relationship betweendm5migu4zj3pb.cloudfront.net/manuscripts/102000/102268/...15 control 122 181.7...
TRANSCRIPT

STUDIES ONDIURETICS. II. THE RELATIONSHIP BETWEENGLOMERULARFILTRATION RATE, PROXIMALTUBULAR
ABSORPTIONOF SODIUMANDDIURETIC EFFICACYOF MERCURIALS1
By ROBERTF. PITTS ANDJOHNJ. DUGGANWITH THE TECHNICAL ASSISTANCE OFPHYLLIS MINER
(From The Department of Physiology, Syracuse University College of Medicine,Syracuse, N. Y.)
(Received for publication November 19, 1949)
According to Merrill (1) and Mokotoff, Rossand Leiter (2), renal plasma flow and glomerularfiltration rate are characteristically low in con-gestive heart failure. These investigators inferthat a reduction in the rate of delivery of sodium,chloride, and bicarbonate ions into tubules havingessentially normal reabsorptive capacities favorsretention of electrolyte and water. In line withthis concept Weston and Escher (3) observed thatpatients who fail to exhibit a satisfactory diureticresponse to intravenous mercurials often haveexceptionally low filtration rates, and that theadministration of aminophylline, which increasesfiltration rate, greatly enhances the diuresis.Others including Seymour (4), Briggs (5), andSinclair-Smith (6) have expressed doubt that areduction in filtration rate is either a constantor a significant finding in congestive failure, andhave observed loss of edema without any ac-companying increase in filtration rate or renalblood flow.
The difficulties in a clinical analysis of the roleof reduced filtration rate in the pathogenesis ofedema are evident. Chronic renal disease is oftenassociated with congestive failure, and reducedfiltration rate might in any given instance be morerelated to the former than to the latter. Further-more, compensation is usually reestablished slowlyand recovery of capacity to excrete salt and watermight be more a function of readjustment of tubu-lar absorptive capacity than of increased deliveryof filtrate into the tubules. The present study onthe dog was initiated with the view of establish-ing whether or not true glomerulo-tubular imbal-ance with relative overabsorption of water andsalt could be induced by a reduction in glomerularfiltration rate independent of changes in tubular
1 Aided by a grant from the National Heart Instituteof the National Institutes of Health.
function. Likewise it was hoped to determinewhether a reduction in filtration rate would reducethe effectiveness of mercurial diuretics.
It has been found that a relatively minor (25%)reduction in glomerular filtration rate very seri-ously impairs the capacity of the dog to excrete agiven load of water and electrolyte both undernormal conditions and following mercurial diu-retics. Weinfer from these experiments that in-sofar as filtration rate is reduced in congestivefailure, this factor contributes to the incapacity ofthe individual to maintain fluid and electrolytebalance, and furthermore limits the efficacy of thecommonly used mercurial diuretics. However, werecognize that such factors as increased venouspressure (7) and overactivity of pituitary andadrenal cortical water and salt conserving mecha-nisms (8, 9) may well play highly significantroles in the pathogenesis of edema and in the de-velopment of clinical mercurial resistance. No at-tempt has been made in this study to assess clini-cally the relative roles played by these several fac-tors. Wemerely feel that we have demonstratedthe fact that a reduction in filtration rate causesglomerulo-tubular imbalance, and that this imbal-ance must be considered as of some etiologic sig-nificance in any edematous patient who exhibits anacute reduction in filtration rate.
METHODS
Experiments included in this paper were performedon dogs lightly anesthetized with pentobarbital sodium(30 mg. per kg. intravenously) and on normal adultmale subjects. In all experiments, the clearance of para-aminohippurate has been used as a measure of minimumeffective renal plasma flow. In dogs the creatinine clear-ance, and in man the inulin clearance have been used asmeasures of glomerular filtration rate. Chemical meth-ods employed have been noted in the previous communi-cation (10).
372

STUDIES ON DIURETICS. II.
TABLE I
The effects of reduced renal arterial pressure on renal plasma flow, glomerular filtratson rate and the absorptionand excretion of sodium and water in an anesthetized dog
Plasma SodiumTotal Renal Renal Renal Glomerular Urine sodium _ _ _ _ _ _ _concurrent circulatory arterial plasma filtration flow concen-
time status pressure flow rate tration Filtered* Excreted Reabsorbed
Perce1t ofmins. mm./Hg cc.misn. cc./min. cc./mis. mEq./mi. mEq./misn. mE0./min. mEq./mis. jUltred
15 control 122 181.7 78.6 1.35 148.2 11.06 0.228 10.83 97.9430 control 124 175.3 79.5 1.73 146.5 11.06 0.302 10.76 97.2745 control 129 171.5 80.4 1.77 146.1 11.15 0.292 10.86 97.3860 aorta 70 161.1 70.3 0.60 147.3 9.84 0.072 9.77 99.2675 clamped 60 137.7 61.3 0.57 147.3 8.58 0.035 8.54 99.5990 control 137 169.6 75.4 4.53 147.0 10.53 0.294 10.24 97.21
105 control 134 161.2 76.8 6.43 149.1 10.81 0.379 10.43 97.51120 aorta 60 143.1 61.7 1.63 147.9 8.67 0.052 8.62 99.40135 clamped 50 118.1 53.3 0.80 146.7 7.43 0.022 7.41 99.70150 control 138 167.8 79.8 7.93 149.4 11.32 0.580 10.74 94.88165 control 147 147.8 77.4 7.44 149.4 10.98 0.594 10.39 94.60180 aorta 55 132.0 59.8 1.07 148.8 8.46 0.065 8.39 99.23195 clamped 50 129.2 57.4 1.00 149.1 8.12 0.045 8.07 99.45210 control 143 164.1 82.9 8.40- 148.2 11.66 0.838 10.82 92.82225 control 147 154.9 83.4 7.70 149.7 11.86 0.851 11.01 92.83
* Calculated with a Donnan factor of 0.95.
In the experiments performed on dogs a condition of and salt are retained relative to the load administeredpseudo-circulatory failure has been induced by the in- and extracellular fluid reserves are progressively ex-fusion of 0.85% sodium chloride at 10 cc. per minute for handed over a period of hours. After two and one-halfsome two and one-half hours prior to and throughout the hours of infusion the animal exhibits hypervolemia, ele-course of the experiment. Under these conditions water vated venous pressure, distended and pulsating jugular
ISM- rs
FIG. 1. THE EFFECTS OF REDUCEDRENALARTERIAL PRESsuRE6N RENALPLASMAFLOW, GLOMERULARFILTRATION RATE, FILTRATION FRACTION ANDSODIUM ExcRETION IN THE SALT ANDWATERLOADEDANIMAL
Data from Table I.
373

ROBERTF. PITTS AND JOHN J. DUGGAN
veins, moist riles in the lungs and some ascites. Severalreasons may be advanced for the utilization of this typeof preparation: (a) it mimics in some ways the stateof congestive failure in man; (b) it permits the adminis-tration of large doses of mercurial diuretics withoutcomplicating renal circulatory disturbances; and (c) byensuring a high rate of sodium and water excretion lini-tially, it magnifies the effects of alterations in filtrationrate.
The relationship between glomerular filtration rateand excretion of electrolyte and water in theanimal in positive sodium and fluid balance
The experiment described in Table I and Figure1 was performed on an anesthetized dog, in whichan adjustable clamp was placed on the aorta abovethe renal arteries but below the origin of the coeliacaxis. The clamp was introduced through a smalllumbar incision and could be opened and closedat will by a screw control which projected fromthe flank of the animal. The pressure referredto as the renal arterial pressure was actually the
Ef9
ala
~0co
t:'K
O0 60 70 s0Glomewrior FCratim Rae
04/M Il
FIG. 2. THE RELATIONSHIP BETWEEN GLOMERULARFILTRATION RATE AND THE PER CENT OF THE FiLTREDSODIUM ABSORBEDIN THE SALT AND WATERLOADEDANIMAL
Data from Table I.
mean femoral pressure (measured with a dampedmercury manometer), for the abdomen was notopened and the kidneys were not disturbed. Fortwo and one-half hours prior to, and throughoutthe course of the experiment, 0.85%o saline con-taining creatinine and para-aminohippurate wasinfused at a constant rate of 10 cc. per minute.The animal was in marked positive sodium andwater balance during the entire experiment, andexhibited the signs of "pseudo-circulatory fail-ure" described under Methods.
After three control collection periods the clampon the aorta was tightened to lower the meanfemoral, and hence the mean renal arterial pres-sure, from 129 mm. Hg to 70 and then to 60 mm.Hg. On release of the clamp the pressure rose toor above the control level. In the succeeding twoperiods during which the aorta was clamped, ar-terial pressure was reduced to 60 and 50 mm. Hg,and then to 55 and 50 mm. Hg respectively.Pressures were held at these values by continualadjustment of the screw clamp.
It is apparent that renal plasma flow and glo-merular filtration rate decreased during the inter-vals of reduced renal vascular pressure, but thatthe reductions were relatively small. On an aver-age, plasma flow and filtration rate were reducedby one-quarter or less. In contrast, striking re-ductions in sodium and water excretion occurredduring these intervals. With each reduction inrenal arterial pressure, sodium excretion fell pre-cipitously to a level only 1/10th to 1/20th that ofthe immediately preceding and succeeding periods.
It is evident from Table I that the absolute quan-tity of sodium reabsorbed was sharply reducedduring each period of clamping of the aorta as adirect consequence of the reduced sodium load de-livered into the renal tubules in the glomerularfiltrate. However, the proportion of the filteredsodium reabsorbed increased during the periodsin which filtration rate was reduced. This rela-tionship is graphically shown in the upper part ofFigure 2. In the lower portion of this figure, percent of filtered sodium absorbed is plotted as acontinuous function of filtration rate. As filtrationrate decreased from 83 to 53 cc. per minute, theproportion of the filtered sodium absorbed in-creased from 93 to 99.7%o.2
2The scatter of points in this chart indicates that un-controlled factors complicate the relationship between
374

STUDIES ON DIURETICS. .I.
Id UD 30 45 b60 5 90U IUD I0V 135 I>V IC5 Ul I95 2I1 225 240 255WIEU ESs
FIG. 3. THE EFFECTS OF REDUCEDGLOMERULARFILTRATION RATE ON SODIUMEXCRETION DURING MERCURIAL DIuREsIs IN THE SALT AND WATER LOADEDANIMAL
The relationship between glomerular filtration rateand proximal tubular absorption of electrolyteand water
From the experiment just described and othersof a similar nature,8 it is evident that the lowerthe volume of filtrate delivered to the tubules themore completely is the sodium and water reab-sorbed from that reduced volume of filtrate. Isthis the consequence of more complete absorptionin the proximal segment, perhaps as a result offiltration rate and sodium absorption, probably those fac-tors which underlie the progressive increase in sodiumexcretion which occurred during the course of the ex-periment. Although these factors have reduced any sig-nificance which could be attached to the form of thecurve, it has not altered qualitatively the fact that com-pleteness of reabsorption increases as filtration rate de-creases.
S Qualitatively similar results were obtained in twoadditional experiments performed in identical fashion.In a number of additional experiments without salt load-ing, reduction in filtration rate has been observed to beattended by a reduction in sodium excretion. However,results in these experiments have been less striking be-cause the initial rate of excretion has been lower; hencethe magnitude of reduction has necessarily been less.
reduced velocity of flow of tubular urine, or is itdue to the fact that less sodium is passed on fromthe proximal to the distal segment, and that thislesser quantity is more completely reabsorbed?
Evidence presented in a preceding paper (10)suggests that an intravenous dose of 100 to 120mg. Hg as mercuhydrin completely blocks the ab-sorption of sodium by the distal segment of therenal tubule. If, as seems probable, distal tubularabsorption is blocked in this manner, changes intubular absorption which occur in consequence ofalterations in glomerular filtration under suchcircumstances may be assigned to the proximalsegment.
The experiment shown in Figure 3 was per-formed in a fashion similar to that of the one justdescribed, i.e., the dog was anesthetized withpentobarbital; an aortic clamp was placed in posi-tion above the renal arteries; and an infusion ofsaline was given at a rate of 10 cc. per minute fortwo and one-half hours prior to starting the ex-periment. After two control periods, 120 mg.Hg as mercuhydrin were administered intra-venously. The excretion of sodium, which ini-
375
ROBERTF. PITTS AND JOHN J. DUGGAN
l . . .. . I50 60 70 80 90 100 10
Glometulor Filtration Ratec.c*/Atin.
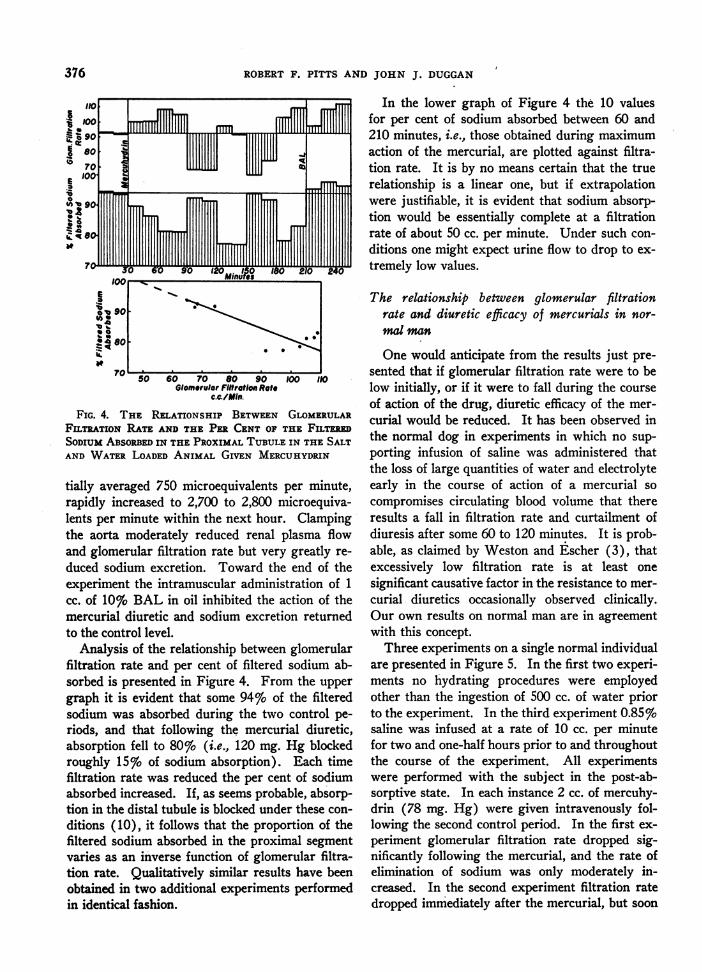
FIG. 4. THE RELATIONSHIP BETWEEN GLOMERULARFILTRATION RATE AND THE PER CENT OF THE FwTHRSODIUMABSORBEDIN THE PROXIMALTUBULEIN THE SALTAND WATERLOADEDANIMAL GIVEN MERCUHYDRIN
tially averaged 750 microequivalents per minute,rapidly increased to 2,700 to 2,800 microequiva-lents per minute within the next hour. Clampingthe aorta moderately reduced renal plasma flowand glomerular filtration rate but very greatly re-
duced sodium excretion. Toward the end of theexperiment the intramuscular administration of 1cc. of 10% BAL in oil inhibited the action of themercurial diuretic and sodium excretion returnedto the control level.
Analysis of the relationship between glomerularfiltration rate and per cent of filtered sodium ab-sorbed is presented in Figure 4. From the uppergraph it is evident that some 94%o of the filteredsodium was absorbed during the two control pe-riods, and that following the mercurial diuretic,absorption fell to 80%o (i.e., 120 mg. Hg blockedroughly 15%o of sodium absorption). Each timefiltration rate was reduced the per cent of sodiumabsorbed increased. If, as seems probable, absorp-tion in the distal tubule is blocked under these con-
ditions (10), it follows that the proportion of thefiltered sodium absorbed in the proximal segmentvaries as an inverse function of glomerular filtra-tion rate. Qualitatively similar results have beenobtained in two additional experiments performedin identical fashion.
In the lower graph of Figure 4 the 10 valuesfor per cent of sodium absorbed between 60 and210 minutes, i.e., those obtained during maximumaction of the mercurial, are plotted against filtra-tion rate. It is by no means certain that the truerelationship is a linear one, but if extrapolationwere justifiable, it is evident that sodium absorp-tion would be essentially complete at a filtrationrate of about 50 cc. per minute. Under such con-ditions one might expect urine flow to drop to ex-tremely low values.
The relationship between glomerular filtrationrate and diuretic efficacy of mercurials in nor-mal man
One would anticipate from the results just pre-sented that if glomerular filtration rate were to below initially, or if it were to fall during the courseof action of the drug, diuretic efficacy of the mer-curial would be reduced. It has been observed inthe normal dog in experiments in which no sup-porting infusion of saline was administered thatthe loss of large quantities of water and electrolyteearly in the course of action of a mercurial socompromises circulating blood volume that thereresults a fall in filtration rate and curtailment ofdiuresis after some 60 to 120 minutes. It is prob-able, as claimed by Weston and Escher (3), thatexcessively low filtration rate is at least onesignificant causative factor in the resistance to mer-curial diuretics occasionally observed clinically.Our own results on normal man are in agreementwith this concept.
Three experiments on a single normal individualare presented in Figure 5. In the first two experi-ments no hydrating procedures were employedother than the ingestion of 500 cc. of water priorto the experiment. In the third experiment 0.85%saline was infused at a rate of 10 cc. per minutefor two and one-half hours prior to and throughoutthe course of the experiment. All experimentswere performed with the subject in the post-ab-sorptive state. In each instance 2 cc. of mercuhy-drin (78 mg. Hg) were given intravenously fol-lowing the second control period. In the first ex-periment glomerular filtration rate dropped sig-nificantly following the mercurial, and the rate ofelimination of sodium was only moderately in-creased. In the second experiment filtration ratedropped immediately after the mercurial, but soon
376

STUDIES ON DIURETICS. II.
NORMALHYDRATION
R.FP
Renol Plosmo Flow (c-c /Man)
LomuuL4LLeWfM
lamerular Filtration Rate(ac IMin
Plasma Sodaum (m.EqI1L.)i
800
400
144141
1500
1000
500
NORMALHYDRATION
R.FR
Renal Plasma Flow (cc/Man)_ aaaFiII l ,
150
omerular Filtration Rate(cC/MaranrmT I
-100 ii
-50
Plasma Sodaum (m.rEq./L.)
TCU
1200
800
400
Mercuhydran
R FP
SALINE INFUSION
Renol Plasmo Flow (cc/Man)
150
Mercuhydran
FIG. 5. THE RELATIONSHIP BETWEENRENAL CIRCULATORYDYNAMICSAND DIURETIC EFFICACYOF A MERCURIALIN A NORMALMAN
Subject R. F. P.
NORMALHYDRATION
J.J.D.
Renol Plasma Flow (c.c./lin.)
W 200
Hill .=..Glomerulor Filtration Rote (cc/Min)O'PMIJL1 111111111111111111111111111111111
50 1
Plasma Sodium°0 (mEqI1L.)
Sodium Excretion(micro Eq./tlin.)
I*
1600
1200
800
142'39
SALINE INfUSION
J.J.D....
Renal Plasma Flow (cc./Min)
MlTDMfm200
rtm
'15LLLW UL~~IL
5 Glomerular Filtration Rote(c.c./minJ
100 Plasma Sodium (m.Eq./L.)
FIG. 6. THE RELATIONSHIP BETWEENRENAL CIRCULATORYDYNAMICSAND
DIURETIC EFFICACY OF A MERCURIAL IN A NORMALMAN
Subject J. J. D.
377
ISO
'100
r50
800
400
142139
1000
500
Mfercuhydran
120
so
40
143140'
2000'
1500
1000'
500
XIIIINTmwIIIIIII;lllllr_
rrrv- -lllllillllllll

ROBERTF. PITTS AND JOHN J. DUGGAN
recovered to the control level, and sodium excre-tion was somewhat enhanced. In the third ex-periment in which saline was administered, filtra-tion rate increased following the mercurial andlarge quantities of sodium were poured out in theurine.
In a second series on another normal subjectshown in Figure 6, peripheral circulatory collapseoccurred some 60 minutes after the mercurial.Renal plasma flow dropped from 943 to 136 cc.per minute and glomerular filtration rate de-creased from 153 to 45 cc. per minute. The ac-companying reduction in sodium excretion is remi-niscent of that observed on clamping the aorta inthe dog experiments. In the second experimentin which saline was infused, renal hyperemia andincreased filtration rate resulted from the mer-curial. Sodium excretion was much enhancedin consequence of the well maintained filtrationrate.
DISCUSSION
The observation that a moderate reduction inglomerular filtration rate very greatly restricts thecapacity of the kidney to eliminate water and salt,constitutes experimental evidence for the conceptthat glomerulo-tubular imbalance may well be asignificant factor in the pathogenesis of edema(11). According to this view, the delivery of areduced quantity of filtrate into tubules havingessentially normal reabsorptive function leadsto the retention of electrolyte and water. Mer-rill (12) maintains that edema accumulates inpatients with reduced cardiac reserve when fil-tration rate falls below 70 cc. per minute, i.e., be-low 60%o of the normal. In the experiments ondogs reported above, a 25% reduction in filtrationrate reduced excretion of salt and water by morethan 90%. Obviously these results cannot be ap-plied quantitatively in a consideration of fluid andelectrolyte metabolism in disease because. of theabnormally high salt and water loads imposed.Nevertheless the observation that a reduction in
4 This reaction, accompanied by pallor, faintness, chilli-ness, and nausea, was undoubtedly a manifestation of mer-curial toxicity not of salt and water loss per se. Toxicityof the mercurial is probably also the cause of the reduc-tion in filtration rate in the first two experiments onR. F. P. However the infusion of saline either protectedagainst or in some manner compensated for toxicity inboth subjects.
filtration rate leads to glomerulo-tubular imbalanceand relative overabsorption of sodium is quali-tatively significant. Indeed these findings andthose recently reported by Selkurt and his associ-ates (13) constitute the only direct experimentalevidence that a fall in filtration rate per se in-duces significant glomerulo-tubular imbalance.
A more serious criticism may be directed againstthe acute oneans by which these results were ob-tained, for edema characteristically accumulatesand recedes gradually. Whether tubular prepon-derance occurring in consequence of a reduction infiltration rate is sustained over relatively longperiods of time cannot be answered in experimentsof this type. It is possible that increased secre-tion of antidiuretic and adrenal cortical hormonesand increased venous pressure play more signifi-cant roles in maintaining glomerulo-tubular im-balance in congestive failure (7, 9, 11) than doesreduced filtration rate. Furthermore reduced hor-mone secretion and reduced venous pressure maybe more significant for the reestablishment of bal-ance than increased filtration rate (5, 6). How-ever, it is evident from the instantaneous changesin the rates of excretion of salt and water thatvariations in hormone activity played no role inour experiments, and that such changes as oc-curred were solely related to alterations in ar-terial circulatory dynamics. We infer that if areduction in filtration rate occurs during the ac-cumulation of edema, that occurrence will per secontribute to the establishment of positive saltand water balance. Wedo not infer that it is thesole etiological factor nor even the most significantone in the pathogenesis of edema.
The finding that the per cent of filtered sodiumabsorbed in the proximal tubule is inversely re-lated to glomerular filtration rate is at variancewith the view expressed by Wesson, Anslow andSmith (14) that a constant fraction of the filteredload is absorbed in the proximal segment. Thevalidity of our interpretation depends directlyupon the validity of the conclusion that large dosesof mercurial diuretics completely block the distaltubular absorption of sodium (10). Althoughconclusive proof is lacking, we feel that the weightof evidence is presently in favor of this concept.It is significant that Shannon (15) some. yearsago considered that reduced velocity of flow oftubular urine through the proximal segment favors
378

STUDIES ON DIURETICS. II.
absorption of electrolyte, and that as filtration de-creases to subnormal levels, absorption of sodiumbecomes essentially complete within this portionof the tubule.
If we accept the fact that proximal tubular ab-sorption is more complete at subnormal than atnormal filtration rates, it is evident that a givendecrease in filtration rate would cause a supra-proportional decrease in the quantity of electrolyteand water delivered to the distal segment. Henceeven were mercurial diuretics to block completelydistal tubular absorption of sodium, little wouldappear in the urine if the rate of glomerular filtra-tion were low. Our experiments support thisview and provide a rational explanation for thefinding of Weston and Escher (3) that those pa-tients who are clinically resistant to mercurialdiuretics have exceptionally low filtration rates,and that a satisfactory diuresis will result if filtra-tion rate can be increased by the administration ofaminophylline. It is, however, possible that exces-sive hormonal stimulation of tubular absorptionplays a significant or even in some instances adominant role in mercurial resistance.
CONCLUSIONS
It has been demonstrated in the dog that amoderate reduction in glomerular filtration ratevery greatly restricts the capacity of the kidney toeliminate water and electrolyte. We interpretour evidence as indicating that this reduction inexcretory capacity is largely due to relative over-absorption of salt and water in the proximal seg-ment in consequence of prolonged contact of thefiltrate with the tubular epithelium. If filtrationrate is significantly below normal, absorption inthe proximal segment may be so nearly completeand such small quantities of sodium may reach thedistal segment that even were complete blockageof absorption by a mercurial diuretic to result, aninsignificant increase in sodium excretion wouldoccur. The relation of these findings to the patho-genesis of edema and to the problem of clinicalmercurial resistance is discussed.
BIBLIOGRAPHY
1. Merrill, A. J., Edema and decreased renal blood flowin patients with chronic congestive heart failure:
evidence of "forward failure" as the primary causeof edema. J. Clin. Invest., 1946, 25, 389.
2. Mokotoff, R., Ross, G., and Leiter, L., Renal plasmaflow and sodium reabsorption and excretion incongestive heart failure. J. Clin. Invest., 1948, 27,1.
3. Weston, R. E., and Escher, D. J., An analysis of theunresponsiveness to mercurial diuretics observedin certain patients with severe chronic congestivefailure. J. Clin. Invest., 1948, 27, 561.
4. Seymour, W. B., Pritchard, W. H., Longley, L. P.,and Hayman, J. M., Jr., Cardiac output, blood andinterstitial fluid volumes, total circulating serumprotein and kidney function during cardiac failureand after improvement. J. Clin. Invest., 1942, 21,229.
5. Briggs, A. P., Fowell, D. M., Hamilton, W. F., Rem-ington, J. W., Wheeler, N. C., and Winslow, J. A.,Renal and circulatory factors in the edema forma-tion of congestive heart failure. J. Clin. Invest.,1948, 27, 810.
6. Sinclair-Smith, B., Kattus, A. A., Genest, J., andNewman, E. V., The renal mechanism of electro-lyte excretion and the metabolic balances of elec-trolytes and nitrogen in congestive cardiac failure;the effects of exercise, rest and aminophyllin.Bull. Johns Hopkins Hosp., 1949, 34, 369.
7. Wegria, R., Blake, W. D., Keating, R. P., and Ward,H. P., Effect of increased renal venous pressure onrenal function. Federation Proc., 1949, 8, 162.
8. Borst, J. G. G., The maintenance of an adequatecardiac output by the regulation of the urinaryexcretion of water -and sodium chloride; an es-sential factor in the genesis of oedema. Acta med.Scandinav., 1948, Suppl. 207, 1.
9. Fremont-Smith, F., The mechanism of edema forma-tion. New England J. Med., 1932, 206, 1286.
10. Duggan, J. J., and Pitts, R. F., Studies on diuretics.I. The site of action of mercurial diuretics. J.Clin. Invest., 1950, 29, 365.
11. Bradley, S. E., and Blake, W. D., Pathogenesis ofrenal dysfunction during congestive heart failure.Am. J. Med., 1949, 6, 470.
12. Merrill, A. J., and Cargill, W. H., The effect of ex-ercise on the renal plasma flow and filtration rateof normal and cardiac subjects. J. Clin. Invest.,1948, 27, 272.
13. Selkurt, E. E., Hall, P. W., and Spencer, M. P.Graded arterial pressure decrement and renalclearance of PAH, creatinine and sodium. Fed-eration Proc., 1949, 8, 143.
14. Wesson, L. G., Jr., Anslow, W. P., Jr., and Smith,H. W., The excretion of strong electrolytes. Bull.New York Acad. Med., 1948, 24, 586.
15. Shannon, J. A., The control of the renal excretion ofwater. I. The effect of variations in the state ofhydration on water excretion in dogs with dia-betes insipidus. J. Exper. Med., 1942, 76. 371.
379