republic of azerbaijan on the rights of the manuscript
TRANSCRIPT

REPUBLIC OF AZERBAIJAN
On the rights of the manuscript
ABSTRACT
of the dissertation for the degree of Doctor of Philosophy
SURGICAL TREATMENT OF IATROGENIC VESICO-VAGINAL FISTULAS AND WAYS
OF RESULTS IMPROVEMENT
Speciality: 3234.01 – Urology
Field of science: Medicine
Applicant: Elza Yusif Binnetova
Baku – 2021

2
The dissertation work was performed at the Department of Urology of Azerbaijan Medical University
Scientific supervisor: Corresponding member of ANAS, doctor of medical sciences, professor Sudeif Bashir Imamverdiyev,
Official opponents: doctor of medical sciences, professor Kamal Ismail Abdullayev
doctor of medical sciences, professor Eldar Yahya Huseynov
doctor of medical sciences Tofik Vahid Mekhtiyev
Dissertation council ED 2.06 of Supreme Attestation Commission under the President of the Republic of Azerbaijan operating at Azerbaijan Medical University
Chairman of the Dissertation council: doctor of medical sciences, professor
___________ Surhay Ismail Hadiyev
Scientific secretary of the Dissertation council: doctor of medical sciences, professor
___________ Fariz Hidayat Jamalov
Chairman of the scientific seminar: doctor of medical sciences, professor
___________ Alimardan Ashur Bagishov

3
GENERAL REVIEW OF THE WORK Relevance of the topic. Different iatrogenic lesions of urinary
genital organs may cause urinary phlegmon, peritonitis and urinary sexual fistulas. Urinary sexual fistulas is one of the main problems of urgent urogynecology1.
Flowing of urine through the uteral tract permanently during the uro-genital fistula causes ulcers in the external genital organs and extremity tissues, has an negative effect on both the social and sexual life of women and causes them to withdraw from society, become introverted and destroy their family life2.
Despite of conducting of scientific investigation on the urogenital fistulas, this subject still remains as actual by being one of the serious and continuous problems of urogynecology. The surgical treatment of vesicovaginal fistulas (VVF) has always been on the focus of the world medicine and new surgical suggestions, approaches, in the meantime, ways of restoring of fistula have developed for gaining of better results along the history and efforts were made for increasing of the success of surgical treatment. Despite of development of medicine at present time, difficult delivery in some countries and large operational interventions in small pelvic joints, laparoscopic operations and Caesarean operations in some countries, caused to increase the number of the VVF3,4.
50% of vesicovaginal fistulas develop as a result of total abdominal hysterectomy, 27,8% as a result of Caesarean operations and 22,2% as a result of delivery traumas in Turkish Republic5.
1Penalver, M., Angioli, R. Urinary diversion. Chapter 11 / In: Gleen Hurt W., editor. Urogynecologic surgery // Second ed. Lippincot: Raven Press, – 2000. – p. 193-206. 2Weston, K. Depression among women withobstetric fistula in Kenya / K.Weston, M.Stephen, J.Mwangi [et al.] // Int. J. Gynecol. Obstet., – 2011. 115, – p. 31-33. 3Лоран, О. Лечение болных со сложными мочевыми свищами / О.Лоран, Л.Синякова, Н.Твердохлебов [и др.] // Врач, – 2008. № 8, – с. 45-47. 4Ouedraogo, I., Payne, C., Nardos, R. Obstetric fistula in Niger: 6-month postop-erative follow-up of 384 patients from the Danja Fistula Center // Int. Urogynecol J., – 2018. 29 (3), – p. 345-351. 5Ateş, K. Experience of our surgery in iatrogenic vesicovaginal fistlas / K.Ateş,
4
The use of Laparoscopy and Da Vinci robotic systems in surgery also had an effect on the VVF removal operations6. New technologies are mainly alternative to the classical open abdominal transperitoneal and extraperitoneal transvesical VVF removal operations7.
As the location and number of fistulas are different, the conducted surgical operations are also different and surgeons choose approaches themselves. In this scientific investigation, we tried to define the surgical approaches by considering the location of fistulas, the condition, number and sizes of tissues and investigate the reasons for developing of recidive fistulas. The possibility of recidives permanently indicates the need for conducting of scientific investigations in this field for the present.
Object of the research. Women with vesicovaginal fistula removal operation made.
Aim of the research. To define the effect of moderan urological equipment on the selection of surgical approaches, the effect of 3 layer suture (additional end to end) technique on the results of operations and the reasons for developing of recidive fistulas.
Research objectives: 1. To analyze the ethiological factors causing vesicovaginal
fistulas to develop under the clinical materials. 2. To define the frequency of encountering of the applied
patients with the VVF in the central cities and regions. 3. To clarify the effect of conducting of cystoscopy, vaginal
examination, cystography, fistuloplasty, EU, CT, MRT examinaions on the selection of the approach of surgical operation in the diagnostics of vesicovaginal fistulas.
4. To define the effect of providing of hermeticity among the walls with 3 layer (additional end to end) stitches put on the urinary
R.Mehmet, S.Selçuk [et al.] // J. Turk Ger. Gynecol. Assoc., – 2010. 11, – p. 137-140. 6De, R. An update on surgery for vesicovaginal and urethrovaginal fistulae // Curr. Opin. Urol., – 2011. 21 (4), – p. 297-300. 7Hemal, A. Wadwa P. Robotic repair of vesico-vaginal fistula. In: Robotics in genitourinary surgery // London: Springer, – 2011. – p. 611-616.
5
bladder and vaginal wall without using any tissue loscut both with transvesical and transvaginal approaches in the surgical treatment of vesicovaginal fistulas on the results of surgical operations.
5. To investigate the reasons for developing of recidive fistulas in the VVF removal operations.
6. To investigate the opportunities of using of less invasive methods in the surgical operations of vesicovaginal fistulas and define their effectiveness in the prophylaxis of recidive fistulas.
Research methods. Cystoscopy, vaginal examination and cys-tography were used as the main diagnostic methods in the study.
Main thesis of the dissertation work to be defended: 1. The vesicovaginal fistulas are one of the most difficult
problems of the medical science and mostly develop due to the gynecological operations – total hysterectomy of uterine, subtotal hysterectomy of uterine and iatrogenic damage of the urinary bladder during Caesarean operations.
2. Defining of the location, size and number of fistulas by performing cystoscopic and vaginal examination in the diagnostics of patients assumes special importance in selection of transvaginal or transvesical surgical approaches.
3. There is importance in defining of the frequency of occurence of the applied patients with both preliminary and recidive fistulas in the central cities and regions as well as the properties of surgical operation of both groups.
4. Learning of the effect of gaining of hermeticity among the walls and 3 layer sutures performed in the urinary bladder and uterus tract without tissue loscut by avoiding of coarse manipulations while removing the fistula tract during the surgical operation on the results, has special importance.
5. The role of catheterization of urinary tract, selection of suitable urinary bladder drainage, provision of adequate operation of urinary bladder drainage in a post-operational period, uterus sanation and antibiotictherapy is important for prevention of the damage of urinary tract and its use for this purpose is unavoidable.
6. Defining of the effect of iatrogenic vesicovaginal fistulas on women’s family and working life and the physical and mental health

6
of their organisms, assumes special importance. Scientific novelty: - It was defined the sufficiency of conduction of cystoscopic
and vaginal examination in the diagnostics of the VVF, instructions on the transvesical and transvaginal VVF removal operations without the need for the EU, CT and MRT examinations (excluding the urinary tract lesions), superiority and insufficiency of approaches in the diagnostics of fistulas in our scientific investigation.
- To prepare examination algorithm in the VVF patients and conduct a patient’s tolerancy test for urethral catether along with localization and size of fistulas and changes in the extremity tissues for prescribing of instruction on every examination and choosing of the therapic tactics and drainage method of urine.
- To gain intertissue hermeticity with 3 layer (additional end to end) suture technique different from the classic VVF removal operations for decreasing of the number of recidive fistula.
Practical importance of the work: The necessity for increasing of professionalism of the
gynecologists, urologists as well as middle medical employees in the regions by encountering of the patients with vesicovaginal fistula and those with recidive fistula in the regions of Azerbaijan more, was defined.
An examination and a therapic plan was developed for preventing of developing of recidive fistulas in the VVF removal operations under the results obtained. All of these increase the importance of this research work and necessitate its use in a large practice.
The possibility for providing of three-layer and edditional end-to-end suture technique as well as hermeticity between urinary and uterine tracts, applying of failing to prevent from turning into the mucous membrane of the urinary bladder in practice.
The modern machines, equipment and suture materials used in our research work allowed to decrease the complications – hemorrhage, urinary tract infections and the number of recidive fistulas in the patients treated surgically with the diagnosis of urogenital fistula, reduce the number of hospitalization and improve
7
the far results of treatment. Approbation. The results of the research have been discussed in
different scientific meetings: the scientific conference dedicated to the 80th anniversary of the professor Abbas Akhundbayli Ahmad, the Honoursed Scientist (Baku, 2018), at the XV Symposium of Azerbaijani Urologists and Andrologists "Genetic Aspects of Urology and Reproductive Medicine" (Baku, 2019), at the XII Student Conference "The First Step in Science" (Sumy, 2021), at III International Scientifics-practical Conference "Theoretical and Practical Aspects of Science and Education Development" Lvov, 2021), at the scientific-practical conference "Actual problems of modern medicine and pharmacy" with the international participation of young scientists and students (Zaporozhye, 2021).
The preliminary discussion of the dissertation work was conducted in the meeting with the participation of employees of departments of “Urology”, “Obstetrics and Gynecology II” and “Surgical diseases III” of Azerbaijan Medical University (05.07.2018, protocol No. 9), the approbation of the work was conducted in the Approbation meeting of D 03.011 Dissertation Board pperating at Azerbaijan Medical University that conducts scientific seminars (07.11.2018, protokol No 13). The work was re-discussed at the scientific seminar of the Dissertation Council ED 2.06 operating at Azerbaijan Medical University (09.03.2021, protocol No 1).
Application of the results. Our research work was applied in the Republican Clinic Hospital named after the academician M.A.Mirgasimov which is the base of the Urological Department of Azerbaijan Medical University.
The name of the organization where the dissertation has been accomplished. The dissertation was completed at the Department of Urology of Azerbaijan Medical University.
Publications. 15 scientific articles on the results of the research have been published.
Volume and structure of the dissertation work. The dissertation is presented on 151 pages (192788 symbols) and contains introduction (5 pages, 8458 symbols), literature review (32
8
pages, 60879 symbols), chapter of material and research methods (19 pages, 19926 symbols), 3 chapters of own research results (61 pages, 74898 symbols), conclusion (11 pages, 20863 symbols), findings (1.5 pages, 2044 symbols), practical recommendations (1.5 pages, 2077 symbols) and bibliography (16 pages). The dissertation work is visualized in 37 tables, 18 figures, 6 charts and 4 schemes. The bibli-ographic index includes 161 works.
MATERIAL AND METHODS OF THE RESEARCH
Our research work included 53 patients exposed to
vesicovaginal fistula removal operation in the Urological Department of the Republican Clinical Hospital which is the base of the Urological Department within the years of 2005 and 2017. 24 patients were operated with transvaginal and 29 people with transvesical approach.
All of the patients were investigated for their anamnesis, complaints, approach of surgical operation, age groups, places of residence, body weigh indexes, diuresis, concomitant diseases, urinary calculus disease, chronicle cystitis, hydronephrosis, gynecological anamnesis, iatrogenic causes, fistula location, size and patients’ physical and mental indexes in a pre-operational period.
The patients’ ages were 45.3±1.4 (min-21, max-68) on average. 4 (7.5%) patients were under 30, 11 (20.8%) persons between 31 and 40 years old, 24 (45.3%) persons between 41 and 50 years old, 11 (20.8%) persons between 51 and 60 years old but 3 (5.7%) persons were over 60 years old (>60), the period of continuity of the disease was 43.4±12.4 (3-516) months. That is, a group of patients applied us early and another group of patients did it some years later.
The patients were placed in two groups according to their places in Baku, Sumgait (those living in the central cities) cities and regions. The persons living in Baku and Sumgait cities made up 11 (20.8±5.6%) patients and those living in the regions made up 42 (79.2±5.6%) patients.
20 (37.7±6.7%) patients did not have natural urinary act, the urine only flowed through the uteral tract. But other 33 (62.3±6.7%)

9
patients had both natural urinary act and the urine flowed through vagina.
8 (15.1±4.9%) persons out of the total patients had calculus disease in their urinary bladders, 3 (5.7±3.2%) patiens were disclosed to have concomitant (Calculous cholecystitis, Umbilical hernia) diseases, and 50 (94.3±3.2%) patients did not have other diseases. The women were taken into control by suitable specialists and they were operated for removal of umbilical hernia and cholecystitis along with the VVF removal operartion. The patients observed to have calculi in their urinary bladders were also conduced lithotripsy and cystolithotomy operations at the same time.
According to the gynecological anamnesis, 45 (84.9±4.9%) patients were pregnant and 8 (15.1±4.9%) persons never had pregnancy.
40 (75.5±5.9%) patients had delivery process but 13 (24.5±5.9%) patients did not have delivery cases. 3 (5.7±3.2%) women were observed to have abortion in their anamneses, 50 (94.3±3.2%) women did not have abortion in their anamneses. According to the anamnesis, 7 (13.2±4.7%) patients had Caesarean operations and the number of the patients who did not have Caesarean operation made up 46 (86.8±4.7%) persons.
In 15 (28.3±6.2%) women were obsered to have VVF removal operations before our operation and they were diagnosed of recidive fistula by us. 11 (20.8±5.6%) patients with recidive fistula had VVF removal operations for twice, 2 (3.8±2.6) patients for twice and 2 (3.8±2.6) patients for three times. 38 (71.7±6.2%) patients were considered as primary patients for the reason that they did not have any VVF removal operations before and they were conducted by as a surgical operation three months after they had the disease.
The patients with vesicovaginal fistulas were investigated for the development of fistula – ethiological facors. The information on ethiology is provided in the Table 1.
Our ovservations show that the percent of occurrence of the damage of urinary bladder during gynecological operations is high.

10
Table 1 Ethiological factors in patients
Reason of development of fistula Number of patients Total uteral hysterectomy with growths 21 (39.6±6.7%) Subtotal uteral hysterectomy 17 (32.1±6.4%) Difficult delivery 3 (5.7±3.2%) Caesarean operation 7 (13.2±4.7%) Trauma 2 (3.8±2.6%) After other operations 2 (3.8±2.6%) Fixation operation for uterus prolapse 1(1.9±1.9%)
Clinical observation of the patients with urinary and uterus
fistulas. The examination was begun with hearing the patients’ complaints and the main complaints were on the urination through uterus, kidney pain of the patients observed to have hydronephrosis during the USE examination, temperature and fever but pain and injection feeling in the middle part of the patients with calculus in their urinary bladders. The patients’ anamneses were collected and their place of residence, age, diseases and operations were specified and the period of illness was defined.
All our patients underwent general and biochemical blood analy-sis prior to surgery, determination of infections in the blood, urinaly-sis in patients urinating, ECG examination and review of patients over age 40 by a cardiologist, chest X-ray, Ultrasound scan of inter-nal organs. Since these examinations were performed in all preopera-tive cases, we did not determine their effect on the results of the sur-gical operation.
The patients were conducted a review as a diagnostic examination, vaginal examination, injection of colored fluid into the urinary bladder (physiological solution dyed with methylene blue), cystoscopy was conducted, location, size, number and relation of fistula with urinary tracts before the operation were defined and it was defined if there was a mass in the urinary bladder located in 2.5-3.0cm higher than supratrigonal-trigon, in the distance of 2.0-2.5cm from the openings of trigon-urinary tract and subtrigonal area as well as the approach of surgical operation was selected and cystography

11
was performed for a patient who was diagnosed hardly. External review is the most important examination during the
VVF operation that the urination through uterus is clearly seen during the review. Scar tissue, suture material or large fistula are felt with palpation. And the vaginal review enables to see the fistula tract.
Cystoscopy, vaginal examination (conducting of colored liquid test during the vaginal examination, click test - inserting of iron female catheter through uretra and taking it out of the fistula) and cystography were conducted as key diagnostic method. The patient was especially conducted vaginal examination while
selecting the approach of surgical operation, the condition of mucouse membram of uterus, diameter of vagina and in the meantime, the location of fistula in the external hole of the urinary bladder and inlet of uterus were specified and the possibility or impossibility of transvaginal manipulation was determined. The following results were gained according to the cystoscopic and vaginal examinations. The patients were conducted vaginal examination and the excretion of liquid from the uterus was seen and 39 (73.6±6.1%) patients were conducted cystoscopy, 19 (35.8±6.6%) patients were conducted click test during the vaginal examination, colored liquid was injected into the urinary bladders of 5 (9.4±4.0%) patients and 1 (1.9±1.9%) patient was performed cystography and her diagnosis of vesicovaginal fistula was approved.
The patients whose fistulas located in a supratrigonal way were 29 (54.7±6.8%) persons and the patients whose fistulas located in the subtrigonal and trigonal zone made up 24 (45.3±6.8%) persons.
We preferred the methods of vaginal and cystoscopic examinations during our scientific investigation and selected the approaches of surgical operation by specifyng the relation of the location of fistulas with urethras. All the patients with fistula were assessed by the anesthesiologist by passing through pre-operational examinations in the period before the operation and suitable anesthesia (general or spinal) was planned and the general principles of fistula removal operations were followed during the surgical operation.

12
Mathematical and statistical methods of analysis. All of the numerical indexes gained in the course of the research were conducted with the use of variation, discriminant and dispersion methods by considering modern advice. All calculations were made in EXCEL-2013 electronic table and SPSS-20 package program but the results were summed up in the tables and diagrams.
RESEARCH RESULTS AND THEIR DISCUSSION
164.0±11.6 (min-70, max-540) minutes were spent on the VVF
removal operation on average. As the urinary tracts of 5.7±3.2% patients were involved in fistula, cystoneostomic operation was needed along with the VVF removal operation and 7.5±3.6% patients whose openings of urinary tracts were very close to fistula, were conducted catheterization for preventing of damaging of the urinary tracts.
The total period of hospitalization of the patients 21.2±1.2 (min-11, max-62) days on average and the post-operational period of hospitalization was 16.6±1.1 (min-5, max-54) days8.
There were gained recovery of 96.2±2.6% patients in the first operations while assessing for far results and success was made in 3.8±2.6% patients after the second operation (Table 2).
It was defined that the age of the patients with primary VVF was 44.4±1.6 (min-21, max-67), the period of continuity of the disease was 30.6±9.3 (min-3, max-324) months, the period of continuity of the disease in the group of recidive patients was 75.9±36.6 (min-3, max 516) months. The age of the patients with recidive vesicovaginal fistula was 47.5±2.7 (min-31, max-68), p=0,374, the patients’ BMI was 27.4±1.5 (min-19, max 40.4) kg/m2 (p=0.423). 10 (26.3±7.1%) persons of the primary patients was those living in the central cities and 28 (73.7±7.1%) persons were the ones living in the regions. Only
8İmamverdiyev, S.B., Binnətova, E.Y. Veziko-vaginal fistulaların diaqnostika və müalicəsi // – Bakı: Azərbaycan Təbabətinin Müasir Nailiyyətləri, – 2015. № 2, – s. 121.

13
1 (6.7±6.4%) persons of the patients with recidive VVF lived in the central cities and 14 (93.3±6.4%) persons were those who lived in the regions p=0.112.
Table 2
Causes of recidive fistula
Factors VVF removal
operation Total χ2 Р N/A Yes
Reaction to urethral catheter
Number 2 – 2 0.820 0.365 % 5.3% 3.8% Urinary tract infection
Number 1 – 1 0.402 0.526 % 2.6% 1.9%
Recidive Number 1 1 2 0.482 0.487 % 2.6% 6.7% 3.8% The period of continuity of the operation of the primary patients
changed between 157.5±11.1 (min-70, max-340) minutes and the period of continuity of the surgical operation of the patients with fistula was 180.3±30.0 (min-75, max-540) minutes (p=0379, F=0.787).
Statistical difference for catheterization of the urinary tract among the groups of patients with primary and recidive fistula was defined to be (p=0.001). Thus, in such cases, the urinary tracts may be involved in fistula that leads to the performance of catheterization of the urinary tract and technical difficulties in conducting of VVF removal operations, extending of the period of continuity of surgical operation (157.5±11.1, min-70, max-340) minutes to 180.3±30.0 (min-75, max-540) minutes, keeping of the urethral drainage in the postoperational period for longer time and longer period of hospitalization9. 9Биннетова, Э.Ю. Наш опыт в лечении рецидивных и первичных везико-вагинальных фистул // – Тюмень: Медицинская наука и образование Урала, – 2019. № 4, – с. 83-88.

14
The total period of hospitalization of primary fistulas was 19.5±1.0 (min-11, max-44) days and the total period of hospitalization of the patients with recidive fistula was 25.3±3.2 (min-13, max-62) days, (p=0.030, F=5.016). İt üas defined that the hospitalization of the primary patients in the post-operational period was 15.1±1.0 (min-5, max-42 days), the hospitalization of the patients with recidive fistula in the post-operational period was 20,6±2,9 (min-8, max-54) days (p=0.026, F=5.267).
The VVF removal operations of the patients were conducted with two etnrances as transvesical and transvaginal (Figure 1).
a)
b)
Fig. 1. Transvaginal (a) and Transvesical (b) VVF removal operations

15
As calculi were observed in the urinary bladders of 8 (15.1±4.9%) patients, 6 (11.3±4.4%) persons were conducted cystolithotomic operations concomittantly and 2 (3.8±2.6%) persons exposed to transvaginal VVF removal operations, were conducted lithotripsy operations.
The urinary tract openings of 3 (5.7±3.2%) patients directly opened into the fistula tract and cystoneostomic operation was needed.
The catheterization of the urinary tracts of 4 (7.5±3.6%) patients whose fistula was close to the openings of the urinary tracts was conducted for preventing of the damage of the urinary tracts.
The drainage of the urinary bladder in the operations was applied in two methods. The patients having reacion to the urethral catheter in their anamneses and a group of patients exposed to transvesical VVF removal operation were applied suprainguinal drainage. 35 (66.0±6.5%) persons of the patients were placed urethral drainage and 18 (34.0±6.5%) persons were applied suprainguinal drainage. The patients for whom long absorbable (Vicryl No. 2/0, 3/0, 0) threads were used as suture material, made up 43 (81.1±5.4%) persons but the number of the patients for whom ordinary catgut, chromic catgut and Vicryl were used made up 10 (18.9±5.4%) persons.
The average age index of the patients in transvaginal group was 46.2±1.8 (min-21, max-66) age and the ages of the patients in the transvesical group was 44.6±2.1 (min-23, max-68), p=0.556 (χ2=3,193).
The period of continuity of the disease of the patients in the transvaginal group was 43.6±21.4 (min-3, max-516) months and the period of continuity of the disease of the patients in the transvesical group was 43.2±14.6, min-3, max-324 months.
7 (29.2±9.3%) patients lived in Baku and Sumgait cities but 17 (70.8±9.3%) patients lived in the regions and the residential place of 4 (13.8±6.4%) persons in the other group was the central cities (Baku, Sumgait) and the residential place of 25 (86.2±6.4%) persons was the regions (p=0.170 χ2=1.887).
The height of the patients in the transvaginal group was

16
160.5±1.2 (min-150, max-172) cm, their weight was 73.9±3.1 (min-48, max-110) kg, BMI was 28.7±1.1 (min-20,9, max-40.4) kg/m2. The height of the patients exposed to surgical operation with transvesical approach was 160.2±1.0, min-146, max-170 cm on average, their body weight was 70.8±3.3, min-47, max-110 kg on average. The BMI was 27.6±1.3 (min-19, max-45.2) kg/m2, p=0.563.
All of the patients who were conducted the transvaginal VVF removal operation, were applied 24 (100%) urethral drainage, the patients exposed to surgical operation with transvesical approach, were used suprainguinal drainage and the urinary bladders of 11 (37.9±9.0%) patients were drained with urethral catheter and 18 (62.1±9.0%) patients were drained by inserting suprainguinal three-way catheter (χ2=22.558; p<0.001). 3 (10.3±5.7%) of the patients with transvesical group were applied urinary tract catheterization for preventing of the damage of urinary tract (χ2=0.718; p=0.397) .
The total hospital days of the patients exposed to the surgical operation with transvaginal approach made up 20.5±1.0 (min-11, max-38) days and the total hospital days of the patients exposed to the surgical operation with transvesical approach made up 22.0±2.0 (min-12,max-62) days, (F=0.583, p=0.449).
But the post-operational hospital days were defined to be 15.8±1.0 (min-5, max-29) days in the transvaginal group and 17.4±1.9 (min-7, max-54) days (F=0.513, p=0.477) in the transvesical group.
The time spent on the surgical operation of the patients included in the transvaginal group was 112.3±5.9 (min-70, max-180) minutes, the period of operation of the transvesical group continued for 206.7±16.9 (min-90, max-540) minutes and the differences of staistical importance between the groups were p<0,001, that is, more time was spent on the VVF removal operation with transvesical approach.
While the patients of the transvesical group were investigated for their far results, the recovery was gained in (100.0%) patients not observed to have recidive and assessed as well as the recovery was gained by assessing 22 (91.7±5.6%) patients conducted VVF removal operation with transvaginal approach well for their far

17
results, 2 (8.3±5.6%) patients were defined to have recidive fistula by being assessed as unsatisfactory (p=0.113, χ2=2.511). The main reason for the VVF recidives 2 (3.8±2.6%) was the reaction to the catheter and these patients (chronic cystitis and decrease in urine) experienced the activation of infection of urinary bladder and tenesmus after fistuloplasty10.
Thus, it becomes clear from our observations that vesicovaginal fistuloplasty surgery requires special experience to pay attention to the cause of the fistula, the history of chronic cystitis, which is often exacerbated and the level of urinary capacity.
Study of patients' quality of life. Investigations were also conducted to define the effect of the existence of uteral fistula of the urinary bladder on the social life of patients. 30 persons were conducted physical and psychological tests for defining of the physical and mental indexes of health.
The problems of patients with fistulas had a serious impact on their social lives, psychological and emotional state in the family, and led to mistrust, the restriction of social life, tension in family life and alienation from their professions. It takes a long time to improve the psychological and emotional state of patients.
Quality of life of patients after vesicovaginal fistula removal operations in primary and recurrent fistulas. A survey was con-ducted to assess the quality of life in patients with primary and recur-rent fistulas, statistical differences between groups were not identi-fied, and all patients were in the same psychological and physical condition. Based on this test, it becomes clear that there is no differ-ence between the physical and mental health of groups of patients with and without a history of fistula removal surgery, all of them have poor emotional state and mental health, they avoid participating in different social activities. The mental and physical quality indica-tors of patients in groups of patients with different iatrogenic causes were determined and it was found that patients had low levels of mental and general health and did not participate in social activities. 10İmamverdiyev, S.B., Binnətova, E.Y. Transvezikal və transvaginal girişlə veziko-vginal fistula ləğvi əməliyyatlarının nəticələri // – Bakı: Sağlamlıq, – 2017. № 5, – s. 180-185.
18
Physical and mental indicators of health were determined by ap-plying a Kruskal-Wallis test for operations that cause the formation of a vesicovaginal fistula. The iatrogenic cause was PF (p=0.635), RP (p=0.315), BP (p=0.838), GH (p=0.657), VT (p=0.694), SF (p=0.223), RE (p=0.013), MH (p=0.322) among statistically honest significant differences between the physical and mental health indi-cators of health of other patient groups with subtotal hysterectomy of the uterus.
The cause was PF (p=0.174), RP (p=0.197), BP (p=0.948), GH (p=0.782), VT (p=0.735), SF (p=0.612), RE (p=0.816), MH (p=0.300) among the physical and mental indicators of health of oth-er patient groups with total hysterectomy of the uterus. Based on this test, it is clear that iatrogenic causes have no significant impact on the indicators of their physical and mental health.
Among age groups, patients with cystitis in the postoperative pe-riod and assessment of close results were of statistically significant. It turns out that the presence of symptoms of cystitis in patients over age 50 in the postoperative period negatively affects patients' physi-cal health.
According to this test, statistically honest significant differences between the physical and mental indicators of health of these patient groups were PF (p=0.444), RP (p=0.940), BP (p=0.255), GH (p=0.079), VT (p=0.855), SF (p=0.056), RE (p=0.7310, MH (p=0.823). It is clear that there is no difference between the physical and mental health indicators of groups of patients of different ages. That is, patients with vesicovaginal fistulas have the same physical and mental health regardless of age.
The impact of the duration of the disease on the physical and men-tal indicators of patients' health was determined as PF (p=0.444), RP (p=0.940), BP (p=0.255), GH (p=0.079), VT (p=0.8550, SF (p=0.056), RE (p=0.731) and MH (p=0.823). Based on this test, it can be concluded that the duration of the disease has no significant impact on the physical and mental health of patients, and these pa-tients are in almost the same physical and psychological condition.
The iatrogenic cause of caesarean section and other patients was PF (p=0.056), RP (p=0.978), BP (p=0.716), GH (p=0.831), VT
19
(p=0.021), SF (p=0.088), RE (p=0.131), MH (p=0.160). Based on this test, it is clear that patients who do not have a history of caesare-an section perform their physical functions more comfortably and have higher vital activities.
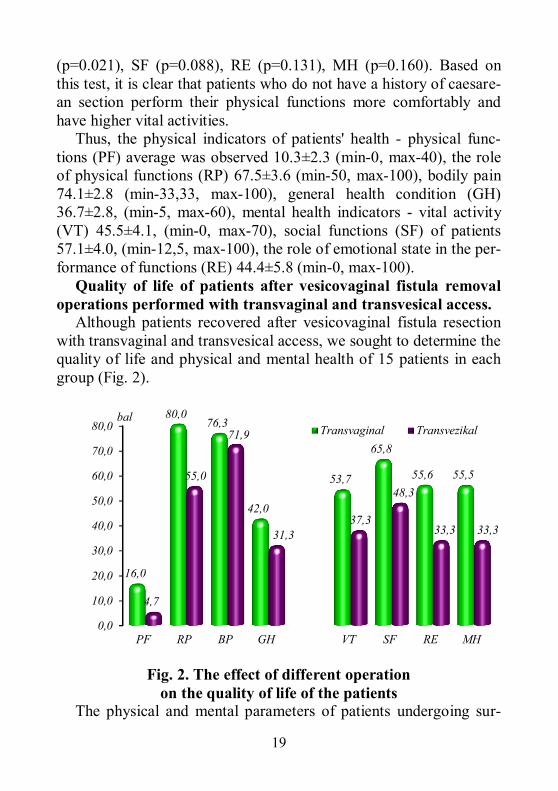
Thus, the physical indicators of patients' health - physical func-tions (PF) average was observed 10.3±2.3 (min-0, max-40), the role of physical functions (RP) 67.5±3.6 (min-50, max-100), bodily pain 74.1±2.8 (min-33,33, max-100), general health condition (GH) 36.7±2.8, (min-5, max-60), mental health indicators - vital activity (VT) 45.5±4.1, (min-0, max-70), social functions (SF) of patients 57.1±4.0, (min-12,5, max-100), the role of emotional state in the per-formance of functions (RE) 44.4±5.8 (min-0, max-100).
Quality of life of patients after vesicovaginal fistula removal operations performed with transvaginal and transvesical access.
Although patients recovered after vesicovaginal fistula resection with transvaginal and transvesical access, we sought to determine the quality of life and physical and mental health of 15 patients in each group (Fig. 2).
Fig. 2. The effect of different operation on the quality of life of the patients
The physical and mental parameters of patients undergoing sur-
0,0
10,0
20,0
30,0
40,0
50,0
60,0
70,0
80,0
PF RP BP GH VT SF RE MH
16,0
80,076,3
42,0
53,7
65,8
55,6 55,5
4,7
55,0
71,9
31,337,3
48,3
33,3 33,3
Transvaginal Transvezikalbal

20
gery with transvesical access RF were 4.7±0.9 (min-0, max-10), p=0.010 and they had difficulty in physical activity compared to the transvaginal group.
Patients were diagnosed with RP 55.0±3,6 (min-50, max-100), p<0.001, BP 71.9±4.7 (min-33.3 max-100), p=0.426, GH 31.3±4.8 (min-5, max-60), p=0.052, VT 37.3±5,6 (min-0, max-55), p=0,042, SF 48.3±4.7 (min-12.5, max-87.5), p=0,024, RE 33.3±8 (min-0, max-66.7), p=0.057, MH 33.3±5.5 (min-0, max-52), p=0.001.
Thus, surgical operations performed according to the Anova test among our patient groups, including transvaginal access from opera-tions we perform with two different access, enabled our patients to return to physical activity more quickly, have less pain in the postop-erative period, and regain their overall health more quickly when looking at transvaginal access, at the same time, from a psychologi-cal point of view, it leads them to acquire their life and social activi-ties, general health faster than other groups, and to be generally men-tally healthy.
Statistics were conducted on the basis of 282 articles on all avail-able literature and found that 39% transvaginal, 36% transabdominal transvesical, 15% laparoscopic, and 3% combined access (transvesi-cal-transvaginal) were performed and it was found that recovery was achieved in 95% of all surgeries and in 63% of those who were con-servatively drained with a long-term catheter11.
In general, we gained recovery by 96.2±2.6% in the first operation in all the VVF removal operations conducted without using tissue loscut and we gained succsess in 3.8±2.6% patients in the second VVF removal operation. If we take it separately, recidive devloped in 8.3±5.6% patients by gaining recovery by 100.0% in the patients performed with transveesical approach but by 91.7±5.6% in the transvaginal group. As vaginal narrowness was observed in the same patients, recovery was gained by 100% by conducting the second VVF removal operation with transvesical approach12.
11Bodner-Adler, B., Hanzal, E., Pablik, E. Management of vesicovaginal fistulas (VVF) in women following benign gynaecologic surgery: Asystematic review and meta-analyşiş // PloS One, 2017. 12 (2), e0171557. 12İmamverdiyev, S.B., Binnətova, E.Y. Sidiklik uşaqlıq yolu fistullarının toxuma
21
3 layer (urinary bladder, paravaginal tissues and uteral tract) in the transvaginal approaches of primary fistula, 3 layer (uteral tract, wall of the urinary bladder and mucous membrane) sutures in transvesical approaches were gradually replaced with smaller tubes after 14-15 days but in the recidive fistula and the patients having reaction to urethral catheter 12 days after epicystostomic tube operation and recovery was provided by 100,0% in 18-20 days.
As ther doctor’s experience increases, the need for transperitoneal fistulaplasty decreases sharply and the prescription for transvesical (54.7%) operation is the high level of fistula, its being closer than 2,0 cm to the urinary tract (a prescription appears for uretherocystoneostomy during fistulaplasty) and vaginal narrowness. In all other cases, the prescriptions for transvaginal (45.3%) fistulaplasty requiring less traumatic and shorter time increases. Fistula must be at least 2,0 cm away from the foramen of urinary tract for being of transvaginal plasty as successful. The location of vesicovaginal fistulas was specified by using endourological equipment in our practice and it was defined that the CT and MRT examinations were not needed in the VVF-in diagnostics and the solution of the problem with transvaginal and transvesical approaches were possible. It was defined that fistulaplastic operation with less invasive approaches has not been needed within the recent 15 years. But it is sometimes possible to have cases on opening of peritoneal cavity for taking enough control while mobilizing fistula tissues and urinary tract during the performance of fistulaplasty. It is an expected process to have peritoneum close to fistula after an gynecological operation.Though the above-said cases make up exception, it is necessary to know the ways of avoiding of such cases.
Thus, as the most beautiful result in the VVF restoration operations is gained in the first operation, we also considered being at least 3 months of the time between the surgical operation conducted in our patients and fistula. We conducted urinary tract stenting or catheterization for preventing of damaging of the urinary loskutu olmadan cərrahi müalicəsi // – Bakı: Urologiya və reproduktiv təbabət jurnalı, – 2018. № 2, – s. 34-37.

22
tracts of the patients prescribed by defining the relations to the ureters, location, number and size of the fistulas in all the patients before the operation. We selected the approach of the fistula removal operation according to the examination and therapic algorithm defined. During the fistula removal operations, we tried to protect the tissues as much as possible and resect the edge of the fistula finely for preventing the vagina narroweness and shortage as well as tissue shortage to happen in future while separating the urinary bladder and vagina. The tissues were put 3 layer (additional end-to-end) sutures in the transvaginal approach – urinary bladder, paravesical tissues and vaginal wall but in the transvesical approach – vaginal wall, muscular and submucosal layer of the urinary bladder and mucous membrane. It was considered not to let the mucous membrane change and cover with muscular layer while putting stitches on the wall of the urinary bladder without using any loscut in the VVF removal operations. While putting stiches on the vagina, “U” shaped stitches and additional end-to-end stitches were put in the regions needed. The sanation of the vagina was conducted with antibioticotherapy and antiseptics by ensuring the adequate functioning of the urinary bladder drainage to provide the recovery of the wound in the primary and infectiousless environment in the post-operational period. It was defined that all of these are the factors that affect the results of the surgical operation and improve the results as well as the recovery is possible without needing any loscut and transperitoneal approach in the fistula operations13.
The reasons for developing of recidive fistulas were also investigated in the scientific investigation. The drainage of urinary bladder turns to be a serious problem in certain cases. Some patients are repeatedly trated for cystitis developing chronic recidive frequently before gynecological operation. Patients always give sharp reaction to keeping of catheter as cicatric tissues develop and the localization of organs change in the small pelvis after the surgical operation made. Though such patients are applied painkilling,
13İmamverdiyev, S.B., Binnətova, E.Y. Sidiklik-uşaqlıq yolu fistulalarının bərpası zamanı transvaginal girişin üstünlükləri // – Bakı: Sağlamlıq, – 2017. № 4, – s. 63-66.

23
spasmolitic and m-cholinolitic medicines 4-5 times a day, it is not possible to create peace in patients. It was defined that one of the reasons of developing of recidive fistulas is the reaction of such patients to urethral catheter. Therefore, it allows us to say that the tolerance test for catheter is one of the measures to be taken for preventing of developing of recidives.
As the practice is formed, fistuloraphy becomes the first choice in most cases by passing thorugh uterus. Despite of that there may always be necessity for using the transvesical, transbdominal and transperitoneal approaches to other approaches. Therefore, a surgeon must be ready for conducting of any form of fistuloplasty operations.
FINDINGS
1. The VVFs mainly appear as a result of total hysterectomy of 21
(39.6±6.7%) uterus together with growths, subtotal hysterectomy of 17 (32.1±6.4%) uterus, 7 (13.2±4.7%) Caesarean operation, 3 (5.7±3.2%) birth and clinical appearance of the disease changes for the location of fistulas. 37.7±6.7% of the patients with subtrigonal fistula do not have natural act of urination and the urine only flows through urinary tract but the urine comes from the uterus in 62.3±6.7% by being natural act of urination [1].
2. It was defined that 79.2±5.6% of the primary fistulas but 93.3±6.4% of the recidive fistulas are met in the women exposed to surgical operation in the regions and the people living in the regions visit the doctor very rarely (75.9±36.6, max-516 months) [11].
3. 73.6±6.1% by cystoscopy for confirming the VVF diagnosis, collusion of two metallic catheters during the vaginal examination (inserted in the urinary bladder through uteral fistula and in the urinary bladder through urethra), clik test 35.8±6.6%, injecting of colored liquid to the urinary tract in some cases 9.4±4.0%, cystography is sufficient in 1.9±1.9% cases and MRT and CT examinations are never needed [12].

24
4. Main reason (3.8±2.6%) of recidives in the VVF removal operations was the drainage of the urinary bladder with catheter after fistulaplasty in the patients having reaction to catheter (activation of chronic cystitis and decreasing of the amount of the urinary bladder) [1, 7].
5. As the doctor’s experience increases, the need for transperitoneal fistulaplasty decreases sharply, prescription for transvesical (54.7%) operation is the high level of fistula, its being closer to the urinary tract than 2,0 cm (prescription is made for ureterocystoneostomy during fistulaplasty) and vaginal narroweness. In all other cases, prescriptions for transvaginal (45.3%) fistulaplasty requiring less traumatic and shorter time increases. The fistula must be at least 2,0 cm away from the foramen of the urinary tracts for being of transvaginal plasty as successful [2, 4, 15].
6. Provision of hermeticity with 3 layer (urinary bladder intransvaginal approaches, paravaginal tissues and uteral tract, uteral tract in transvesical approaches, wall of the urinary bladder and mucous membrane) stiches in the VVF removal operations, the urethral catheter in the primary fistulas for 14-15 days, in the recidive fistulas for 18 days and the gradual replacement of the tubes with smaller tubes in epicystostomic tube placement 12 days after the operation provides recovery in 18-20 days (100,0%) [11].
PRACTICAL RECOMMENDATIONS
1. It is possible to specify the location, size and relation of fistula
with the urinary tracts, calculus in the urinary bladder by conducting of cystoscopic (uretherorenoscopy in case of hydronephrosis in the USE) and vaginal examinations in the diagnostics of these patients and the conformity of the surgical operation with transvaginal or transvesical approach after defining of the diameter of vagina.
2. If the VVF removal operation is conducted for the 1st time, it must be conducted after 2.5 months or more but in those with
25
recidive over 3 months pass from the development of fistula. According to the VVF, the repeated fistulaplasty of the patients exposed to two or more unsuccessful operations, may only be successful when it is conducted by the doctors having a high urogynecological experience.
3. The size of the VVF hole enlarges for 2-3 times after the cicatric tissues are removd and may be closer to the urinary tracts that this case must be considered while defining the approach of an operation. Therefore, it is advised to define the location, size, number, relation of fistula to ureters and decide by thinking the approach of a surgical operation so that they will not lack tissue in the repeatedly conducted operations in recidive cases which may happen and the conduction of transvesical VVF removal will be possible. We did not use any tissue loscut in the patients included in this scientific investigation and no patient had the shortage of tissue. In possible cases, we advise to avoid more invasive approaches.
4. The opportunity for treating of the tissues as sensitive as possible while removing the fistula way irrespective of the surgical approach during the VVF removal operations, preventing of the muscous membrane from turning while using of urinary bladder sutures and bringing closer of the tissues in more favourable way, must be leading one. We may not consider necessary the idea on putting of one of the sutures on the urinary wall and uterus as vertical and the other in the transverse way. Sutures must be put on the urinary wall and vagina in such a way that they will not have gap between the strata. Otherwise, the collection of tissue fluid in the interstratum area will increase the risk for infection and it may have a crucial effect on the result of the operation.
5. It will allow to select the method of draining of urinary bladder during the operation on conducting of tolerancy test on the patients without urethral catheter in their anamneses in the pre-operation period against catheter and may be advised to prevent recidives.

26
LIST OF SCIENTIFIC REFERENCES, PUBLISHED ON THE TOPIC OF THE DISSERTATION:
1. İmamverdiyev, S.B., Binnətova, E.Y. Veziko-vaginal
fistulaların diaqnostika və müalicəsi // – Bakı: Azərbaycan Təbabətinin Müasir Nailiyyətləri, – 2015. № 2, – s. 121-125.
2. Binnətova, E.Y., İmamverdiyev S.B. Yatrogen veziko-vaginal fistulaların transperitoneal girişlə ləğvinə müasir baxışlar // – Bakı: Cərrahiyyə, – 2016. № 1, – s. 62-65.
3. İmamverdiyev, S.B., Binnətova E.Y. Veziko-vaginal fistulaların müalicəsində transvezikal girişin rolu // – Bakı: Cərrahiyyə, – 2016. № 3, – s. 11-15.
4. İmamverdiyev, S.B., Binnətova E.Y. Sidiklik-uşaqlıq yolu fistulalarının bərpası zamanı transvaginal girişin üstünlükləri // – Bakı: Sağlamlıq, – 2017. № 4, – s. 63-67.
5. İmamverdiyev, S.B., Binnətova E.Y. Transvezikal və transvaginal girişlə veziko-vaginal fistula ləğvi əməliyyatlarının nəticələri // – Bakı: Sağlamlıq, – 2017. № 5, – s. 180-187.
6. İmamverdiyev, S.B., Binnətova E.Y. Veziko-vaginal fistula ləğvi əməliyyatlarının nəticələri // – Bakı: Azərbaycan Təbabətinin Müasir Nailiyyətləri, – 2018. № 2, – s. 148-152.
7. Имамвердиев, С.Б., Биннетова, Э.Ю. Преимушество трансвагинального доступа при ликвидации везико-вагинальных фистул // – Астана: Вестник Хирургии Казахстана, – 2017. № 4/53, – s. 38-44.
8. Имамвердиев, С.Б., Биннетова, Э.Ю. Хирургическое лечение безтканеного лоскута везиковагинальных фистул // – Минск: Репродуктивное Здоровье. Восточная Европа, – 2018. № 3, – с. 321-325.
9. İmamverdiyev, S.B., Binnətova, E.Y. Sidiklik uşaqlıq yolu fistullarının toxuma loskutu olmadan cərrahi müalicəsi // – Bakı: Urologiya və reproduktiv təbabət jurnalı, – 2018. № 2, – s. 34-39.
10. Binnətova, E.Y. Yatrogen veziko-vaginal fistulların cərrahi müalicəsinin nəticələri // Əməkdar elm xadimi, professor

27
Abbas Əhməd oğlu Axundbəylinin anadan olmasının 80 illik yubileyinə həsr olunmuş elmi konfransın materialları. – Bakı, – 2018, – s.114-115.
11. Биннетова, Э.Ю. Наш опыт в лечении рецидивных и первичных везико-вагинальных фистул // – Тюмень: Медицинская наука и образование Урала, – 2019. № 4, – с. 83-88.
12. Binnətova, E.Y. Veziko-vaginal fistulların diaqnostikasında sistoskopiya və vaginal müayinələrin rolu // – Bakı: Azərbaycan Tibb Jurnalı, – 2019. № 4, – s. 30-33.
13. Binnetova E.Yu. Vesico-vaginal fistula as a topical problem of modern medicine // Перший крок у науку: матеріали XII студентської конференції, Суми: – 18-19 березня, – 2021. – с. 22.
14. Биннетова Э.Ю. Сравнительная характеристика эффектив-ности хирургических операций у пациентов с везико-вагинальными фистулами // Матеріали ІІІ міжнародної на-уково-практичної конференції теоретичні та практичні ас-пекти розвитку науки та освіти, Львів: – 10-11 квітня, – 2021. – с. 20.
15. Binnetova E.Yu. Comparative characteristics of patients with primary and secondary vesicovaginal fistulas // Збірник тез доповідей науково-практичної конференції з міжнародною участю молодих вчених та студентів «Актуальні питання сучасної медицини і фармації – 2021», Запоріжжя: – 15-16 квітня, – 2021. с. 125-126.
28
LIST OF ABBREVIATIONS AMU – Azerbaijan Medical University BMI – Body Mass Index BP – Bodily pain EU – Excretor urography GH – General health CT – Computer tomography MRT – Magnetic resonance tomography PF – Physical function RE – Role of emotional condition RCH – Republican Clinic Hospital RP – Role of physical functions SF – Social function USE – Ultrasound examination VT – Life activeness VVF – Vesicovaginal fistula

29

30

31
The defense will be held on______ ________ ________ at _______ at the meeting of the Dissertation council ED.2.06 of Supreme Attestation Commission under the President of the Republic of Azerbaijan operating at Azerbaijan Medical University.
Address: AZ 1022, Baku, А.Gasimzade str, 14 (meeting hall).
Dissertation is accessible at the Azerbaijan Medical University Library.
Electronic versions of dissertation and its abstract are available on the official website of the Azerbaijan Medical University.
Abstract was sent to the required addresses on_____ _______ _____

32
Signed for print: 08.05.2021
Paper format: 60 x 84 1/16
Volume: 37991
Number of hard copies: 20