raouf (ron) gharbo d.o. voma spring conference 2010 williamsburg, virginia
TRANSCRIPT

Raouf (Ron) Gharbo D.O.VOMA Spring Conference 2010Williamsburg, Virginia


A personal and unreasoned judgment. Merriam-Webster
One commercial break for our sponsor
Not looking for more Fibromyalgia referrals

What is your definition of Management?
Does it imply holistic approach?Not recognized by America Board of
Medical SpecialtiesNational and individual outcomes? Interventionalist Isn’t Fibromyalgia a pain syndrome?
The American Academy of Pain Medicine– “An unpleasant sensation and emotional response to that sensation”
The real issue is anguish/emotional suffering▪ Barbuto; Am. J. Phys. Med. Rehab. 2008
Anxiety is a fuel for pain Insomnia is a fuel for anxiety and visa
versa Fear , anger, unrealistic expectations are
fuels for anxiety

A painful or apprehensive uneasiness of mind usually over an impending or anticipated ill
Inconvenient to treat Friday afternoon breakthrough anxiety-fear
Lifestyle choices Atypical Chest Pain? Medication efficacy Avoidance is a coping strategy Somatization is one avoidance strategy Why don’t so IT pain pumps seem to
work?

An unpleasant often strong emotion caused by anticipation or awareness of danger and accompanied by increased autonomic activity
The amygdala (emotional memory center) is activated and initiates the flight or fight response
Disabled Distressed Rats: Fear of re-injury and pain are major causes of disability

A strong feeling of displeasure & belligerence
Anger is a emotion when threatened Frymoyer & Bigos Studies 1990’s
▪ Anger towards direct supervisorWhy don’t we see many angry
fibromyalgia men?

Amygdala Pituitary –
sympathetic response
HPA axis: Adrenals release of cortisol
Systemic & Cardiac Adrenaline effects
What about chronic stress


Chronic somatically focused LBPFear of Re-injury? Job loss? Who’s fault is it if our patients are
afraid of degenerative arthritis, fibromyalgia or discogenic pain?

Bradykinesia & kinesophobia signs of F.O.S.?
“Your spine is going to crumble into a fine dust”
Fear of reinjuryAge appropriate changesWolfe’s Law and spine stabilityStraightening of cervical lordosis?

Does it exist?Syndrome: A set of symptoms
occurring together; the sum of signs of any morbid state
Fibromyalgia is different from good ole American chronic low back pain
Dicle Univeristy Physiatry
Oath to treat only convenient patients that keep us on schedule?
To validate or not to validate? Hamlet
▪ Validate Pharma commercials? Your choices:
▪ Scoot quickly out of room & be afraid of every f/u▪ Dump on your colleagues▪ Take on their burden and risk your own survival?▪ Kubler-Ross 5 stages of provider grieving▪ Accept to take on their treatment, but not their
burden


Hearing dialPain dial: elevated levels of
substance P in muscle tissueAwareness/Proprioception dial

Printed website handout Second visit: 30min f/u Listen and assess motivation by quality
of Q’s Answer questions Validate with eye contact & limit to
office, move on, in office revalidation, move on, in office revalidation, move on
Sleep habits TPI & Nutrition covered in another lecture
Passive Trapezius muscle stretching▪ Breathing, awareness and slowing down▪ High stress reduces efficacy of medications
Active Cervical ROM▪ Sand down Ca++ deposit rough edges from
lack of use

Rational Polypharmacy?Muscle Relaxers??Dantrolene SodiumCyclobenzaprine & TCA’sGabapentin & Pregabalin(Lyrica)SNRI’s“what if that doesn’t work?”
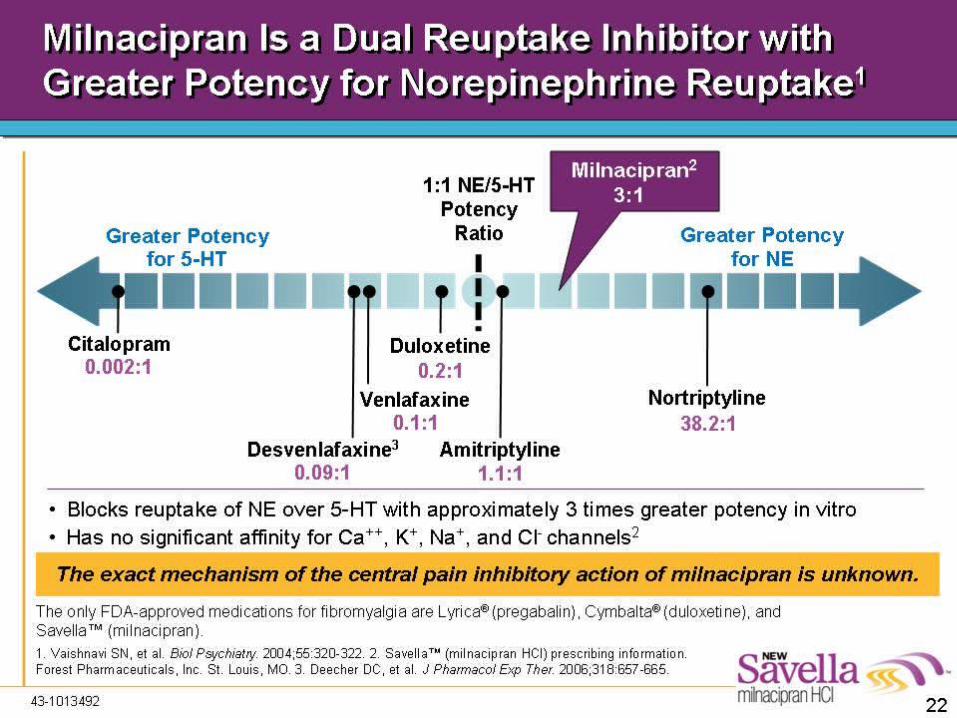

Two SNRI’s have been shown to reduce pain in Fibromyalgia -Duloxetine-Cymbalta 1 to 0.2 S:N affects -Milnacipran-Savella - 1 to 3 S:N affects
Only medication to increase function(SF36) at 3 & 6 months is Milnacipran▪ Mease 2009 N=888 & Clauw 2008 N=1196
Renal excretion >10 years of safety Weight neutral at worst

Somatizing patients without comorbid depression or anxiety disorder. N=290
Results extrapolated to national level 256 billion/yr in medical care costs are attributable to the incremental effect of somatization alone.
Approximately 2x the annual medical care costs of nonsomatizing patients.
▪ Barsky; Arch of Gen Psychiatry 2005 Remember costs come with procedure
and medication risks

Psychiatry DSM criteria and definitions
Somatically Preoccupied▪ Spitzer JAMA 1991
The real issue is anguish/emotional suffering▪ Barbuto Commentary: Am. J. Phys. Med.
Rehab. 2008

Maladaptive avoidance behavior that results in a disparity between physical impairment and function regardless of organic pathology

Entities that validate or magnify minimal organic impairments reinforcing maladaptive avoidance behavior

Opioids Monthly vicodin
merry go round Discogenic pain Discograms 5th vital sign Lumbar scars Interventionalists (Myopic ones)

Pain is not a diagnosisLow back pain with or without leg painCharacteristics of a good screening test
▪ No false negatives▪ Reliable outcome measures (pain?)▪ Inexpensive▪ Noninvasive▪ Well defined condition▪ Treatment has good outcomes

45 asymptomatic patients with normal psychometric testing
143 discs evaluated by MRI13 discs showed HIZ on lumbar MRI9 abnormal on discography
▪ Carragee, Spine 2000Please don’t ever send any of my
family members for a discogram
Primum non nocere: Do No HarmBeneficence vs. Do No Harm?
▪ “I believe my patients”▪ “They came to me to do something”▪ Acute pain model simply doesn’t work for
chronic somatically focused low back pain patients
Protect your patients against willful myopia

Intelligent disciplined diverters -criminal act worthy of discharge
Substance abuse -medical condition with specific patterns worthy of medical treatment, appropriate opioid weaning, and a measure of empathy
Anxiety/Somatization-worthy of greater time & attention, rational opioids and protect from unnecessary risk

No dumping “I do not prescribe” is
not acceptable if you maintain a DEA#
Lying is just a symptom of abuse
Baseball rule One Mulligan Maintain good habits
without escalation (be effective, not right)
No gotcha Pseudoaddiction “Not all pain can be
relieved” Some patients not
ready change Pain and suffering
often look the same-Barbuto
Opioids can validate and enable
A single provider can’t….

Legitimate diagnosis documented and communicated
Stable dose and mood No major workup or decline of condition
expected Documented functional gains for
nonmalignant pain May follow up prn for dose escalation



Slight increase HR with inspiration & slight decrease with expiration
Habituate gratitude
Less hopelessness then less helplessness

Do No Harm Protect your patientsDon’t be right and escalate, be
effectiveListening is counselingValidate Fibromyalgia with eye
contact and move onDon’t validate avoidance behavior