qolop: the brno quality of life longitudinal study of paediatric oncology patients. developmental...
TRANSCRIPT

QOLOP: THE BRNO QUALITY OF LIFE LONGITUDINAL STUDY OF PAEDIATRIC
ONCOLOGY PATIENTS. Developmental approach.
Tomas Kepak1, Marek Blatny2, Alena Slezackova 2, Irena Vlckova1, Kristina Tothova1, Martin Jelinek2, Veronika Sobotkova2, Milan Pilat3, Sarka Karova4, Hana
Hrstkova1, Jaroslav Sterba1
(1) University Hospital Brno, Paediatric Oncology, Brno, Czech republic(2) Czech Academy of Sciences, Institute of Psychology, Brno(3) University Hospital Brno, Paediatric Psychiatry and Clinical Psychology, Brno (4) Masaryk University, Institute of Psychology, Brno, Czech republic
7th PanCare Meeting Brno, April, 2011
“qolop” project description
• “qolop” = quality of life longitudinal study of paediatric oncology patients = prospective longitudinal study, designed to meet contemporary requirements on research methodology
• Aims to reflect changes in QoL during the time• Complex study design in terms of health, social and
educational issues, parental-child relationship etc.• Focus both on positive and negative outcomes (stress,
PTSD, PTG)• Research data as a base for future preventive and
interventional strategies for Czech/Slovak survivors
Kepak, Blatny et al.: The Brno Quality of Life Longitudinal Study of Pediatric Oncology Patients
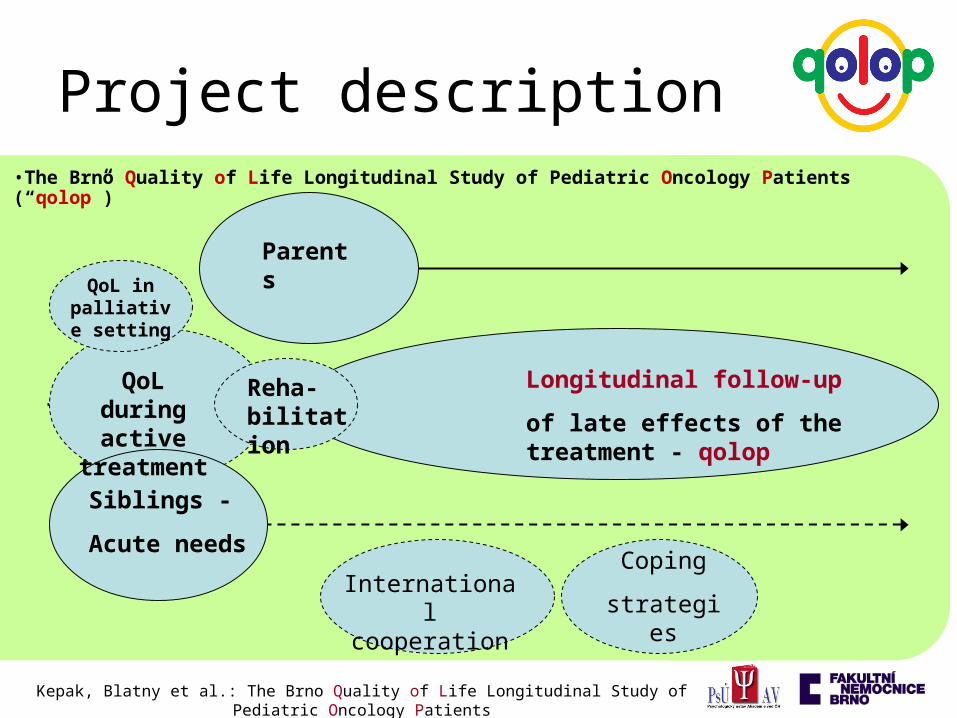
Longitudinal follow-up
of late effects of the treatment - qolop
Parents
Siblings -
Acute needs
Reha- bilitation
QoL during active
treatment
QoL in palliative setting
Coping
strategiesInternational cooperation
Project description•The Brno Quality of Life Longitudinal Study of Pediatric Oncology Patients (“qolop”)
Kepak, Blatny et al.: The Brno Quality of Life Longitudinal Study of Pediatric Oncology Patients
“qolop” questionnaire set
Methods / Domains:• MMQL: health related QoL• Modified SQUALA: values + life satisfaction• CDI: emotion, depression scale• SAHA:
– daily routine, activities– abusus– parent – child intearctions
• HBSC: dietary habits, physical activity• Social support measure (based on several scales)• NEO-FFI: personality
Kepak, Blatny et al.: The Brno Quality of Life Longitudinal Study of Pediatric Oncology Patientsc

Health and Wellness questionnaire
Versions for age
brackets:
8 – 12 years
13 – 18 years
„mini“ version
Parents:
- QoL of the child
- impact on family life
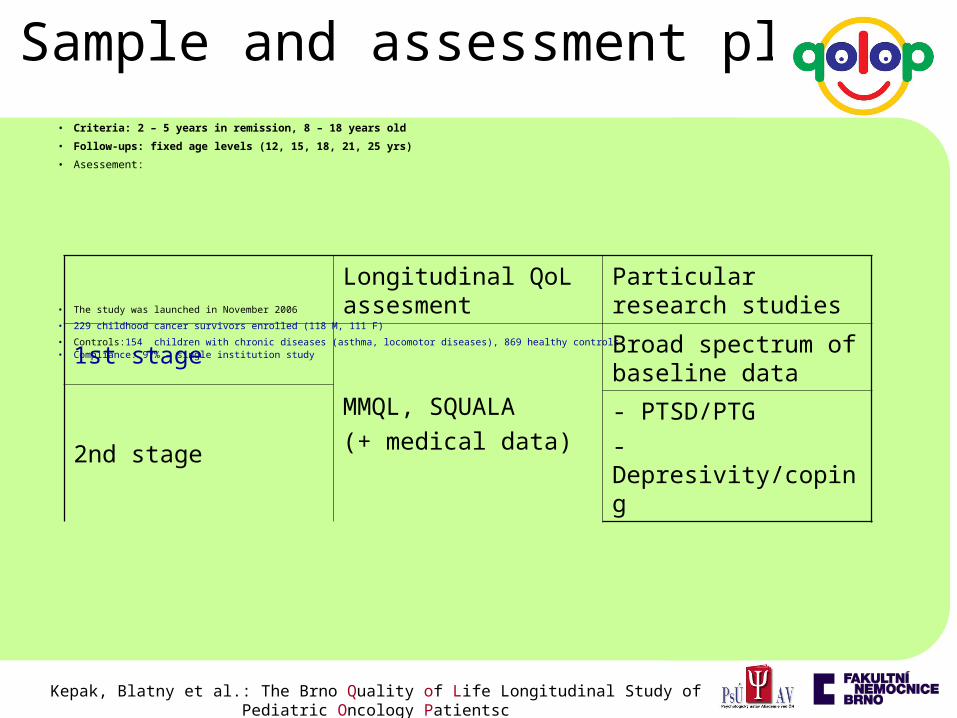
• Criteria: 2 – 5 years in remission, 8 – 18 years old
• Follow-ups: fixed age levels (12, 15, 18, 21, 25 yrs)
• Asessement:
• The study was launched in November 2006
• 229 childhood cancer survivors enrolled (118 M, 111 F)
• Controls:154 children with chronic diseases (asthma, locomotor diseases), 869 healthy controls• Compliance: 97% – single institution study
Longitudinal QoL assesment
Particular research studies
1st stage MMQL, SQUALA
(+ medical data)
Broad spectrum of baseline data
2nd stage - PTSD/PTG
- Depresivity/coping
Sample and assessment plan
Kepak, Blatny et al.: The Brno Quality of Life Longitudinal Study of Pediatric Oncology Patientsc
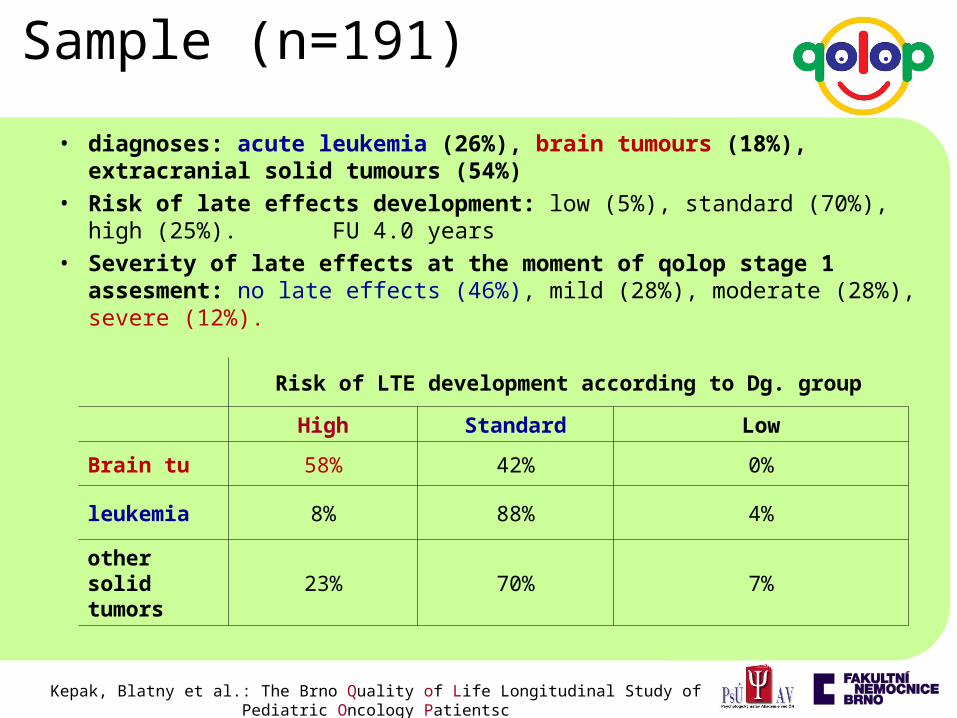
• diagnoses: acute leukemia (26%), brain tumours (18%), extracranial solid tumours (54%)
• Risk of late effects development: low (5%), standard (70%), high (25%). FU 4.0 years
• Severity of late effects at the moment of qolop stage 1 assesment: no late effects (46%), mild (28%), moderate (28%), severe (12%).
Sample (n=191)
Risk of LTE development according to Dg. group
High Standard Low
Brain tu 58% 42% 0%
leukemia 8% 88% 4%
other solid tumors
23% 70% 7%
Kepak, Blatny et al.: The Brno Quality of Life Longitudinal Study of Pediatric Oncology Patientsc

• Endocrinological late effects including growth problems, hypothyreosis, obesity
• amputations
• Vision impairment, hearing impairement
• Neurocognitive impairement
• Organopaties (kidney, lung, heart etc.)
Sample
Late effects present at the time of qolop stage 1 assesment (FU 4.0 years)
Brain tumors Leukemiaother solid
tumors
88% 25% 57%
Kepak, Blatny et al.: The Brno Quality of Life Longitudinal Study of Pediatric Oncology Patientsc

• Sample: 91 children and adolescents (44 M, 47 F), age 8-18
• Healthy controls (matched by sex and age, 3 random controls/1 survivor) - MANOVA
• Variables:
– Conventional involvement– Parent-child ineractions
• Parental INVOLVEMENT• Parental CONTROL • Parental WARMTH• INCONSISTENCY of parenting
– Depressivity– MMQL ( 8-12 y/o ) MMQL ( 13-18 y/o)
Kepak, Blatny et al.: The Brno Quality of Life Longitudinal Study of Pediatric Oncology Patients
Study 1 – comparison with healthy children and adolescents
Physical functioningCognitive functioningPsychological functioningSocial functioningIntimate relationshipsOutlook on life
Physical symptoms (e.g. I am having headaches)Physical functioning (e.g. I have enough energy) Psychological functioning (e.g. I feel lonely)Outlook on life (e,g, I am satisfied with the things how they are)
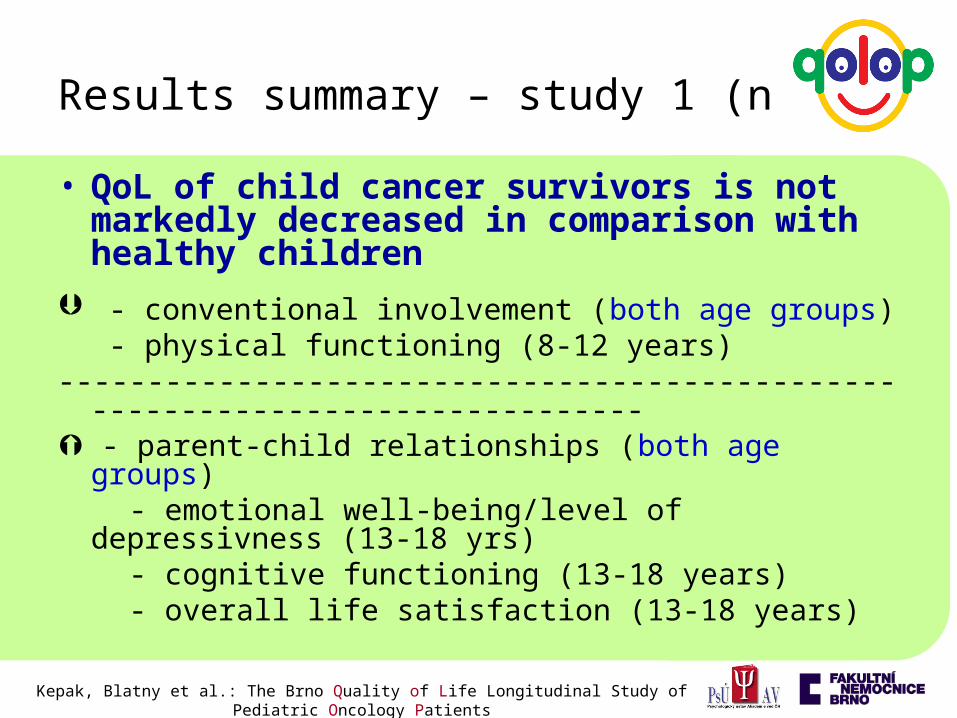
Results summary – study 1 (n=91)
• QoL of child cancer survivors is not markedly decreased in comparison with healthy children
- conventional involvement (both age groups) - physical functioning (8-12 years)
------------------------------------------------------------------------------ - parent-child relationships (both age groups) - emotional well-being/level of depressivness (13-18 yrs) - cognitive functioning (13-18 years) - overall life satisfaction (13-18 years)
Kepak, Blatny et al.: The Brno Quality of Life Longitudinal Study of Pediatric Oncology Patients
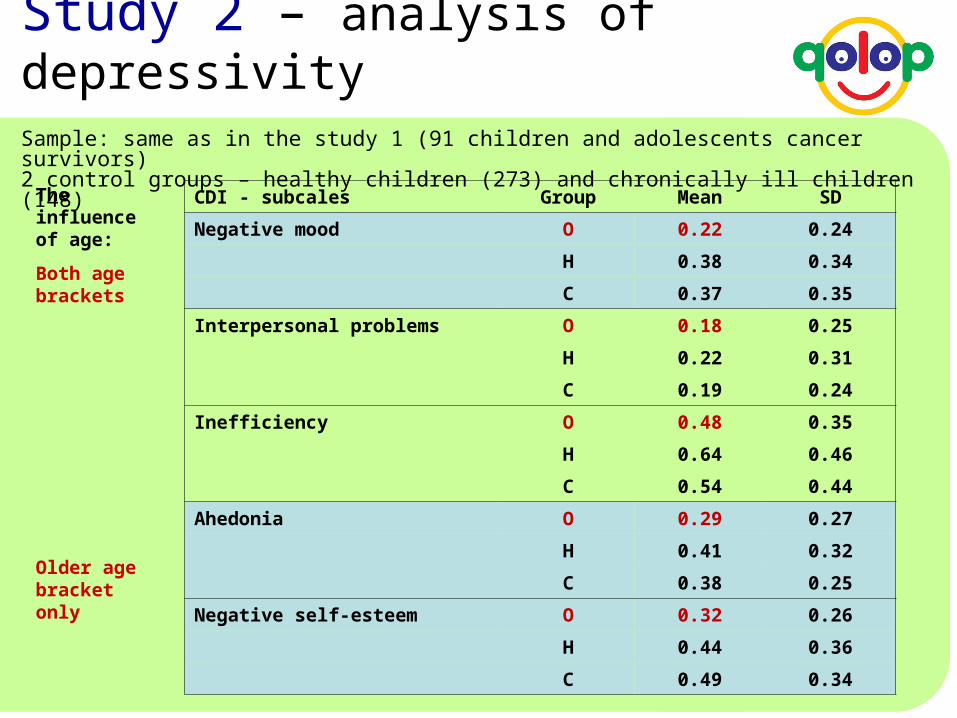
CDI - subcales Group Mean SD
Negative mood O 0.22 0.24
H 0.38 0.34
C 0.37 0.35
Interpersonal problems O 0.18 0.25
H 0.22 0.31
C 0.19 0.24
Inefficiency O 0.48 0.35
H 0.64 0.46
C 0.54 0.44
Ahedonia O 0.29 0.27
H 0.41 0.32
C 0.38 0.25
Negative self-esteem O 0.32 0.26
H 0.44 0.36
C 0.49 0.34
The influence of age:
Both age brackets
Older age bracket only
Sample: same as in the study 1 (91 children and adolescents cancer survivors) 2 control groups – healthy children (273) and chronically ill children (148)
Study 2 – analysis of depressivity
8 - 12 y/o Diagnosis
Brain tumours leukemia other solid tumorsKruskal-Wallis
md md md χ2 p
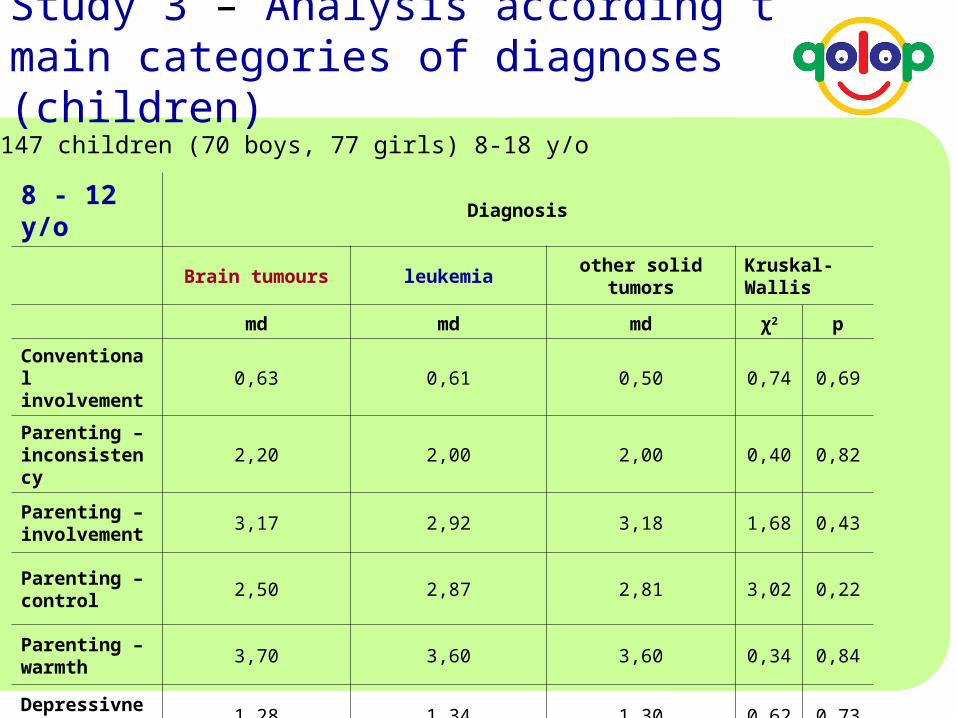
Conventional involvement
0,63 0,61 0,50 0,74 0,69
Parenting – inconsistency
2,20 2,00 2,00 0,40 0,82
Parenting – involvement
3,17 2,92 3,18 1,68 0,43
Parenting – control
2,50 2,87 2,81 3,02 0,22
Parenting – warmth
3,70 3,60 3,60 0,34 0,84
Depressivness 1,28 1,34 1,30 0,62 0,73
Study 3 – Analysis according to main categories of diagnoses (children)
Sample: 147 children (70 boys, 77 girls) 8-18 y/o

MMQL Diagnosis
(8–12 y/o) Brain tumours leukemia other solid tumorsKruskal-Wallis
md md md χ2 p
Life satisfaction 3,20 3,25 3,44 0,48 0,79
Physical symptoms
1,42 1,50 1,45 0,32 0,85
Physical functioning
2,83 2,83 3,00 1,94 0,38
Psychological functioning
2,87 3,00 2,94 0,59 0,75
Kepak, Blatny et al.: The Brno Quality of Life Longitudinal Study of Pediatric Oncology Patients
Study 3 – Analysis according to main categories of diagnoses (children)
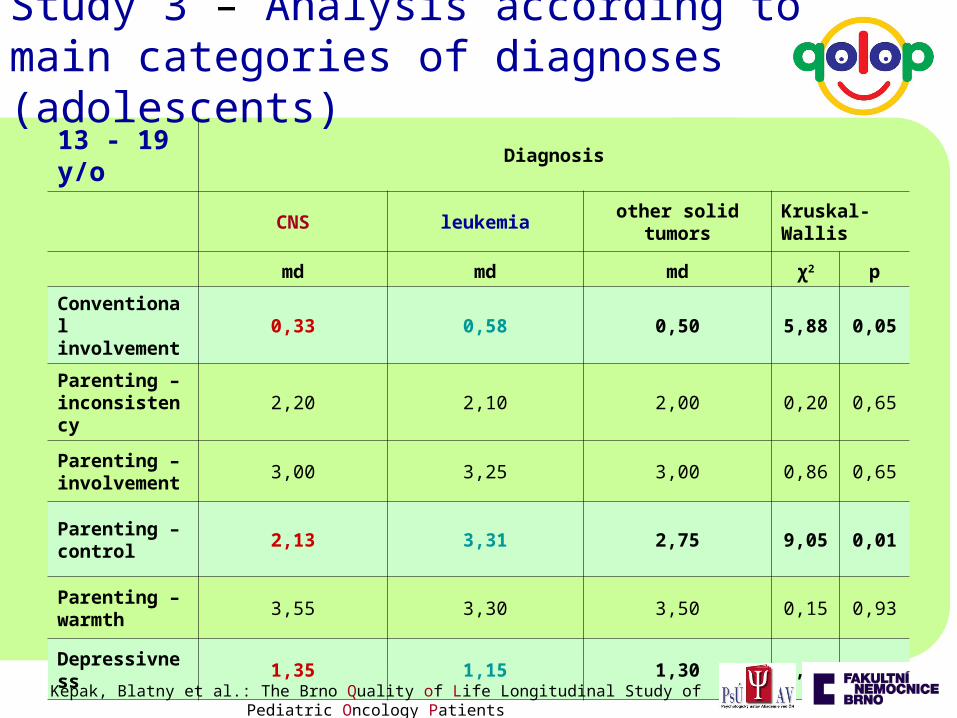
13 - 19 y/o Diagnosis
CNS leukemia other solid tumorsKruskal-Wallis
md md md χ2 p
Conventional involvement
0,33 0,58 0,50 5,88 0,05
Parenting – inconsistency
2,20 2,10 2,00 0,20 0,65
Parenting – involvement
3,00 3,25 3,00 0,86 0,65
Parenting – control
2,13 3,31 2,75 9,05 0,01
Parenting – warmth
3,55 3,30 3,50 0,15 0,93
Depressivness 1,35 1,15 1,30 6,63 0,04
Kepak, Blatny et al.: The Brno Quality of Life Longitudinal Study of Pediatric Oncology Patients
Study 3 – Analysis according to main categories of diagnoses (adolescents)

MMQL (13–18) Diagnosis
CNS leukemia other solid tumors Kruskal-Wallis
md md md χ2 p
Physical functioning
3,28 4,13 3,78 7,23 0,03
Cognitive functioning
3,67 4,11 4,00 1,48 0,48
Psychological functioning
3,94 4,17 3,89 3,49 0,17
Body image 3,67 4,50 4,00 10,15 0,01
Social functioning
3,83 4,50 4,00 8,34 0,02
Life satisfaction 3,33 4,17 4,33 10,06 0,01
Intimate relationships
3,25 4,00 3,75 7,65 0,02
Kepak, Blatny et al.: The Brno Quality of Life Longitudinal Study of Pediatric Oncology Patients
Study 3 – Analysis according to main categories of diagnoses (adolescents)
• QoL of cancer survivors doesn´t differ much compared to healthy children and adolescents, in some areas cancer survivors report even better QoL (PTSD +/- PTG)
• Brain tumour survivors most impacted• Most differences in QoL (both among dg. groups as well as
compared to healthy controls) in older age bracket (adolescents – 13-18 y/o)
• They differ mainly in social functioning & intimate relationships (including satisfaction with her/his body development) as well as in physical functioning (including conventional involvement)
• Low level of depressivity – ambiguity of the interpretation
• QoL is a dynamic variable, changes over the time, necessitating an individual approach respecting a developmental stage of each given individual
• QoL depends on presence/severity of late effects• Further research needed …………
Kepak, Blatny et al.: The Brno Quality of Life Longitudinal Study of Pediatric Oncology Patients
Conclusions

PanCare QoL Longitudinal survey?
• Is there a need of study on QoL within PanCare/ENCCA umbrella?
• Background: Paucity of longitudinal studies
x most appropriate setting
• Brno expertise (Czech Academy of Sciences, Institute of Psychology)
– Qolop since 2006 (250)
– SAHA (national probability sample 5000)
– Lifespan development since 1961
• Plan for Amsterdam PanCare meeting?
- methods? (e.g. MMQL based?)
- willing to participate (on-line questionnaire to PanCare members?)
- multicenter study x national samples?
……plenary discussion