reducing patient falls - fons
TRANSCRIPT

© Karen Barnett 2002 Mid Yorkshire Hospitals NHS Trust
1
Reducing Patient Falls
Contents:
Reducing Patient Falls (Overview and background)----------------------2 - 4Definition of a Fall 5Fall Definition wall poster 6Literature review and references 7 - 14Morse Falls Risk Assessment--------------------------------------------------15 - 17Patient Care Management Plan 18 - 19Levels of Risk 20Traffic Light Visual Clues 21 - 22Environmental Assessment Tool-----------------------------------------------23 - 31Patient Information 32 - 33
Guidelines on the Use of Bed Rails-------------------------------------------34 - 38Review Process Form 39References and Bibliography 40
Protocol for the Provision of Hip Protectors---------------------------------41 - 42Patient leaflet - Hip Protectors 43Sample Business Case for Hip Protectors 44 - 45
Other documents available:
1. Falls Resource Pack Charts:• Patient Falls Risk Assessment Tool• Log Book• Patient Falls Audit Form• "If a Patient Falls" Flowchart
2. Falls Assessment Flowchart
3. Hip Protector Protocol Chart
All documents are available in Adobe Acrobat Reader (or .pdf) Format on theFoundation of Nursing Studies website
http://www.fons.org/projects/falls.htm

© Karen Barnett 2002 Mid Yorkshire Hospitals NHS Trust
2
Reducing Patient Falls
Aim of ProjectTo implement a Trust Wide falls reduction strategy in order to reduce the totalnumber of falls occurring in hospital, and to reduce the RIDDOR reportablefalls by 20%.
Objectives! To collect pre-pilot data regarding:
" Fall rate" Injury rate" Injuries sustained" Recurrent fallers
! To meet ward managers of Pilot wards and inform them of the project
! Advise ward managers and other key staff on the progress of the project
! Calibrate the tool for different units
! Pilot the tool with six agreed wards
! Educate the staff involved in the project on the assessment tool andstrategies for reducing falls.
! Analyse the data from the pilot regarding:" Fall rate" Injuries sustained" Causes of falls" No. at risk who did fall" No. at risk who did not fall" No. not at risk who did fall" Nursing satisfaction with
questionnaire" Strategies used to reduce falls
following assessment" Totalling of scores
! Disseminate pilot analyses to appropriate parties
! Implement Trust wide
! Support staff Trust wide on assessment/ falls strategies available
! Analyse following implementation
© Karen Barnett 2002 Mid Yorkshire Hospitals NHS Trust
3
Background Information
Reducing Patient Falls in Hospital
Introduction
There is a national1 and local2 agenda to reduce the number of falls inhospital. The Trusts Risk management Plan 2000 has pledged to reduce theRIDDOR reportable falls by 20%. This will have a knock-on effect of reducingthe number of recurrent fallers and subsequent injuries from falls.
Background to Project
A multidisciplinary group was set up in 1999 to devise a strategy for reducingpatient falls. They were successful in securing funding for a seconded post tomanage the project and the post was filled in January 2001.
The project leader was Karen Barnett, seconded from the OccupationalTherapy Department two days a week with the following responsibilities: -
♦ Co-ordinate the pilot of the assessment tool and fall prevention strategy♦ Calibrate the tool for individual areas♦ Evaluate the pilot stage of the project♦ Implement the fall prevention programme trust wide♦ Monitor, critically appraise and report incidence of falls within the trust♦ Establish links with companies specialising in fall prevention equipment♦ Evaluate the project♦ Disseminate project results
Report on Pilot Project
The assessment tool that was chosen was the Morse Falls Assessment Tool3as it has a relatively large amount of literature written about it and there is atraining video for staff which highlights how the scale identifies potentialfallers. It has had rigorous testing for validity and reliability and stands up wellto statistical analysis in sensitivity and specificity testing.
The pilot areas were on three hospital sites - PGH Q ward (Elderly medicine)
Neurological Rehabilitation Centre (NRC) Pinderfields Medical Rehabilitation Unit (PMRU)
Clayton Nurse Led Unit (Elderly care) PGI Ward 2 (orthopaedic surgery) Ward 5 (general surgery)
Ward 11 (acute medicine)
These areas were chosen to provide a diversity of clinical areas so that thetool and subsequent fall prevention strategies can be trialed in differentclinical areas.

© Karen Barnett 2002 Mid Yorkshire Hospitals NHS Trust
4
The project manager initially calibrated the tool on the seven different wardsand each clinical area had their own levels of risk, split into low, medium andhigh risk. All pilot areas have used the tool and collected data on the levels ofrisk, the number of fallers and the strategies in place following a high-riskassessment.
The pilot areas have also piloted documentation, in line with the Trusts newdocumentation policy on care planning. Fall prevention strategies arehighlighted in the appropriate care plans and the named nurse reports anysignificant information related to patients individual needs in the care plan.
Implementation throughout the Trust
Following the evaluation of the pilot project a number of changes were madeto the documentation. A rolling programme of implementation was devised toensure that the project manager could meet ward sisters and discuss theproject on an individual basis. By the end of August 2001 all wards will havethe relevant information and be in a position to be using the tool routinely forall patients.
The assessment tool and care planning documentation provides a structuredand standardised way to assess a patient’s level of risk and determineappropriate strategies for reducing the chance of them falling.
However it does not reduce the necessity for nurses to use their ownprofessional judgement and clinical reasoning skills.
Future plans for the Project
The project has highlighted the nurses’ role in reducing patient falls, but hasnot established the role of other members of the multi-disciplinary team. TheNational Service Framework4 has provided an opportunity to develop thework already done into multi-disciplinary care pathways. There are obviousresource implications for this type of approach but the evidence suggests thata multi-disciplinary proactive approach will be beneficial in reducing falls bothin the community and in hospital.
References:1 DOH (1999) Saving Lives Our Healthier Nation2 Pinderfields & Pontefract Hospitals NHS Trust Risk Management Report20003 Morse JM, Morse R, Tylko S (1989) Development of a scale to identify thefall prone patient. Canadian Journal on Ageing. 8(4): 366-3774 DOH (2001) National Service Framework for Older People
© Karen Barnett 2002 Mid Yorkshire Hospitals NHS Trust
5
Definition of a Fall
“An untoward event which results in the patient coming to restunintentionally on the ground or other lower surface”
(Morris & Isaacs, 1980)
Accidental Fall: A slipping, tripping or othermishap generally related toenvironmental factors
Anticipated Physiological Fall: Falls that occur with patientsthat are identified as at risk offalling.
Unanticipated Physiological Fall: Attributed to physiologicalcauses but are created byconditions that cannot bepredicted before the firstoccurrence.
(Morse, 1997)
The Falls Risk Assessment tool is used to identify anticipated physiologicalfalls.
It is important to report all falls.

© Karen Barnett 2002 Mid Yorkshire Hospitals NHS Trust
6
WHAT IS A FALL?
"AN UNTOWARDEVENT WHICH
RESULTS IN THEPATIENT COMING TO
RESTUNINTENTIONALLY ON
THE GROUND OROTHER LOWER
SURFACE”Morris & Isaacs, 1980
If a FALL occurs – REPORT IT!

© Karen Barnett 2002 Mid Yorkshire Hospitals NHS Trust
7
Patient Falls in Hospital
A Literature Review.
Patient falls are a leading cause of death from injury in people over the age of75 years, and are the most common cause of hospital admission for olderpeople. Evans and Hodgkinson (1999) state that one third of people over 65suffer at least one fall per year.
Falls increase the length of hospital stay and not only have a physical impacton the patient, that of discomfort, injury, increased morbidity or even death(Cohen & Guin, 1991), but have an economic impact on the health caresystem (Wilson, 1998). Falls also result in psychological implications for thepatient with a decrease in self-confidence and a fear of further falls. Thiscontributes to a decrease in mobility and culminates in a significant reductionin quality of life (Mitchell & Jones, 1996).
The literature abounds with information on risk factors associated with anincreased risk of falling. Parker (2000) suggests that risk of falling increaseswith age due to the pathophysiological changes that occur with ageing,including such factors as reduced mobility, poor gait, diminished mentalcapacity and continence problems. Wilson (1998) in a detailed report on thecontributing risk factors describes both intrinsic and extrinsic factors related tofalling. She concludes that medication is constantly cited as contributing to therisk of falling and that it is important not to forget the cognitive and emotionalfactors that may increase the potential of falling.
Rutledge(1998) surmises that there is no single cause for the occurrence of afall but suggest that most falls in hospitals are generally predictable and oftenpreventable. Uden (999) contradicts this statement by stating that not allaccidents are preventable and goes on to suggest that it is important to find abalance between the adequate supervision by staff and encouragingindependence and quality of life for patients.
Evans (1999) undertook a systematic review of fall risk factors in an acutehospital setting. Throughout the review of eleven studies they discovered 27different factors discussed in the literature, with sixteen of these beingsignificant in only one study. The most significant risk factor throughout theliterature, cited in nine of the eleven studies was cognitive impairment. TheEffective Health Care Bulletin (1996) which reviewed 36 randomisedcontrolled trial, concluded that there are over 400 variable risk factorsmentioned throughout the literature, the most frequent being nutritional status,environmental hazards, medication, lack of exercise, ageing changes andmedical conditions.
A consistent approach expressed in the literature is that of a need to assesspatients in order to highlight those that are considered to be at high risk offalling. It is therefore important to assess risk factors in individuals, however,there are a number of risk assessment tools to choose from, depending on

© Karen Barnett 2002 Mid Yorkshire Hospitals NHS Trust
8
which risk factors are considered a priority (Morse 1989, McCollam 1995,Uden 1999). Whichever tool is chosen the basic rules for the choice ofassessment tool would be one that is valid, reliable, sensitive to change andspecifically identifies patients at high risk. It needs to be quick to administerand easy to use, so that nursing staff feel that it is a benefit rather than ahindrance.
Once the risk factors have been identified and an appropriate tool chosen it isnecessary to consider how to deal with the problems that the assessment toolhighlights. There needs to be strong fall prevention strategy thatencompasses a number of different interventions. Evans & Hodgkinson(1999) conclude that no one single intervention has been demonstrated asbeing effective over another, but this may be due to lack of rigorous researchrather then the interventions themselves. Gillespie (2000) concluded that astrategy targeting multiple risk factors is more likely to be successful. Thereare however some interventions that have been demonstrated to have noimpact on reducing patient falls. Widder (1985) noted that there was no effecton fall numbers when using an ambularm attached to the patient, and Mayo(1994) used bracelets to identify high risk patients, but again this failed toreduce the number of falls.
Patient education strategies have consistently proved to be successful in theliterature. These strategies include orientating the patient to the ward area,placing a call light within reach, instructing the patient on when/how to call forassistance, teaching patients how to transfer and to safely use assistivedevices. Kilpack (1991) suggests placing posters in patients’ rooms toencourage them to ask for assistance.
Innes & Turman (1983) suggested that high risk patients who appear to beconfused/disorientated ought to be nursed in a highly visible area of the wardso that nurses can intervene if necessary.
Staff education has also been proved to be a valuable strategy. There are anumber of strategies that can be implemented♦ Having visual cues on the nursing Kardex or on a patients door (Gillespie
(2000) Cohen & Guin (1991), Kilpack (1991)),♦ Having written protocols for standardised care plans (Cohen & Guin,
1991),♦ Informing staff on falls statistics for their area (Wilson, 1998) and♦ Providing formal education programs to increase staff awareness (Wilson
1998, McCollam 1995).
Good basic nursing care, including keeping the bed on low when notperforming physical care, locking wheels into position onbeds/lockers/wheelchairs and commodes and wiping up fluids all contribute toreducing the risk of falling and are just as important as having specific fallprevention strategies. It is also important to communicate between shifts andbetween professionals so that everyone knows that falls have occurred andwhat strategies are in place. Rutledge (1998) concludes that educating staff
© Karen Barnett 2002 Mid Yorkshire Hospitals NHS Trust
9
leads to measurably heightened staff awareness which in itself assists inpreventing falls.
A number of physiotherapy led research projects have concluded thatexercise, balance retraining, muscle strengthening and specific classes suchas Tai Chi has a positive effect on reducing the number of falls or reducinginjury if a fall does occur (Skelton & McLaughlin (1996), Judge (1993),Hopkins(1990)).
In conclusion, there is a growing amount of evidence that supports the use ofindividual risk assessment and multiple fall prevention strategies in order toreduce the number of falls within the hospital setting. Preventing falls is a win-win situation. It benefits patients, staff and organisations by enablingindependence, shortening hospital stays and preventing injuries.
Good basic nursing care, along with appropriate risk assessment and astructured approach to recording interventions that reduce the risk of falls willassist this organisation to reduce the number of falls occurring, which shouldin turn reduce the number of injuries that occur as a result of falls.
References
Cohen l, Guin P (1991) Implementation of a patient fall preventionprogram.Journal of Neuroscience Nursing. 23(5): 315-319
Effective Health Care Bulletin (1996) NHS Centre for Reviews andDisseminationEffective Health Care: Preventing Falls andSubsequent Injury in Older People. April 1996:2(4)
Evans D, Hodgkinson B, Lambert L, Wood J (1999)Fall Prevention: a systematic review.Clinical Effectiveness in Nursing (1999) 3, 106-111
Gillespie WJ, Cumming R, Lamb SE, Rowe BH (2000)Interventions for preventing falls in the elderly.The Cochrane Library (2000). Issue 4
Hopkins DR, Murrah B, Hoeger WWK, Rhodes RC(1990)Effect of low-impact aerobic dance on thefunctional fitness of elderly women.The Gerontologist (1990); 30: 189-192
Innes EM, Turman WG (1983)Evaluation of patient falls.

© Karen Barnett 2002 Mid Yorkshire Hospitals NHS Trust
10
Quality Review Bulletin. 9, 30-35
Judge OJ, Lindsey C, Underwood M, Winsemius D(1993)Balance improvements in older women: effects ofexercise training.Physical training 1993; 73:254-262
Kilpack V, Boehm J, Smith N, Mudge B (1991)Using Research based interventions to decreasepatient falls.Applied nursing research. 1991; 4(2): 50-56
McCollam M (1995) Evaluation and Implementation of a researchbased falls assessment innovation.Nursing Clinics of North America. 1995. 30(3);507-514
Mitchell A, Jones N (1996) Striving to prevent falls in an acute care setting –action to enhance quality.Journal of Clinical nursing 1996:5; 213-220
Morse J M, Morse R, Tylko S (1989)Development of a scale to identify the fall pronepatient.Canadian Journal on Ageing. 1989:8(4): 366-377
Parker R (2000) Assessing the risk of falls among older inpatients.Professional nurse May 2000. 15(8): 511-514
Rutledge DN, Donaldson NE, Pravikoff DS (1998)Fall risk assessment and prevention in healthcarefacilities.Cinahl Information Systems (Glendale CA)Dec15 1998
Skelton D & McLaughlin AW (1996) Training functional ability in old age.Physiotherapy 1996; 82:159-167
Uden G, Ehnfors M, Sjostrom K (1999) Use of initial risk assessment andrecording as the main nursing intervention inidentifying risk of falls.Journal of Advanced Nursing 29(1), 145-152
Widder B (1985) A New Device to decrease falls.Geriatric Nursing, 6(5), 287-288
Wilson Eileen (1998) Preventing patient falls.AACN Clinical Issues, 9(1), 100-108

© Karen Barnett 2002 Mid Yorkshire Hospitals NHS Trust
11
References
Arbesman M, Wright C (1999)Mechanical Restraints, rehabilitation Therapies,and staffing adequacy as risk factors for falls in anelderly hospitalised population.Rehabilitation Nursing. 24(3), 122-128
Brennan S (1999) Dangerous Liaisons.Nursing Times. November 3 Vol. 95. No. 44 1999
Cameron I, Stafford B, Cumming R, Birks C, Kurple S, Lockwood K, Quine S,Finnegan T, Salkeld G (2000)
Hip Protectors improve falls self-efficacy.Age and ageing 29, 57-62
Cohen l, Guin P (1991) Implementation of a patient fall preventionprogram.Journal of Neuroscience Nursing. 23(5): 315-319
NHS Centre for Reviews and Dissemination (1996)Effective Health care: Preventing Falls andSubsequent Injury in Older People. April 1996:2(4)
Evans D, Hodgkinson B, Lambert L, Wood J (1999)Fall Prevention: a systematic review.Clinical Effectiveness in Nursing (1999) 3, 106-111
Feder G, Cryer C, Donovan S, Carter Y (2000)Guidelines for the Prevention of Falls in peopleover 65.British Medical Journal 2000:321:1007-1011(21October)
Fitzsimons V (1985) Maintaining a Positive Environment for the olderadult.Orthopaedic Nursing 1985. 4(3): 48-51
Gallinagh R, Nevin R, Campbell L, Mitchell F, Ludwig R (2001)Relatives perceptions of side rail use on the olderperson in hospital.British Journal of Nursing 10(6)
Gillespie LD, Gillespie WJ, Cumming R, Lamb SE, Rowe BH (2000)Interventions for preventing falls in the elderly.The Cochrane Library (2000). Issue 4
Gluck, T, Wientjes HJFM, Rai GS (1996)An Evaluation of Risk Factors for In Patient Falls inAcute and Rehabilitation Elderly care wards.
© Karen Barnett 2002 Mid Yorkshire Hospitals NHS Trust
12
Gerontology.1996:42:104-107
Govier I, Kingdom A (2000) The Rise and Fall of Cot sides.Nursing Standard. 14; 31, 40-41
Green J (2000) Working Together for injury reduction: a study ofaccident alliances in Southeast England.Health education Journal (2000) 59, 23-28
Grimshaw J, Freemantle N, Wallace S, Russell I, Hurwitz B, Watt I, Long A,Sheldon T (1995)Developing and Implementing Clinical Guidelines.Quality in Health Care 1995; 4:55-64
Johnson S (2000) Use of ICP’s to manage unpredictable situations.Professional Nurse. December 2000. 16(3); 956-958
Jordan S (1995) Bionursing: explaining falls in elderly people.Nursing Standard. September 6. 9(50) 30-32
Kannus P, Parkkari J, Niemi S, Pasanen M, Palvanen M, Jarvinen M, VuoriI (2000) Prevention of Hip fractures in elderly People with
use of a hip protector.The New England Journal of Medicine. 343(21),1506-1563
Kilpack V, Boehm J, Smith N, Mudge B (1991)Using Research based interventions to decreasepatient falls.Applied nursing research. 1991; 4(2): 50-56
Lauritzen J, Peterson M, Lund BEffect of external hip protectors on hip fractures.The Lancet 341, Jan 2, 1993
Innes EM, Turman WG (1983)Evaluation of patient falls.Quality Review Bulletin. 9, 30-35
McCollam M (1995) Evaluation and Implementation of a researchbased falls assessment innovation.Nursing Clinics of North America. 1995. 30(3);507-514
Mitchell A, Jones N (1996) Striving to prevent falls in an acute care setting –action to enhance quality.Journal of Clinical nursing 1996:5; 213-220
Moss F (1995) Risk Management and quality of care.
© Karen Barnett 2002 Mid Yorkshire Hospitals NHS Trust
13
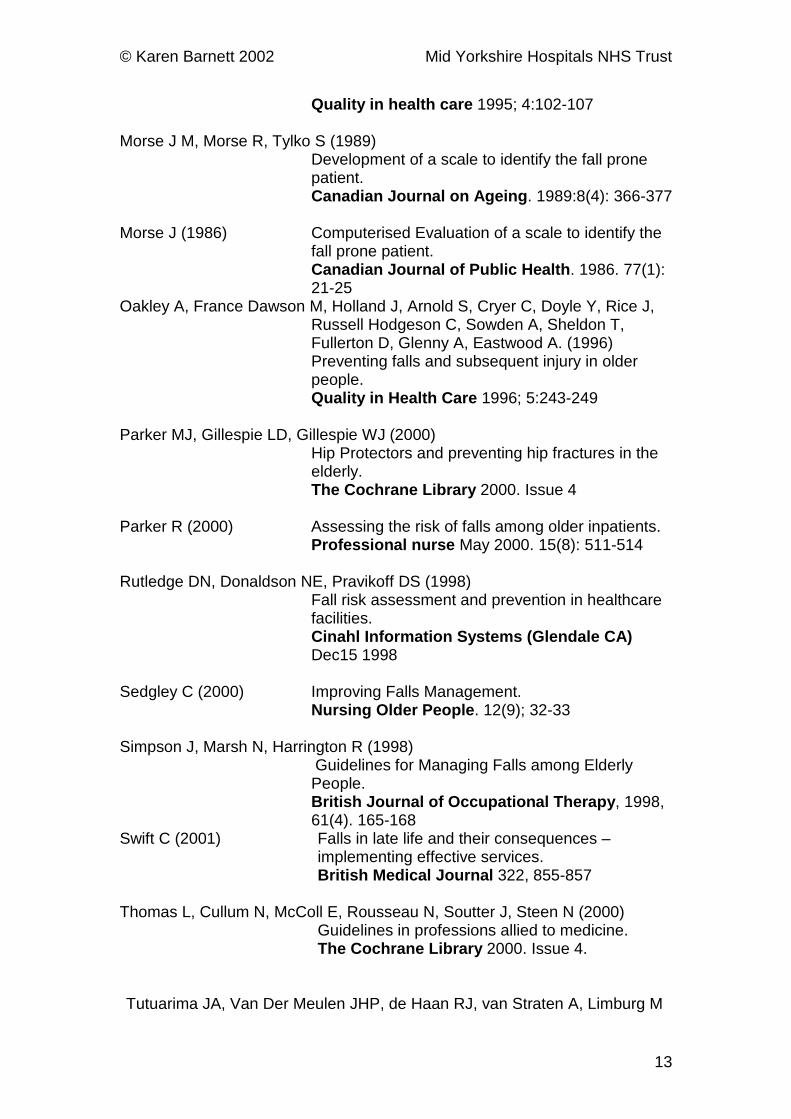
Quality in health care 1995; 4:102-107
Morse J M, Morse R, Tylko S (1989)Development of a scale to identify the fall pronepatient.Canadian Journal on Ageing. 1989:8(4): 366-377
Morse J (1986) Computerised Evaluation of a scale to identify thefall prone patient.Canadian Journal of Public Health. 1986. 77(1):21-25
Oakley A, France Dawson M, Holland J, Arnold S, Cryer C, Doyle Y, Rice J,Russell Hodgeson C, Sowden A, Sheldon T,Fullerton D, Glenny A, Eastwood A. (1996)Preventing falls and subsequent injury in olderpeople.Quality in Health Care 1996; 5:243-249
Parker MJ, Gillespie LD, Gillespie WJ (2000)Hip Protectors and preventing hip fractures in theelderly.The Cochrane Library 2000. Issue 4
Parker R (2000) Assessing the risk of falls among older inpatients.Professional nurse May 2000. 15(8): 511-514
Rutledge DN, Donaldson NE, Pravikoff DS (1998)Fall risk assessment and prevention in healthcarefacilities.Cinahl Information Systems (Glendale CA)Dec15 1998
Sedgley C (2000) Improving Falls Management.Nursing Older People. 12(9); 32-33
Simpson J, Marsh N, Harrington R (1998)Guidelines for Managing Falls among ElderlyPeople.British Journal of Occupational Therapy, 1998,61(4). 165-168
Swift C (2001) Falls in late life and their consequences –implementing effective services.British Medical Journal 322, 855-857
Thomas L, Cullum N, McColl E, Rousseau N, Soutter J, Steen N (2000)Guidelines in professions allied to medicine.The Cochrane Library 2000. Issue 4.
Tutuarima JA, Van Der Meulen JHP, de Haan RJ, van Straten A, Limburg M

© Karen Barnett 2002 Mid Yorkshire Hospitals NHS Trust
14
(1997) Risk Factors for Falls of Hospitalised StrokePatients.
Stroke. 1997; 28:297-301
Uden G, Ehnfors M, Sjostrom K (1999) Use of initial risk assessment andrecording as the main nursing intervention inidentifying risk of falls.Journal of Advanced Nursing 29(1), 145-152
Widder B (1985) A New Device to decrease falls.Geriatric Nursing, 6(5), 287-288
Wilson Eileen (1998) Preventing patient falls.AACN Clinical Issues, 9(1), 100-108
Wong S, Glennie K, Muise M, Lambie E, Meagher D (1981)An exploration of environmental variables and
patient falls.Dimensions in Health Service, 6, 9-11

© Karen Barnett 2002 Mid Yorkshire Hospitals NHS Trust
15
Morse Falls Risk Assessment
1.1 The falls risk assessment tool must be completed within 48 hours ofadmission.
1.2 The six categories of assessment are:♦ History of falling♦ Secondary diagnosis♦ Mobility Aids♦ Attachment to equipment♦ Gait♦ Mental status
1.3 History of fallingIf the patient has fallen immediately prior to admission or during thepresent hospital admission, score 25, If no history of falling score 0
1.3.1 If the patient has fallen immediately prior to admission or duringthe admission, even if the admission is some time ago, it is stillnecessary to score 25
1.3.2 If the patient suffered a physiological fall, such as a stroke,epilepsy or from impaired gait, immediately prior to admission, thiswill score 25
1.4 Secondary Diagnosis If the patient has more than one diagnosis in their records, score 15.
1.4.1 The diagnosis needs to be relevant and causing ongoing problems inorder to be included in the score. For example if a patient hashysterectomy indicated in their documentation it may be relevant if it isless than a year since the surgery and recovery is still occurring.However, if the surgery occurred 10 years ago and the patient is fullyrecovered then it is not a relevant diagnosis for this assessment.
1.4.2 The diagnosis would be relevant if the patient is taking prescribedmedication for the condition, even if they appear to be stable on themedication.
1.5 Mobility Aids1.5.1 If the patient walks without walking aids, walks with assistance of a
nurse, is on bed rest or completely wheelchair dependent then 0 isscored.
1.5.2 If the patient uses walking aids, such as a stick, frame, crutches, then15 is scored.

© Karen Barnett 2002 Mid Yorkshire Hospitals NHS Trust
16
1.5.3 If the patient does not use walking aids but grasps for furniture duringambulation, then score 30
1.6 Attachment to equipment1.6.1 If patient attached to IV fluids or syringe driver, Score 201.6.2 If a patient has a catheter and uses a stand rather than a leg bag,
Score 201.6.3 If not attached to equipment, Score 0
1.7 Gait Assessment of gait uses the terminology normal, weak, impaired gait.
1.7.1 Normal Gait (score 0) Patient walks with head erect, armsswinging freely at the side, striding unhesitantly.
1.7.2 Weak Gait (score 10) Patient is stooped but able to lift head whilewalking without losing balance. If support from the furniture is required,it is for reassurance only, rather than grabbing to remain upright.
1.7.3 Impaired gait (score 20) Patient may have difficulty rising from achair, attempting to get up by pushing on the arms of the chair and/orbouncing. Patient’s head is down and they watch the ground. Thepatient takes short steps and shuffles. Because balance is poor, theyare unable to mobilise without the support of a mobility aid,another person or furniture.
1.8 Mental status This relates to the patient’s ability to determine his orher own ability in mobilising.
1.8.1 Ask the patient “Are you able to go to the bathroom alone or doyou need assistance?”If the patient can answer consistently with your assessment of mobilitythen they are rated as normal (score 0)If they are inconsistent or unrealistic then they are considered tooverestimate his/her abilities and be forgetful of limitations (score 15)
1.9 The scores must be added together to produce a total score.
1.10 The total score will relate to a high/medium/low riskof falling, calibrated to your particular clinical area.
2. Care Planning and Nursing Documentation
2.1 A relevant care plan relating to the patient’s level of risk must be placedin the nursing documentation.
2.2 Any nursing care relating to preventing falls must be entered into thecare plan so that there is clear communication to all concerned aboutthe strategies in place aimed at reducing the risk of falling.
2.3 The patient must be informed at all times if any strategies for fallprevention are to be used
© Karen Barnett 2002 Mid Yorkshire Hospitals NHS Trust
17
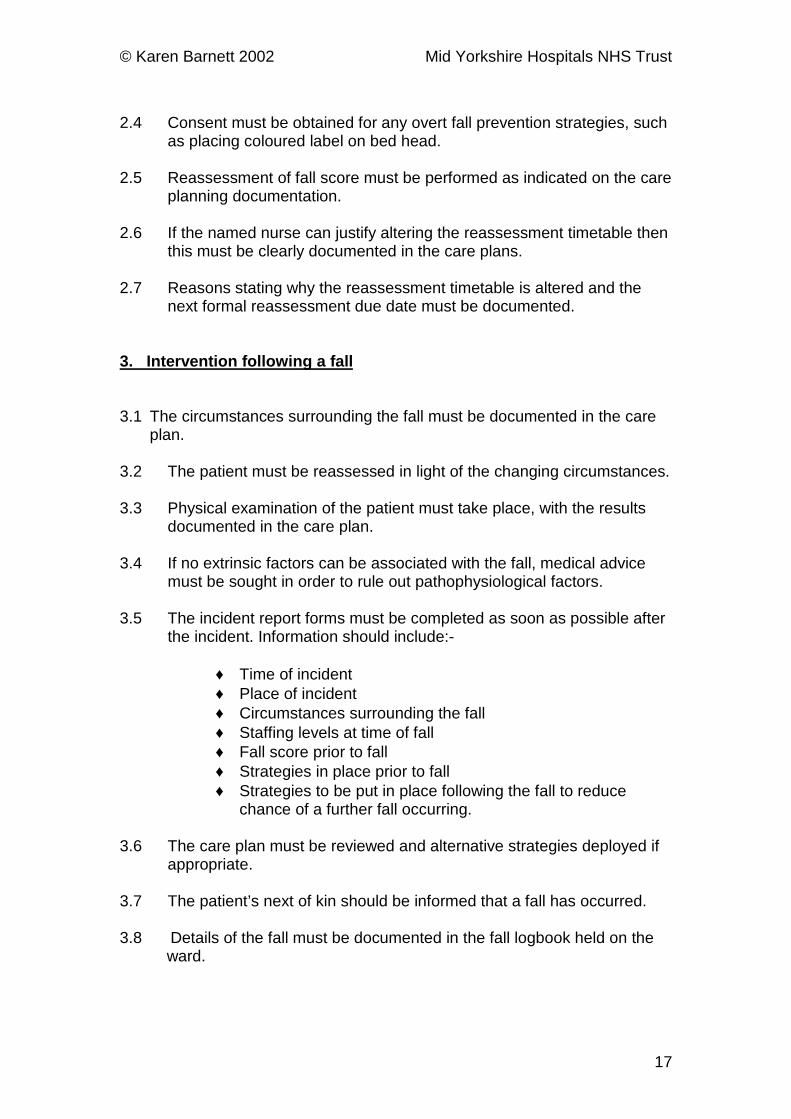
2.4 Consent must be obtained for any overt fall prevention strategies, suchas placing coloured label on bed head.
2.5 Reassessment of fall score must be performed as indicated on the careplanning documentation.
2.6 If the named nurse can justify altering the reassessment timetable thenthis must be clearly documented in the care plans.
2.7 Reasons stating why the reassessment timetable is altered and thenext formal reassessment due date must be documented.
3. Intervention following a fall
3.1 The circumstances surrounding the fall must be documented in the careplan.
3.2 The patient must be reassessed in light of the changing circumstances.
3.3 Physical examination of the patient must take place, with the resultsdocumented in the care plan.
3.4 If no extrinsic factors can be associated with the fall, medical advicemust be sought in order to rule out pathophysiological factors.
3.5 The incident report forms must be completed as soon as possible afterthe incident. Information should include:-
♦ Time of incident♦ Place of incident♦ Circumstances surrounding the fall♦ Staffing levels at time of fall♦ Fall score prior to fall♦ Strategies in place prior to fall♦ Strategies to be put in place following the fall to reduce
chance of a further fall occurring.
3.6 The care plan must be reviewed and alternative strategies deployed ifappropriate.
3.7 The patient’s next of kin should be informed that a fall has occurred.
3.8 Details of the fall must be documented in the fall logbook held on theward.
© Karen Barnett 2002 Mid Yorkshire Hospitals NHS Trust
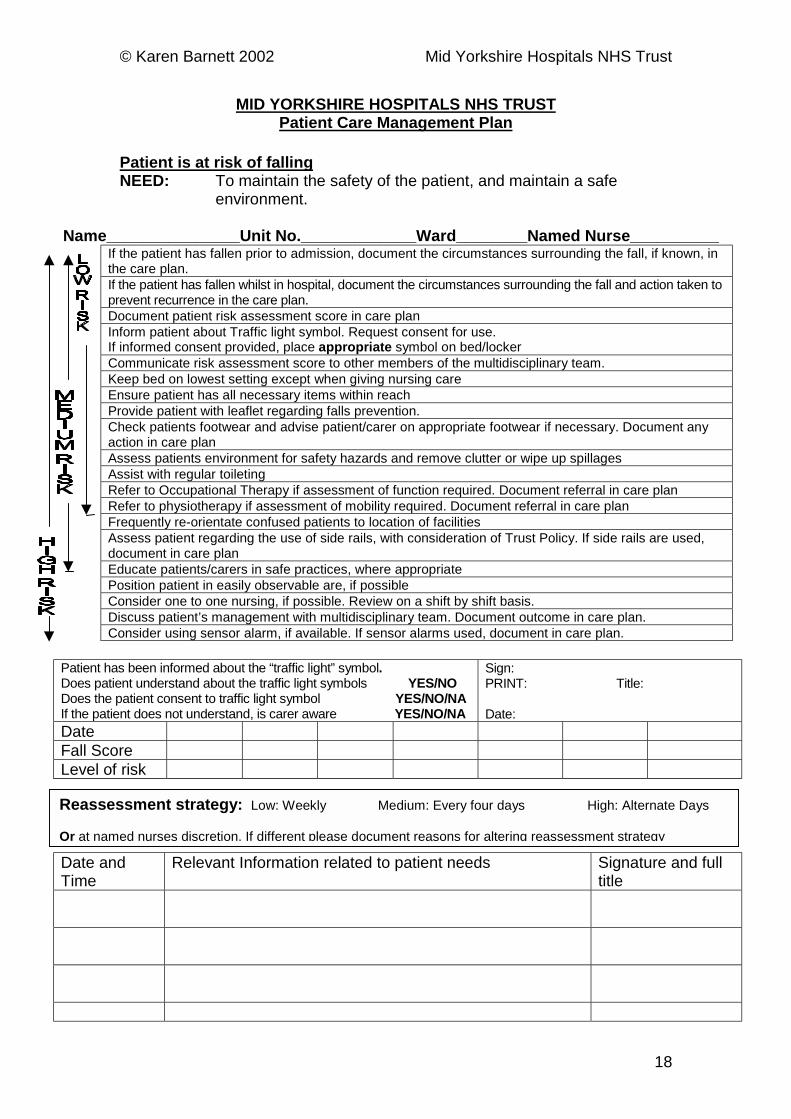
MID YORKSHIRE HOSPITALS NHS TRUSTPatient Care Management Plan
Patient is at risk of fallingNEED: To maintain the safety of the patient, and maintain a safe
environment.
Name_______________Unit No._____________Ward________Named Nurse__________If the patient has fallen prior to admission, document the circumstances surrounding the fall, if known, inthe care plan.If the patient has fallen whilst in hospital, document the circumstances surrounding the fall and action taken toprevent recurrence in the care plan.Document patient risk assessment score in care planInform patient about Traffic light symbol. Request consent for use.If informed consent provided, place appropriate symbol on bed/lockerCommunicate risk assessment score to other members of the multidisciplinary team.Keep bed on lowest setting except when giving nursing careEnsure patient has all necessary items within reachProvide patient with leaflet regarding falls prevention.Check patients footwear and advise patient/carer on appropriate footwear if necessary. Document anyaction in care planAssess patients environment for safety hazards and remove clutter or wipe up spillagesAssist with regular toiletingRefer to Occupational Therapy if assessment of function required. Document referral in care planRefer to physiotherapy if assessment of mobility required. Document referral in care planFrequently re-orientate confused patients to location of facilitiesAssess patient regarding the use of side rails, with consideration of Trust Policy. If side rails are used,document in care planEducate patients/carers in safe practices, where appropriatePosition patient in easily observable are, if possibleConsider one to one nursing, if possible. Review on a shift by shift basis.Discuss patient’s management with multidisciplinary team. Document outcome in care plan.Consider using sensor alarm, if available. If sensor alarms used, document in care plan.
Patient has been informed about the “traffic light” symbol.Does patient understand about the traffic light symbols YES/NODoes the patient consent to traffic light symbol YES/NO/NAIf the patient does not understand, is carer aware YES/NO/NA
Sign:PRINT: Title:
Date:DateFall ScoreLevel of risk
Reassessment strategy: Low: Weekly Medium: Every four days High: Alternate Days
Or at named nurses discretion. If different please document reasons for altering reassessment strategy
18
Date andTime
Relevant Information related to patient needs Signature and fulltitle

© Karen Barnett 2002 Mid Yorkshire Hospitals NHS Trust
19
© Karen Barnett 2002 Mid Yorkshire Hospitals NHS Trust
20
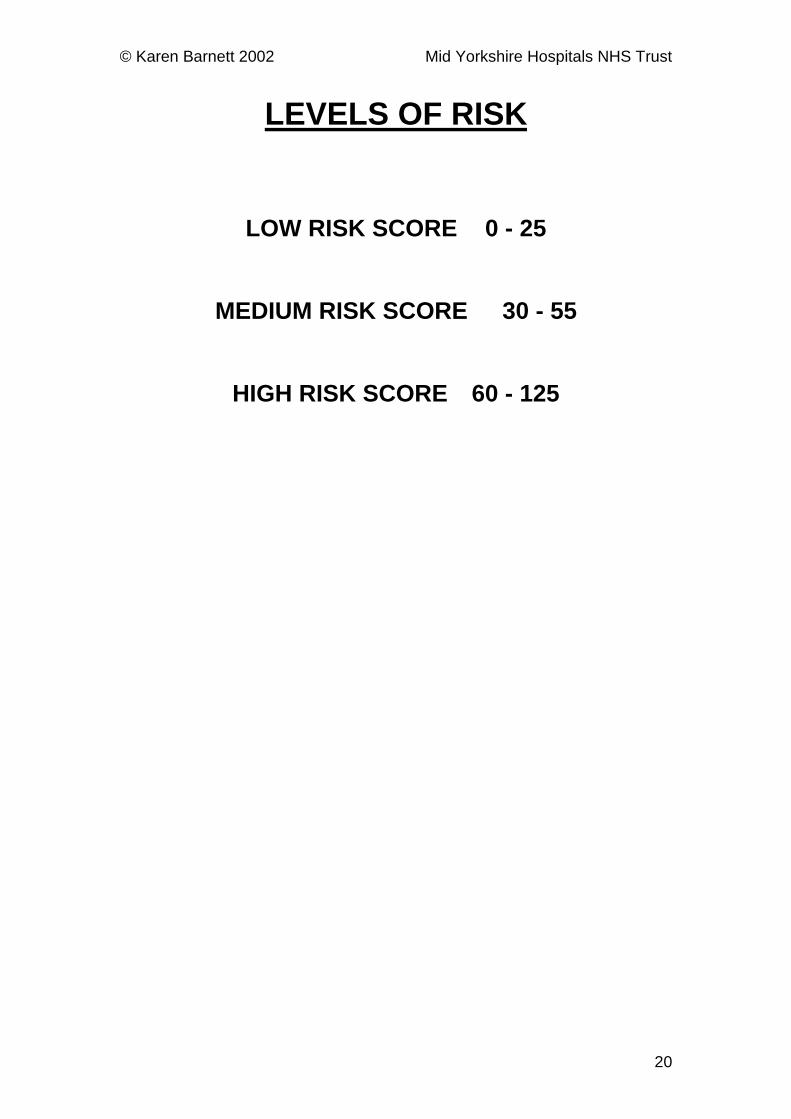
LEVELS OF RISK
LOW RISK SCORE 0 - 25
MEDIUM RISK SCORE 30 - 55
HIGH RISK SCORE 60 - 125

© Karen Barnett 2002 Mid Yorkshire Hospitals NHS Trust
21
Traffic Light Visual Cues
Visual Cues on individual patients beds are one strategy that is supported inthe literature to reduce the number of patient falls.
Each ward will be issued with a traffic light system. This will be 8cm laminatedcards that can be placed by the patients bed. This is intended to remindpermanent and peripatetic staff of the individual’s risk of falling.
RED HIGH RISK OF FALLING
YELLOW MEDIUM RISK OF FALLING
GREEN LOW RISK OF FALLING
It is recommended that all wards use the traffic light system so that there is aconsistent approach throughout the Trust.
However, some ward sisters/charge nurses may feel that it is inappropriate touse the system for some patients. If the system is not to be used, or if it isused for some but not all patients, it is advised that ward sisters write theirown policy for the use of the traffic light system and make sure that all staffworking on the ward (including visiting staff) are aware of how the level of riskis to be communicated on the ward.

© Karen Barnett 2002 Mid Yorkshire Hospitals NHS Trust
TRAFFIC LIGHT VISUAL CUES
LOW RISK OF FALLING
FMEDIUM RISK OF FALLING
HIGH RISK OF FALLING
FF
22

© Karen Barnett 2002 Mid Yorkshire Hospitals NHS Trust
23
Mid Yorkshire Hospitals NHS TrustReducing patient Falls – Environmental Assessment ToolWARD:………………… No. of Beds:………………….. LAYOUT OF WARD: (Nightingale/Cubicles/ beds per cubicle)
……………………………………………………………………………….
Client Group: ……………………………….Age Range:………………………………….Staffing Levels:
Shift Average TrustGuidelines
EarlyLateNight
GUIDELINES:
There is evidence to suggest that environmental factors contributesignificantly to the number of patient falls within the ward area. The followingenvironmental categories therefore require assessing within the ward area,toilet, bathroom and day room:
! Flooring! Temperature! Lighting! Space! Accessibility! Alarms! Equipment
An environmental assessment should be completedon an annual basis, or more regularly if there is
significant change in the ward environment.The assessment should be completed by the Ward
Sister or by an appropriately trained delegatedindividual.
The document should be copied and sent to theHealth and Safety Manager

© Karen Barnett 2002 Mid Yorkshire Hospitals NHS Trust
24
Assessment of flooringENVIRONMENT TYPE OF FLOORING EVEN/
UNEVENIN GOODREPAIR(Y/N)
CorridorNurses stationBed SpaceBathroomToiletDay room
Category Yes No CommentsTemperature
Is heating systemappropriate
Does heatingsystem workAre windows
easily openedLighting
Are corridorsclearly lit
Do bed lights workAre night lights
workingObstructions
Is thereappropriate
storage on theward
Are visitors chairsstored
appropriatelyAre hoists stored
appropriatelyAre wheelchairs
storedappropriately
Is patients mobilityequipment stored
appropriatelySpace
Is there adequateward spaceconsidering
number of beds

© Karen Barnett 2002 Mid Yorkshire Hospitals NHS Trust
25
Category Yes No CommentsIs there adequate
space to storeequipment
appropriatelyAccessibility
Are the doorseasily opened by
patients:a) toiletb) bathroomc) ward entry
Is the wardwheelchair
friendly?Is there sufficient
space for hoistaccess whereappropriate?
Is there sufficientspace for patients
to mobilise withmobility
equipment?Door entrysystems
What type ofsystem is in place
Do they workAre they regularly
maintainedDate of last check
SignpostsAre there signposts to toilet
facilitiesDo sign posts
indicate how touse open/close
doorsAlarmsAre the alarmseasily accessibleto patients in:a) toiletb) bathroomc) bedd) chaire) day room

© Karen Barnett 2002 Mid Yorkshire Hospitals NHS Trust
26
Category Yes No CommentsAre the alarms
audible to staff notat nurses station
Do all alarms workAre the alarms
visible to staff notat nurses station
Do the emergencypull cords work
Date of last check:Are there other
alarms used in theward
Are they regularlymaintained
BATHROOMToilet
Are thereadequate patienttoilet facilities on
wardAre there
adequate raisedtoilet seats
Are the raisedtoilet seats fitted
appropriatelyAre the raised
toilet seats in goodworking order
Are rails fitted inappropriate
positionIs the toilet roll
accessible topatients
Are there locks ontoilet door
Can access begained in anemergency
SinksAre sinks in good
working orderAre taps
appropriate forclient group

© Karen Barnett 2002 Mid Yorkshire Hospitals NHS Trust
27
Category Yes No CommentsAre there hot
water warningsigns
Do taps haveindicated hot/cold
Are there plugsavailable
If so are they onchains
Are sinks atappropriate height
for patient groupAre the sinksappropriately
positionedIs there a seat
available near thesink
Are thereappropriate places
for clothing/towels/ toiletries
Is there anaccessible mirror
for patientsBath
Is thereappropriate
manual handlingequipment
Is thereappropriate bath
board/seatavailable
Are they fittedappropriately
Does the bathhave non-slip base
Is theretemperature
control on the tapsShowers
Is there a showerseat
Is the shower seatsafe
Is there a non-slipfloor
© Karen Barnett 2002 Mid Yorkshire Hospitals NHS Trust
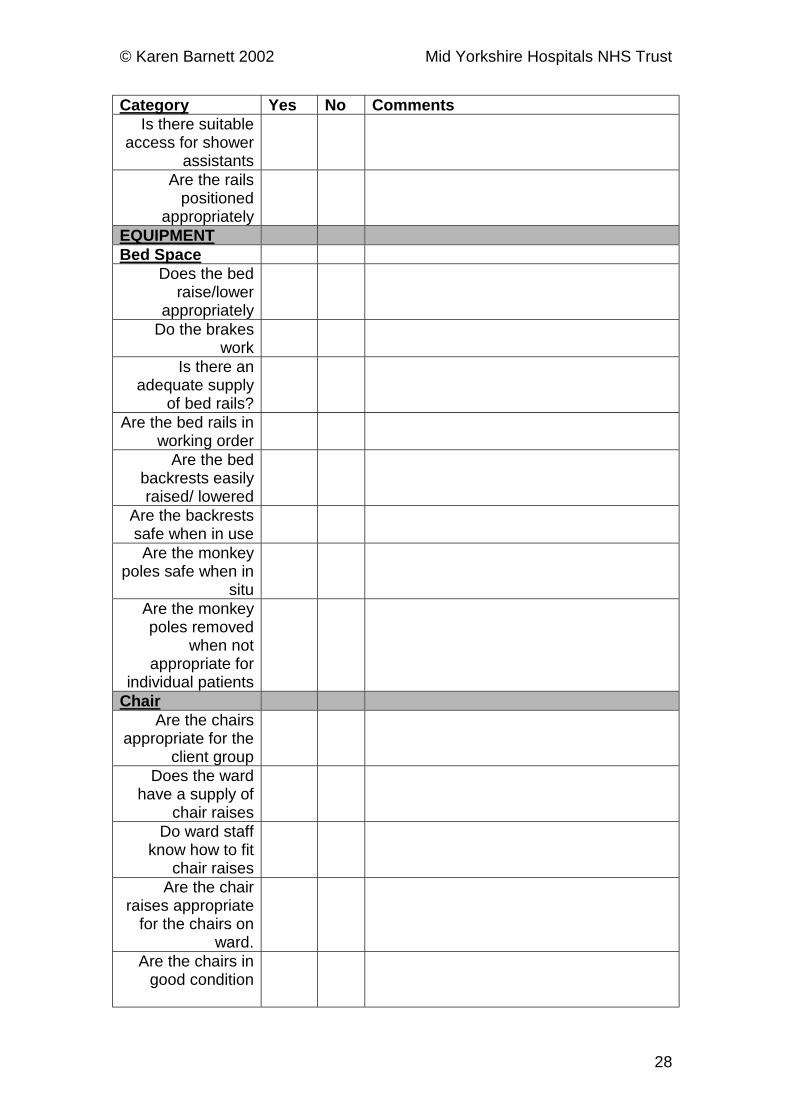
28
Category Yes No CommentsIs there suitable
access for showerassistants
Are the railspositioned
appropriatelyEQUIPMENTBed Space
Does the bedraise/lower
appropriatelyDo the brakes
workIs there an
adequate supplyof bed rails?
Are the bed rails inworking order
Are the bedbackrests easilyraised/ lowered
Are the backrestssafe when in useAre the monkey
poles safe when insitu
Are the monkeypoles removed
when notappropriate for
individual patientsChair
Are the chairsappropriate for the
client groupDoes the ward
have a supply ofchair raises
Do ward staffknow how to fit
chair raisesAre the chair
raises appropriatefor the chairs on
ward.Are the chairs in
good condition

© Karen Barnett 2002 Mid Yorkshire Hospitals NHS Trust
29
Category Yes No CommentsBed Tables
Do theyraise/lower
appropriatelyDo they wheel
easilyDo the tables have
brakesDo the brakes
workLocker
Are the lockersmobile
Are theyappropriately
positionedDrip StandsAre the drip stands
in good workingorder
Do they wheelevenly
Are theypositioned
appropriately toallow access in/out
of bed ifappropriate
CommodesIs there an
appropriateamount for client
groupAre they in good
working orderDo they have
removable armsDo the brakes
workDoes it manoeuvre
easilyCan it be
accommodatedwithin the bed
space safely

© Karen Barnett 2002 Mid Yorkshire Hospitals NHS Trust
30
Category Yes No CommentsWheelchairs
Are there enoughwheelchairs for the
patient groupDo they have a
maintenancecontract
Do the brakeswork
Are the tyrespumped fully
Are they storedappropriately
HoistsAre the
appropriate slingsprovided
Is the hoist storedappropriately
Do the brakeswork
Do they have amaintenance
contract
Are there any other pieces of equipment/ factors that need assessing withregard to patient safety?
Equipment Comments

© Karen Barnett 2002 Mid Yorkshire Hospitals NHS Trust
31
ENVIRONMENTAL RISK ASSESSMENT
Factors contributingto increased risk of
patient falls
Action taken tominimise risk
Further action requiredto reduce risk
Responsible Person
Risk assessment completedby:…………………………………………….(PRINT)…………………………………………(SIGN)
Date Risk assessment undertaken…………………………………………Next Risk assessment due on …………………………………………….Copy to :

© Karen Barnett 2002 Mid Yorkshire Hospitals NHS Trust
32
Patient Information
Am I at risk from falling?
One problem that has been highlighted through research is the high numberof patients that fall whilst recovering from illness or surgery in hospital.
It may be that whilst you are in hospital you may be more at risk of falling thanin your own home.
If you have had surgery, or spent some time in bed following an illness, youare weaker than usual.
It is common that once a fall has happened, a person will lose confidence andbe at higher risk of falling.
What is the ward doing to reduce the risk of falling?
Patients admitted to the ward will be assessed regarding their individual levelof risk within 48 hours of admission.
All members of staff involved in your care will be made aware of the results ofthe assessment so that they can consider what can be done to reduce thechance of you falling.
What can I do to reduce the risk of falling?
The staff are here to help you recover from your illness or surgery. If youneed their help, then ask.By working together we can reduce the chance of falling in the following ways:-
1. The nursing staff will ensure that the call system is within easy reach. Ifyou are unable to reach something from your locker/table use the callalarm system for help.
2. Wait for a nurse to come to you once you have alerted them with the callalarm. They will try to attend to you as quickly as possible.
3. If you do not feel you can manage to walk on your own, ask for help.Someone will walk with you until you feel safer on your feet.
4. Be aware that you will be weaker than usual after surgery or illness, or ifyou have been in bed for a long time.
5. Wear sensible footwear when moving around the ward. If slippers areworn, check that they fit snugly. Shoes should fit properly, have a low heeland be fastened so that they do not slip when walking.

© Karen Barnett 2002 Mid Yorkshire Hospitals NHS Trust
33
Is there anybody else that can help to reduce the risk of falling?
If the ward staff assess that you would benefit, you may be referred to aphysiotherapist or occupational therapist.
They will assess you and provide you with the necessary treatment in orderfor you to become more independent in walking, transferring or managing dayto day activities (washing, dressing, bathing, toileting).

© Karen Barnett 2002 Mid Yorkshire Hospitals NHS Trust
34
MID YORKSHIRE HOSPITALS NHS TRUSTGUIDELINES ON THE USE OF BED RAILS
Aims and Rationale of the Guidelines
These guidelines have been produced by the Reducing Patient FallsSteering Group to provide support to nurses and midwives in their
decision making process around the use of bed rails in wards,departments and in the home environment. This document draws
together best practice to prevent adverse incidents associated with theuse of bed rails. These guidelines should be used bearing in mind the
lack of evidence describing possible risk factors or preventionstrategies. The steering group asks individual practitioners to make
them aware of any additional evidence which becomes available.
Target Group
All nurses and midwives within the Trust.
Risks associated with the use of Bed Rails
Most commonly, nurses and midwives use bed rails to prevent patients fromharm. However indiscriminate use of bed rails can contribute to the risk ofinjury to the patient. Evidence suggests that inappropriate use of bed railsincreases agitation and increases the risk of falls. Bed rails increase thedistance a patient will fall and hence the greater the risk of injury (Marks 1992,Tineth 1992, Strumpf Evans 1998). Asphyxial deaths attributed to bed rail usehave also been reported (Ruben, Dube 1993, MDA HN 2000 (10) MDA SN2001(35)).
Other potential risks include obstructing the vision of the patient whichmay increase agitation. The patient may feel isolated, trapped or
imprisoned. This in itself can cause reduced esteem and dignity andsubsequently hinder the rehabilitation process.
Therefore, any nurse or midwife who applies any kind of restraint mustbe able to justify the reasons for using it. Bed rails should only be usedfollowing a thorough assessment of the patient, the risks involved and
alternatives explored.
Only extra height bed rails should be used on a bed with a mattress overlay.Electric profiling beds are fitted with bed rails as standard. The same riskassessment and decision making processes should be undertaken prior tobed rails on these beds being used.

© Karen Barnett 2002 Mid Yorkshire Hospitals NHS Trust
35
1Legal and Ethical Issues
Restraint
The use of bed rails are considered as a form of restraint. There is no preciselegal definition of what constitutes restraint but in broad terms restraint meansrestricting someone’s liberty, preventing them from doing something they wantto do. It is therefore important to ensure that nurses and midwives are fullyaware of their duty of care, assess the patient for riskand obtain informedconsent.
Bed rails are not considered a restraint when the patient requests them orwhen used for babies and young children.
Alternatives to the use of bed rails
Bed rails should only be used when all other methods of managing theidentified problems are not considered suitable or have failed.
Some alternatives suggested instead of the use of bed rails are: realityorientation, diversional therapy, consideration of the position of the bed inrelation to the ward environment and requesting relatives/carers to stay withthe patient for periods of time. Some patients may require nursing on amattress on the floor. This intervention would be as a result of a riskassessment and following discussion with the multidisciplinary team and thepatient’s relatives. In this case all staff must adhere to moving and handlingregulations.
Duty of Care
As a nurse or midwife, the code of conduct states that no action oromission on their part or within their sphere of influence is detrimentalto the condition or safety of the patient (UKCC 1992). The patient needs
are paramount and all care should be directed towards achieving andmaintaining the dignity of the patient.
Consent
Patients should be informed partners in their health care. Informedconsent should be obtained prior to bed rails being attached. For olderpeople with mental health needs informed consent is often difficult orimpossible to obtain. Families and/or carers and the multidisciplinaryteam should be involved in this process. Nurses and midwives have to
be especially careful to act only in the best interests of the patient.
2

© Karen Barnett 2002 Mid Yorkshire Hospitals NHS Trust
36
Principles of Practice
Assessment
All patients should have a documented nursing or midwiferyassessment made within 24 hours of admission which includes
maintaining a safe environment. The focus of the safety assessment willvary according to speciality, but in areas caring for elderly or cognitively
impaired patients specific consideration to the risk of falling from bedshould be documented.
Where assessment indicates the patient at risk of falling from bed, specificfactors such as hemiparesis etc., should be stated and documented clearly tosupport any decision for bed rail use. Involvement of the multi-disciplinaryteam is essential in this assessment at the earliest possible time.
If a patient who has been assessed as requiring bed rails but subsequentlyrefuses the use of the bed rails, it must be clearly documented. Furtherdiscussion with the patient/relative/carer and multi-disciplinary team must beundertaken.
Planning Care
If a patient is identified as at risk of falling from bed, a plan of care with anevaluation schedule should be formulated. The plan of care should detailactivities, which both investigates the cause and prevents immediate dangerfrom falling. The re-assessment strategy should be specified. Reassessmentshould be at least on a daily basis.
Where bed rail use is indicated, evidence should be documented that thepotential risk of injury from the bed rail and the use of protective bumpers hasbeen taken into consideration.
When a patient or carer specifically requests the use of bed rails bothprovision and non-provision should be considered. If there is anydisagreement of approach, further discussions and outcome should bedocumented.
Implementing Care
Prior to fitting, bed rails should be in good working order and checked forcompatibility with the beds they are being fitted to. Bed rails should be fittedin the correct position to ensure that they are not a risk to others and do notextend beyond the length of the bed.
At the time of fitting ensure that bed rails are assessed in combination with thebed and the patient to determine if any entrapment hazards exist. Care mustbe taken when selecting, positioning and adjusting bed rails to ensure thatany spaces within the rails or between the rails and mattress or parts of thebed do not allow entrapment of the patient’s head or body. Due care must

© Karen Barnett 2002 Mid Yorkshire Hospitals NHS Trust
37
also be taken to prevent injury to the patient when lowering the bed rails toperform interventions. Bed rails should be lowered in the event of a cardiacarrest.
Relevant discussion about the use of bed rails with the patient, relatives/carerand members of the multi-disciplinary team should be documented andshould include outcomes.
If an injury or fall occurs an incident form must be completed, the patientshould be re-assessed and the plan of care reviewed.
When bed rails are in use they should be inspected for defects and securityeach time they are raised. Each member of staff has a responsibility toremove unsafe equipment from use and report it. It is stipulated within theMDA safety notice MDA 2001(35) that those that use and fit bed rails shouldensure that:
1. All stored bed rails are inspected before issue to ascertain that they arecomplete and in good condition
2. All bed rails identified as defective are quarantined and under nocircumstances used
3. All bed rails fitted are inspected regularly to ensure that they are in goodcondition and appropriately installed
4. Bed rails inspected and found to have parts missing or damaged areremoved from the bed straight away
5. Beds should be maintained at the low position when bed rails are in use.
Evaluating Care
When bed rails are not required by the patient they should be removed fromthe bed, if appropriate and stored safely.
Ward Sisters should monitor the use of bed rails, monitor training needsof staff and meet these accordingly and evaluate their own use in
conjunction with the ward/department team.
Bed rails that are defective should be reported to the equipment librarymanager. They will then be checked and repaired if possible, or condemned.
Purchase of new bed rails
When bed rails are purchased consideration should be given to thecompatibility of the beds and the bed rails.
Within the Trust bed replacement programme, any new electric profiling bedswill have bed rails attached. However, those wards wishing to purchase newbed rails for old beds should purchase the recommended bed rails from thelist provided.

© Karen Barnett 2002 Mid Yorkshire Hospitals NHS Trust
38
The use of bed rails in the home environment should be monitored andnurses and midwives should evaluate their use in conjunction with the patient,carer and general practitioner.
A flow diagram is included to support decision making.
Timetable for Implementing
January/February 2001. Trustwide audit of current practice in relation touse of bed rails taking place.
Submission of new guideline January 2001.
Implementation of guidelines April/May 2001. Implementation will involveraising awareness presentations, dissemination of guidelines and audit ofguidelines implementations Summer 2001.
Review of guidelines February 2002
Audit tool linked with Nursing Charter developed Feb 2002 for use from April2002
4

© Karen Barnett 2002 Mid Yorkshire Hospitals NHS Trust
39
Review Process
Review date February 2003.
Reviewed annually by Nursing Directorate. Method for review will includereviewing the evidence available, audit of practice and audit of incidentsrelating to bed rail use.
Signature of Author ........................................................Date .............................
© Karen Barnett 2002 Mid Yorkshire Hospitals NHS Trust
40
REFERENCES AND BIBLIOGRAPHY
Marks W. Physical restraints in the practice of medicine. Current concepts.Ach Intern. Med 1992; 152: 2203. 2206.
Medical Devices Agency HN 2000 (10) July. Bed side rails (cot sides) Risk ofEntrapment and Asphyxiation.
Medical Devices Agency SN 2001 (35) December. Bed side rails (cot sides)Risk of Entrapment and Asphyxiation.
O’Keefe M.D. et al. Use of restraints and bed rails in a British hospital. JAGS.44: 1086 – 1088, 1996. American Geriatrics Society.
Royal College of Nursing (1987). Focus on Restraint – Guidelines on the useand restraint in elderly people.
Ruben B.S., Dube A.H. Mitchell A.K. Asphyxial death due to physicalrestraint. A case series. Arch Fam Med. 1993, 2: 405-408.
Strumpf N.E., Evans L.K. Physical Restraint of the hospitalised elderly:perceptions of patients and nurses. Nursing Res. 1988. 37: 32-137.
Tinetti M.E., Liu W.L. Ginter S. F. Mechanical restraints use and fall relatedinjuries among residents of skilled nursing facilities. Ann Intern Med. 1992116: 369-374.
UKCC (1992) Code of Professional Conduct.

© Karen Barnett 2002 Mid Yorkshire Hospitals NHS Trust
41
Protocol for the provision of hip protectors1) Assessment for suitability
Following admission the patient is assessed for the risk of falls usingthe Morse falls risk assessment tool and an appropriate care plan isthen implemented.
If the assessment score is over 65, and the patient has the following riskfactors then the named nurse then may suggest that the patient issuitable for hip protectors.
a) Patient under the care of the physiciansb) Morse falls assessment score of 65+c) Age 70+d) History of previous fallse) One or more of the additional risk factors:
i) Diagnosis of osteoporosisii) Low body weightiii) History of smokingiv) Family history of osteoporosisv) Poor lower limb muscle strength
It is important to include the patient in the decision making process and thatthey can be informed partners in their care.
Details regarding the rationale for providing hip protectors and patient consentmust be documented within the patient falls care plan.
The Modern Matron responsible for patient falls needs to be informed so thatthey can keep budgetary control and audit the effectiveness of the garmentswith regard to preventing hip fracture
2) Ordering of garments
A call off order for approximately 90 garments will be negotiated with thehip protector company (RobinsonCare) and a number of different
sizeswill be stored with the surgical appliances department on bothsites.
When a patient has been identified as requiring hip protectors a surgicalappliances request can be completed by the ward staff and signed by themodern matron responsible for falls.
The surgical appliances officer will provide the patient with the appropriatesize of garment.
It is anticipated that each patient will require 3 garments each, for launderingpurposes.

© Karen Barnett 2002 Mid Yorkshire Hospitals NHS Trust
42
3) Providing garments to patients
Once the garments have been given to the patient, they are then deemedto belong to the individual patient.
Laundering of garments can be undertaken by the hospital laundering serviceor by patients relatives. If they are to be laundered by the hospital then theymust have the patients name written clearly inside the garments.
4) Letter to GP/ Aftercare
Once the hip protector has been provided a note needs to be clearlymade on the patients notes, so that an audit trail can be developed.
A letter to the GP should be sent within the discharge documentation,detailing the rationale behind wearing the garments and requesting the GP toreview the patients compliance with the garments whenever they are seen.
5) Evaluation /Audit
If the patient is re-admitted to hospital, the modern matron responsible for fallsshould be informed and the corresponding audit information completed.

© Karen Barnett 2002 Mid Yorkshire Hospitals NHS Trust
43
Patient leaflet – hip protectors
Am I at risk of hip fracture?
You have been assessed by the ward staff as being at high risk offalling.
This may be because you have had surgery, or spent some time in bedfollowing an illness and be weaker than usual. It is common that once a fallhas happened, a person will lose confidence and be at higher risk of falling?
Most hip fractures in older people occur due to a fall on to the hip, as the armsare not strong enough to break the fall.
What can I do to reduce the risk of injuring myself?
The ward staff will discuss with you some of the ways to reduce the risk offalling. In some instances it may be appropriate to wear a device called a hipprotector.
What is a hip protector?
A hip protector is a padded plastic shield that is integrated into a pair of pants.It is designed to reduce the force exerted on the hip joint during a fall.
Where do I get hip protectors?
The nursing staff will discuss the options with you and you will decide togetherwhether hip protectors would benefit you. If you wish to wear them you will be
given 3 pairs by the hospital.
How do I care for hip protectors?
The garments can be washed in the same way as normal underwear at 60º C.
What happens when I am discharged?
The hip protectors are your property. You are advised to continue wearing hipprotectors while you are at risk of falling.
Your GP will be informed that you are wearing hip protectors and may be ableto replace them if you require further pairs at a later date. You will need todiscuss this with your GP on discharge from hospital.

© Karen Barnett 2002 Mid Yorkshire Hospitals NHS Trust
44
Sample Business Case for Hip Protectors
Hip Protectors
Hip fracture in older people is usually the result of a simple fall. Due to othermedical problems associated with ageing, hip fracture usually results inincreased morbidity and mortality. The majority of falls resulting in hip fractureoccur in females with an average age of 80 years1 and are due to the inabilityto put the arms out to prevent the fall and weaker bone strength2.
Strategies to reduce hip fracture include preventing bone fragility, increasemuscle strength around the hip, avoidance of falls and methods to attenuatethe impact on the hip during a fall. In this age group however, little can bedone to influence the prevalence of osteoporosis. Intervention strategies arealready in place within the acute Trust to assess the risk of falling onadmission and to put in place strategies to reduce the risk.
One approach to reduce the impact of falls is the use of hip protectors.Various types of hip protector have been developed. Most consist of plasticshields, which are kept in place by pockets within specifically designedunderwear.
Eighteen hip fractures occurred within the Medical CSU in 2000 as a result ofa fall. In order to reduce this level within the Medical CSU, it is proposed tosupply hip protectors to those individuals assessed as being most at risk fromfracture following a fall.
The evidence suggests that hip protectors do appear to reduce the risk of hipfracture within a selected population at high risk of sustaining hip fracture3. Itis therefore important to select appropriate individuals that would benefit fromthe intervention in order to avoid wasting valuable resources.
Strict inclusion criteria for hip protector provision would be recommended. Hipprotectors would be provided to those people admitted to the medical wardswith the following:
• Morse falls assessment score of 65+• Age 70+• History of falls
With one or more of additional risk factors:• Diagnosis of osteoporosis• Low body weight (under 9 stones)
1 Parker MJ, Pryor GA. (1993) Hip Fracture management. Oxford. Blackwell Scientificpublications2 Cummings SR, Nevitt MC (1989) A hypothesis: the causes of hip fracture. Journal ofGerontology 1989; 44:107-113 Parker MJ, Gillespie LD, Gillespie WJ(2000). Hip Protectors for preventing hip fractures inthe elderly (Cochrane Review) In: The Cochrane Library, Issue 4, 2000. Oxford: UpdateSoftware

© Karen Barnett 2002 Mid Yorkshire Hospitals NHS Trust
45
• History of smoking• Family history of osteoporosis• Poor muscle strength
This criteria is likely to be limited to a small number of people admitted to themedical wards in a year. It would therefore be appropriate to purchase asupply of hip protectors for 20 patients. In order to appropriately monitor theresource allocation it is important to put in place a mechanism for controllingthe supply of hip protectors. One person would be identified as responsible forissuing and tracking the resources and for ensuring the effectiveness of thehip protectors in a hospital setting.
Each patient supplied with the hip protectors would be provided with threepairs of garments. It would be envisaged that on discharge they wouldcontinue to wear the garments and that the GP will be informed that they havebeen supplied. If additional garments were required then the GP would beresponsible for supplying them.
Costs of supplying 20 people with hip protectors within Mid YorkshireHospitals NHS Trust.
Hip Protectors: £50.00 per pairPer Patient: £150.00 (for 3 pairs)
Supply of 3 garments for 20 patients £3000
Costs of hip fracture: 10 bed days at £204 per day = £2040 Hip replacement = £2113
In conclusion, there is strong evidence to suggest hip protectors are effectivein reducing the incidence of hip fracture in a selected group of patients. Theresource allocation of £3000 would be a beneficial inclusion within the Trustsfalls reduction strategy for those elderly people at high risk of falling and withadditional risk factors associated with hip fracture.