rc-3b external dosimetry: operational quantities and …irpa11.irpa.net/pdfs/rc-3b.pdf · 11th...
TRANSCRIPT

RC-3b
External Dosimetry: Operational Quantities and their Measurement
Christian Wernli
Paul Scherrer Institute, Villigen, Switzerland

11th International Congress of the International Radiation Protection Association (IRPA)
Madrid, May 2004
Refresher Course RC-3b
External Dosimetry:
Operational Quantities and their Measurement
Christian Wernli
Paul Scherrer Institute 5232 Villigen, Switzerland
Contents
1. Introduction 2 2. Concept of radiation protection quantities 2 3. Limiting quantities (protection quantities) 3
3.1 Absorbed dose and equivalent dose in an organ or tissue 3 3.2 Radiation weighting factors 3 3.3 Effective dose 4
4. Operational quantities 5 4.1 The concept of operational quantities 5 4.2 Dose equivalent and quality factor 5 4.3 Operational quantities for area monitoring 6
4.3.1 The ICRU sphere phantom 6 4.3.2 Concept of expanded and aligned radiation field 6 4.3.3 Ambient dose equivalent, H*(d) 6 4.3.4 Directional dose equivalent, H’(d, Ω) 7
4.4 Operational quantities for individual monitoring, Hp(d) 7 5. Summary of quantities and units for external dosimetry 8 6. Procedures for calibration 9 7. Monitoring techniques 11
7.1 External photon/beta radiation 11 7.2 Neutron radiation 12 7.3 Workplace monitoring 12 7.4. Recent developments on monitoring methods and techniques 12 7.5. Outlook 13
8. References 15
2
1. Introduction
The development of dosimetric concepts and the definition of specific quantities for use in radiation protection have a long history. The International Commission on Radiation Units and Measurements (ICRU) and the International Commission on Radiological Protection (ICRP) are the key organisations in this field. In 1991 in its Publication 60 [1], the ICRP has published its most recent general recommendations for radiation protection. These recommendations include basic concepts and guidelines for radiation protection, a concept for radiation protection quantities and limits for occupational and public exposure. In the following, this concept for radiation protection quantities and the operational quantities introduced by ICRU for monitoring of external exposure will be described. In 2003, the ICRP Publication 92 [2] on “Relative Biological Effectiveness (RBE), Quality Factor (Q), and Radiation Weighting Factor (wR)” appeared as the result of a re-appraisal of the radiation weighting factor values. The newly proposed wR values are listed for comparison with ICRP 60 data but not further used throughout the text.
Internationally agreed conversion coefficients for photon, neutron and electron radiation are a necessary basis for implementation of the operational quantities into practice. In addition, ISO and IEC have published standards on radiation fields used for calibration and on calibration procedures.
For individual monitoring of external radiation new techniques are emerging. Active and passive electronic dosemeter systems are offering new solutions for dosimetry and data handling, including direct dose readout capabilities and application of modern data networks.
2. Concept of radiation protection quantities
The international commissions ICRP and ICRU have developed a hierarchy of quantities for radiation protection applications which can be described by primary limiting dose quantities (called "protection quantities") taking account of human body properties and operational dose quantities for monitoring of external exposure.
The basic idea of a primary limiting quantity is to relate the "risk" of exposure to ionising radiation (exposure by internal and external radiation sources) to a single (dose) quantity which takes account of the man as a receptor, the different radiation sensitivities of various organs and tissues and the different radiation qualities. Other influence parameters, however, e.g. the influence of dose and dose rate or sex and age of a person exposed on the biological response to the exposure risk, were not considered in the definition of these quantities. These effects are to some extent taken into account by the various limitations of exposure.
Operational quantities are dose quantities defined for use in radiation protection measurements for external exposure (area or individual monitoring). They usually should provide an estimate of or an upper limit for the value of the limiting quantities due to an exposed, or potentially exposed, person and are often used in place of those quantities in practical regulations. Operational quantities are needed for monitoring external exposures because protection quantities generally are not measurable.
Both, protection quantities and operational quantities can be related to "basic physical quantities" as specified in ICRU Report 33 [3], which are generally used in radiation metrology and in radiation dosimetry in particular, and are defined without considering any specific aspect of radiation protection. Basic physical quantities are quantities whose units are directly obtained through

3
primary standards at national standards laboratories, e. g. air kerma for photons, fluence for neutrons, and absorbed dose for beta radiation.
Most of the radiation protection quantities mentioned above either are not directly measurable or their values are not directly traceable to primary standards. For this reason, knowledge of the numerical relations between the basic physical quantities and these dose quantities is a very important condition for the practical implementation of the whole system of radiation protection quantities.
Therefore, it is vital that an agreed set of data accepted by national and international authorities is available so that confusion is avoided. Following ICRP Publication 60, conversion coefficients for photon, neutron and electron radiation were evaluated and published in ICRP Publication 74 [4] in 1996.
3. Limiting quantities (protection quantities)
3.1 Absorbed dose and equivalent dose in an organ or tissue
The absorbed dose in an organ or tissue, DT, is the absorbed dose averaged over the volume of a tissue or organ T (rather than at a point). While the absorbed dose at a point generally is the fundamental dose quantity, in radiation protection, the mean dose in an organ becomes the basic protection quantity correlated with the exposure risk. This concept, therefore, is obviously based on the linear dose-effect relationship and the additivity of doses for risk assessment as an appropriate approximation in the low dose region. Otherwise, averaging of doses and adding of doses over long periods would not be an acceptable procedure.
The equivalent dose in an organ or tissue is defined by:
HT = Σ wR DT,R ,
where DT,R is the mean organ dose in the organ or tissue T from radiation of type R incident on the human body and wR are radiation weighting factors characterising the biological effectiveness of the specific radiation R relative to photons. The sum is taken over all types of radiation involved.
3.2 Radiation weighting factors
For external irradiation, the values of the radiation weighting factors are given by the parameters of the external radiation field only (by the type and spectral distribution of the radiation incident on the body). This means that wR is a body-averaged value representing a mean value for the relative biological effectiveness of all tissues of the body. Because the wR value is the same for all organs in a body, this procedure obviously ignores any local variation of the radiation quality in the human body which may result from the generation of secondary radiation of different types in the human body. This effect is important mainly in the case of incident neutrons where secondary photons strongly contribute to the absorbed doses of various organs.
The wR values for various types of radiation are specified in ICRP 60 and most recently, in ICRP 92 (see Table 1). For photons, electrons and muons of all energies a value of one is fixed with the exception of Auger electrons emitted from nuclei bound to DNA, but this is of no importance for external irradiation. The radiation weighting factor for neutrons depends on the neutron energy.
4
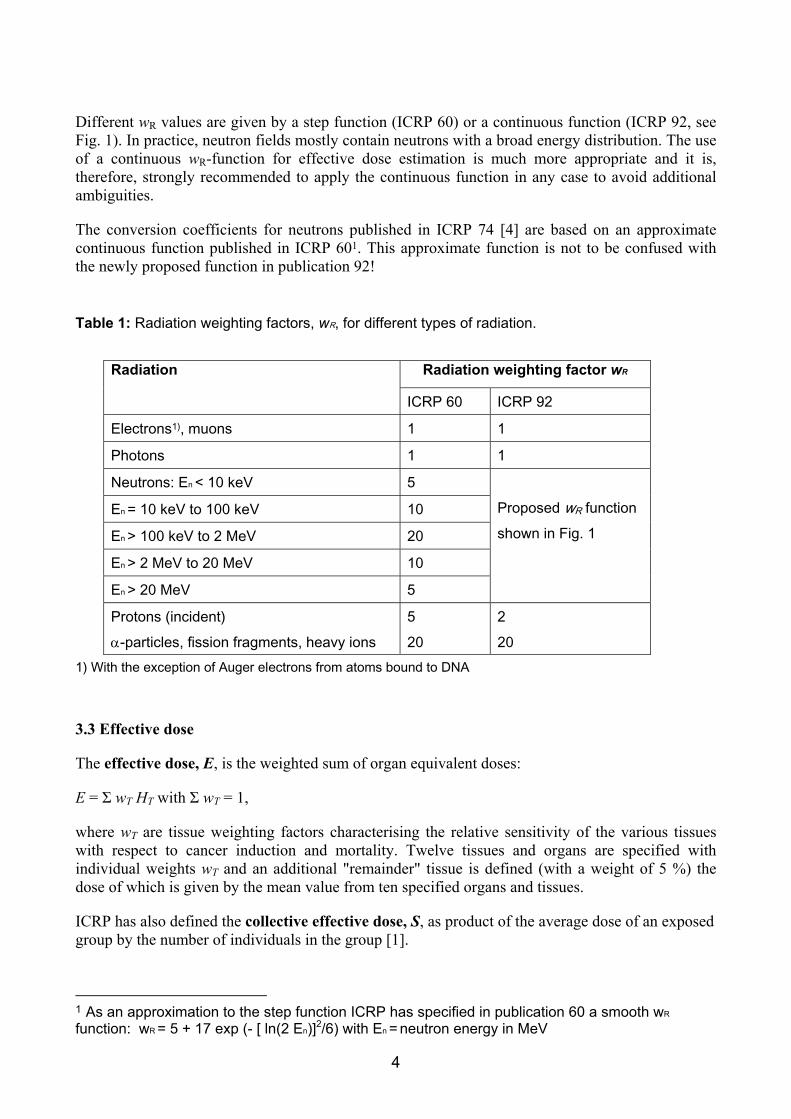
Different wR values are given by a step function (ICRP 60) or a continuous function (ICRP 92, see Fig. 1). In practice, neutron fields mostly contain neutrons with a broad energy distribution. The use of a continuous wR-function for effective dose estimation is much more appropriate and it is, therefore, strongly recommended to apply the continuous function in any case to avoid additional ambiguities.
The conversion coefficients for neutrons published in ICRP 74 [4] are based on an approximate continuous function published in ICRP 601. This approximate function is not to be confused with the newly proposed function in publication 92!
Table 1: Radiation weighting factors, wR, for different types of radiation.
Radiation weighting factor wR Radiation
ICRP 60 ICRP 92
Electrons1), muons 1 1
Photons 1 1
Neutrons: En < 10 keV 5
En = 10 keV to 100 keV 10
En > 100 keV to 2 MeV 20
En > 2 MeV to 20 MeV 10
En > 20 MeV 5
Proposed wR function shown in Fig. 1
Protons (incident) α-particles, fission fragments, heavy ions
5 20
2 20
1) With the exception of Auger electrons from atoms bound to DNA
3.3 Effective dose
The effective dose, E, is the weighted sum of organ equivalent doses:
E = Σ wT HT with Σ wT = 1,
where wT are tissue weighting factors characterising the relative sensitivity of the various tissues with respect to cancer induction and mortality. Twelve tissues and organs are specified with individual weights wT and an additional "remainder" tissue is defined (with a weight of 5 %) the dose of which is given by the mean value from ten specified organs and tissues.
ICRP has also defined the collective effective dose, S, as product of the average dose of an exposed group by the number of individuals in the group [1].
1 As an approximation to the step function ICRP has specified in publication 60 a smooth wR
function: wR = 5 + 17 exp (- [ ln(2 En)]2/6) with En = neutron energy in MeV

5
Figur 1: Radiation weighting factors wR for neutron radiation. Current discontinuous convention (ICRP 60) and proposed continuous function (ICRP 92)
4. Operational quantities
4.1 The concept of operational quantities
The basic concept of the operational quantities is described in the ICRU Reports 39 and 43 [5, 6]. The present definitions are given in ICRU Report 51 [7]. The radiation incident on a human body is characterised as penetrating radiation or low-penetrating radiation, depending on the ratio of the skin dose to effective dose. Radiation is considered to be low-penetrating when the dose equivalent received by the skin (dose received at a depth of 0.07 mm) in the case of normal incidence of a broad radiation beam is higher than ten times the effective dose - otherwise it is considered to be penetrating. Low-penetrating radiations are α-particles, β-particles with energies below 2 MeV and photons with energies below about 12 keV. Neutrons always are penetrating radiation.
Due to the different tasks in radiation protection monitoring - area monitoring for controlling the radiation at workplaces and definition of controlled areas or individual monitoring for the control and limitation of individual exposures - different operational quantities were defined. While measurements with an area monitor are mostly performed free in air, an individual dosemeter is usually worn on the front of the body. As a consequence, in a given situation, the radiation field "seen" by an area monitor free in air differs from that "seen" by an individual dosemeter worn on a body where the radiation field is strongly influenced by the backscatter and absorption of radiation in the body. The operational quantities allow for this effect.
4.2 Dose equivalent and quality factor
The quantity dose equivalent, H, has been defined by
H = Q D,
0
5
10
15
20
25
0.001 0.01 0.1 1 10 100 1000
radi
atio
n w
eigh
ting
fact
or
neutron energy / MeV
proposed wR
Proposed and current (ICRP 60) convention
current discontinuousconvention
6
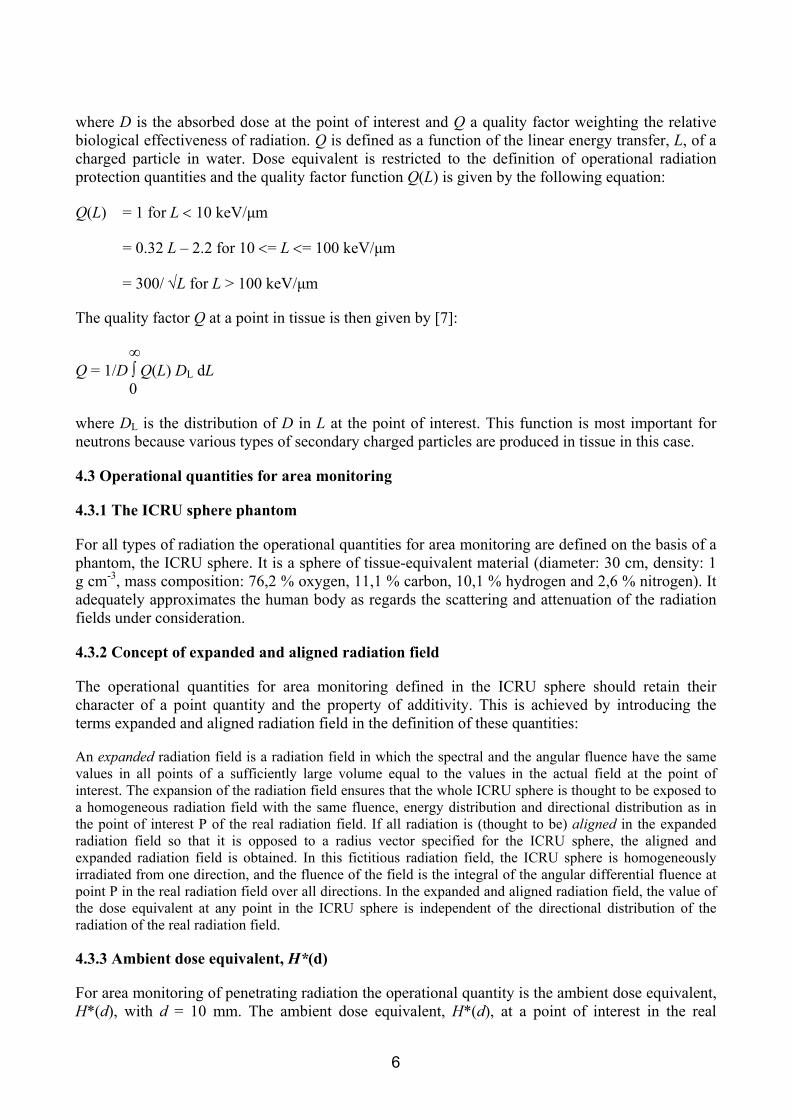
where D is the absorbed dose at the point of interest and Q a quality factor weighting the relative biological effectiveness of radiation. Q is defined as a function of the linear energy transfer, L, of a charged particle in water. Dose equivalent is restricted to the definition of operational radiation protection quantities and the quality factor function Q(L) is given by the following equation:
Q(L) = 1 for L < 10 keV/µm
= 0.32 L – 2.2 for 10 <= L <= 100 keV/µm
= 300/ √L for L > 100 keV/µm
The quality factor Q at a point in tissue is then given by [7]:
∞ Q = 1/D ∫ Q(L) DL dL
0
where DL is the distribution of D in L at the point of interest. This function is most important for neutrons because various types of secondary charged particles are produced in tissue in this case.
4.3 Operational quantities for area monitoring
4.3.1 The ICRU sphere phantom
For all types of radiation the operational quantities for area monitoring are defined on the basis of a phantom, the ICRU sphere. It is a sphere of tissue-equivalent material (diameter: 30 cm, density: 1 g cm-3, mass composition: 76,2 % oxygen, 11,1 % carbon, 10,1 % hydrogen and 2,6 % nitrogen). It adequately approximates the human body as regards the scattering and attenuation of the radiation fields under consideration.
4.3.2 Concept of expanded and aligned radiation field
The operational quantities for area monitoring defined in the ICRU sphere should retain their character of a point quantity and the property of additivity. This is achieved by introducing the terms expanded and aligned radiation field in the definition of these quantities:
An expanded radiation field is a radiation field in which the spectral and the angular fluence have the same values in all points of a sufficiently large volume equal to the values in the actual field at the point of interest. The expansion of the radiation field ensures that the whole ICRU sphere is thought to be exposed to a homogeneous radiation field with the same fluence, energy distribution and directional distribution as in the point of interest P of the real radiation field. If all radiation is (thought to be) aligned in the expanded radiation field so that it is opposed to a radius vector specified for the ICRU sphere, the aligned and expanded radiation field is obtained. In this fictitious radiation field, the ICRU sphere is homogeneously irradiated from one direction, and the fluence of the field is the integral of the angular differential fluence at point P in the real radiation field over all directions. In the expanded and aligned radiation field, the value of the dose equivalent at any point in the ICRU sphere is independent of the directional distribution of the radiation of the real radiation field.
4.3.3 Ambient dose equivalent, H*(d)
For area monitoring of penetrating radiation the operational quantity is the ambient dose equivalent, H*(d), with d = 10 mm. The ambient dose equivalent, H*(d), at a point of interest in the real

7
radiation field, is the dose equivalent that would be produced by the corresponding aligned and expanded radiation field, in the ICRU sphere at a depth d, on the radius vector opposing the direction of radiation incidence. For penetrating radiation it is d = 10 mm and H*(d) is written H*(10). As a result of the imaginary alignment and expansion of the radiation field, the contributions of radiation from all directions add up. The value of H*(10) is therefore independent of the directional distribution of the radiation in the actual field. This means that the reading of an area dosemeter for the measurement of H*(10) should be independent of the directional distribution of the radiation - an ideal detector should have an isotropic fluence response. H*(10) should give a conservative estimate of the effective dose a person would receive when staying at this point. This is always the case for photons below 10 MeV in contrast to the formerly used free-in-air quantities air kerma or exposure which are non-conservative in the photon energy range near 80 keV. For neutrons the situation is different. H*(10) is not conservative with respect to E under AP irradiation conditions in the energy range from 1 eV to about 50 keV. In realistic neutron fields with a broad neutron energy distribution, however, this energy range mostly is of small importance and in practice H*(10) therefore remains in most cases conservative with respect to E.
4.3.4 Directional dose equivalent, H’(d, Ω)
For area monitoring of low-penetrating radiation the operational quantity is the directional dose equivalent, H’(d, Ω) with d = 0.07 mm or, in rare cases, d = 3 mm. The directional dose equivalent, H’(d, Ω), at a point of interest in the actual radiation field, is the dose equivalent that would be produced by the corresponding expanded radiation field, in the ICRU sphere at a depth d, on a radius in a specified direction Ω.
For low-penetrating radiation d is equal to 0.07 mm and H’(d, Ω) is written H’(0.07, Ω). In case of monitoring the dose to the eye lens H’(3, Ω) with d = 3 mm may be chosen. For unidirectional radiation incidence the quantity may be written H’(0.07, α), where α is the angle between the direction Ω and the direction opposite to radiation incidence.
In practice, H’(0.07, Ω) is almost exclusively used in area monitoring for low-penetrating radiation, even if irradiation of the eye lens cannot be precluded. The value of the directional dose equivalent can strongly depend on the direction Ω, i.e. on how the ICRU sphere is oriented in the expanded radiation field. The same is true of instruments for measuring low-penetrating radiation - e.g. beta- or alpha-particle radiation the reading of which can strongly depend on the orientation in space. In radiation protection practice, however, it is always the maximum value of H’(0.07, Ω) at the point of interest which is of importance. It is usually obtained by rotating the dose rate meter during the measurement and looking for the maximum reading.
4.4 Operational quantities for individual monitoring, Hp(d)
Individual monitoring is usually performed with dosemeters worn on the body and the operational quantity defined for this application takes this situation into account. For individual monitoring the operational quantity is the personal dose equivalent, Hp(d). The personal dose equivalent, Hp(d), is the dose equivalent in ICRU tissue at a depth d in a human body below the position where an individual dosemeter is worn. For monitoring of the skin dose d = 0.07 mm is recommended and for monitoring effective dose d = 10 mm. In rare cases of monitoring the dose to the lens of the eye a depth d = 3 mm may be appropriate. The operational quantities for individual monitoring meet several criteria. They are equally defined for all types of radiation, additive with respect to various directions of radiation incidence, take into account the backscattering from the body and can be approximately measured with a dosemeter worn on the body. The personal dose equivalent

8
quantities, Hp(10) and Hp(0.07), are defined in the person, in the actually existing radiation field, and are measured directly on the person.
Other requirements the quantities should satisfy can, however, be fulfilled only with additional specifications. Obviously, the person influences the radiation field by scattering and attenuating the radiation. Since Hp(10) and Hp(0,07) are defined in the body of each person considered, their values vary from one person to another and also depend on the location on the body where the dosemeter is worn. In a non-isotropic radiation field the value of personal dose equivalent also depends on the orientation of the person in this field.
An operational quantity for individual monitoring should allow the effective dose to be assessed or should provide a conservative estimate under nearly all irradiation conditions. This obviously is not always possible. For example, if a dosemeter is worn at the front side of the body and the person is exposed from the back, this condition cannot be fulfilled because most of the radiation will already be absorbed within the body and not reach the front where the dosemeter is positioned. Even if the dosemeter correctly measures Hp(10) in this case, this value is not a conservative estimate of the effective dose, E. It is, therefore, an additional requirement in individual dosimetry that the personal dosemeter must be worn at a position on the body which is representative of body exposure. For a dosemeter position in front of the trunk, however, the quantity Hp(10) mostly furnishes a conservative estimate of E even in cases of lateral or isotropic radiation incidence on the body. A further requirement for an operational quantity is that it allows dosemeters to be calibrated under reference conditions in terms of that quantity. The personal dose equivalent is defined in the individual human body and it is obvious that individual dosemeters cannot be calibrated in front of a real human body. For a calibration procedure, the human body must therefore be replaced by an appropriate phantom.
Three standard phantoms have been defined by ISO for this purpose and the definition of Hp(10) and Hp(0.07) is extended to define positions and doses not only in the human body but also in three phantoms of ICRU tissue, a slab phantom (30 cm x 30 cm x 15 cm), a wrist phantom (a cylinder of 73 mm in diameter and 300 mm in length) and a finger phantom (a cylinder of 19 mm in diameter and 300 mm in length). In reference radiation fields used for calibration, the values of the quantities in these phantoms are defined as the true values of the corresponding Hp-quantities.
The question remains whether H*(10) and Hp(10) can be used as operational quantities in very high energy radiation fields, e.g. fields at flight altitudes or in space or close to high-energy accelerators. This needs to be further investigated and discussed on the basis of calculated conversion coefficients.
5. Summary of quantities and units for external dosimetry 5.1 Basic physical quantities Quantity Unit Application Air kerma, Ka Gray (Gy) Traceable reference quantity for photon radiation Fluence, Φ cm-2 Traceable reference quantity for neutron radiation Absorbed dose, D Gray (Gy) Traceable reference quantity for electron radiation

9
5.2 Operational quantities Quantity Unit Application Personal dose equivalent, Hp(d) Sievert (Sv) Individual monitoring Ambient dose equivalent, H*(d) Sievert (Sv) Area monitoring for penetrating radiation Directional dose equivalent, H’(d, Ω)
Sievert (Sv) Area monitoring for low-penetrating radiation
5.3 Primary limiting or protection quantities Quantity Unit Application Organ absorbed dose, DT Gray (Gy) Dose limitation Organ equivalent dose, HT Sievert (Sv) Dose limitation Effective dose, E Sievert (Sv) Dose limitation Collective effective dose, S man sievert Optimisation
Figure 2: Relationship between the basic physical quantities, the operational quantities and the protection quantities [8]. The conversion coefficients relating the numerical values of these quantities are published in ICRP 74 [4], see Annex.
6. Procedures for calibration 6.1 Calibration of area monitors [8] Calibration of area monitors in terms of H*(d) and, rarely, H’(d, Ω) is performed free in air. The relevant operational quantity is obtained by determining the appropriate basic physical quantity
Physical quantities
Particle fluence, Φ Kerma, K Absorbed dose, D
Operational quantities Ambient dose equivalent, H*(d) Directional dose equivalent, H'(d,Ω) Personal dose equivalent, Hp(d)
Protection quantities Organ absorbed dose, DT
Organ equivalent dose, HT Effective dose, E
Calculated using Q(L) and simple phantoms (sphere or slab) validated by measure-
ments and calculations
Compared by measurement and calculations (using wR, wT and anthropomorphic
phantoms)
Calculated using wR, wT and anthropomorphic phantoms
10
- Air kerma for photon radiation - Fluence for neutrons, or - Absorbed dose for electrons
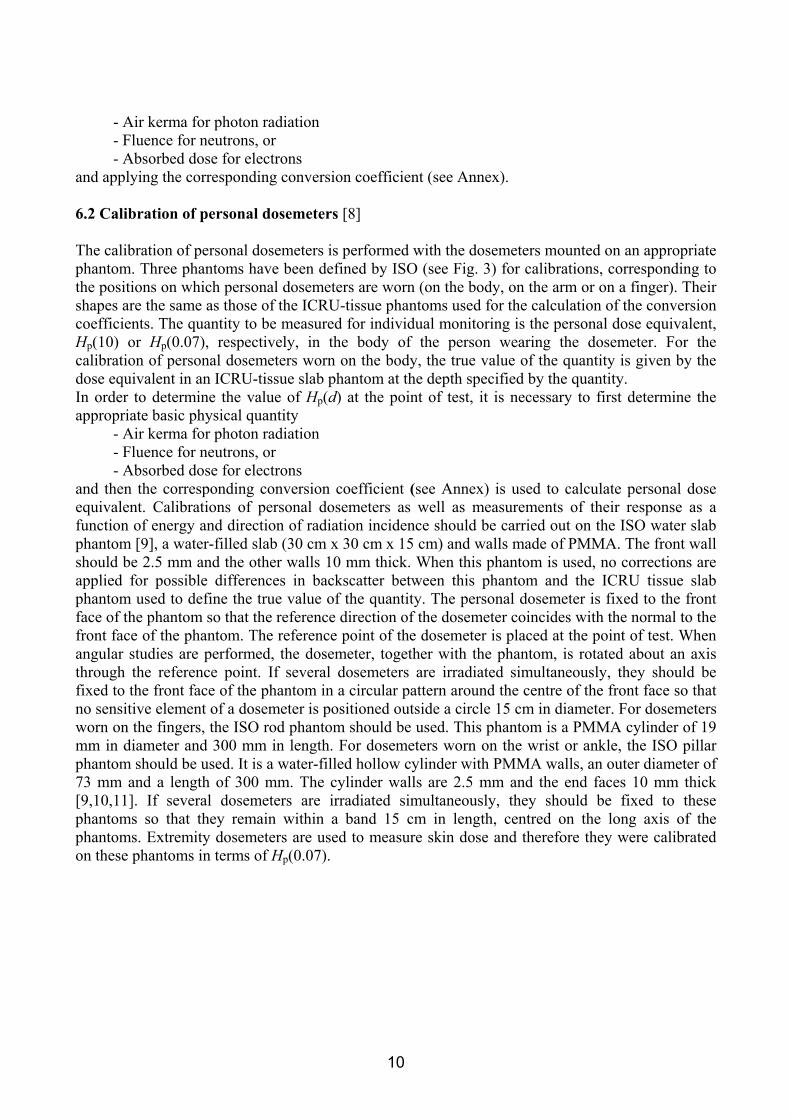
and applying the corresponding conversion coefficient (see Annex). 6.2 Calibration of personal dosemeters [8] The calibration of personal dosemeters is performed with the dosemeters mounted on an appropriate phantom. Three phantoms have been defined by ISO (see Fig. 3) for calibrations, corresponding to the positions on which personal dosemeters are worn (on the body, on the arm or on a finger). Their shapes are the same as those of the ICRU-tissue phantoms used for the calculation of the conversion coefficients. The quantity to be measured for individual monitoring is the personal dose equivalent, Hp(10) or Hp(0.07), respectively, in the body of the person wearing the dosemeter. For the calibration of personal dosemeters worn on the body, the true value of the quantity is given by the dose equivalent in an ICRU-tissue slab phantom at the depth specified by the quantity. In order to determine the value of Hp(d) at the point of test, it is necessary to first determine the appropriate basic physical quantity
- Air kerma for photon radiation - Fluence for neutrons, or - Absorbed dose for electrons
and then the corresponding conversion coefficient (see Annex) is used to calculate personal dose equivalent. Calibrations of personal dosemeters as well as measurements of their response as a function of energy and direction of radiation incidence should be carried out on the ISO water slab phantom [9], a water-filled slab (30 cm x 30 cm x 15 cm) and walls made of PMMA. The front wall should be 2.5 mm and the other walls 10 mm thick. When this phantom is used, no corrections are applied for possible differences in backscatter between this phantom and the ICRU tissue slab phantom used to define the true value of the quantity. The personal dosemeter is fixed to the front face of the phantom so that the reference direction of the dosemeter coincides with the normal to the front face of the phantom. The reference point of the dosemeter is placed at the point of test. When angular studies are performed, the dosemeter, together with the phantom, is rotated about an axis through the reference point. If several dosemeters are irradiated simultaneously, they should be fixed to the front face of the phantom in a circular pattern around the centre of the front face so that no sensitive element of a dosemeter is positioned outside a circle 15 cm in diameter. For dosemeters worn on the fingers, the ISO rod phantom should be used. This phantom is a PMMA cylinder of 19 mm in diameter and 300 mm in length. For dosemeters worn on the wrist or ankle, the ISO pillar phantom should be used. It is a water-filled hollow cylinder with PMMA walls, an outer diameter of 73 mm and a length of 300 mm. The cylinder walls are 2.5 mm and the end faces 10 mm thick [9,10,11]. If several dosemeters are irradiated simultaneously, they should be fixed to these phantoms so that they remain within a band 15 cm in length, centred on the long axis of the phantoms. Extremity dosemeters are used to measure skin dose and therefore they were calibrated on these phantoms in terms of Hp(0.07).

11
Figure3: Phantoms to be used for calibration of dosemeters: (a) ISO slab phantom, (b) ISO pillar phantom, and (c) ISO rod phantom
7. Monitoring techniques
7.1 External photon/beta radiation
There are three main techniques used for external dosimetry of photon/beta radiation:
- Photographic film
- Thermoluminescence (TLD)
- Optically Stimulated Luminescence (OSL)
Until some 30 years ago, film was the almost only technique used. Since then there has been a continuous tendency towards TLD. Most recently, a significant shift from film to OSL has taken place in the US [12] and in Japan [13].
On a smaller scale radio-photo-luminescence (RPL) dosimeters (mainly in Germany and Japan), ion chamber based pen dosimeters and newly designed electronic dosimeters (see section 7.4) are in use.
For extremity dosimetry TLD is used in almost all cases.
Modern systems generally fulfill the technical requirements for individual monitoring, with the exception of low energy beta radiation, where only few systems are fully satisfactory [14].
12
7.2 Neutron radiation
For neutron dosimetry two main techniques are used:
- Differential TLD measurements for thermal neutrons, e.g. 6LiF/7LiF albedo dosimeters
- Track etch techniques, e.g. CR-39 for fast, and with converter also for thermal neutrons
Until recently NTA film was a widely used neutron detector, but production was not further guaranteed, urging some services to replace their systems.
On smaller scales bubble detectors are used.
Individual monitoring for neutron radiation is still today a challenge. Energy dependence of the response, sensitivity, and dynamic range are limiting factors of most available systems [14]. These deficiencies may be somewhat eased by the fact, that neutron dose values are usually rather low. Exceptions could be criticality accidents, which regained attention after the accident in Tokaymura in 1999.
7.3 Workplace monitoring
Workplace monitoring includes measurement of radioactivity on surfaces and in the air as well as radiation field analysis. These methods normally complement individual monitoring. In some cases dose is not individually measured but derived from workplace monitoring methods. The most prominent application of this method is dose assessment for aircrew. Today, irradiation conditions in cruising altitudes are rather well known [15] and dose assessment may be performed by computation of dose rate as a function of altitude, geomagnetic latitude and longitude, and phase of solar cycle, combined with flight profiles and staff rosters. These calculations are supported or validated with measurements [16, 17].
For a large number of persons occupationally exposed to naturally occurring radioactive material (NORM), no individual monitoring is in place and the occupational dose can be estimated on workplace monitoring data only.
7.4. Recent developments on monitoring methods and techniques
A radiation protection monitoring program includes many more purposes than just assessment of dose. Therefore, the methods have always been optimized to offer additional information besides dose. A strong argument for using film or OSL dosimeters, was their capability to render information on the irradiation conditions (estimation of photon energy, angle of irradiation, movement during irradiation, etc.). Recent developments with electronic dosimeters add completely new options [18, 19, 20]. Most striking, the dose values can be made available immediately after the irradiation. With modern IT systems, this information is immediately accessible for all persons involved, allowing actions to be taken for specific actual situations in due time and the recorded dose can be attributed to work done in given time and given locations (so called “job-dosimetry”). In nuclear industries such “operational dosimeters” have been used in parallel with the official passive dosimeters for long time. Today, modern technology allows the use of electronic systems as legal dosimeters, omitting the annoying need to use two different dosimeters for the same radiation type. In UK and Switzerland legal electronic dosimeters have been approved for routine use [21, 22].

13
The following individual monitoring system consisting of Direct Ion Storage (DIS-1) photon/beta detectors and CR-39 neutron detectors has recently been proposed for use at high energy accelerator centres, such as PSI and CERN [23]:
- Every worker who possibly enters a radiation zone is equipped with a combined passive personnel dosemeter for the measurement of Hp(10) and Hp(0.07) for photon and beta radiation, as well as of Hp(10) for neutron radiation.
- A number of local readout stations (e.g. ∼ 40 for CERN) for the photon/beta dosemeters are distributed over the site. These stations display the accumulated dose locally and via LAN all readouts are registered automatically in a central database of the dosimetry service.
- The workers are asked to read their dosemeters periodically, e.g. at the end of each month at any station nearby. In addition, the workers are free to read their dosemeters as often as they like to do so.
- For job dosimetry a specific group of workers may be asked to read their dosemeters each time they enter or leave a given area.
- The dosemeters stay with the worker for up to one year. Every month about 10% of all dosemeters are exchanged. If the photon dose exceeds 2 mSv per month, the dosemeter is immediately exchanged.
- On return of the dosemeter to the dosimetry service, the neutron detectors are removed and processed for readout. The photon/beta dosemeters are quality controlled, the dose cleared, the badge loaded with a new neutron detector and made available for new issuing.
- Neutron dose is booked in the year of readout of the neutron dosemeter if not exceptional conditions indicate otherwise.
Electronic neutron dosimeters appear increasingly on the market. Most designs are handicapped by very limited energy dependence and low sensitivity or bulky construction and high cost. New developments are more promising and in near future a reasonable selection of commercial systems may be available [24]. For aircrew dosimetry complete software packages have been developed and tested, such as “CARI”, “Sievert” or “EPCARD” [17]. Dose computation is based on simulation of galactic cosmic rays incidence and cascade production of secondary particles. Some versions also include corrections from experimental data. The entry data are: Flight profile (altitude levels and duration), solar activity, and flight trajectory (great circle approach). The standard output data is effective dose E, but “EPCARD” also provides results in terms of ambient dose equivalent H*(10) and the contributions from high and low LET components.
7.5. Outlook
Dosimetry for photon radiation: This is the bulk of dosimetric activities, attracting commercial companies to take over and to control the market. Such large services have the advantage of well-developed and standardized methods and low cost for the customer. On the other hand, as a consequence of the commercial concentration of services, the local expertise in radiation dosimetry may diminish and flexibility for site-specific solutions may become limited. It may also be not easy for national authorities to verify the quality of foreign services operating in their region of responsibility and to receive feedback requested according to national legislation.
The techniques used for photon dosimetry have a high potential for a significant change in the near future. The use of passive or active electronic devices as legal dosimeters in combination with the corresponding IT networks and software may change the practice of individual monitoring. But the requirements for legal electronic dosimeters will have to be further specified, e.g. to separate
14
functions of workplace monitoring (such as ambient dose rate indication of the quantity H*(10)) from measurement of Hp(d).
Dosimetry for beta radiation: The main application is extremity dosimetry. New designs of detectors comfortable to wear and less energy dependent are still needed. Active devices are still missing, but would attract some interest.
Dosimetry for neutron radiation: All available passive systems have some limitations and no immediate relieve is expected. Further improvements of detector materials, together with sophisticated converter materials and evaluation procedures may remedy the existing constraints. Electronic neutron dosimeters are emerging on the market. Their use may complement passive systems in various applications, but presumably not replace them.
Workplace monitoring / aircrew dosimetry: Workplace monitoring for dose assessment may increasingly involve measurements of radon and radon progeny. Such projects would need to be started to initiate expansion of the services needed.
For aircrew dosimetry the main activities are on the formal level to decide on procedures and software programs to be used. Measurements are mainly needed for verification of computed data.
Most recent developments and announced future options of occupational radiation monitoring systems enable direct electronic readout of legal dosimeters. As a consequence, data networks may become an increasingly important aspect of dose registering, reporting and record keeping. With increasing mobility of workers the importance of central dose registries becomes even more pronounced. To simplify international data exchange for workers, a standardized format (radiation passport) would be helpful. The ICRP/ICRU concept of quantities and units is an adequate basis for external dosimetry and its rigorous implementation in national legislations, regulations and work procedures is highly recommended.
15
8. References
1. ICRP. Recommendations of the International Commission on Radiological Protection. ICRP Publication
60, Annals of ICRP 21 (1-3) (1991) 2. ICRP. Relative Biological Effectiveness (RBE), Quality Factor (Q), and Radiation Weighting Factor (wR).
ICRP Publication 92, Annals of ICRP 33 (4) (2003) 3. ICRU. Radiation Quantities and Units. ICRU Report 33 (ICRU: Washington) (1980) 4. ICRP. Conversion Coefficients for Use in Radiological Protection against External Radiation. ICRP
Publication 74, Annals of ICRP 26 (3-4) (1996) 5. ICRU. Determination of Dose Equivalents Resulting from External Radiation Sources. ICRU Report 39
(ICRU Publications: Bethesda) (1985) 6. ICRU. Measurement of Dose Equivalents from External Radiation Sources, Part 2. ICRU Report 43
(ICRU Publications: Bethesda) (1988) 7. ICRU. Quantities and Units in Radiation Protection Dosimetry. ICRU Report 51 (ICRU Publications:
Bethesda) (1993) 8. IAEA Safety Reports Series No 16: Calibration of Radiation Protection Monitoring Instruments, 2000. 9. ISO 4037. X and gamma reference radiations for calibrating dosemeters and dose rate meters and for
determining their response as a function of photon energy. ISO 4037-1 (1996) - Part 1: Radiation characteristics and production methods. ISO 4037-2 (1997) - Part 2: Dosimetry for radiation protection over the energy range 8 keV to 1.3 MeV and 4 MeV to 9 MeV. ISO 4037-3 (1999) - Part 3: Calibration of area and personal dosemeters and the measurement of their response as a function of energy and angle of incidence. International Organization for Standardization, Geneva, Switzerland
10. ISO 6980 (1996). Reference beta-radiations for calibrating dosimeters and dose rate meters and for determining their response as a function of beta-radiation energy. ISO/CD 6980-2 (2000). Beta particle reference radiations - Part 2: Calibration fundamentals related to the basic quantities characterizing the radiation field. ISO 6980-3 (1998) - Part 3: Calibration of area and personal dosemeters and the determination of their response as a function of beta-radiation energy and angle of incidence. International Organization for Standardization, Geneva, Switzerland
11. Alberts, W.G., Böhm, J., Kramer, H.M., Iles, W.J., McDonald, J., Schwartz, R.B. and Thompson, I.M.G., International Standardisation of Reference Radiations and Calibration Procedures for Radiation Protection Instruments. Proc. German-Swiss Radiation Protection Association Meeting, May 24-26, 1994, Karlsruhe, Germany, (1994)
12. Landauer Inc., 2001 Annual Report. 13. Norimichi J., Personal communication, 2002. 14. European Radiation Dosimetry Group (EURADOS). Harmonisation and Dosimetric Quality Assurance in
Individual Monitoring for External Radiation. Radiat. Prot. Dosim. Vol. 89 Nos. 1-2, 2000. 15. Roesler S., et. al., Monte Carlo Calculation of the Radiation Field at Aircraft Altitudes. Radiat. Prot.
Dosim. Vol. 98, No. 4, pp. 367-388 (2002). 16. Bartlett D., Investigation of Radiation Doses at Aircraft Altitudes during a Complete Solar Cycle. NRPB,
UK. 17. Saez J., Monitoring of the Cosmic Radiation at Iberia Commercial Flights: One Year Experience of
Inflight Measurements. CIEMAT, Madrid. 18. Wernli C. and Butterweck G., Recent Developments on Electronic Dosimeters. V Regional Congress on
Radiation Protection and Safety, Recife, Brazil, 2001. 19. Bolz M. and Pécossais P., La première solution complète pour une dosimétrie personnelle active : une
technique d’avant-garde conçue pour l’utilisateur. Radioprotection Vol. 37, No. 2, 2002. 20. Wahl W., Wie wird, wie soll die Personendosimetrie der Zukunft aussehen? Wünsche und Forderungen
aus der Praxis. StrahlenschutzPRAXIS, Heft 2/2002. 21. Weeks A.; Farrell P.; Pottinger M.; Devine I. The use and operational experience of the Siemens
electronic personal dosimeter by BNFL Magnox Generation. Proceedings of IRPA 10, Hiroshima 2000.

16
22. Boschung M., Fiechtner A., Wernli C., A legally approved personal dosemeter for photon and beta radiation based on direct ion storage. Radiat. Prot. Dosim. Vol. 101, Nos. 1-4, pp 271-274 (2002)
23. Wernli C., Boschung M., A Novel Concept and Technique for Individual Monitoring for Photon, Beta and Neutron Radiation, IRPA11, 2004.
24. Luszik-Bhadra M., Elektronische Personendosimeter: Stand der Technik und neue Entwicklungen. StrahlenschutzPRAXIS, Heft 2/2002.
17
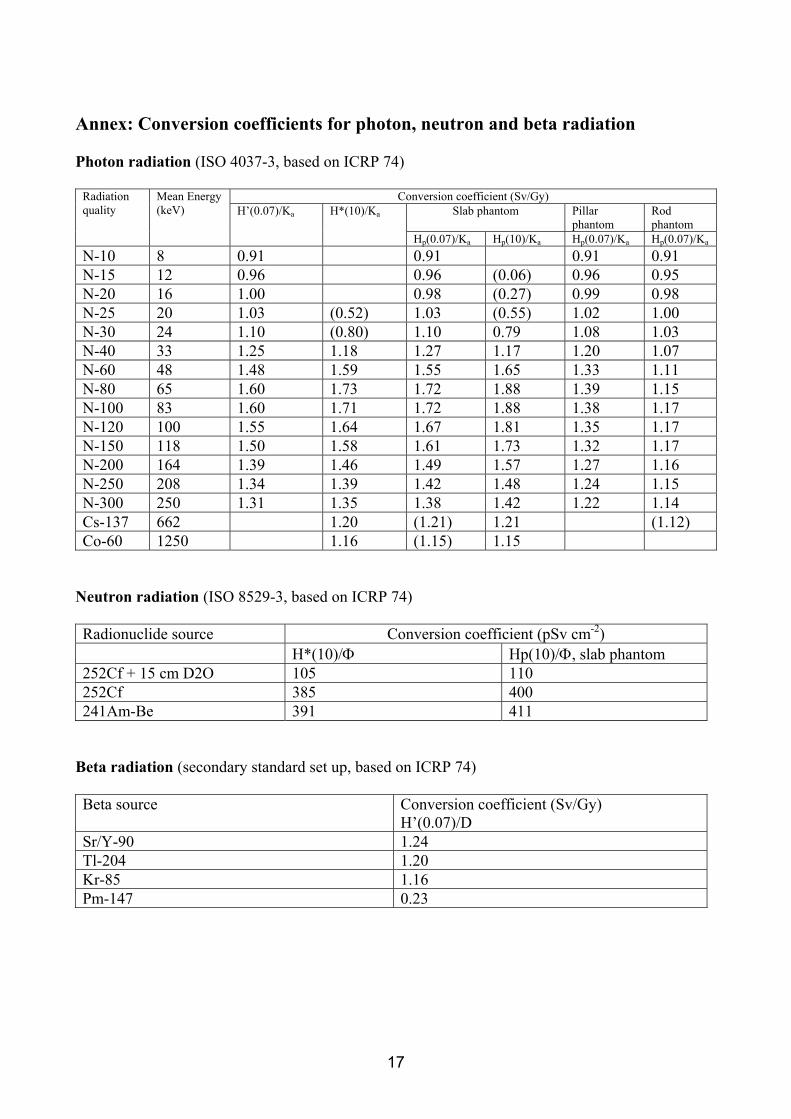
Annex: Conversion coefficients for photon, neutron and beta radiation Photon radiation (ISO 4037-3, based on ICRP 74)
Conversion coefficient (Sv/Gy) Slab phantom Pillar
phantom Rod phantom
Radiation quality
Mean Energy (keV) H’(0.07)/Ka H*(10)/Ka
Hp(0.07)/Ka Hp(10)/Ka Hp(0.07)/Ka Hp(0.07)/Ka N-10 8 0.91 0.91 0.91 0.91 N-15 12 0.96 0.96 (0.06) 0.96 0.95 N-20 16 1.00 0.98 (0.27) 0.99 0.98 N-25 20 1.03 (0.52) 1.03 (0.55) 1.02 1.00 N-30 24 1.10 (0.80) 1.10 0.79 1.08 1.03 N-40 33 1.25 1.18 1.27 1.17 1.20 1.07 N-60 48 1.48 1.59 1.55 1.65 1.33 1.11 N-80 65 1.60 1.73 1.72 1.88 1.39 1.15 N-100 83 1.60 1.71 1.72 1.88 1.38 1.17 N-120 100 1.55 1.64 1.67 1.81 1.35 1.17 N-150 118 1.50 1.58 1.61 1.73 1.32 1.17 N-200 164 1.39 1.46 1.49 1.57 1.27 1.16 N-250 208 1.34 1.39 1.42 1.48 1.24 1.15 N-300 250 1.31 1.35 1.38 1.42 1.22 1.14 Cs-137 662 1.20 (1.21) 1.21 (1.12) Co-60 1250 1.16 (1.15) 1.15
Neutron radiation (ISO 8529-3, based on ICRP 74) Radionuclide source Conversion coefficient (pSv cm-2) H*(10)/Φ Hp(10)/Φ, slab phantom 252Cf + 15 cm D2O 105 110 252Cf 385 400 241Am-Be 391 411
Beta radiation (secondary standard set up, based on ICRP 74) Beta source Conversion coefficient (Sv/Gy)
H’(0.07)/D Sr/Y-90 1.24 Tl-204 1.20 Kr-85 1.16 Pm-147 0.23