resident’s conference cynthia lan, md june 21, 2005
TRANSCRIPT

Resident’s ConferenceResident’s Conference
Cynthia Lan, MDCynthia Lan, MDJune 21, 2005June 21, 2005

Case presentationCase presentation
CC: “I have a knot under my chin”CC: “I have a knot under my chin”HPI: 29 AAF who c/o “knot” under her chin x 1 week. About 2 weeks HPI: 29 AAF who c/o “knot” under her chin x 1 week. About 2 weeks
ago, she had some upper respiratory symptoms (nasal congestion, ago, she had some upper respiratory symptoms (nasal congestion, rhinorrhea, sore throat). She went to see her doctor and was given rhinorrhea, sore throat). She went to see her doctor and was given amoxicillin. Her respiratory symptoms resolved, but the mass amoxicillin. Her respiratory symptoms resolved, but the mass under her chin remained. The patient does not feel the mass has under her chin remained. The patient does not feel the mass has grown in size, but it has not decreased in size either so she was grown in size, but it has not decreased in size either so she was concerned.concerned.She denies fevers, chills, or weight loss. ROS otherwise negative.She denies fevers, chills, or weight loss. ROS otherwise negative.
PMH: 1) AsthmaPMH: 1) Asthma2) C sxn x 22) C sxn x 23) Tonsillectomy3) TonsillectomyMedications: NoneMedications: NoneAllergies: NoneAllergies: NoneSoc Hx: Married. Has 3 healthy children, ranging from ages 9 to 13. Soc Hx: Married. Has 3 healthy children, ranging from ages 9 to 13.
Works as store manager at Albertson’s. Occasional ETOH use. Works as store manager at Albertson’s. Occasional ETOH use. Quit smoking 5 years ago. Denies IV drug abuse. Quit smoking 5 years ago. Denies IV drug abuse.
FH: Negative for cancerFH: Negative for cancer

• PE: afebrile, BP 107/76, P 90, R 18PE: afebrile, BP 107/76, P 90, R 18
• General: well developed, well nourished African American General: well developed, well nourished African American female in NADfemale in NAD
• HEENT: PERRL, EOMI, OP clearHEENT: PERRL, EOMI, OP clear
• Neck: Right sided submandibular mass, firm, mobile, non Neck: Right sided submandibular mass, firm, mobile, non tender, about 3 cm in diameter. No other adenopathy tender, about 3 cm in diameter. No other adenopathy appreciated.appreciated.
• Lungs: CTABLungs: CTAB
• Breasts: no massesBreasts: no masses
• Abd: +BS, soft, NT, NDAbd: +BS, soft, NT, ND
• Extrem: no edemaExtrem: no edema
• Neuro: CN 2-12 intactNeuro: CN 2-12 intact

Labs:Labs:
• Chem 8 normalChem 8 normal
• CBC: WBC 21,000, hgb 10.9, hct 34.1, plt 613. (diff 83% CBC: WBC 21,000, hgb 10.9, hct 34.1, plt 613. (diff 83% neutrophil, 10% lymph, 4% mono, 1% eos)neutrophil, 10% lymph, 4% mono, 1% eos)
• LFTs normal, alb 3.8LFTs normal, alb 3.8

CXRCXR
• Core biopsy of anterior mediastinal mass: Classical Core biopsy of anterior mediastinal mass: Classical Hodgkin’s lymphoma, nodular sclerosing type. Hodgkin’s lymphoma, nodular sclerosing type. Immunohistochemical studies were positive for CD15 and Immunohistochemical studies were positive for CD15 and CD30, and are negative for CD45 and CD 20.CD30, and are negative for CD45 and CD 20.
• Bone marrow biopsy: negative for Hodgkin’s lymphoma.Bone marrow biopsy: negative for Hodgkin’s lymphoma.


CD30 +

CD15 +

CD20 -

Hodgkin’s LymphomaHodgkin’s Lymphoma
• The incidence of HL is 2.7 per 100,000.The incidence of HL is 2.7 per 100,000.
• Occurs slightly more often in men.Occurs slightly more often in men.
• In North America, there is a higher incidence among those In North America, there is a higher incidence among those of higher socioeconomic status.of higher socioeconomic status.
• Cumulative lifetime risk of developing Hodgkin’s lymphoma Cumulative lifetime risk of developing Hodgkin’s lymphoma in North America is approximately 1 in 250 to 1 in 300.in North America is approximately 1 in 250 to 1 in 300.
• The highest rates of HL are seen in the US, Canada, The highest rates of HL are seen in the US, Canada, Switzerland, and northern Europe.Switzerland, and northern Europe.
• Intermediate rates are seen in southern and eastern EuropeIntermediate rates are seen in southern and eastern Europe
• Low rates are see in Japan, China and other Asian countries.Low rates are see in Japan, China and other Asian countries.

• Unsure why there is a variation in Unsure why there is a variation in
incidence ratesincidence rates
• Postulated reasons include differencesPostulated reasons include differences
in incidence, age of onset, or genotypein incidence, age of onset, or genotype
of Epstein-Barr virus infection; of Epstein-Barr virus infection;
crowding during childhood as a result ofcrowding during childhood as a result of
lower socioeconomic status, or intrinsiclower socioeconomic status, or intrinsic
genetic differences in susceptibility.genetic differences in susceptibility.

• Bimodal age related distribution of incidence of HL, with a Bimodal age related distribution of incidence of HL, with a first peak occurring in the 20s and a second after the age of first peak occurring in the 20s and a second after the age of 55. 55.
• Only 5% of cases occur below the age of 15 and 5% over Only 5% of cases occur below the age of 15 and 5% over the age of 70 years. the age of 70 years.

Etiology and pathogenesisEtiology and pathogenesis• Cause of HL remains unknownCause of HL remains unknown
• Epstein-Barr virus likely plays a role in etiology but mechanism Epstein-Barr virus likely plays a role in etiology but mechanism is not clear.is not clear.
• No clear association with occupational or environmental No clear association with occupational or environmental factors has been found.factors has been found.
• Neoplastic cell is a B-cell that has lost its ability to produce Neoplastic cell is a B-cell that has lost its ability to produce antibody but does not undergo expected cell death due to antibody but does not undergo expected cell death due to defective or blocked apoptosis.defective or blocked apoptosis.
• Genetic factor? Genetic factor? – First degree relatives of people with HL have up to a five-First degree relatives of people with HL have up to a five-
fold increased risk of developing HL. fold increased risk of developing HL. – Monozygotic twins are almost 100-fold more likely to Monozygotic twins are almost 100-fold more likely to
develop HL compared with dizygotic twins of an affected develop HL compared with dizygotic twins of an affected person.person.
– It is speculated that genetically predisposed individuals It is speculated that genetically predisposed individuals could react differently to the virus, increasing their chances could react differently to the virus, increasing their chances that a lymphoid neoplasm be induced.that a lymphoid neoplasm be induced.

• HL has a unique cellular composition, containing a minority HL has a unique cellular composition, containing a minority of neoplastic cells (Reed Sternberg cells) in an of neoplastic cells (Reed Sternberg cells) in an inflammatory background.inflammatory background.
• Currently classified (by the REAL classification) into two Currently classified (by the REAL classification) into two distinct diseases: classical HL and nodular lymphocyte distinct diseases: classical HL and nodular lymphocyte predominance HL.predominance HL.
• Classical HL are further subclassified according to the Classical HL are further subclassified according to the morphology of the Reed-Sternberg cells and the morphology of the Reed-Sternberg cells and the composition of the cellular background: nodular sclerosis, composition of the cellular background: nodular sclerosis, mixed cellularity, lymphocyte-rich, and lymphocyte mixed cellularity, lymphocyte-rich, and lymphocyte depletion. depletion.

History of Hodgkin’s LymphomaHistory of Hodgkin’s Lymphoma
• The first recorded description of Hodgkin’s disease was The first recorded description of Hodgkin’s disease was published in 1666 by Marcello Malpighi, an Italian published in 1666 by Marcello Malpighi, an Italian physiologist. His paper was entitled De viscerum structuru physiologist. His paper was entitled De viscerum structuru excercitatio anatomica.excercitatio anatomica.
• In 1832, Sir Thomas Hodgkin (a British Pathologist) In 1832, Sir Thomas Hodgkin (a British Pathologist) published his paper on lymphatic disease “On Some Morbid published his paper on lymphatic disease “On Some Morbid Appearances of the Absorbant Glands and Spleen.” In this Appearances of the Absorbant Glands and Spleen.” In this paper, he describes a small series of cases of lymph node paper, he describes a small series of cases of lymph node or splenic enlargement. or splenic enlargement.
• 1865 Samuel Wilks (another British Physician) describes the 1865 Samuel Wilks (another British Physician) describes the same disease, independently of Hodgkin and with greater same disease, independently of Hodgkin and with greater precision. As he later became acquainted with Hodgkin’s precision. As he later became acquainted with Hodgkin’s prior work, he named the condition after Hodgkin. prior work, he named the condition after Hodgkin.

Sir Thomas Hodgkin (1789-1866)Sir Thomas Hodgkin (1789-1866)

• 1872 Theodore Langhans (a German pathologist and 1872 Theodore Langhans (a German pathologist and anatomist) publishes the first histopathologic features of anatomist) publishes the first histopathologic features of Hodgkin’s diseaseHodgkin’s disease
• 1878 Greenfield publishes the pathology of lymphomas 1878 Greenfield publishes the pathology of lymphomas with histopathologic features of Hodgkin’s disease.with histopathologic features of Hodgkin’s disease.
• 1894 Sir William Osler’s textbook, The Principles and 1894 Sir William Osler’s textbook, The Principles and Practice of Medicine, was the first publication to mention Practice of Medicine, was the first publication to mention chemotherapy for lymphoma (Fowler’s solution—an arsenic chemotherapy for lymphoma (Fowler’s solution—an arsenic containing medicinal).containing medicinal).
• 1898 Carl von Sternberg (an Austrain pathologist) first 1898 Carl von Sternberg (an Austrain pathologist) first described the giant cells now called Reed-Sternberg cells. described the giant cells now called Reed-Sternberg cells. However he never clearly separated Hodgkin's disease However he never clearly separated Hodgkin's disease from active tuberculosis, since a number of his patients from active tuberculosis, since a number of his patients had both disorders.had both disorders.
• 1902 Dorothy Reed (an American pathologist) 1902 Dorothy Reed (an American pathologist) independently described Reed-Sternberg cells and she first independently described Reed-Sternberg cells and she first clearly separated TB from HD.clearly separated TB from HD.

Dr. Dorothy Reed Mendenhall 1874-1964Dr. Dorothy Reed Mendenhall 1874-1964
• American pathologistAmerican pathologist• Born in Columbus, Ohio, to a wealthy family, Born in Columbus, Ohio, to a wealthy family, • but her father died when she was only but her father died when she was only • 6 years old, so she went into medicine 6 years old, so she went into medicine • as a result of her family’s financial decline.as a result of her family’s financial decline.• She attended John’s Hopkins school of medicineShe attended John’s Hopkins school of medicine• In 1900, she won a prestigious internship with In 1900, she won a prestigious internship with Dr. William Osler, and in 1901 she won a Dr. William Osler, and in 1901 she won a pathology fellowship with Dr. William Welch.pathology fellowship with Dr. William Welch. Working in the Hopkins laboratories, sheWorking in the Hopkins laboratories, she first clearly separated tuberculosis from first clearly separated tuberculosis from Hodgkin's disease, and maintained that the Hodgkin's disease, and maintained that the term Hodgkin disease should be limited to term Hodgkin disease should be limited to histological findings in which "her" histological findings in which "her" giant cells were present. She later wongiant cells were present. She later won international recognition for her work. international recognition for her work.

Reed-Sternberg Cell Reed-Sternberg Cell
• Measure 20 to 60 micrometers in diameter, display a large rim of Measure 20 to 60 micrometers in diameter, display a large rim of cytoplasm, have 2 nuclei with acidophilic nucleoli that covers more cytoplasm, have 2 nuclei with acidophilic nucleoli that covers more than 50% of the nuclear area. than 50% of the nuclear area.
History (cont)History (cont)
• WWII Explosion in Bari, Italy exposes servicemen to toxic WWII Explosion in Bari, Italy exposes servicemen to toxic effects of mustard gases. Follow-up of the exposed men shows effects of mustard gases. Follow-up of the exposed men shows marrow and lymphatic system suppression.marrow and lymphatic system suppression.
• 1943 Nitrogen Mustard (a mustard gas derivative) was 1943 Nitrogen Mustard (a mustard gas derivative) was submitted to Goodman and Gilman at Yale for treatment of HD submitted to Goodman and Gilman at Yale for treatment of HD and lymphosarcoma.and lymphosarcoma.
• In mid 1940s Gilbert and Craft advocate irradiation of nodes In mid 1940s Gilbert and Craft advocate irradiation of nodes and surrounding areas-5 year survival reported to be 25-35%and surrounding areas-5 year survival reported to be 25-35%
• 1963 Development of MOMP – first combination chemotherapy 1963 Development of MOMP – first combination chemotherapy for HD (cyclophosphamide, vincristine, methotrexate, for HD (cyclophosphamide, vincristine, methotrexate, prednisone)prednisone)
• 1964 MOPP combination chemotherapy derived by replacing 1964 MOPP combination chemotherapy derived by replacing methotrexate with procarbazine in MOMP. methotrexate with procarbazine in MOMP.

• 1980s Several studies comparing ABVD (doxorubicin, 1980s Several studies comparing ABVD (doxorubicin, bleomycin, vinblastine, dacarbazine) to MOPP.bleomycin, vinblastine, dacarbazine) to MOPP.
• 2001 WHO Classification for Lymphomas Published—term 2001 WHO Classification for Lymphomas Published—term Hodgkin’s Lymphoma is preferred over Hodgkin’s disease. Hodgkin’s Lymphoma is preferred over Hodgkin’s disease.

Clinical PresentationClinical Presentation• Most patients present with lymphadenopathy, usually in the Most patients present with lymphadenopathy, usually in the
cervical, axillary or mediastinal areas.cervical, axillary or mediastinal areas.
• In only 10% of patients does the nodal disease present initially In only 10% of patients does the nodal disease present initially below the diaphram.below the diaphram.
• Very large mediastinal masses can develop with only modest Very large mediastinal masses can develop with only modest symptoms.symptoms.
• Lymph nodes involved are usually painless, but occasionally a Lymph nodes involved are usually painless, but occasionally a patient will note discomfort in the involved sites right after patient will note discomfort in the involved sites right after drinking alcohol. drinking alcohol.
• The classic B symptoms (weight loss greater than 10% of baseline, The classic B symptoms (weight loss greater than 10% of baseline, night sweats, persistent fevers) only develop in 25% of patients.night sweats, persistent fevers) only develop in 25% of patients.
• Such sx usually indicate widespread or locally extensive disease Such sx usually indicate widespread or locally extensive disease and the need for at least some systemic treatment as part of the and the need for at least some systemic treatment as part of the plan.plan.
• Pruitus can precede the diagnosis of HL by up to several years.Pruitus can precede the diagnosis of HL by up to several years.
• An occasional patient will present with symptomatic anemia or An occasional patient will present with symptomatic anemia or incidentally noticed pancytopenia because HL can involve the incidentally noticed pancytopenia because HL can involve the bone marrow.bone marrow.

Pathology/Biology Pathology/Biology
• Diagnosis of Hodgkin’s lymphoma is based on seeing Reed-Diagnosis of Hodgkin’s lymphoma is based on seeing Reed-Sternberg cells in an appropriate cellular background in Sternberg cells in an appropriate cellular background in tissue from a lymph node or extralymphatic organ such as tissue from a lymph node or extralymphatic organ such as the bone marrow, lung or bone.the bone marrow, lung or bone.
• Open biopsy is required for diagnosis, to determine the Open biopsy is required for diagnosis, to determine the histologic subtype. (FNA can be suggestive but is not histologic subtype. (FNA can be suggestive but is not adequate for diagnosis of HL.) adequate for diagnosis of HL.)
• Immunohistochemical studiesImmunohistochemical studies– Classical HL is positive for CD30 and CD15, negative for Classical HL is positive for CD30 and CD15, negative for
CD45 and CD79aCD45 and CD79a– Nodular lymphocyte predominant HL is negative for Nodular lymphocyte predominant HL is negative for
CD30 and CD15, positive for CD45 and CD79a and CD20CD30 and CD15, positive for CD45 and CD79a and CD20
EvaluationEvaluation
• History: Ask for B symptoms (fever, weight loss, night History: Ask for B symptoms (fever, weight loss, night sweats)sweats)
• PE: LAD, organomegalyPE: LAD, organomegaly
• Labs: CBC, ESR, liver function, renal function, hepatitis B, Labs: CBC, ESR, liver function, renal function, hepatitis B, HIV (if risk factors are present), and albumin.HIV (if risk factors are present), and albumin.
• Bone marrow biopsy for patients with B symptoms or WBC Bone marrow biopsy for patients with B symptoms or WBC <4,000 or advanced disease.<4,000 or advanced disease.
• CT scan of chest/abd/pelvisCT scan of chest/abd/pelvis
• PET can be useful to asses residual masses during or after PET can be useful to asses residual masses during or after planned treatment to identify the minority who should planned treatment to identify the minority who should receive altered or additional therapy. receive altered or additional therapy.
• ?Role of staging laparotomy—in the past, certain stage I-II ?Role of staging laparotomy—in the past, certain stage I-II patients without B symptoms and nodular sclerosis patients without B symptoms and nodular sclerosis histology may undergo staging laparotomy (a laparotomy histology may undergo staging laparotomy (a laparotomy with splenectomy and liver biopsy) because if negative, with splenectomy and liver biopsy) because if negative, patients can be treated with mantle field radiation alone.patients can be treated with mantle field radiation alone.
• However, it is rarely done these days because of the However, it is rarely done these days because of the associated morbidity and lack of survival advantage in associated morbidity and lack of survival advantage in patients with favorable prognosis disease. Also, most pts patients with favorable prognosis disease. Also, most pts with stage I-II disease now receive chemo in addition to with stage I-II disease now receive chemo in addition to radiation anyway.radiation anyway.
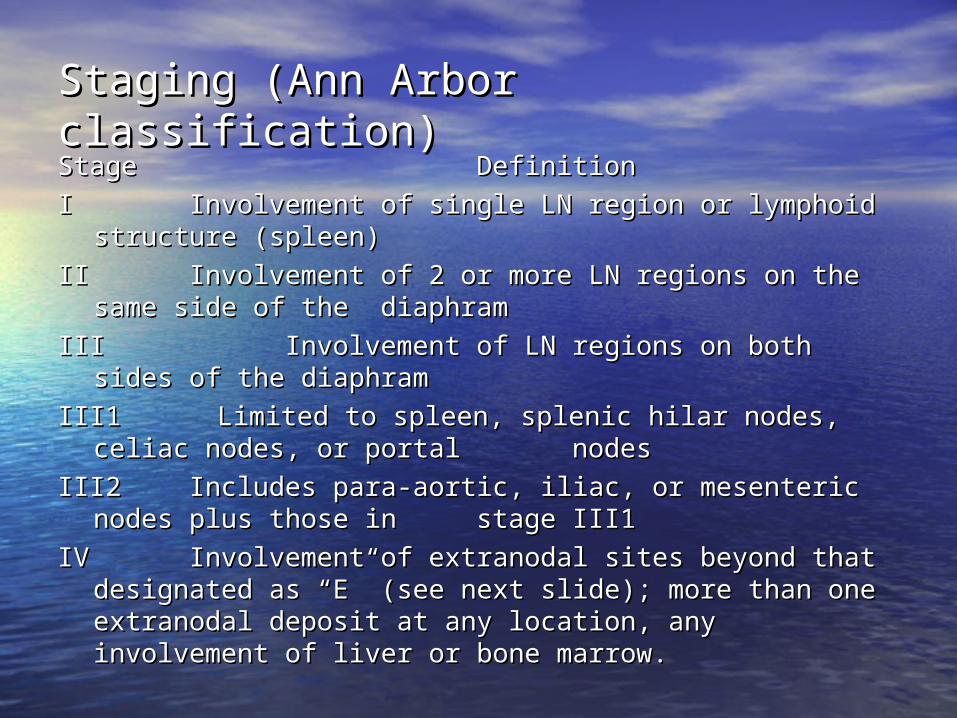
Staging (Ann Arbor classification)Staging (Ann Arbor classification)StageStage DefinitionDefinition
II Involvement of single LN region or lymphoid Involvement of single LN region or lymphoid structure (spleen)structure (spleen)
IIII Involvement of 2 or more LN regions on the same Involvement of 2 or more LN regions on the same side of the side of the diaphramdiaphram
IIIIII Involvement of LN regions on both sides of the Involvement of LN regions on both sides of the diaphramdiaphram
III1 Limited to spleen, splenic hilar nodes, celiac nodes, or III1 Limited to spleen, splenic hilar nodes, celiac nodes, or portal portal nodesnodes
III2III2 Includes para-aortic, iliac, or mesenteric nodes plus Includes para-aortic, iliac, or mesenteric nodes plus those in those in stage III1stage III1
IVIV Involvement of extranodal sites beyond that Involvement of extranodal sites beyond that designated as “E” (see next slide); more than one designated as “E” (see next slide); more than one extranodal deposit at any location, any involvement of liver extranodal deposit at any location, any involvement of liver or bone marrow.or bone marrow.

Staging (cont)Staging (cont)
AA No B symtomsNo B symtoms
BB Unexplained weight loss greater than 10% in the last Unexplained weight loss greater than 10% in the last 6 6 months, unexplained fever >100.4 F in the past months, unexplained fever >100.4 F in the past month, month, recurrent drenching night sweats in the past recurrent drenching night sweats in the past monthmonth
X X Bulky disease, mass greater than 10 cm, mediastinal Bulky disease, mass greater than 10 cm, mediastinal mass mass greater than 1/3 the chest diameter at T5-6greater than 1/3 the chest diameter at T5-6
EE Localized solitary involvement of extralymphatic Localized solitary involvement of extralymphatic tissue, except tissue, except liver and bone marrowliver and bone marrow

PrognosisPrognosis
• Prognosis of patients with HL has improved over the past 50 Prognosis of patients with HL has improved over the past 50 years. years.
• Two factors dominate the prognosis: Age and stage.Two factors dominate the prognosis: Age and stage.
• Elderly patients (those older than 65) make up only 5% of all Elderly patients (those older than 65) make up only 5% of all pts with HL, but their likelihood of being cured is only ½ that of pts with HL, but their likelihood of being cured is only ½ that of younger pts (comorbid conditions, loss of organ reserve with younger pts (comorbid conditions, loss of organ reserve with aging, and intrinsic resistance of the disease in older pts).aging, and intrinsic resistance of the disease in older pts).
• Pts with limited-stage disease have at least a 90 to 95% Pts with limited-stage disease have at least a 90 to 95% likelihood of cure.likelihood of cure.
• Pts with advanced disease have 65% chance of cure with Pts with advanced disease have 65% chance of cure with primary treatment.primary treatment.
• Relapsed disease: cure in more than 40 to 50% with high dose Relapsed disease: cure in more than 40 to 50% with high dose chemotherapy.chemotherapy.
Primary TreatmentPrimary Treatment
• Currently, most pts with Hodgkin’s disease are cured so Currently, most pts with Hodgkin’s disease are cured so minimizing long-term consequences of treatment is minimizing long-term consequences of treatment is important.important.
• Although the chances of being cured of HL is high, overall Although the chances of being cured of HL is high, overall expectation of survival is not normal. expectation of survival is not normal.
• Challenge in treating pts with HL is not only to cure the Challenge in treating pts with HL is not only to cure the disease but to do so while holding the potential for long disease but to do so while holding the potential for long term toxicity to a minimum.term toxicity to a minimum.
• This usually means choosing an initial approach to cure the This usually means choosing an initial approach to cure the majority of pts and using secondary treatment for the majority of pts and using secondary treatment for the minority who relapse. minority who relapse.

Favorable and unfavorable prognosis stage Favorable and unfavorable prognosis stage I-II Hodgkin’s disease I-II Hodgkin’s disease
• Among stage I-II pts, retrospective studies have identified a Among stage I-II pts, retrospective studies have identified a number of adverse prognostic criteria: large mediastinal number of adverse prognostic criteria: large mediastinal adenopathy, age >50, and B symtoms. adenopathy, age >50, and B symtoms.
• Large mediastinal adenopathy predicts an increased risk of Large mediastinal adenopathy predicts an increased risk of relapse, but date is conflicting on whether these findings relapse, but date is conflicting on whether these findings cause a lower rate of survival. cause a lower rate of survival.
• Older age: have a lower survival rate than younger Older age: have a lower survival rate than younger patients, probably due to less successful treatment at patients, probably due to less successful treatment at relapse and a greater mortality risk from other causes (i.e. relapse and a greater mortality risk from other causes (i.e. second tumors and cardiac disease)second tumors and cardiac disease)
• Pts with B symptoms have higher relapse rate.Pts with B symptoms have higher relapse rate.

Treatment of favorable Stage I-II HL Treatment of favorable Stage I-II HL
• Favorable prognostic indicators (as defined by the Favorable prognostic indicators (as defined by the European Organization for the Research and Treatment of European Organization for the Research and Treatment of Cancer H7 and H8 trials) : age 50 or under, no large Cancer H7 and H8 trials) : age 50 or under, no large mediastinal adenopathy, ESR < 50/h and no B symptoms or mediastinal adenopathy, ESR < 50/h and no B symptoms or ESR < 30/h with B symptoms, disease limited to one to ESR < 30/h with B symptoms, disease limited to one to three regions of involvement.three regions of involvement.
• Currently there are several treatment options, and Currently there are several treatment options, and although there are differences in relapse rates, there is no although there are differences in relapse rates, there is no difference in overall survival.difference in overall survival.– ABVD for 3-6 cycles, followed by involved field ABVD for 3-6 cycles, followed by involved field
irradiation with 30 Gy with an optional boost of 6 Gy to irradiation with 30 Gy with an optional boost of 6 Gy to individual nodes of concern.individual nodes of concern.
– Mantle field irradiation (neck, chest, axillary LN) to 30 Mantle field irradiation (neck, chest, axillary LN) to 30 Gy with a total dose of 36 to 40 Gy to regions of initial Gy with a total dose of 36 to 40 Gy to regions of initial involvement followed by paraaortic and splenic involvement followed by paraaortic and splenic irradiation to 30 Gy. (Risk of second malignancies is irradiation to 30 Gy. (Risk of second malignancies is increased with these larger radiation fields.) increased with these larger radiation fields.)
– Full dose chemotherapy alone is under investigation in Full dose chemotherapy alone is under investigation in clinical trials.clinical trials.
(ABVD = doxorubicin, bleomycin, vinblastine, dacarbazine)(ABVD = doxorubicin, bleomycin, vinblastine, dacarbazine)

Randomized Comparison of ABVD Chemotherapy With a Randomized Comparison of ABVD Chemotherapy With a Strategy that includes radiation therapy in patients with Strategy that includes radiation therapy in patients with limited-stage Hodgkin’s lymphoma: National Cancer Institute limited-stage Hodgkin’s lymphoma: National Cancer Institute of Canada Clinical Trials Group and the Eastern Cooperative of Canada Clinical Trials Group and the Eastern Cooperative Oncology Group (Meyer, et al. J of Clinical Oncology, vol 23, no Oncology Group (Meyer, et al. J of Clinical Oncology, vol 23, no 21) Published ahead of print on April 18, 2005 (Original date 21) Published ahead of print on April 18, 2005 (Original date July 20, 2005)July 20, 2005)• Randomized trial comparing ABVD alone to ABVD + radiation in Randomized trial comparing ABVD alone to ABVD + radiation in
399 pts.399 pts.
• Pts with nonbulky stage I to IIA Hodgkin’s lymphoma were Pts with nonbulky stage I to IIA Hodgkin’s lymphoma were stratified into favorable and unfavorable cohorts. (Unfavorable stratified into favorable and unfavorable cohorts. (Unfavorable cohort: age >40 yr, ESR>50, mixed cellularity or lymphocyte cohort: age >40 yr, ESR>50, mixed cellularity or lymphocyte deplete histology, >4 sites of disease)deplete histology, >4 sites of disease)
• Randomized to ABVD alone or treatment that includes radiation Randomized to ABVD alone or treatment that includes radiation therapy. In the ABVD group, both cohorts (favorable and therapy. In the ABVD group, both cohorts (favorable and unfavorable) received ABVD as a single modality x 4-6 cycles. In unfavorable) received ABVD as a single modality x 4-6 cycles. In the treatment with radiotherapy group, the favorable cohort the treatment with radiotherapy group, the favorable cohort received sub total nodal radiation therapy only, while the received sub total nodal radiation therapy only, while the unfavorable cohort received combined modality therapy with unfavorable cohort received combined modality therapy with ABVD x 2 cycles plus sub total nodal irradiation therapy.ABVD x 2 cycles plus sub total nodal irradiation therapy.
• Median follow up is 4.2 years.Median follow up is 4.2 years.

• Results: Compared to ABVD alone, 5 yr freedom from Results: Compared to ABVD alone, 5 yr freedom from disease progression is superior in pts allocated to radiation disease progression is superior in pts allocated to radiation therapy (93% v 87%, P=0.006), but no differences in event therapy (93% v 87%, P=0.006), but no differences in event free survival (88% v 86%, P=0.06) or overall survival (94% free survival (88% v 86%, P=0.06) or overall survival (94% v 96%, p = 0.4) were detected. In subset analysis v 96%, p = 0.4) were detected. In subset analysis comparing pts stratified into the unfavorable cohort, FFD comparing pts stratified into the unfavorable cohort, FFD progression was superior in pts assigned to progression was superior in pts assigned to ABVD+radiation group compared to ABVD alone (95% v ABVD+radiation group compared to ABVD alone (95% v 88%, p = 0.004), but no difference in overall survival was 88%, p = 0.004), but no difference in overall survival was detected (92% v 95%, p = 0.3)detected (92% v 95%, p = 0.3)
• Conclusion: In pts with limited stage HL, no difference in Conclusion: In pts with limited stage HL, no difference in overall survival was detected between pts randomly overall survival was detected between pts randomly assigned to receive treatment that includes radiation assigned to receive treatment that includes radiation therapy vs ABVD alone. Although 5-year FFD progression therapy vs ABVD alone. Although 5-year FFD progression was superior in pts receiving radiation therapy, this was superior in pts receiving radiation therapy, this advantage is offset by deaths due to causes other than advantage is offset by deaths due to causes other than progressive HL or acute treatment related toxicity. progressive HL or acute treatment related toxicity.

Treatment of unfavorable Stage I-II disease Treatment of unfavorable Stage I-II disease
• Combined modality therapy (chemo + radiation)Combined modality therapy (chemo + radiation)• Chemotherapy (ABVD or MOPP/ABVD) is given to maximal Chemotherapy (ABVD or MOPP/ABVD) is given to maximal
tumor response (usually 4 to 6 monthly cycles), as judged by CT tumor response (usually 4 to 6 monthly cycles), as judged by CT scan and PET, after which 2 additional cycles of consolidation scan and PET, after which 2 additional cycles of consolidation chemotherapy are given followed by limited radiation therapy. chemotherapy are given followed by limited radiation therapy.
• Radiation fields can be limited to involved regions (shown on CT Radiation fields can be limited to involved regions (shown on CT or PET). Restricting fields reduces the risk of pulmonary or PET). Restricting fields reduces the risk of pulmonary complications related to the radiation. Also, in young women, complications related to the radiation. Also, in young women, the elimination of axillary irradiation reduces the risk of the elimination of axillary irradiation reduces the risk of subsequent breast cancer. subsequent breast cancer.
MOPP = (nitrogen mustard/mechlorethamine, vincristine, MOPP = (nitrogen mustard/mechlorethamine, vincristine, procarbazine, prednisone)procarbazine, prednisone)

Treatment of advanced (stage III-IV) Hodgkin’s Treatment of advanced (stage III-IV) Hodgkin’s diseasedisease
• The prognosis of stage III varies with the absence (A) or The prognosis of stage III varies with the absence (A) or presence (B) of B symptoms. Stage IIIA actually is a presence (B) of B symptoms. Stage IIIA actually is a category of intermediate malignancy. category of intermediate malignancy.
• Chemotherapy has become curative for many patients with Chemotherapy has become curative for many patients with advanced stages of HD. advanced stages of HD.
• Since the 1960s, MOPP has been the main effective chemo Since the 1960s, MOPP has been the main effective chemo for advanced stage HD, but toxicity has been an important for advanced stage HD, but toxicity has been an important limitation. (Late complications include sterility and limitation. (Late complications include sterility and increased risk of acute nonlymphocytic leukemia.)increased risk of acute nonlymphocytic leukemia.)
• ABVD is more effective and less toxic, and is currently the ABVD is more effective and less toxic, and is currently the standard for advanced HD. standard for advanced HD.

• With ABVD, 60 to 70% of pts will be alive and free of With ABVD, 60 to 70% of pts will be alive and free of disease at 5 years. disease at 5 years.
• Recommendation: pts be monitored for response during Recommendation: pts be monitored for response during treatment (6 cycles minimum) and receive 2 courses of treatment (6 cycles minimum) and receive 2 courses of chemo beyond best response.chemo beyond best response.
• The addition of radiotherapy improves freedom from The addition of radiotherapy improves freedom from progression, but not survival.progression, but not survival.
• Randomized trials have not been done, but combined Randomized trials have not been done, but combined modality treatment is currently favored for pts with massive modality treatment is currently favored for pts with massive mediastinal disease. mediastinal disease.
Other chemotherapy used for advanced stage Other chemotherapy used for advanced stage Hodgkin’s lymphomaHodgkin’s lymphoma
• BEACOPP (Bleomycin, etoposide, doxorubicin, BEACOPP (Bleomycin, etoposide, doxorubicin, cyclophosphamide, vincristine, procarbazine, and prednisone) cyclophosphamide, vincristine, procarbazine, and prednisone) was developed by the German Hodgkin’s Lymphoma Study was developed by the German Hodgkin’s Lymphoma Study Group.Group.– May be particularly useful in pts with highest risk diseaseMay be particularly useful in pts with highest risk disease– Higher rates of toxicity, including infertility and a higher risk of Higher rates of toxicity, including infertility and a higher risk of
MDS/AML when compared to ABVD.MDS/AML when compared to ABVD.
• Stanford V (doxorubicin, vinblastine, mechlorethamine, Stanford V (doxorubicin, vinblastine, mechlorethamine, vincristine, bleomycin, etoposide, prednisone), a combined vincristine, bleomycin, etoposide, prednisone), a combined modality treatment with the great majority of pts receiving modality treatment with the great majority of pts receiving radiation.radiation.– Best results are in pts with less than 3 adverse risk factorsBest results are in pts with less than 3 adverse risk factors– Ongoing trials comparing Stanford V with ABVD.Ongoing trials comparing Stanford V with ABVD.

Patients who relapsePatients who relapse
• 20 to 40% of pts with advanced HD who enter complete 20 to 40% of pts with advanced HD who enter complete remission with initial chemo will relapse.remission with initial chemo will relapse.
• Poor prognostic factors for response to first line chemo Poor prognostic factors for response to first line chemo include B symptoms, age >45, bulky mediastinal disease, include B symptoms, age >45, bulky mediastinal disease, extranodal involvement, low hct, high ESR and high levels extranodal involvement, low hct, high ESR and high levels of CD 30.of CD 30.
• Pts with resistant disease (those who do not have CR after Pts with resistant disease (those who do not have CR after initial treatment with ABVD) should be offered high dose initial treatment with ABVD) should be offered high dose chemo, with or without radiotherapy followed by bone chemo, with or without radiotherapy followed by bone marrow transplant. marrow transplant.

Second malignancies after treatment of Hodgkin’s Second malignancies after treatment of Hodgkin’s diseasedisease• Increasing success in the treatment of Hodgkin’s disease Increasing success in the treatment of Hodgkin’s disease
has been associated with second malignancies. has been associated with second malignancies. • There is an increased risk of leukemia (10-80 fold), Non-There is an increased risk of leukemia (10-80 fold), Non-
Hodgkin’s lymphoma (3 to 35 fold), and solid tumors (lung, Hodgkin’s lymphoma (3 to 35 fold), and solid tumors (lung, breast, bone, stomach, colon, thyroid, melanoma, over 2 breast, bone, stomach, colon, thyroid, melanoma, over 2 fold) fold)
• Acute Leukemia--Highest risks and greatest number of Acute Leukemia--Highest risks and greatest number of cases occur between 5 and 10 years after the initiation of cases occur between 5 and 10 years after the initiation of treatment, usually with alkylating agents. treatment, usually with alkylating agents.
• Non-Hodgkin’s Lymphoma—incidence ranged from 0.9% Non-Hodgkin’s Lymphoma—incidence ranged from 0.9% at 6.7 years followup to 1.6 % at 15 years.at 6.7 years followup to 1.6 % at 15 years.
• One-half to two-thirds of second malignancies are solid One-half to two-thirds of second malignancies are solid tumors after 15 or more years of follow-up.tumors after 15 or more years of follow-up.
• The risk is inversely related to age at initial treatment. The risk is inversely related to age at initial treatment. • Lung and breast cancer are the two most common second Lung and breast cancer are the two most common second
malignancies.malignancies.• Other malignancies include bone and soft tissue cancer, Other malignancies include bone and soft tissue cancer,
thyroid cancer, melanoma, and GI cancers.thyroid cancer, melanoma, and GI cancers.

• NEJM 1996 Breast Cancer and other second neoplasms after NEJM 1996 Breast Cancer and other second neoplasms after childhood Hodgkin’s Disease (Bhatia, et al.)childhood Hodgkin’s Disease (Bhatia, et al.)– Cohort of 1380 children with Hodgkin’s disease (age at dx = 1-Cohort of 1380 children with Hodgkin’s disease (age at dx = 1-
16 yr)16 yr)– Estimated incidence of any second neoplasm 15 years after the Estimated incidence of any second neoplasm 15 years after the
diagnosis of HD was 7.0%diagnosis of HD was 7.0%– The incidence of solid tumors was 3.9%The incidence of solid tumors was 3.9%– Breast cancer was the most common solid tumor with an Breast cancer was the most common solid tumor with an
incidence that approached 35% by 40 years of age. incidence that approached 35% by 40 years of age. – The estimated incidence of leukemia was 2.8% at 14 years after The estimated incidence of leukemia was 2.8% at 14 years after
diagnosis.diagnosis.– Treatment with alkylating agents, recurrence of HD, and late Treatment with alkylating agents, recurrence of HD, and late
stage of disease at diagnosis were risk factors for leukemia. stage of disease at diagnosis were risk factors for leukemia.

Issues for the futureIssues for the future• In the past, Hodgkin’s disease was largely incurable, but at In the past, Hodgkin’s disease was largely incurable, but at
present it is often curable.present it is often curable.• With 15% of pts still dying of lymphoma, there are new With 15% of pts still dying of lymphoma, there are new
treatments on the horizontreatments on the horizon• Currently under investigation for treatment of HL is Currently under investigation for treatment of HL is
gemcitabine (a pyrimidine antimetabolite that inhibits DNA gemcitabine (a pyrimidine antimetabolite that inhibits DNA synthesis). synthesis). – Small Phase II study done in Italy and Germany (Santoro, et al. Small Phase II study done in Italy and Germany (Santoro, et al.
Journal of Clinical Oncology, Vol 18, No 13, 2000)Journal of Clinical Oncology, Vol 18, No 13, 2000)– 23 pts with refractory or relapsed HD, who had more than one 23 pts with refractory or relapsed HD, who had more than one
previous chemotherapy regimenprevious chemotherapy regimen– Overall response rate of 39% with gemcitabine therapyOverall response rate of 39% with gemcitabine therapy
• Targeted immunotherapy is a new treatment being Targeted immunotherapy is a new treatment being researched. Rituximab (anti CD20 monoclonal antibody) researched. Rituximab (anti CD20 monoclonal antibody) has proven useful for several different types of B-cell has proven useful for several different types of B-cell lymphomas, and the nearly universal expression of CD20 on lymphomas, and the nearly universal expression of CD20 on the neoplastic cells of lymphocyte predominant HL suggests the neoplastic cells of lymphocyte predominant HL suggests that this lymphoma might be treated successfully with that this lymphoma might be treated successfully with rituximab. rituximab.

Follow up on our patientFollow up on our patient
• Hodgkin’s lymphoma, nodular sclerosing type.Hodgkin’s lymphoma, nodular sclerosing type.
• Stage IIIAX (PET CT showed mediastinal, right supraclavicular, Stage IIIAX (PET CT showed mediastinal, right supraclavicular, infraclavicular and pancreatic hypermetabolic localization infraclavicular and pancreatic hypermetabolic localization consistent with Hodgkin’s lymphoma, with the largest lesion consistent with Hodgkin’s lymphoma, with the largest lesion in the mediastinum measuring 13 cm).in the mediastinum measuring 13 cm).
• She has completed 6 cycles of chemotherapy with ABVD.She has completed 6 cycles of chemotherapy with ABVD.
• Her mediastinal mass has decreased in size to 7.85 x 6.4 cm.Her mediastinal mass has decreased in size to 7.85 x 6.4 cm.
• Her most recent PET scan after 6 cycles shows decreased Her most recent PET scan after 6 cycles shows decreased metabolic activity in thoracic mass, implying fair response to metabolic activity in thoracic mass, implying fair response to therapy. The other areas of abnormal intensities have therapy. The other areas of abnormal intensities have resolved and no new abnormalities are noted.resolved and no new abnormalities are noted.
• She is scheduled to undergo 2 more cycles of ABVD.She is scheduled to undergo 2 more cycles of ABVD.

ReferencesReferences• Abeloff: Clinical Oncology, 3Abeloff: Clinical Oncology, 3rdrd ed., 2004. pp 2985–3011. ed., 2004. pp 2985–3011.
• Bhatia, et al. Breast cancer and other second neoplasms after Bhatia, et al. Breast cancer and other second neoplasms after childhood Hodgkin’s disease. NEJM 1996;334:745-51.childhood Hodgkin’s disease. NEJM 1996;334:745-51.
• Hasenclever D, Diehl, V, A prognostic score for Advanced Hodgin’s Hasenclever D, Diehl, V, A prognostic score for Advanced Hodgin’s disease. NEJM 1998;339:1506-1514disease. NEJM 1998;339:1506-1514
• Meyer, et al. J of Clin Oncol vol 23, no 21. Randomized Comparison of Meyer, et al. J of Clin Oncol vol 23, no 21. Randomized Comparison of ABVD Chemotherapy with a strategy that includes radiation therapy in ABVD Chemotherapy with a strategy that includes radiation therapy in patients with limited stage Hodgkin’s lymphoma: National Cancer patients with limited stage Hodgkin’s lymphoma: National Cancer Institute of Canada Clinical Trials group and the Eastern Cooperative Institute of Canada Clinical Trials group and the Eastern Cooperative Oncology Group. Pp1-9.Oncology Group. Pp1-9.
• Santoro, et al. J of Clin Oncol vol 18, no 13. Gemcitabine in the Santoro, et al. J of Clin Oncol vol 18, no 13. Gemcitabine in the treatment of Refractory Hodgkin’s disease: results of a multicenter treatment of Refractory Hodgkin’s disease: results of a multicenter phase II study. Pp 2615-2619.phase II study. Pp 2615-2619.
• Tierney, Jr. et al. 2002 Current Medical Diagnosis and Treatment. 549. Tierney, Jr. et al. 2002 Current Medical Diagnosis and Treatment. 549.
• www.lymphomainfo.netwww.lymphomainfo.net
• www.Uptodate.comwww.Uptodate.com
• www.whonamedit.comwww.whonamedit.com