radiotherapy planning - videoserver1.iaea.org · proton radiation therapy for retinoblastoma:...
TRANSCRIPT

IAEA Pediatric Radiation Oncology TrainingDr Laskar Version 1 June 2009
PEDIATRIC ORBITAL TUMORS
RADIOTHERAPY PLANNING

IAEA Pediatric Radiation Oncology TrainingDr Laskar Version 1 June 2009
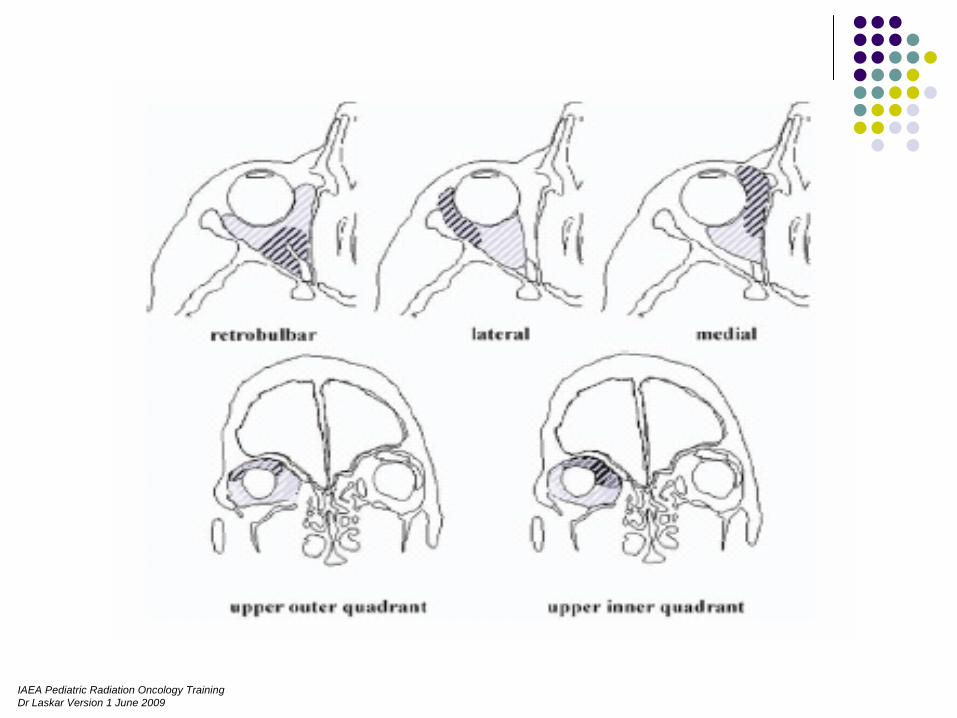
ANATOMY
IAEA Pediatric Radiation Oncology TrainingDr Laskar Version 1 June 2009
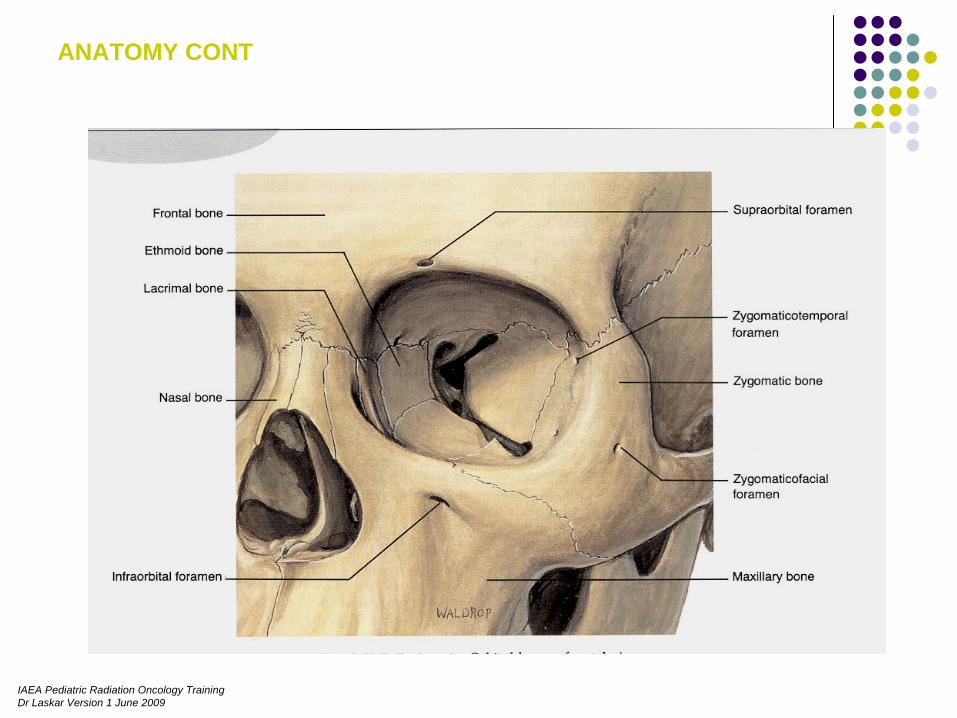
ANATOMY CONT

IAEA Pediatric Radiation Oncology TrainingDr Laskar Version 1 June 2009
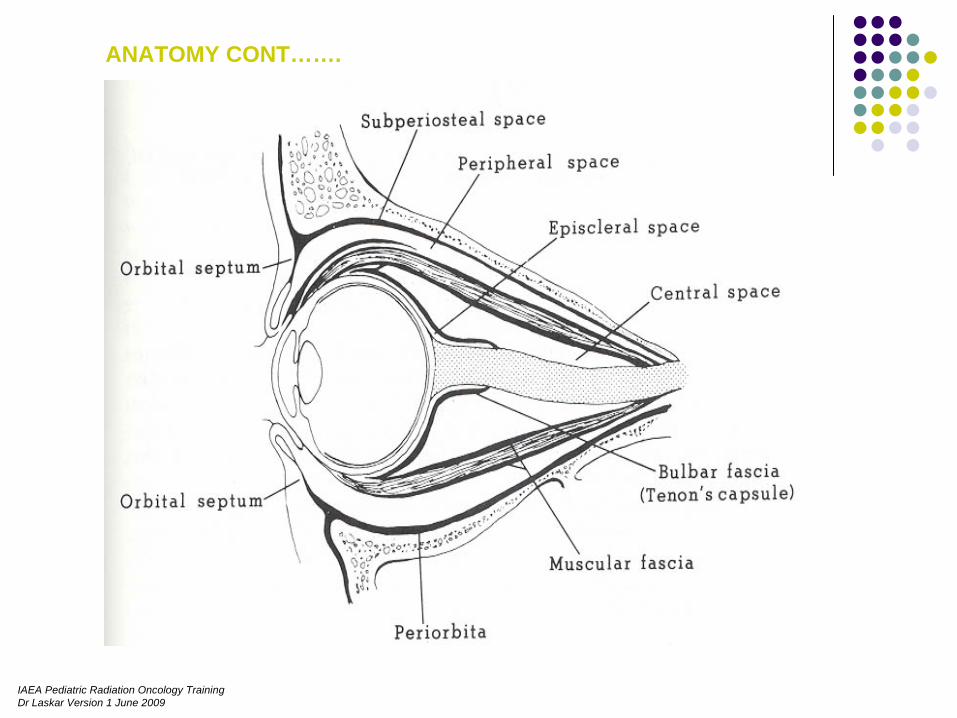
ANATOMY CONT…….
IAEA Pediatric Radiation Oncology TrainingDr Laskar Version 1 June 2009
ANATOMY CONT…….
IAEA Pediatric Radiation Oncology TrainingDr Laskar Version 1 June 2009
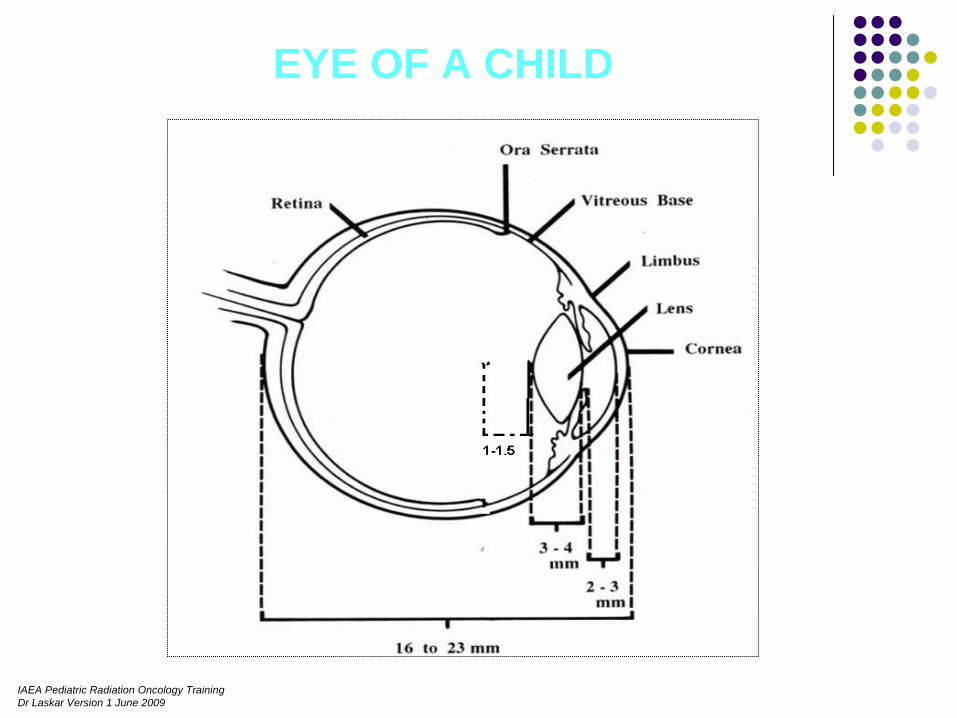
EYE OF A CHILD
IAEA Pediatric Radiation Oncology TrainingDr Laskar Version 1 June 2009
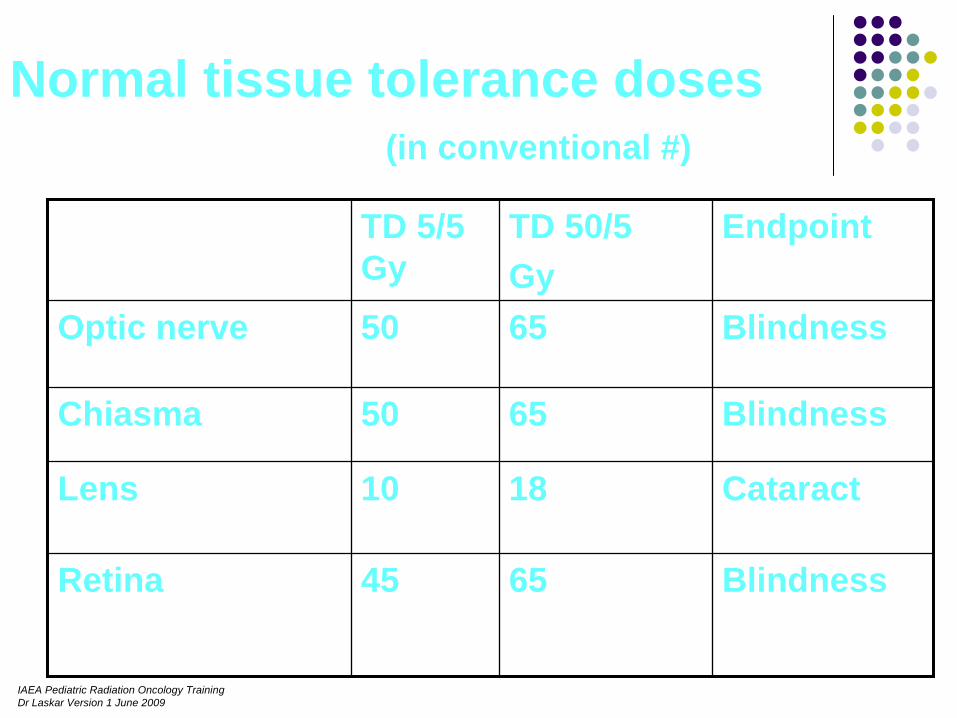
Normal tissue tolerance doses (in conventional #)
TD 5/5 Gy
TD 50/5 Gy
Endpoint
Optic nerve 50 65 Blindness
Chiasma 50 65 Blindness
Lens 10 18 Cataract
Retina 45 65 Blindness

IAEA Pediatric Radiation Oncology TrainingDr Laskar Version 1 June 2009
COMMON PEDIATRIC ORBITAL TUMORS
Intraocular Tumors Intraorbital Tumors
_ Retinoblastoma - Rhabdomyosarcoma_ Uveal Melanoma - Lymphoma
_ Metastasis - Optic Nerve Glioma
- Optic nerve sheath
meningioma
- Metastasis

IAEA Pediatric Radiation Oncology TrainingDr Laskar Version 1 June 2009
Rhabdo- myosarcoma
Most common orbital malignant tumor
IAEA Pediatric Radiation Oncology TrainingDr Laskar Version 1 June 2009
When To Treat ?Age
- > 1 yr- < 1 yr
Extent of disease at presentation.- Localised to Orbit - Orbit with
intracranial extension

IAEA Pediatric Radiation Oncology TrainingDr Laskar Version 1 June 2009
PLANNING ……..

IAEA Pediatric Radiation Oncology TrainingDr Laskar Version 1 June 2009
IMMOBILIZATIONThermoplastic mould Vacuum bagSedation General anesthesia
Planning CT scan ~ 3mm cuts
IAEA Pediatric Radiation Oncology TrainingDr Laskar Version 1 June 2009
RADIOTHERAPY PLANNING……….Depending upon
SITE to be treated
DEPTH to be treated
How to plan ?
IAEA Pediatric Radiation Oncology TrainingDr Laskar Version 1 June 2009
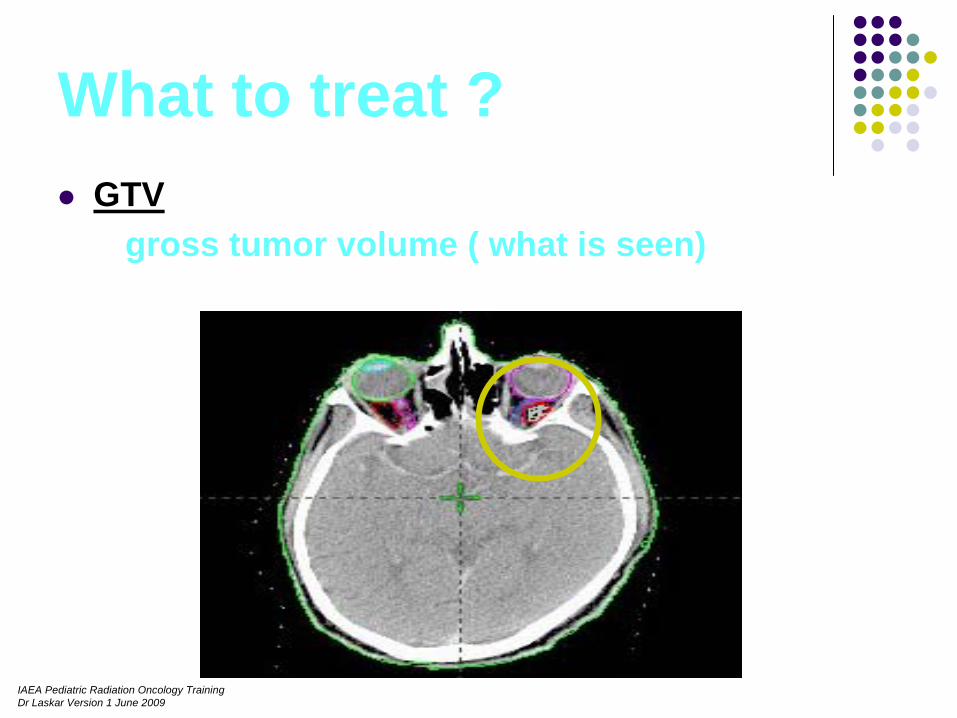
What to treat ?GTV
gross tumor volume ( what is seen)
IAEA Pediatric Radiation Oncology TrainingDr Laskar Version 1 June 2009
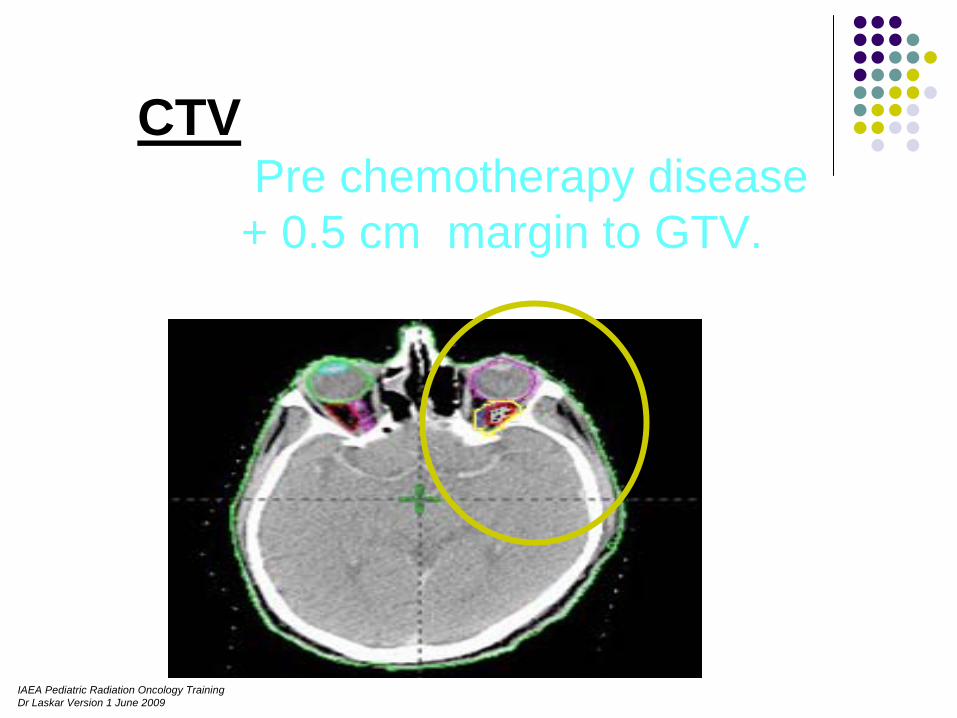
CTV Pre chemotherapy disease
+ 0.5 cm margin to GTV.
IAEA Pediatric Radiation Oncology TrainingDr Laskar Version 1 June 2009
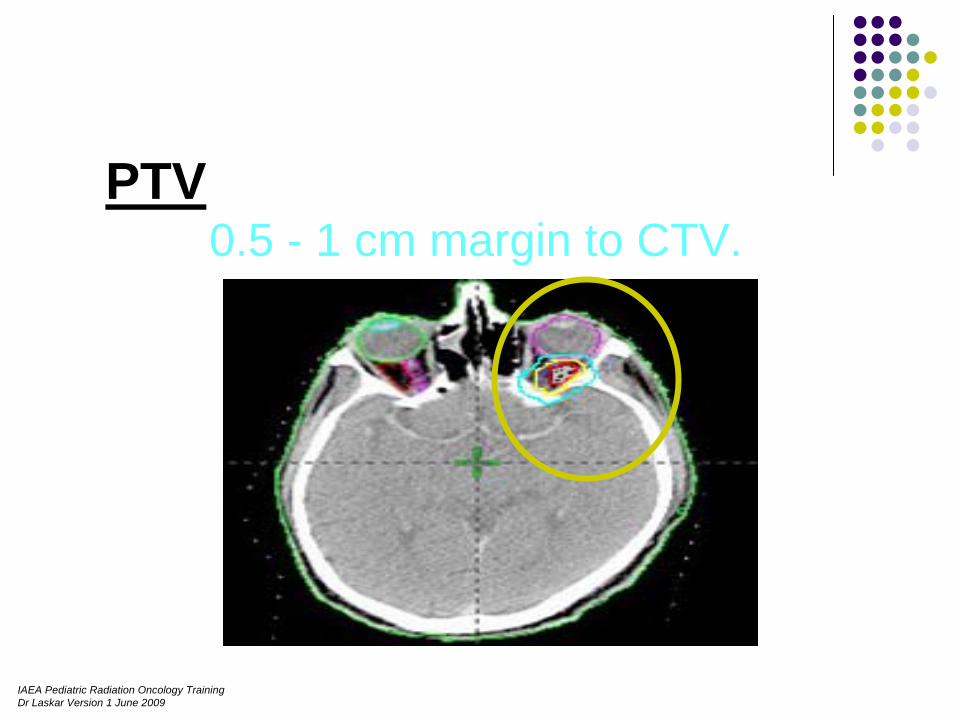
PTV 0.5 - 1 cm margin to CTV.

IAEA Pediatric Radiation Oncology TrainingDr Laskar Version 1 June 2009
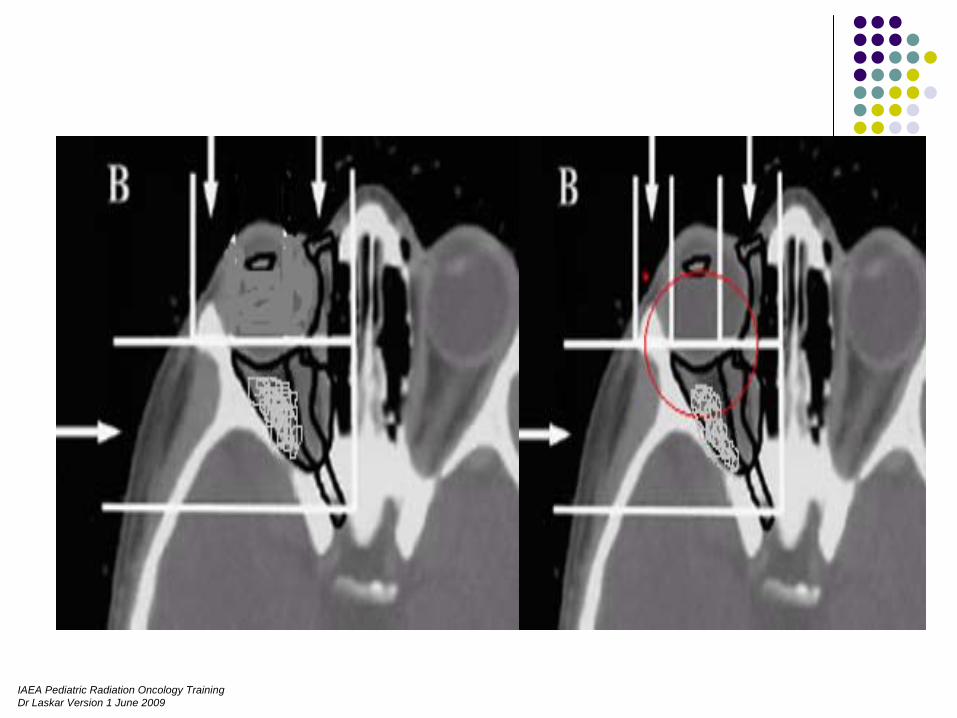
BEAM ARRANGEMENT
IAEA Pediatric Radiation Oncology TrainingDr Laskar Version 1 June 2009
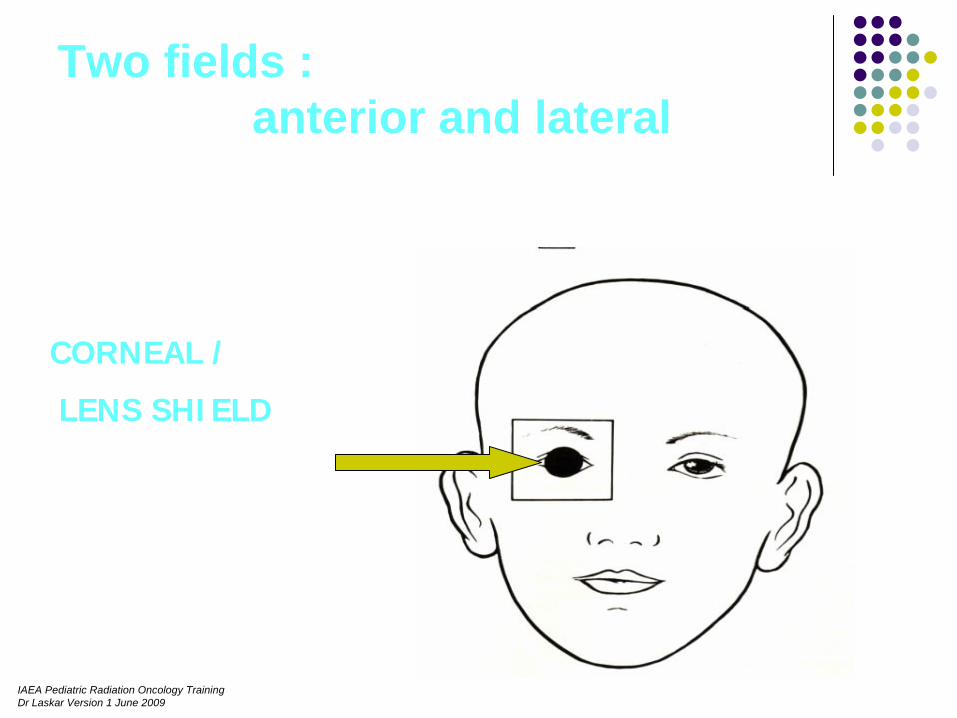
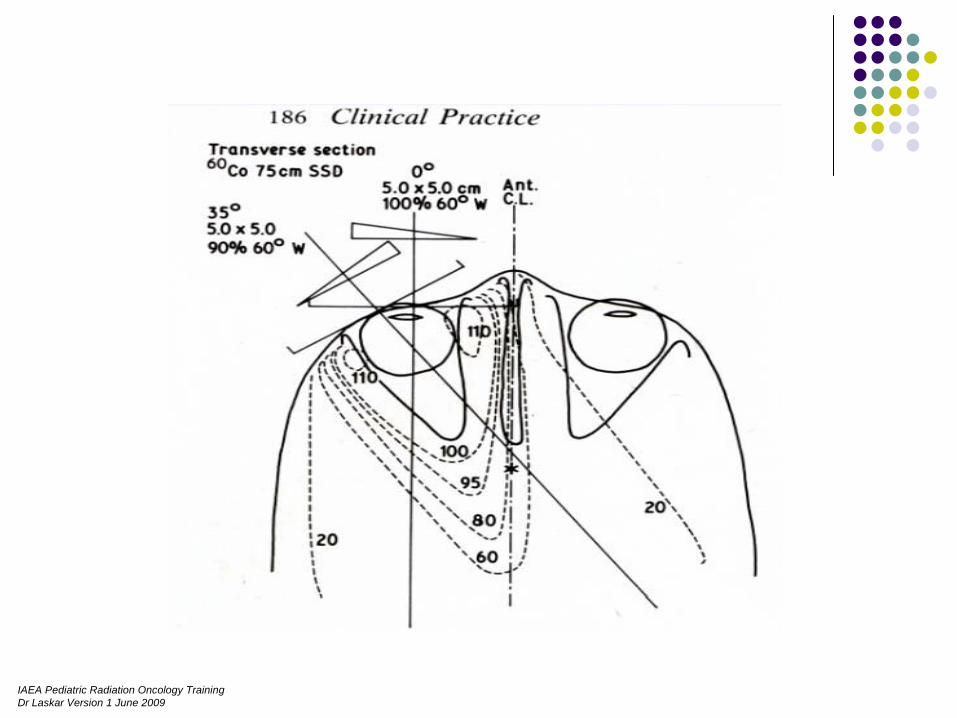
Two fields : anterior and lateral
CORNEAL /
LENS SHIELD
IAEA Pediatric Radiation Oncology TrainingDr Laskar Version 1 June 2009
IAEA Pediatric Radiation Oncology TrainingDr Laskar Version 1 June 2009
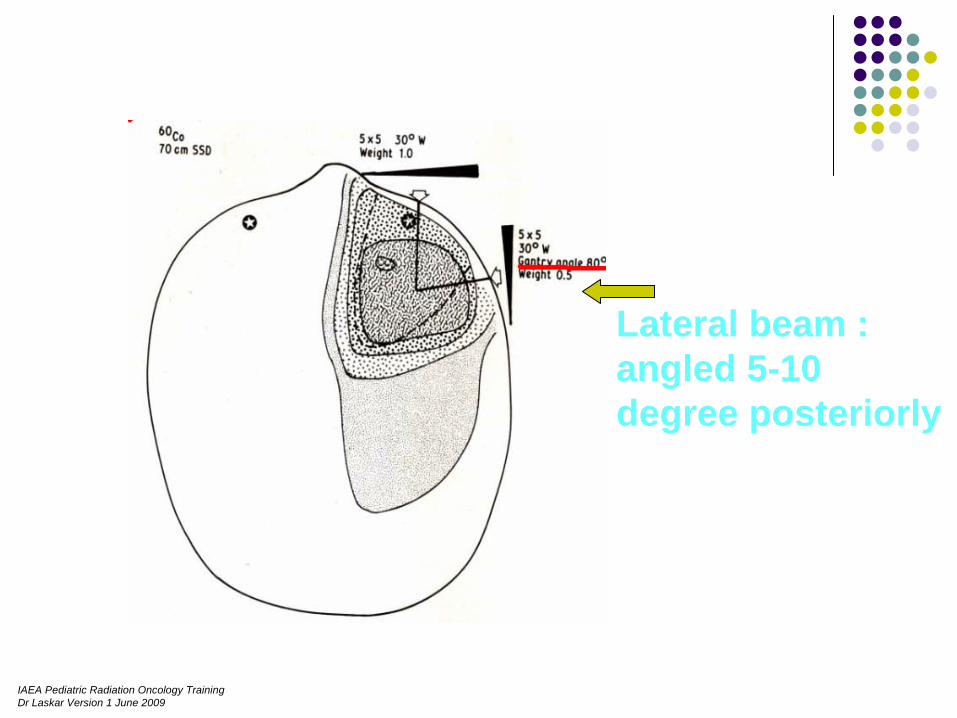
Lateral beam : angled 5-10 degree posteriorly
IAEA Pediatric Radiation Oncology TrainingDr Laskar Version 1 June 2009
IAEA Pediatric Radiation Oncology TrainingDr Laskar Version 1 June 2009
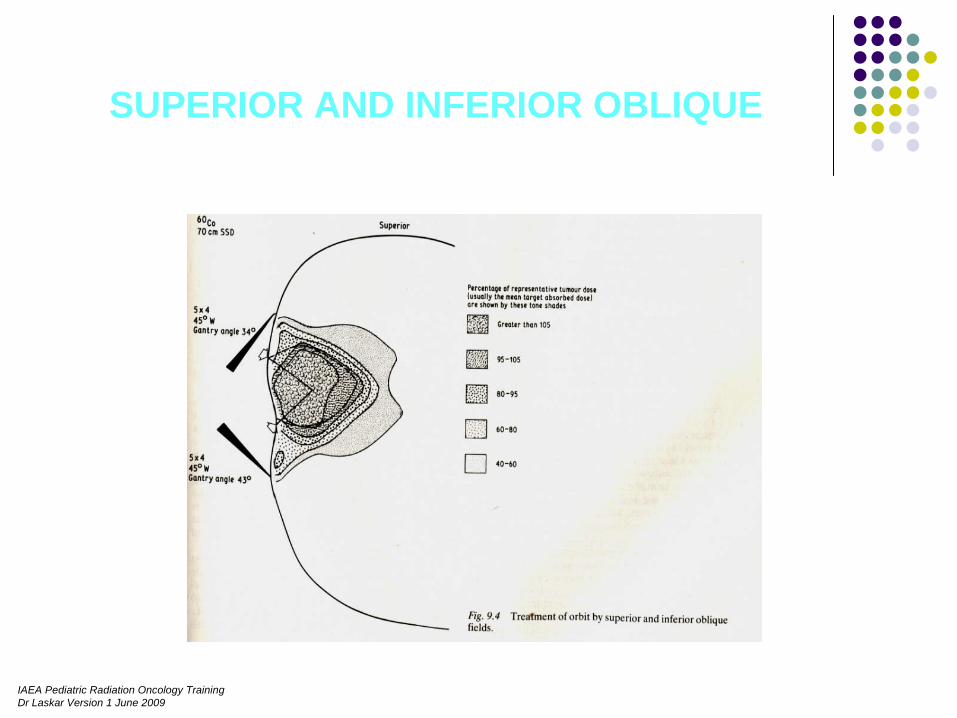
SUPERIOR AND INFERIOR OBLIQUE
IAEA Pediatric Radiation Oncology TrainingDr Laskar Version 1 June 2009

IAEA Pediatric Radiation Oncology TrainingDr Laskar Version 1 June 2009
Medial obliques
IAEA Pediatric Radiation Oncology TrainingDr Laskar Version 1 June 2009
Electron beam
Single anterior electron beam.
Combined electron –photon beam.
IAEA Pediatric Radiation Oncology TrainingDr Laskar Version 1 June 2009
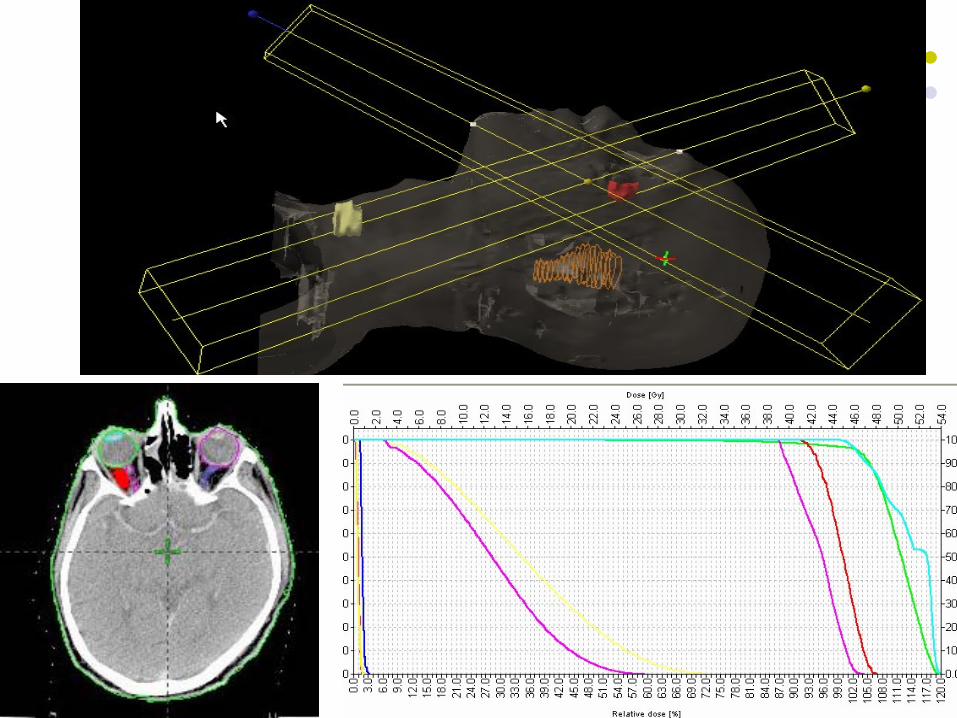
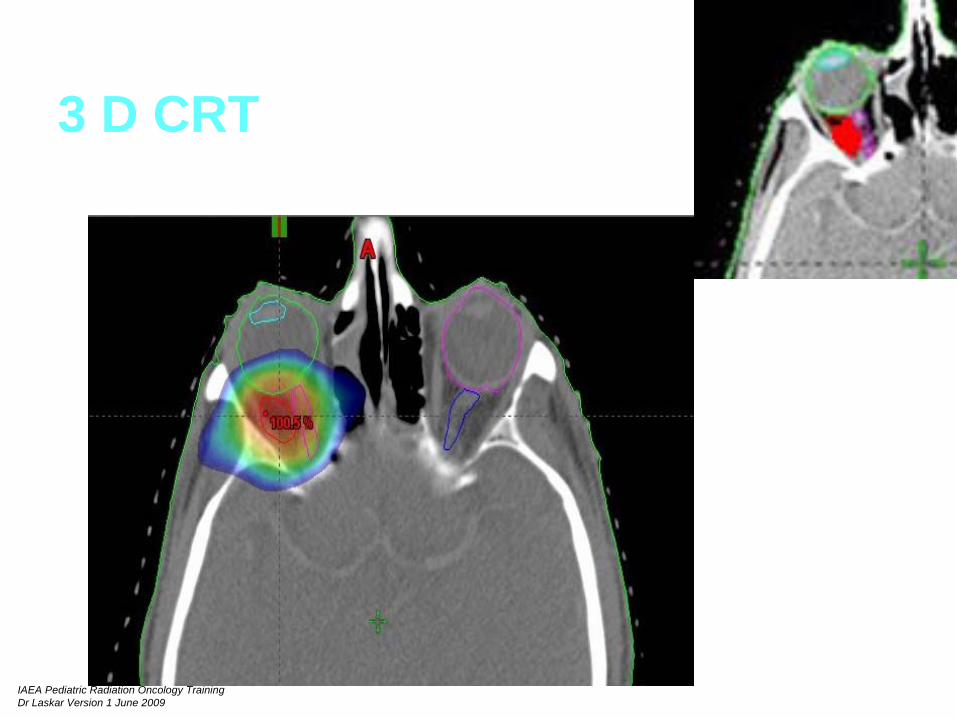
3 D CRT

IAEA Pediatric Radiation Oncology TrainingDr Laskar Version 1 June 2009
IAEA Pediatric Radiation Oncology TrainingDr Laskar Version 1 June 2009
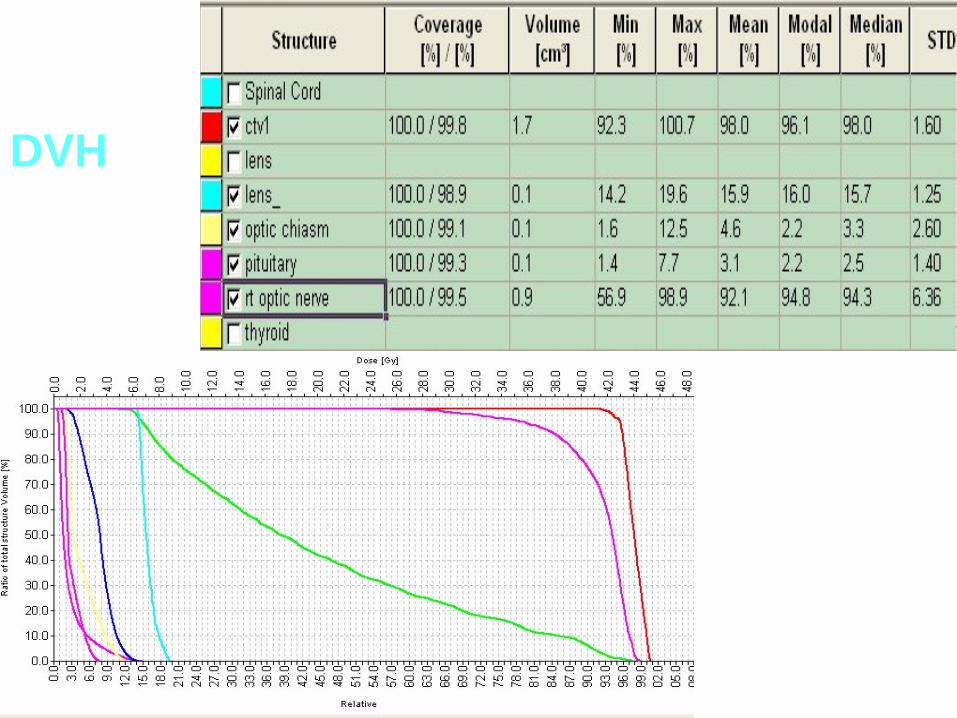
DVH
IAEA Pediatric Radiation Oncology TrainingDr Laskar Version 1 June 2009
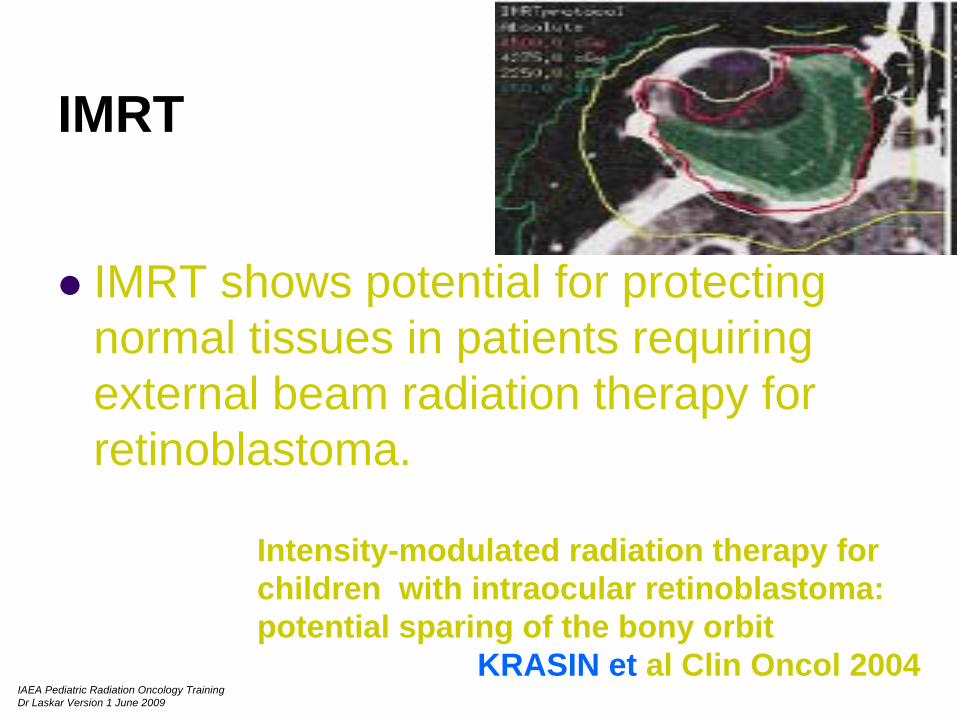
IMRT
IMRT shows potential for protecting normal tissues in patients requiring external beam radiation therapy for retinoblastoma.
Intensity-modulated radiation therapy for children with intraocular retinoblastoma: potential sparing of the bony orbit
KRASIN et al Clin Oncol 2004
IAEA Pediatric Radiation Oncology TrainingDr Laskar Version 1 June 2009
IAEA Pediatric Radiation Oncology TrainingDr Laskar Version 1 June 2009
IAEA Pediatric Radiation Oncology TrainingDr Laskar Version 1 June 2009
IAEA Pediatric Radiation Oncology TrainingDr Laskar Version 1 June 2009

IAEA Pediatric Radiation Oncology TrainingDr Laskar Version 1 June 2009
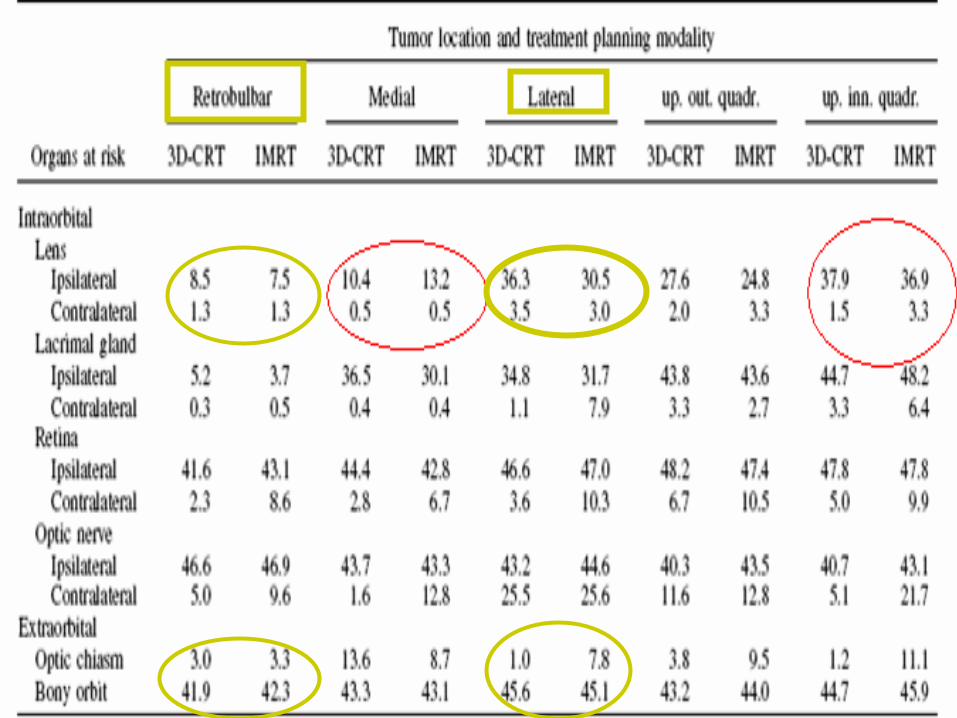
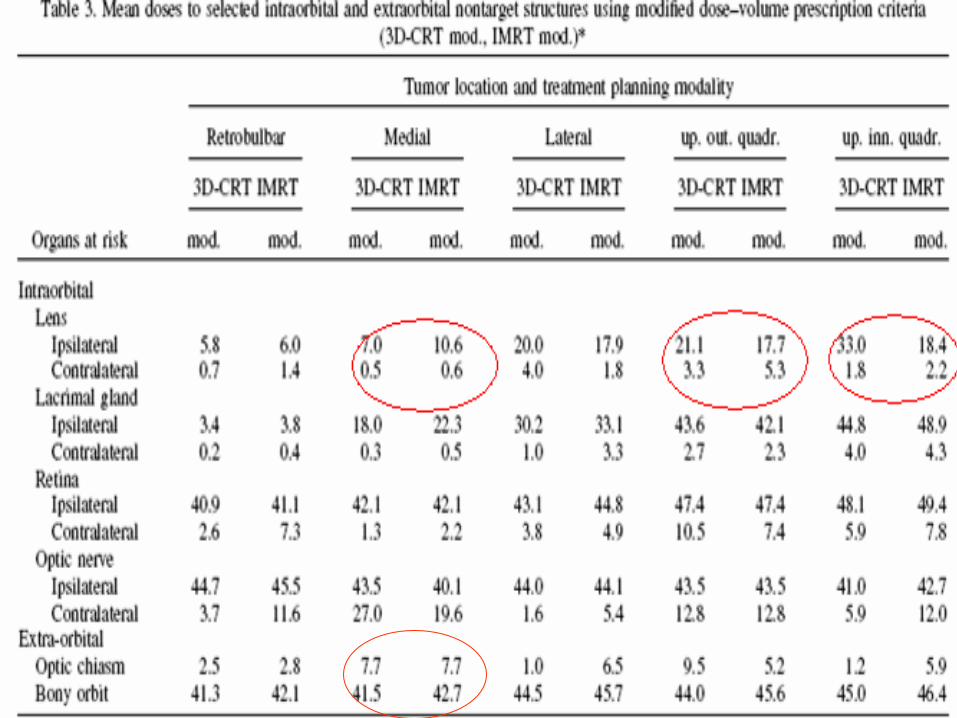
Conclusion :
,IMRT planning significantly reduced lens doses. This was not accomplished to the same degree with 3D-CRT.
Our study underlines the importance of appropriate selection of planning objectives to maximize the specific capabilities and advantages of IMRT in terms of sufficient target coverage and simultaneous sparing of critical structures.
IAEA Pediatric Radiation Oncology TrainingDr Laskar Version 1 June 2009

IAEA Pediatric Radiation Oncology TrainingDr Laskar Version 1 June 2009
stereotactic radiation therapy
fractionated stereotactic radiation therapy of uveal melanoma results in excellent local control with only mild side effects
.
Karin Muller M.D.IJROBP63(1)2005 116-122
IAEA Pediatric Radiation Oncology TrainingDr Laskar Version 1 June 2009
Stereotactic radiosurgery as a salvage treatment for recurrent skul base adenoied cystic carcinoma
Yoshimasa MORI , STEREOTACTIC AND FUNCTIONAL NEUROSURGERY 2006

IAEA Pediatric Radiation Oncology TrainingDr Laskar Version 1 June 2009
PROTON BEAM THERAPY
IAEA Pediatric Radiation Oncology TrainingDr Laskar Version 1 June 2009
Proton radiation therapy for retinoblastoma: Comparison of various intraocular tumor locations and beam arrangements
KRENGLI Marco
. Doses of 46 cobalt grey equivalent (CGE) to gross tumor volume (GTV) and 40 CGE to clinical target volume (CTV).
. The anterolateral oblique approach with an intrarotated eye resulted in additional reduction of bony volume and exposure of only one growth center.No appreciable dose was delivered to the contralateral eye, brain tissue, or pituitary gland. Conclusions: Proton therapy achieved homogeneous target coverage with true lens sparing. Doses to orbit structures, including bony growth centers, were minimized with different beam arrangements and eye positions.Proton therapy could reduce the risks of second malignancy and cosmetic and functional sequelae.
IGROBP 2005
IAEA Pediatric Radiation Oncology TrainingDr Laskar Version 1 June 2009
Lymph node irradiation
Pre-auricular / upper deep cervical ~ 20%
IAEA Pediatric Radiation Oncology TrainingDr Laskar Version 1 June 2009
Radiation DoseRetinoblastoma
Radical : ~ 45 Gy / 25 #Post operative : ~ 40 Gy / 25 #Palliative 30Gy / 10 #
Rhabdomyosarcoma Radical : >/= 55 Gy ( conventional # )41.5 Gy + 10 Gy
Lymphoma : 20-25 Gy/30 -35 Gy (conventional #) Optic nerve gloima : 50–54 Gy (conventional # )Metastatic disease : ~ 30Gy / 2 wks, 8 – 10 Gy / 1 wk, 10x3 / 5x4Leukemic retinopahy : 10 – 15 Gy / 4- days
IAEA Pediatric Radiation Oncology TrainingDr Laskar Version 1 June 2009
Re-irradiationConservation treatment of the eye: Conformal proton reirradiation for recurrent uveal melanoma.
31 patienttotal doses between 118 and 140 CGE 20 NED , 9 enucleationMarucci L IJROBP. 2006 Mar 15;64(4):1018-22
.
Radiotherapy for localised relapse in patient with NHL
Katsumasa, Radiation Medicine ,2000
IAEA Pediatric Radiation Oncology TrainingDr Laskar Version 1 June 2009
Complication post radiotherapy
Radiation induced Second malignant neoplasmwithin RT field ………..
_ Osteosarcoma / fibrosarcoma / other spindle cell sarcoma / malignant melanoma / thyroid carcinoma
Incidence : Abramson et al 198520% - 10 yr
50% - 20 yr 90 % - 30 yr
Facial / orbital deformitiesShort strature / precocious puberty
IAEA Pediatric Radiation Oncology TrainingDr Laskar Version 1 June 2009
Ophthalmic :
Dry eye> 30Gy/ 3wks
Corneal damage>50 Gy/ 5wks
Cataractopacities >200rad,cataract >800 rads
Retinal damage>50 Gy / 5 wks
Radiation recall phenomenon