quality follow up programme in primary care. experiences from västra götaland
DESCRIPTION
Quality follow up programme in primary care. Experiences from Västra Götaland what have we learned? Staffan Björck, Analysenheten, Regionkansliet, Västra Götalandsregion. Region Västra Götaland 1.5 mil. Inhab. 16% of Sweden. Göteborg. Västra Götalandsregionen. - PowerPoint PPT PresentationTRANSCRIPT

• Quality follow up programme in primary care. Experiences from Västra Götaland
what have we learned?
Staffan Björck, Analysenheten, Regionkansliet, Västra Götalandsregion

Region Västra Götaland1.5 mil. Inhab.16% of Sweden
Göteborg

Västra Götalandsregionen
• financing, primary care centres:
• Capitation, listed patients• Age and gender• ACG, adjusted clinical groups• CNI, care need index• Distance to hospital
– P4P (quality)• initially 3 % with aim to increase• 4,3 % 2011

Number of patients with diabetes in regional database
Effect of ACG on reporting of diagnoses
0
10 000
20 000
30 000
40 000
50 000
60 000
70 000
2005
2006
2007
2008
2009
2010
patie
nts
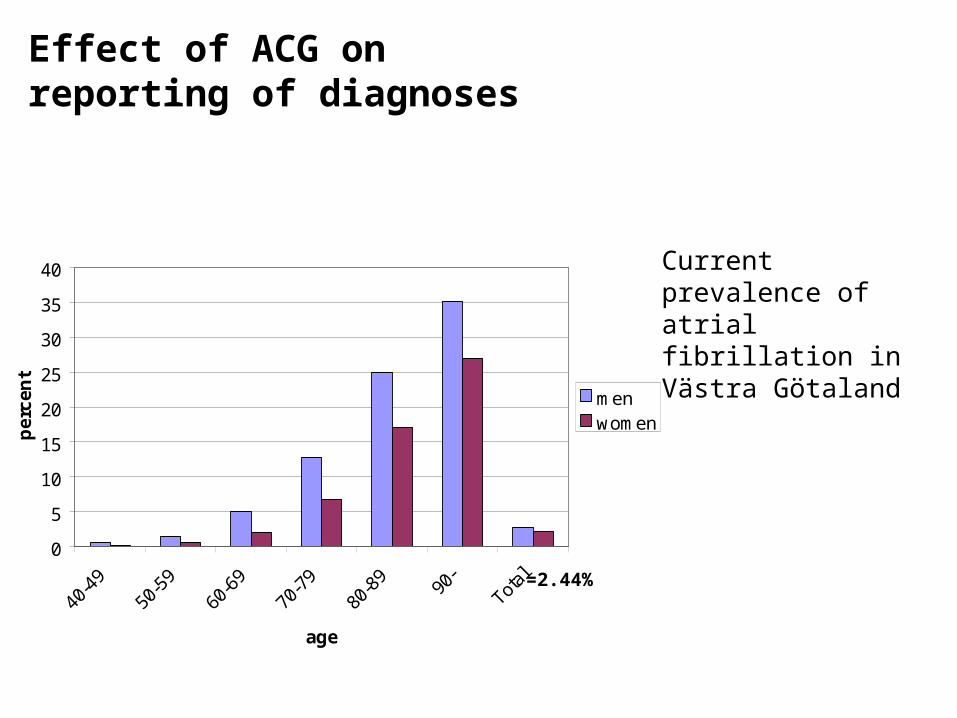
Current prevalence of atrial fibrillation in Västra Götaland
Effect of ACG on reporting of diagnoses
0
5
10
15
20
25
30
35
40
40-
49
50-
59
60-
69
70-
79
80-
89 90-
Total
age
pe
rcen
t
menwomen
=2.44%
Follow up quality of care
• Identify indicators
• System for payment for performance
How to do it?Learn from others
Develop your own version

• Learn from others– Reports on Swedish experiences– International experience

Most common Indicators for P4P in Sweden, Anell 2009
måttCounties
nAdherence to drug recommendations 11Access by telephone 10Diabetic patients in national registry 9Patients visits to own centre 9Right choice of UTI antibiotics 7Prescription of physical activity 5Choice of least expensive BP lowering drug 4
”It is clear that there is a need for better follow up systems for primary care in Sweden and there is a great potential for cooperation between counties”

How to select indicators?
Q-indicators
PaymentResults to bemade public Medical audit
Useful informationto centres
Principles 1

Principles 2
• Quality indicators– Automated data collection– Evidence based– Avoid ”how”, focus on results – As few as possible but enough to
give meaningful information– Enough measures to spread
economic risk

Principles 3 What do they do in primary care and what is
important?
0
50 000
100 000
150 000
200 000
250 000
300 000
<1 1 >1-2 >2-4 >3-4 >4
antal läk.besök/år vuxna
ind
ivid
er
Satis
fact
ion, w
ait
times
, dru
g choic
e
etc
Chronic
dis
ease
≈ 50 % rare visitors
≈ 50 % chronic disease
Number of doctors visits during 2 years
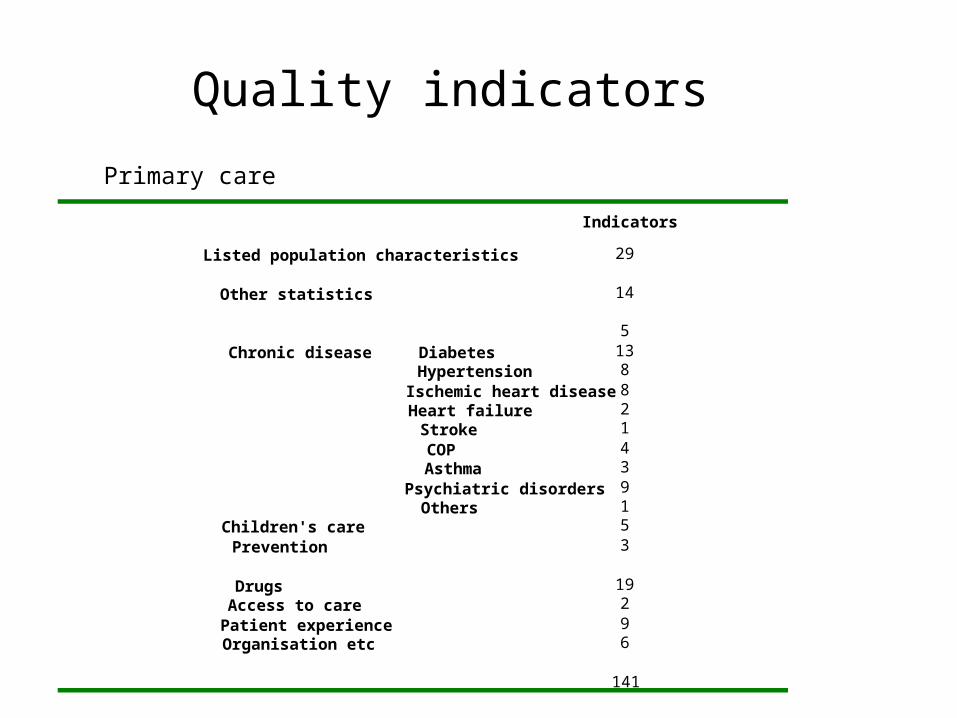
Quality indicators
Primary care
29
14
5138821439153
19296
141
Indicators
Listed population characteristics
Other statistics
Chronic disease DiabetesHypertensionIschemic heart diseaseHeart failureStrokeCOPAsthmaPsychiatric disordersOthers
Children's care Prevention
Drugs Access to carePatient experience Organisation etc

Indicators, Diabetes Primary care
regi
stra
tion
resu
ltsIndicator
1 Registration national database
2 Blood pressure3 Smoking4 HbA1c5 LDL-kolesterol6 Albuminuria7 Target for HbA1c8 Target for HbA1c, recent onset9 Target for Blood pressure
10 Target for LDL-cholesterol
11 Patient education
12 Integrated care
13 Influenza immunisation

Principles P4Pexample diabetes
High/low limits
Weight
Limits Relativepoints
Registration national database 70-90 5
Registration blood pressure
80-95 0,5
Registration blood pressure 70-90 0,5 Registration HbA1c 80-95 0,5 Registration LDL-cholesterol 50-80 0,5 Registration albuminuri 70-90 0,5
Target for HbA1c 45-65 0,5 Target for blood pressure 30-50 0,5 Target for LDL-cholesterol- 35-50 1 sum 9,5
• Principles– pay for registration– Relative weights– No sharp thresholds– Spread of economic
risk
+ 4 other indicators without P4P

• Differences vs NHS example– No exception reporting– Targets more difficult to reach– Much lower financial incentive– Focus on registration to give high quality feed
back of results

0
10
20
30
40
50
60
70
80
perc
ent
0
10
20
30
40
50
60
70
80p
erc
en
t
ExamplesResults
Influenza immunisation, patients 65+
Children with antibiotic prescriptions/ year
P4P range
Each dot = a primary care center, with confidence intervals

Webb access to results
160 000patients

• Main data sources– National diabetes registry– Regional Primary care quality registry – Drug prescription registry – Regional database for contacts– Swedish vaccination registry– Manual reporting

The regional primary care quality registry
• Automated data collection from local patient files– Ischemic heart disease– Hypertension– COP– Asthma– Diabetes
• Monthly update and back-reporting to centres

Interaction between diseases, primary care register
Hypertension
198 238
Diabetes 65 730
Ischemic. Heart disease
44 317
58 %
9 %
14 %
6 %
1 % 3 %
8 %
Total 239 349

• P4P – 41 indicators
• How to pay? 3 principles – Decided standard– Professional recommendations– Statistical limits
• For example 25 % full payment, 25 % no payment

Diabetes registry. Proportion reaching target for LDL-kolesterol (<2,5 mmol/l)
Targets for payment?
Statistical limits
0
10
20
30
40
50
60
70
80
90
100
pe
rce
nt
Each dot = a primary care center

• Example of difficulties, P4P– Professional scepticism– Patient groups to small for reliable
comparisons– Data sources have to be created– Leads to focus on money, not on results,
wrong focus– Resource consuming technical solutions

• Lessons learned– P4P just one small part of quality improvement programme – Focus on pay for registration, – < 4% of total payment– Involve profession!– Easy access to results– Must be combined with continuous analysis and discussion,
reports, seminars etc. Professional dialogue. – Transaction cost– National cooperation
• National primary care register• Cooperation between local quality registers
