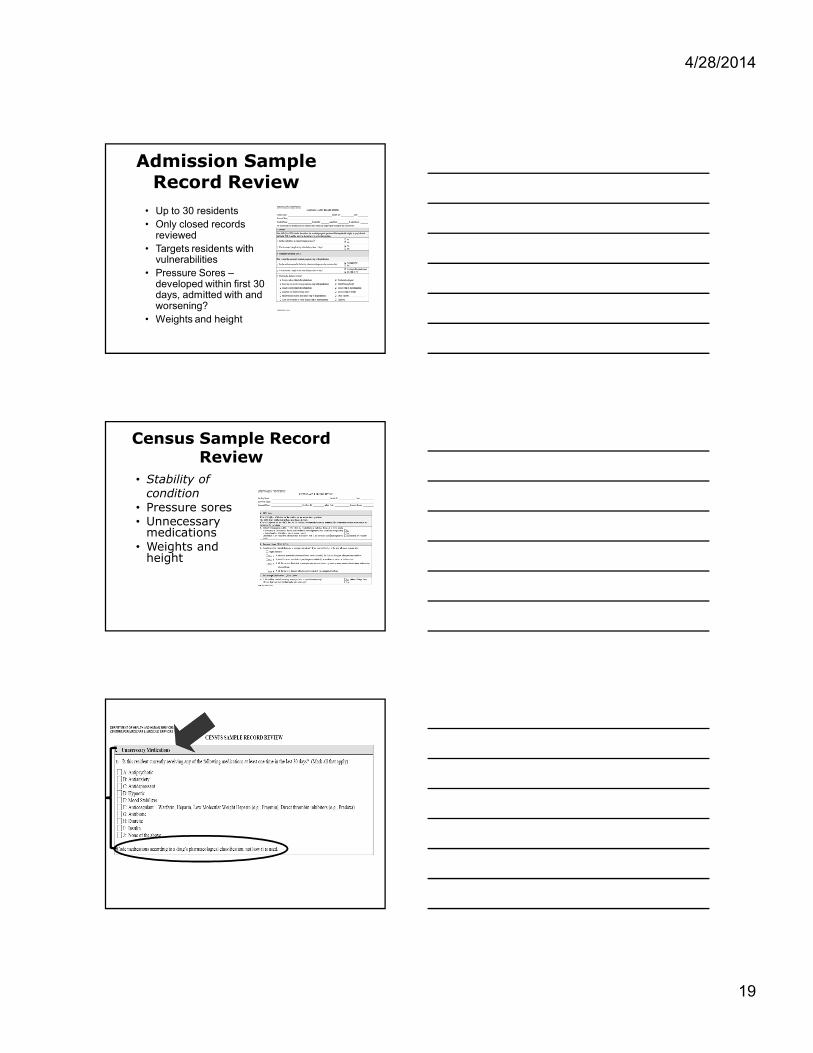
Admission Sample Record Review
• Up to 30 residents
• Only closed records reviewed
• Targets residents with vulnerabilities
• Pressure Sores –developed within first 30 days, admitted with and worsening?
• Weights and height
Census Sample Record Review
• Stability of condition
• Pressure sores• Unnecessary
medications• Weights and
height

4/28/2014
20
Unnecessary Medications Sampling Algorithm for QIS
• Census Sample residents are chosen for the Unnecessary Medications
• Residents receive a score based on the medications that they receive
• Algorithm scores range from 0 to 18.
• 5 residents with the highest scores are included in the sample
Unnecessary Medication Scoring
• Residents with diagnosis of dementia or Alzheimer's AND receiving Antipsychotic
– 3 points
• Residents who have a fall or fracture AND receiving:– Antipsychotic – Antianxiety – Antidepressant – Hypnotic – Mood Stabilizer – Diuretic
• 2 points
• Resident score point(s) for receiving each of the following:
– Antipsychotic (excluding Alzheimer’s/dementia diagnosis)
– Antianxiety – Antidepressant – Hypnotic – Mood Stabilizer – Anticoagulant – Insulin
• Up to 7 points • Residents receive an additional
points when they receive med above and a marked as sedated, weight loss, 2 or more of these meds, Alzheimer's/ dementia and/or falls
• 1 point for each
Unnecessary Medication Algorithm
• QIS software will select 5 resident based on surveyor responses to selected questions in the Census Sample resident observation, record review, and staff interview components of the QIS.
• Scores range from 0 to 18.
• The five residents with the highest scores are included in the sample

4/28/2014
21
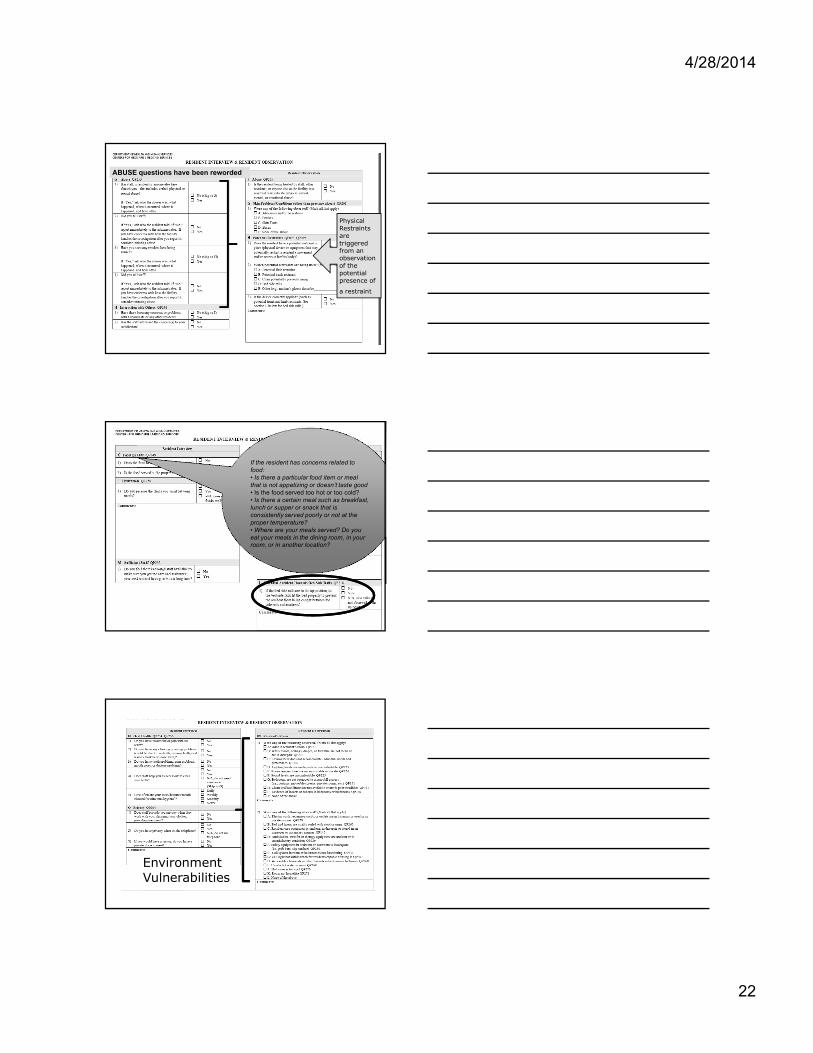
Resident Interview & Observation
Key surveyor interview and observation tool
• Surveyor makes final decision after talking with each individual resident
• The BIMS is used to determine Interviewablity
– Score > or = to 8, resident is interviewable
– Score < or = to 7 or 99, resident is non interviewable and set to family interview status
The second part of each of the questions intended to probe for additional information when a resident responds negatively to the initial portion of the question. Probing questions may be asked to obtain appropriate information to start an investigation in Stage 2
Participation Participation in Care Plan: •Physician orders a change in your medications and RESIDENT is made aware of the change? •If the physician is contacted about you, are you made aware of the results? •Does staff tell you the results of tests like lab work or x-rays? •If you need to have an appointment scheduled (for instance with an outside physician), are you informed of the appointment? • Have you brought questions or concerns about your care to the attention of facility’s staff? If so, what happened as a result?
4/28/2014
22
ABUSE questions have been reworded
Physical Restraints are triggered from an observation of the potential presence of
a restraint
4/28/2014 65
If the resident has concerns related to food: • Is there a particular food item or meal that is not appetizing or doesn’t taste good• Is the food served too hot or too cold? • Is there a certain meal such as breakfast, lunch or supper or snack that is consistently served poorly or not at the proper temperature? • Where are your meals served? Do you eat your meals in the dining room, in your room, or in another location?
EnvironmentVulnerabilities

4/28/2014
23
4/28/2014 67
The surveyor may need to The surveyor may need to ask probing questions to help determine if the resident understands the difference between a commercial bank account and the facility’s
Sleeping Resident?
Staff Interview
• Staff interviews are conducted with licensed staff, either the RN or LPN– Catheter Use
– Nutrition
– Skin care/ Pressure Ulcers
– Side Rails
– Contractures
– Falls or fractures
Family Interview• Three family members or resident representatives
who know the resident well and visit the facility
• Choices
• Activities
• Privacy
• Dignity
• Interactions with others
• Sufficient staff
• Activities of daily living (ADL) assistance
• Oral health
• Abuse
• Personal property
• Building and environment
• Exercise of rights
• Costs and personal funds
• Admission process
• Notification of change
• Participation in care plan
4/28/2014
24
Facility Level Investigations
• Resident Council President/ Representative interview
• Dining observation
• Kitchen/ food service Infection control
• No second probe
• Liability Notice and Beneficiary Appeal Rights
• Quality assessment and assurance review
• Infection Control
• Medication Pass
• CMS policy change to reduce from 50 to 25 opportunities
Resident Council President
• To ensure that the facility listens to and responds in a timely manner to concerns voiced by the residents– Council F 243
– Grievances F244
– Rules F242/F244
– Rights F151, F153, F156, F167, F179, F172, F242
Dining
• Observation of overall dining experience (in various dining rooms and resident rooms) and the availability of staffing to assist the residents– Staff prepare, serve, and assist at meal times F353/F362– Meals served within 14hours / or 16 hours w/substantial
snack F368– Assistance with meal F311/F312– Staff infection control F371/ F441– Dignity and Independence F241
• Non-disposable cutlery and plates/napkins• Resident desires considered when using clothing protectors
– Meal service including substitutes F366– Positioning F310– Dining room atmosphere F464/F258/F253– Furnishings and space F464– Food quality F364– Liquids at meal time F327

4/28/2014
25
Kitchen/ Food Service
• To observe general sanitation practices, cleanliness of the kitchen and any practice that might indicate potential food-borne illness– Food storage F371
– Storage temperatures F371/F456
– Food preparation and service F364/F371
– Dinnerware sanitization and storage F371
– Refuse/ pest control F372/F369
– Equipment Safe/Clean F456
Infection Control
• System to prevent the development and transmission of diseases F441
• Flu and Pneumococcal immunization policy F334
• Surveyors will observe specific areas of the facility at various times during the survey F441– Hand washing techniques
– Glove issues
– Staff free from communicable diseases
– Linen handling, sharps disposal, dressings, disposals
– Isolation procedures
Liability Notice & Beneficiary Appeal Rights
• To ensure the facility properly handles Medicare non-coverage
• Advanced Beneficiary Notice (ABN – SNF)
• Notices include– Appropriate notice information F156
– Date of non-coverage F156
– Provided prior to date of non-coverage F156
– Acceptable reason F156
– Option to request demand bill and was handled appropriately F 492
4/28/2014
26
Quality Assessment and Assurance
• Part I (all facilities) F520– Determine if the facility has functioning QAA
committee
– Medical director involvement
– Identify participants
– Identify committee leader
– Determine frequency of meetings
• Part 2 (completed when potential quality deficiencies are identified) F520– Determine if the QAA committee effectively
identifies and addressing quality deficiencies
Medication Administration
• To observe facility’s medication administration system in operation and to verify the accuracy, technique and compliance with professional standards
• Selection of 10 residents
• 25 medication administrations per team –prefer to view different routes, shifts and staff
• Observe medicine storage
• Review the MAR
Transition from Stage I to Stage II
• Software calculates the indicators and compares results to national rates– Determine what stage II facility level tasks
have been triggered and require an in-depth investigation is required
• Stage II sample selected by software– Fewest residents with most issues
• Normally three residents - each triggered area
• Triggered Tasks– Environmental review– Resident Funds– Admission, Transfer, and Discharge– Sufficient Staff– Abuse prohibition review

4/28/2014
27
Environmental Review
• Resident Care Equipment
• Ambulation, Transfer and
Therapy Equipment
• Bedroom Privacy
• Clean Linens Available
• Unsafe Hot Water
• Lack of Hot Water
• Room Furnishings
• Electric Cords and Outlets
• Bathing Safety Equipment
• Pest Control
• Room Odors
• Functioning Call System
• Call Light in Reach
• Chemical/Hazards in
Room
• Homelike Environment
• Room Accommodations
• Clean Building
• Lighting Levels
• Comfortable sound levels
• Comfortable Room
Temperatures
Resident Funds
• Ensure that the facility appropriately handles a residents personal funds– Informed services and costs F156
– Week end access to $$ F159
– Accounting practices, interest, surety bond F159
– Quarterly statements F159
– Notice w/in $200 Medicaid limit F159
– Conveyance upon death F160
Admission, Transfer, and Discharge Review
• To ensure that the facility properly handles resident admission, transfers and discharges– Application for Medicare and Medicaid
benefits F208
– Inform of rights F156
– Room changes F247
– Third party guarantee F208
– Bed hold F205
– Facility initiated discharge/transfer F204, F250, F309
4/28/2014
28
Sufficient Staff
• Sufficient staff available to meet the residents’needs F353 and F354
• Facility has licensed registered nurses and available to provide and monitor the delivery of care
• Advised of care plan changes
• Adequate to meet care needs of resident
• Appropriately deployed
– RN coverage
– Nursing aides
– Adequate assistance with meals
Abuse Prohibitions
• To determine if the facility has developed and operationalized policies and procedures including 1. Screening of potential employees;
2. Training of employees (both for new employees, and ongoing training for all employees);
3. Prevention policies and procedures;
4. Identification of possible incidents or allegations which need investigation;
5. Investigation of incidents and allegations;
6. Protection of residents during investigations; and
7. Reporting of incidents, investigations, and facility response to the results of their investigations.
Unnecessary Drug
• Appropriate dose – consider duplicative therapy?
• In the presence of adverse consequences which would indicate the dose should be reduced or discontinued
• Adequate indication for use?• Adequate monitoring?• Appropriate duration?• Gradual dose reductions – unless clinically
contraindicated• Medication dose reduced or discontinued in presence
of adverse drug reactions or side effects• Appropriate monitoring, duration, dose and indication
for use.

4/28/2014
29
Critical Element Pathway
• Each CE Pathway is set up with the same basic format– Assessment (F272)– Care planning (F279)– Professional Standards of care (F281)– Provision of care and services (F281)– Care plan revision (F280)– Concerns with structure, process and/or outcomes related to
process of care
• Guides surveyors through investigation
• Each pathway suggest specific F-tags that should be considered plus additional areas to consider/ investigate
SOM Guidance Only
• Abuse
• Accidents/ Falls
• Resident Rights
• Choices
• Accommodations of needs
• Dignity
• Privacy
• Social services
• Rehabilitation
• Food quality
• Nutrition
• Hydration
• Foot care
• Notification of change
• Personal property
• Participation -care plan
Critical Element Pathways• Activities
• ADLs/ ROM
• Behavioral and emotional status
• Incontinence, Catheters, UTIs
• Communication and sensory problems
• Dental status and services
• Dialysis
• General
• Hospice-Paliative Care
• Hospitalization or death
• Pain management
• Physical restraints
• Pressure ulcers
• Psychoactive medications
• Rehabilitation and community discharges
• Unnecessary Meds
• PASARR
• Hydration
• Ventilator dependent residents
• Tube feeding status
• Dementia (2014)
4/28/2014
30
Dementia Investigation F309• Assess behavior (onset, duration, intensity, possible precipitating events
or environmental triggers, etc.) and related factors (appearance, alertness, etc.) I
• Staff assess the underlying cause of behaviors
• When there is a suspected change in condition or worsening from baseline, did staff contact the attending physician/practitioner immediately for a medical evaluation
• If medical causes are ruled out, did staff attempt to establish other root causes of the behavior using individualized knowledge about the person and when possible, information from the resident, family, previous caregivers and/or direct care staff?
• As part of the comprehensive assessment did facility staff evaluate:
– The resident’s usual and current cognitive patterns, mood and behavior, and whether these present a risk to the resident or others?
– How the resident typically communicates a need such as pain, discomfort, hunger, thirst or frustration?
– Prior life patterns and preferences customary responses to triggers such as stress, anxiety or fatigue, as provided by family, caregivers, and others who are familiar with the resident before or after admission?
Dementia Care Planning• Was the resident and/or family/representative involved in discussions
about the potential use of any interventions, and was this documented in the medical record?
• Does the care plan reflect an individualized team approach with measureable goals, timetables and specific interventions for the management of behavioral and psychological symptoms?
• Does the care plan include:
• Involvement of the resident/representative to the extent possible?
• A description of and how to prevent targeted behaviors?
• Why behaviors should be prevented or otherwise addressed (e.g., severely distressing to resident)?
• Monitoring of the effectiveness of any/all interventions?
• If the resident or family/representative refused a recommended treatment or approach, was counseling on consequences and alternative approaches to address behavioral symptoms provided?
Care Plan Implementation• Identify, document and communicate specific targeted
behaviors and expressions of distress as well as desired outcomes?
– Implement individualized, person-centered interventions by qualified persons and document the results?
– Communicate and consistently implement the care plan, over time and across various shifts?
– If there is a sudden change in the resident’s condition and medical causes of behavior or other symptoms are suspected, is the physician contacted immediately and treatment initiated?
• Is there a sufficient number of staff to consistently implement the care plan? (Surveyors should focus on observations of staff interactions with residents who have dementia to determine whether staff consistently applies basic dementia care principles in the care of those individuals).

4/28/2014
31
Resident Care
• If during the survey a concern is identified that an antipsychotic medication is given by staff for purposes of discipline or convenience and not required to treat the resident’s medical symptoms, review F222 – §483.13(a).
• If the physician does not respond to the notification, does staff contact the medical director for further review? If the medical director was contacted, does he/she respond and intervene as needed?
• Did the facility provide the necessary care and services for a resident with dementia to support his or her highest practicable level of physical, mental and psychosocial well-being in accordance with the comprehensive assessment and plan of care? If No, cite F309
Care Plan Revision/Monitoring and Follow up
• Does staff, in collaboration with the practitioner, adjust the interventions based on the impact on behavior or other symptoms as well as any adverse consequences related to treatment?
• When concerns related to the effectiveness or adverse consequences of a resident’s treatment regimen are identified:
• Does staff modify the care plan and, if appropriate, notify the physician and does the physician respond and initiate a change to the resident’s care as necessary?
Quality Assessment and Assurance
• Do resident care policies and procedures clearly outline a systematic process for the care of residents with dementia?
• Does the QAA Committee monitor for consistent implementation of the policies and procedures for the care of residents with dementia?
• Has the QAA committee corrected any identified quality deficiencies related to the care of residents with dementia?
• Has the QAA committee provided monitoring and oversight for the care and services for a resident with dementia?
4/28/2014
32
General
• The critical element pathway is utilized when the area of investigation is not addressed by other CEs such as:– Non-pressure related wound care (venous/arterial
or neuropathic ulcers)
– Bowel management problems including fecal impaction
– Diabetes mellitus and congestive heart failure
– Accidents and supervision including falls
– Fractures
– Elopement
– Other hazards related to the use of assistive devices
Activities
• Assessment – Identify individual activity preferences and interests
– Adaptations
• Care Planning – Input from the resident and/or representative that provides to the
extent that provides for the resident's participation in activities of choice?
• Associated tags– F 164 privacy
– F 172 Access and Visitation
– F 242 Self Determination
– F 246 Accommodation of Needs
– F250 Social Services
– F 353 Sufficient Staff
– F464 Dining and Activities Rooms
ADLs
• Determine: – Adequately assess to
determine the level of ADL, functional ROM and contractures
– Causal and contributing factors
– Potential to improve?
– Consistent implementation
– Staff knowledge
– Changes in condition
– Effectiveness
– Risks and approaches
• Various F-tags including– F310 Current ADL
performance
– F311 potential for improvement but none
– F312 Resident unable
– F309 Unable to position
– F317 No limitations, but now has some
– 318 Limitations but potential for…

4/28/2014
33
97
Behavioral and Emotional Status • Observations
– Staff and resident interactions, appropriate care for behavioral, mental and/or emotional status and ensuring safety
• Assessment and care Planning– Individualize interventions that are known to the staff and are
consistent including protocols for treatment including deviations
• Associated tags– F319 appropriate treatment for mental/ psychosocial difficulties
– F320 no development of unavoidable mental issues
– F309 Provide necessary care for highest practical well being
– F223 abuse
– F241 dignity
– F250 social services
– F329 unnecessary medications
Bowel and Bladder Function
• Assessment
– Resident's overall condition including continence status and patterns
– Fluid intake
– Medications
– Clinical reasons for catheter and alternatives
• Care planning– Identifies objectives and
potential psychosocial complications
– Education component– Environmental approaches
• F tag issues
– F315 urinary incontinence
– F241 dignity
– F309 quality of care
– F312 ADLs
– F353 sufficient staff
– F385 physician services
– F444 infection control
Communications
• Observations
– Activities and interactions consider any limitations in communications including vision and hearing
• Assessment
– Considers all contributing factors, potential for decline and lack of improvement
• Care Planning– Specific protocols that are
known to all staff and implemented consistently
– Need for assistive devices and use
– Examinations
– Environmental factors
– Risks for accidents
• F –tags– F310/ F311 ADLs
– F313 Vision and hearing

4/28/2014
34
Dental• Observations
– Difficulties with chewing– Denture issues– Mouth care– Medications– Hygiene issues– Knowledge of staff and
interventions delivered– Dentist services available
• Assessment
– Contributing factors
– Impact of oral health on functions such as eating, social, overall health
• Care planning
– Consistent with specific needs of resident
– Treatment protocols
• Consistent with goals and strengths
• F tags
– F411 and F412 Dental services
Residents Who Receive Dialysis
• Assessment– Medical status including vital signs– Psychosocial needs– Risk factors and complications
• Care Planning– Developed for specifics of the
resident and related to dialysis services, including
• Nutritional and hydration issues• Medications• Care of access site• Infection control and skin
measures• Vital signs and weights
• F tags
– F309 quality of care
– F282 qualified staff
– F425 Pharmacy services
– F455 emergency power
Hospice
• Assessment– Contributing factors
– Continence
– Nutrition
– Medication interactions or side effects
– Spiritual needs
– Values, wishes, choices and goals
• Care planning– Meets specific needs of
resident conditions, risks, needs, behaviors, preferences and current standards of practice
• F tag considerations
– F309 Quality of care
– F164 Privacy and confidentiality
– F172 Access and visitation
– F242 Self determination
– F246 Accommodation of Need
– F250 Social services
4/28/2014
35
Hospitalization or Death
• Professional standards
– ID acute issues
– Vital signs, pain, ID potential contributing and/or causal factors such as meds, falls, labs
– Appropriate staff available
– Notified physician & family
• F tags
– F309 Quality of care
– F241 Dignity
– F242 Self determination
– F353 Sufficient staff
– F385 Physician services
– F501 Medical director
Nutrition, Hydration, Tube Feed
• Assessment
– Baseline status
– Diet calculation
– Intake issues
– Weight history
– Terminal illness
• Care Planning– Prevent and/or address weight
issues and dehydration concerns
– Prevent unnecessary tube feeding
– Restorative dining
– End of life consistent with wishes and address decreased appetite
• F tags
– F321 Naso-gastric tubes
– F322 Naso-gastric tube
– F325 Nutrition
– F327 Hydration
– F328 Parenteral and enteral fluids
Pain
• Assessment– History including
conditions, risks and contributing factors
– Identify functional limitations
• Care Planning– Address impact of pain on
function
– Monitoring for sign and symptoms
– Intervention strategy
• F tag considerations
– F309 Quality of care
– F157 Notification of changes
– F172 Access and visitation
– F242 Self determination
– F246 Accommodation of Need
– F250 Social services
– F 353 Sufficient staff
– F385 Physician
– F501 Medical director

4/28/2014
36
Physical Restraints
• Assessment– Medical symptoms
– Function
– Risk and benefit
• Care planning– Goals for use and intended
improvement in function
– Type of restraint and in what circumstances for use
– Frequency and monitoring
– Interventions/ services when not in use
– Interventions to limit functional decline
• F tags– F221 restraints
– F242 self determination and participation
– F246 accommodation of need
– F248 activities
– F323 accidents
– F353 sufficient staff
– F385 physician services
– F406 specialized rehab
Pressure Sores
• Assessment– Resident function,
medications, skin condition, cognitive status, nutrition
– Identifies factors that increase risks for development or healing
• Care planning– Developed to address
the specific conditions, risks, needs, behaviors, and preferences (and standards of practice)
• F tag considerations
– F157 Notification of changes
– F309 Quality of Care
– F314 Pressure Ulcers
– F325 Nutrition
– F327 Hydration
– F353 sufficient staff
– F406 specialized rehabilitation
– F385 physician services
Rehabilitation and Community Discharge
• Assessment– Resident status including
overall health and psychosocial status
– Identifies risks, strengths, weaknesses
• Care planning
– Goals, needs and strengths
– Care plan known by staff responsible and delivered consistently
– Preparations for discharge
• F tag considerations– F250 social services
– F 311 Activities of daily living
– F406 specialized rehabilitation
– F241 dignity
– F246 accommodation of needs
– F 309 quality of care
– F318 range of motion
– F353 sufficient staff
– F385 physician services

4/28/2014
37
Ventilator Dependant
• Assessment• Potential weaning,
psychosocial issues, advanced directives, ADLs
• Care planning– Vent equipment
– Alarms (power failure)
– Ventilator use
– Ventilator setting
– Type of airways
– Adjunctive interventions
– Psychosocial issues
– Monitoring for use/changes
– Emergency issues
•F tag considerations
–F157 Notification of changes
–F325 Nutrition
–F327 Hydration
–F328 Special care
–F353 sufficient staff
–F406 specialized rehabilitation
–F385 physician services
Extended Survey
• Extended Survey is not part of the QIS standard survey
• Surveyor-initiated – before the exit conference or within two weeks of completion of the standard survey
• When the survey team determines during the standard survey that substandard quality of care exists.
– One or more deficiencies with scope/severity levels of F, H, I, J, K, or L in any of these regulatory groupings:
• Nursing Services (F353-354)
• Physician Services (F385-390)
• Administration (F490-F522)
Regulatory Compliance
• Potential citations are agreed too and statement of deficiency is developed by with integration of findings
• Combine stage I and II findings across residents by F-tag– Identify deficiencies
– Scope and severity
• Exit conference
4/28/2014
38
Quality Management
• Quality management must deliver bottom-line
– Measure true impact of time and investment
• Quality is everyone’s job
– Practices and understanding of the continuous nature of quality
• Quality management will increasingly be absorbed in each of our jobs
– Moving from ‘doing’ quality to coaching for quality
• Customer expectations are increasing
– Customers are accustomed to speed, efficiency, and excellent customer service will demand that of long term care too
Core Principles
• We want a better future than the future we have
• If we do what we have always done, we will get what we always had
• Know the truths and share them
• Core changes is a function of new truth
• There are things that we know that are the exact opposite of what the public believes
• Honesty
• We are change agents
• Educate vs. telling
Person-centered Care? • What does the nursing home do to make residents
feel comfortable
• Do They take a person's personal habits into consideration when developing plans of care
• Do residents make choices about – When they wake up, eat meals, bathe, or take
medications?
– What they do with their day?
• Does nursing home have any house pets? And do you allow residents to have pets of their own?
• What types of programs or activities does nursing home offer that allow residents to feel like contributing members of society?
4/28/2014
39
Compliance Versus Quality Improvement
Compliance
• Floor is goal
• Crisis management
• High stress
• High costs
• “Turn around effect?”
Quality
• Goals increase/change
• Success is planned for
• Manageable challenge
• Manageable challenge
• Recruitment/retention
A Case for Preparation:
“Look, I really want the fancy scroll work on the rails. In a hundred years, who’ll know I scrimped on the soil samples?”
S&C Memos
• Survey and certification memo inform state and regional offices of CMS
• ‘Google” Survey and Certification memo

4/28/2014
40
Resources
www.cms.com
www.med-pass.com
Quality Indicator Survey: “Process Tools and Resources Manual”
Kenneth Daily, [email protected]
• Consulting and education focusing on quality improvement, survey compliance, and facility management.
• Comprehensive Traditional and QIS technical assistance, Mock surveys and audits
– Standard/traditional and QIS preparation
– Directed Plan of Correction development and implementation
• Immediate Jeopardy Assistance
• Quality/Performance Improvement Program development and implementation
• Corp Compliance Plans
END