respiratory emergencies provena regional ems. what we know air is good air is good pink is good pink...
TRANSCRIPT

Respiratory Respiratory EmergenciesEmergencies
Provena Regional EMSProvena Regional EMS

What we knowWhat we know
Air is goodAir is good Pink is goodPink is good Blue is badBlue is bad Air goes in Air goes in Air goes outAir goes out

Ventilation isVentilation is
Movement of air in and outMovement of air in and out

Upper AirwayUpper Airway
In through noseIn through nose• WarmsWarms• HumidifiesHumidifies• FiltersFilters
Past epiglottisPast epiglottis
Into tracheaInto trachea• Anterior to esophagusAnterior to esophagus

Sellick’s ManeuverSellick’s Maneuver
Pressure on cartilagePressure on cartilage• Pushes trachea more posterior for visualization of vocal Pushes trachea more posterior for visualization of vocal
cords in intubationcords in intubation• Compresses esophagus to inhibit vomitingCompresses esophagus to inhibit vomiting

BronchiBronchi• Branch off tracheaBranch off trachea
BronchiolesBronchioles• 33 divisions to alveoli33 divisions to alveoli• No air exchange until No air exchange until
alveolialveoli• Dead air spaceDead air space• Must ventilate with 500 cc Must ventilate with 500 cc
of inspired air to of inspired air to
get to alveoliget to alveoli

AlveoliAlveoli Elastic muscles around bronchioles can cause spasm Elastic muscles around bronchioles can cause spasm Network of capillaries around alveoli for gas exchangeNetwork of capillaries around alveoli for gas exchange
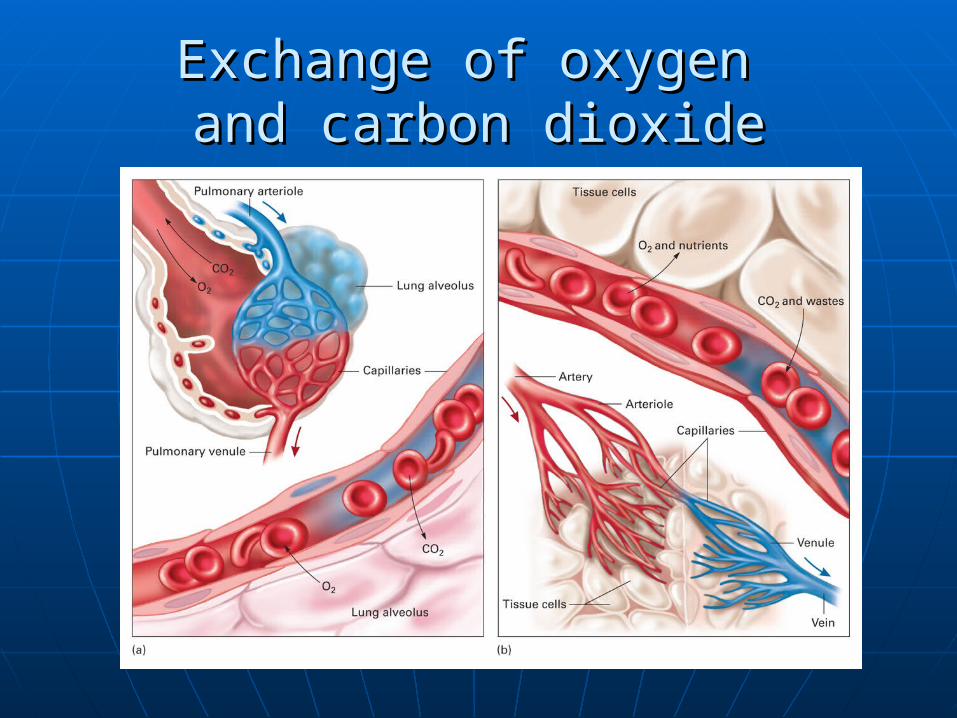
Exchange of oxygen Exchange of oxygen and carbon dioxideand carbon dioxide

VentilationVentilation

Mechanics of BreathingMechanics of Breathing Inspiration chest expands – creates vacuum – air rushes inInspiration chest expands – creates vacuum – air rushes in Expiration chest contracts – creates pressure – air rushes outExpiration chest contracts – creates pressure – air rushes out

DiffusionDiffusion– process of moving oxygen into – process of moving oxygen into blood and carbon dioxide outblood and carbon dioxide out
Diffusion is movement of particles (gas) Diffusion is movement of particles (gas) from an area of high concentration to an from an area of high concentration to an area of low concentrationarea of low concentration

HemoglobinHemoglobin 98% of inspired oxygen attached to the protein, 98% of inspired oxygen attached to the protein,
hemoglobin in RBChemoglobin in RBC
alveolialveoli cellscells

Hypoxia – low oxygen to cellsHypoxia – low oxygen to cells
Causes of hypoxiaCauses of hypoxia Hypoxic hypoxia – not enough oxygenHypoxic hypoxia – not enough oxygen Anemic hypoxia– not enough hemoglobinAnemic hypoxia– not enough hemoglobin Stagnant hypoxia – not enough perfusionStagnant hypoxia – not enough perfusion
• shockshock Histotoxic hypoxia – unable to downloadHistotoxic hypoxia – unable to download
• Cyanide poisoningCyanide poisoning

Causes of Causes of Respiratory EmergenciesRespiratory Emergencies
Failure of:Failure of:• Ventilation: air in/ air outVentilation: air in/ air out• Diffusion: movement of gasesDiffusion: movement of gases• Perfusion: movement of bloodPerfusion: movement of blood
Relieved by: epinephrine based Relieved by: epinephrine based medications medications
(such as Beta 2 agonist– albuterol, terbutaline)(such as Beta 2 agonist– albuterol, terbutaline)
Compounded by:Compounded by: Inflammation/mucus productionInflammation/mucus production

AssessmentAssessment
Scene size upScene size up• Scene safetyScene safety• EnvironmentEnvironment
What in and around the patient suggests What in and around the patient suggests that this is a respiratory emergency?that this is a respiratory emergency?

General Impression of PatientGeneral Impression of Patient
PositionPosition ColorColor Mental StatusMental Status Ability to SpeakAbility to Speak Respiratory EffortRespiratory Effort

Is this patient in distress?Is this patient in distress?

Look for pursed lip breathing or prolonged Look for pursed lip breathing or prolonged expirationexpiration

Tripod position suggests distress, resting weight on Tripod position suggests distress, resting weight on knees helps with chest expansionknees helps with chest expansion

Slow labored breathing is a sign of Slow labored breathing is a sign of respiratory failurerespiratory failure

Cyanosis – blue discoloration Cyanosis – blue discoloration suggests hypoxiasuggests hypoxia

Initial AssessmentInitial Assessment
Airway – open,no noisesAirway – open,no noises Breathing – 12-20 times per minuteBreathing – 12-20 times per minute Circulation – warm, pink, dry, strong Circulation – warm, pink, dry, strong
pulsespulses Disability – mental status clearDisability – mental status clear Vital SignsVital Signs

Focused HistoryFocused History
SAMPLESAMPLE OPQRSTOPQRST
• How long has this been going on?How long has this been going on?• Start gradual or abruptStart gradual or abrupt• Better or worse with positionBetter or worse with position• CoughCough
Productive of sputumProductive of sputum Color of sputum– white? Yellow? Red? Color of sputum– white? Yellow? Red?
green? brown? green? brown?

Additional SymptomsAdditional Symptoms
Chest painChest pain Fever/chillsFever/chills WheezingWheezing Smoking historySmoking history TraumaTrauma

Medications Currently TakingMedications Currently Taking
AntibioticsAntibiotics OxygenOxygen SteroidsSteroids
• EmphysemaEmphysema• AsthmaAsthma
Inhalers/nebulizersInhalers/nebulizers• EmphysemaEmphysema• AsthmaAsthma
Cardiac drugsCardiac drugs

Respiratory EmergenciesRespiratory Emergencies
For each, considerFor each, consider• Cause/PathologyCause/Pathology• Signs and symptomsSigns and symptoms• ManagementManagement

Upper Airway ObstructionUpper Airway Obstruction Due to Due to
• Foreign bodies – food, toysForeign bodies – food, toys• TongueTongue• SwellingSwelling
Underlying Problem – VENTILATIONUnderlying Problem – VENTILATION Assessment/Associated SymptomsAssessment/Associated Symptoms
• Airway movementAirway movement• Ability to speakAbility to speak• DyspneaDyspnea• HypoxiaHypoxia• Sounds – snoring, stridorSounds – snoring, stridor• Oxygen saturation will be low Oxygen saturation will be low

Upper Airway ObstructionUpper Airway Obstruction
ManagementManagement• BLS– Heimlich maneuverBLS– Heimlich maneuver• ALS Foreign Body – Magill ForcepsALS Foreign Body – Magill Forceps• Allergic Reaction – epi-pen and ALS Allergic Reaction – epi-pen and ALS
protocolprotocol• Epiglottitis – rapid transportEpiglottitis – rapid transport• Croup– humidified oxygenCroup– humidified oxygen• Sleep apnea– Prescribed CPAPSleep apnea– Prescribed CPAP

EmphysemaEmphysema
Destruction of alveolar wallsDestruction of alveolar walls Underlying Problem: DiffusionUnderlying Problem: Diffusion Assessment/Associated SymptomsAssessment/Associated Symptoms
• Dyspnea with exertionDyspnea with exertion• History of exposureHistory of exposure• Barrel chestBarrel chest• Prolonged expiratory phaseProlonged expiratory phase
Pursed lip breathingPursed lip breathing
• Thin and emaciatedThin and emaciated• Pink puffer Pink puffer (extra hemoglobin to make up for poor oxygen (extra hemoglobin to make up for poor oxygen
pick up)pick up)

ManagementManagement
Won’t call till there is a problemWon’t call till there is a problem Secure airwaySecure airway Correct hypoxia Correct hypoxia
• Respiratory drive from low oxygen not high Respiratory drive from low oxygen not high CO2CO2
IV access (dehydration)IV access (dehydration) Albuterol for Bronchodilation if Albuterol for Bronchodilation if
wheezingwheezing

Chronic BronchitisChronic Bronchitis
Increased mucus productionIncreased mucus production Decreased alveolar ventilation Decreased alveolar ventilation Underlying Problem: VENTILATION Underlying Problem: VENTILATION
AND INFLAMMATIONAND INFLAMMATION Assessment/Associated SymptomsAssessment/Associated Symptoms
• History of long term exposure to toxinsHistory of long term exposure to toxins• Frequent respiratory infectionsFrequent respiratory infections• Heavy sputum productionHeavy sputum production• Obese and cyanotic (blue bloater)Obese and cyanotic (blue bloater)

ManagementManagement
Secure airwaySecure airway Correct hypoxiaCorrect hypoxia IV access (dehydration)IV access (dehydration) Albuterol Bronchodilation if wheezingAlbuterol Bronchodilation if wheezing

AsthmaAsthma
Lower airway obstructionLower airway obstruction• BronchospasmBronchospasm• EdemaEdema• MucusMucus
Caused byCaused by• IrritantsIrritants• Respiratory infectionRespiratory infection• Emotional distressEmotional distress

AsthmaAsthma
Underlying Problem: VENTILATION Underlying Problem: VENTILATION AND INFLAMMATIONAND INFLAMMATION
Assessment/Associated SymptomsAssessment/Associated Symptoms• Non productive coughNon productive cough• WheezingWheezing• Speech dyspnea – one word sentencesSpeech dyspnea – one word sentences• Use of accessory musclesUse of accessory muscles• Status Asthmaticus– Status Asthmaticus– not responding to not responding to
treatmenttreatment

Breath sounds?Breath sounds? IF BRONCHOLES TOTALLY OCCLUDED IF BRONCHOLES TOTALLY OCCLUDED
NO BREATH SOUNDS AT ALL ---NO BREATH SOUNDS AT ALL ---SILENCE IS BAD, BAD, BADSILENCE IS BAD, BAD, BAD

ManagementManagement
Secure airwaySecure airway Correct hypoxiaCorrect hypoxia IV access (dehydration)IV access (dehydration) Bronchodilation Beta 2 agonist Bronchodilation Beta 2 agonist
• Inhaled, nebulized and/or subcutaneousInhaled, nebulized and/or subcutaneous• Albuterol, terbutalineAlbuterol, terbutaline

PneumoniaPneumonia
Infection of the lungsInfection of the lungs Alveoli and interstitial spaces fill with Alveoli and interstitial spaces fill with
fluidfluid Includes Severe Acute Respiratory Includes Severe Acute Respiratory
Syndrome (SARS) and tuberculosisSyndrome (SARS) and tuberculosis
Underlying Problem: DIFFUSIONUnderlying Problem: DIFFUSION

Assessment/Associated SymptomsAssessment/Associated Symptoms• Looks illLooks ill• Fever and chillsFever and chills• Productive coughProductive cough• Chest pain with respirationChest pain with respiration

ManagementManagement
BSI – wear a maskBSI – wear a mask Secure airwaySecure airway Correct hypoxiaCorrect hypoxia IV access (dehydration)IV access (dehydration) If wheezing -- Bronchodilation Beta 2 If wheezing -- Bronchodilation Beta 2
Agonist -- albuterolAgonist -- albuterol

CostochondritisCostochondritis
Viral chest wall painViral chest wall pain Inflammation of muscle walls and Inflammation of muscle walls and
cartilage of chestcartilage of chest
Underlying problem: VENTILATION Underlying problem: VENTILATION AND INFLAMMATIONAND INFLAMMATION

Assessment/Associated SymptomsAssessment/Associated Symptoms• Sudden onsetSudden onset• No traumaNo trauma• Pain on deep inhalation Pain on deep inhalation • Pain on palpationPain on palpation• May have fever or history of coldMay have fever or history of cold

ManagementManagement
Correct hypoxiaCorrect hypoxia Symptom reliefSymptom relief Anti-inflammatory medicationsAnti-inflammatory medications
• IbuprofenIbuprofen

Toxic InhalationToxic Inhalation
Inhalation ofInhalation of• Super heated airSuper heated air• ChemicalsChemicals• Combustion productsCombustion products• SteamSteam
Lower airway edemaLower airway edema BronchospasmBronchospasm Underlying Problem: VENTILATION, Underlying Problem: VENTILATION,
INFLAMMATION, DIFFUSIONINFLAMMATION, DIFFUSION

Assessment/Associated SymptomsAssessment/Associated Symptoms• Nature of inhalantNature of inhalant• Burns to face, nose, mouthBurns to face, nose, mouth• StriderStrider

ManagementManagement
Rescuer safetyRescuer safety Remove from further exposureRemove from further exposure Secure airway – may need intubationSecure airway – may need intubation Correct hypoxiaCorrect hypoxia IV accessIV access Rapid transportRapid transport Correct wheezing with beta 2 Correct wheezing with beta 2
agonist-- albuterolagonist-- albuterol

Carbon Monoxide PoisoningCarbon Monoxide Poisoning Inhalation of gas that binds with Inhalation of gas that binds with
hemoglobin hemoglobin Underlying Problem: CELLULAR HYPOXIAUnderlying Problem: CELLULAR HYPOXIA Assessment/Associated SymptomsAssessment/Associated Symptoms
• HeadacheHeadache• IrritabilityIrritability• Errors in judgmentErrors in judgment• ConfusionConfusion• VomitingVomiting• Flu symptomsFlu symptoms• Pink colorPink color

ManagementManagement
Rescuer safetyRescuer safety Remove from sourceRemove from source Secure airwaySecure airway High flow oxygenHigh flow oxygen Hyperbaric chamberHyperbaric chamber

Pulmonary EmboliPulmonary Emboli
Blood clot (or other emboli) in Blood clot (or other emboli) in pulmonary circulation blocking blood pulmonary circulation blocking blood flowflow
Ventilation perfusion mis-matchVentilation perfusion mis-match Underlying problem: PERFUSION, Underlying problem: PERFUSION,
DIFFUSIONDIFFUSION

Assessment/Associated Symptoms:Assessment/Associated Symptoms:• Sudden onset acute chest painSudden onset acute chest pain• Sudden onset acute dyspneaSudden onset acute dyspnea• Tachypnea – fast breathingTachypnea – fast breathing• Tachycardia – fast heart rateTachycardia – fast heart rate• Recent history of being inactiveRecent history of being inactive
ManagementManagement
Secure AirwaySecure Airway Correct hypoxiaCorrect hypoxia IV AccessIV Access

Spontaneous PneumothoraxSpontaneous Pneumothorax
Sudden loss of pleural sealSudden loss of pleural seal Underlying Problem: DIFFUSION, Underlying Problem: DIFFUSION,

Assessment/Associated SymptomsAssessment/Associated Symptoms• Non traumatic Non traumatic • Sudden onset dyspneaSudden onset dyspnea• No pain on palpationNo pain on palpation• May develop tension and JVDMay develop tension and JVD
Breath sounds absent on 1 sideBreath sounds absent on 1 side

ManagementManagement
Secure airwaySecure airway Correct hypoxiaCorrect hypoxia Watch for tension pneumothoraxWatch for tension pneumothorax IV access IV access

HyperventilationHyperventilation
Increased minute volumeIncreased minute volume Underlying problem: too much oxygen and not Underlying problem: too much oxygen and not
enough carbon dioxide (ACID/BASE DISRUPTION)enough carbon dioxide (ACID/BASE DISRUPTION) Assessment/Associated SymptomsAssessment/Associated Symptoms
• TachypneaTachypnea• Numbness and tingling of fingers, toes, mouthNumbness and tingling of fingers, toes, mouth
(Carpopedal spasms)(Carpopedal spasms)

Breath sounds are present on both Breath sounds are present on both sidessides
Oxygen Saturation is greater than Oxygen Saturation is greater than 94% on room air94% on room air

ManagementManagement
Secure airwaySecure airway Correct respiratory rate – slow downCorrect respiratory rate – slow down Oxygen by mask as 6 litersOxygen by mask as 6 liters IV access IV access

Central Nervous System Central Nervous System Dysfunction -- BrainDysfunction -- Brain
Head trauma, stroke, brain tumor, insulin Head trauma, stroke, brain tumor, insulin shock, drug toxicityshock, drug toxicity
Underlying Problem: VENTILATIONUnderlying Problem: VENTILATION
Assessment/Associated SymptomsAssessment/Associated Symptomsslow shallow breathingslow shallow breathing
decreased tidal volume and minute decreased tidal volume and minute volumevolume
cyanosiscyanosis

ManagementManagement
Secure airwaySecure airway Correct hypoxiaCorrect hypoxia May need to assist ventilationsMay need to assist ventilations IV accessIV access Treat underlying cause if ableTreat underlying cause if able

Central Nervous System Central Nervous System Dysfunction– Spinal CordDysfunction– Spinal Cord
Trauma, polio, multiple sclerosis, Trauma, polio, multiple sclerosis, myasthenia gravis, ALSmyasthenia gravis, ALS
Underlying problem: VentilationUnderlying problem: Ventilation
Assessment/Associated Symptoms:Assessment/Associated Symptoms:• Slow shallow respirationsSlow shallow respirations• Poor use of chest musclesPoor use of chest muscles• Decreased tidal volume and minute Decreased tidal volume and minute
volumevolume

ManagementManagement
Secure airwaySecure airway Correct hypoxiaCorrect hypoxia May need to assist ventilationsMay need to assist ventilations IV accessIV access

Respiratory FailureRespiratory Failure
Inability of the to meet the basic Inability of the to meet the basic demands for tissue oxygenationdemands for tissue oxygenation
Underlying Problem: VENTILATION, Underlying Problem: VENTILATION, PERFUSION, DIFFUSIONPERFUSION, DIFFUSION

Assessment/Associated Symptoms:Assessment/Associated Symptoms:• Gradual onset ofGradual onset of
Inadequate oxygen productionInadequate oxygen productionInadequate CO2 removalInadequate CO2 removalTachycardia and Tachypnea Tachycardia and Tachypnea
• Followed in end stages byFollowed in end stages byBrady cardia and BradypneaBrady cardia and BradypneaCyanosisCyanosisPoor chest wall movementPoor chest wall movementProfound acidosisProfound acidosis

ManagementManagement
Open airway and mechanically Open airway and mechanically ventilateventilate
IV access and correct hypovolemiaIV access and correct hypovolemia Work to correct underlying problemWork to correct underlying problem


ReviewReview
Answer the following questions as a group.Answer the following questions as a group. If doing this CE individually, please e-mail If doing this CE individually, please e-mail
your answers to:your answers to: [email protected]@provena.org
Use “Nov 2008 CE” in subject box.Use “Nov 2008 CE” in subject box. You will receive an e-mail confirmation. You will receive an e-mail confirmation.
Print this confirmation for your records, Print this confirmation for your records, and document the CE in your PREMSS CE and document the CE in your PREMSS CE record book.record book.

What do you know? Question 1What do you know? Question 1 You are in a restaurant when a middle-aged man at the You are in a restaurant when a middle-aged man at the
next table begins to act strangely while eating steak. He next table begins to act strangely while eating steak. He appears to be in acute distress but is completely silent. His appears to be in acute distress but is completely silent. His eyes are open wide and he is staggering about. As you eyes are open wide and he is staggering about. As you approach him, he slumps into your arms unconscious. approach him, he slumps into your arms unconscious. What has possibly happened to this man?What has possibly happened to this man?• A. Acute asthma attackA. Acute asthma attack• B. EmphysemaB. Emphysema• C. Foreign body airway obstructionC. Foreign body airway obstruction• D. HyperventilationD. Hyperventilation

Question 1 part BQuestion 1 part B
How do you want to manage the patient in How do you want to manage the patient in question 1?question 1?• A. call 911 and apply oxygenA. call 911 and apply oxygen• B. call 911 and attempt BLS maneuvers to B. call 911 and attempt BLS maneuvers to
remove a Foreign Bodyremove a Foreign Body• C. call 911 and administer an epi-penC. call 911 and administer an epi-pen• D. Begin CPRD. Begin CPR

Question 2Question 2 You are called to attend a 56-year old man whose chief You are called to attend a 56-year old man whose chief
complaint is dyspnea. He states that he has a chronic complaint is dyspnea. He states that he has a chronic cough that has gotten worse over the last few days. The cough that has gotten worse over the last few days. The sputum he is coughing up has changed in color from white sputum he is coughing up has changed in color from white to yellow/green. The man is heavy set and has a cyanotic to yellow/green. The man is heavy set and has a cyanotic color. He has loud wheezes and gurgling in his chest. His color. He has loud wheezes and gurgling in his chest. His vitals are BP 150/90, Pulse 110 and respirations 28. vitals are BP 150/90, Pulse 110 and respirations 28. Oxygen saturation on room air is 88%. What is wrong with Oxygen saturation on room air is 88%. What is wrong with this man?this man?• A. Acute foreign body airway obstructionA. Acute foreign body airway obstruction• B. Allergic reaction to the environmentB. Allergic reaction to the environment• C. AsthmaC. Asthma• D. Chronic bronchitis with an acute infectionD. Chronic bronchitis with an acute infection

Question 2 part BQuestion 2 part B
How do you want to manage the patient in How do you want to manage the patient in question 2?question 2?• A. apply oxygenA. apply oxygen• B. attempt BLS maneuvers to remove a B. attempt BLS maneuvers to remove a
Foreign Body Foreign Body• C. administer an epi-penC. administer an epi-pen• D. begin CPRD. begin CPR

Question 3Question 3 You are called to help a 24 year old woman with difficulty You are called to help a 24 year old woman with difficulty
breathing. She is sitting up when you find her, bending breathing. She is sitting up when you find her, bending forward and fighting to breathe. Her chest is not moving forward and fighting to breathe. Her chest is not moving much and only faint wheezing can be heard when you listen much and only faint wheezing can be heard when you listen to her chest. She is so short of breath that she cannot talk. to her chest. She is so short of breath that she cannot talk. She takes inhalers daily. What is wrong with this patient?She takes inhalers daily. What is wrong with this patient?• A. Acute asthma attackA. Acute asthma attack• B. Airway obstruction from a Foreign bodyB. Airway obstruction from a Foreign body• C. Hyperventilation syndromeC. Hyperventilation syndrome• D. PneumoniaD. Pneumonia

Question 3 part BQuestion 3 part B
How do you want to manage the patient in How do you want to manage the patient in question 3?question 3?• A. apply oxygenA. apply oxygen• B. attempt BLS maneuvers to remove aB. attempt BLS maneuvers to remove a
Foreign BodyForeign Body• C. administer an epi-penC. administer an epi-pen• D. apply oxygen and assist the patient with D. apply oxygen and assist the patient with
taking her inhaler or (advanced providers) taking her inhaler or (advanced providers) administer albuteroladminister albuterol

Question 4Question 4 You are called to a restaurant to attend a patient in You are called to a restaurant to attend a patient in
respiratory distress. Speaking hoarsely, he tells you that he respiratory distress. Speaking hoarsely, he tells you that he was eating shrimp cocktail and that his throat feels swollen. was eating shrimp cocktail and that his throat feels swollen. He tells you that he has been allergic to lobster in the past. He tells you that he has been allergic to lobster in the past. You notice that he has swelling of his lips and hives on his You notice that he has swelling of his lips and hives on his face. His respiratory distress is increasing and his face. His respiratory distress is increasing and his respirations are wheezing and shallow. What is wrong with respirations are wheezing and shallow. What is wrong with this patient?this patient?• A. Acute asthma attackA. Acute asthma attack• B. Acute allergic reactionB. Acute allergic reaction• C. Acute foreign body airway obstructionC. Acute foreign body airway obstruction• D. Chronic bronchitisD. Chronic bronchitis

Question 4 part BQuestion 4 part B
How do you want to manage the patient in How do you want to manage the patient in question 4?question 4?• A. apply oxygenA. apply oxygen• B. attempt BLS maneuvers to remove a Foreign B. attempt BLS maneuvers to remove a Foreign
BodyBody• C. apply oxygen and administer an epi-penC. apply oxygen and administer an epi-pen• D. begin CPRD. begin CPR

Question 5Question 5 A 60 year old woman has been unable to walk since A 60 year old woman has been unable to walk since
surgery. She has been either in bed or in a chair for several surgery. She has been either in bed or in a chair for several weeks. She only walks to the bathroom and back. weeks. She only walks to the bathroom and back. Suddenly she feels extremely short of breath and has Suddenly she feels extremely short of breath and has developed sharp chest pain . You find her anxious with developed sharp chest pain . You find her anxious with labored respirations. Her vitals are BP 100/60, pulse 120, labored respirations. Her vitals are BP 100/60, pulse 120, respirations 28, oxygen saturation 90% on room air. What respirations 28, oxygen saturation 90% on room air. What is most likely wrong with this woman?is most likely wrong with this woman?• A. Acute asthma attackA. Acute asthma attack• B. Pulmonary emboliB. Pulmonary emboli• C. Acute myocardial infarctionC. Acute myocardial infarction• D. Acute allergic reactionD. Acute allergic reaction

Question 5 part BQuestion 5 part B
How do you want to manage the patient in How do you want to manage the patient in question 5?question 5?• A. apply oxygen and transport immediatelyA. apply oxygen and transport immediately• B. apply oxygen and administer albuterol by B. apply oxygen and administer albuterol by
nebulizernebulizer• C. apply oxygen and administer an epi-penC. apply oxygen and administer an epi-pen• D. begin CPR and prepare to defibrillateD. begin CPR and prepare to defibrillate

Question 6Question 6 You are called to a large party for a man who is short of You are called to a large party for a man who is short of
breath. You find a thin 19 year old man who is breathing 40 breath. You find a thin 19 year old man who is breathing 40 times a minute. His respirations are not wheezing and his times a minute. His respirations are not wheezing and his skin is pink, warm and dry. He is very anxious and skin is pink, warm and dry. He is very anxious and complaining of tightness in his chest. His fingers are complaining of tightness in his chest. His fingers are painful and cramped. What is wrong with this patient?painful and cramped. What is wrong with this patient?
• A. Acute asthma attackA. Acute asthma attack• B. Acute myocardial infarctionB. Acute myocardial infarction• C. Hyperventilation syndromeC. Hyperventilation syndrome• D. Foreign body airway obstruction D. Foreign body airway obstruction

Question 6 part BQuestion 6 part B
How do you want to manage the patient in How do you want to manage the patient in question 6?question 6?• A. apply oxygen by mask at 6 liters and A. apply oxygen by mask at 6 liters and
attempt to slow breathingattempt to slow breathing• B. attempt BLS maneuvers to remove a Foreign B. attempt BLS maneuvers to remove a Foreign
BodyBody• C. apply oxygen and administer an epi-penC. apply oxygen and administer an epi-pen• D. begin CPR and prepare to defibrillateD. begin CPR and prepare to defibrillate

Question 7Question 7 You respond to a house fire to assist a 30 year old woman. You respond to a house fire to assist a 30 year old woman.
She has facial burns with singed eyebrows and nasal hairs. She has facial burns with singed eyebrows and nasal hairs. Her voice is very hoarse and she has soot in her sputum. Her voice is very hoarse and she has soot in her sputum. What two airway emergencies are going on with this lady?What two airway emergencies are going on with this lady?
• A. Toxic inhalation and chronic bronchitisA. Toxic inhalation and chronic bronchitis• B. Acute asthma attack and airway burnsB. Acute asthma attack and airway burns• C. Foreign body obstruction and chronic bronchitisC. Foreign body obstruction and chronic bronchitis• D. Toxic inhalation and airway burnsD. Toxic inhalation and airway burns

Question 7 part BQuestion 7 part B
How do you want to manage the patient in How do you want to manage the patient in question 7?question 7?• A. apply oxygen, if Advanced provider prepare A. apply oxygen, if Advanced provider prepare
to intubateto intubate• B. attempt BLS maneuvers to remove a Foreign B. attempt BLS maneuvers to remove a Foreign
BodyBody• C. apply oxygen and administer an epi-penC. apply oxygen and administer an epi-pen• D. begin CPR and prepare to defibrillateD. begin CPR and prepare to defibrillate

Question 8Question 8
Most respiratory emergencies are due to a failure Most respiratory emergencies are due to a failure of:of:• A. PerfusionA. Perfusion• B. VentilationB. Ventilation• C. Diffusion of gasesC. Diffusion of gases• D. All of the aboveD. All of the above

Question 9Question 9
Respiratory emergencies are frequently Respiratory emergencies are frequently complicated by:complicated by:• A. InflammationA. Inflammation• B. Mucus productionB. Mucus production• C. History of toxic exposure such as cigarette smokeC. History of toxic exposure such as cigarette smoke• D. All of the aboveD. All of the above

Question 10Question 10 Hypoxia, low oxygen delivery to the cells can be Hypoxia, low oxygen delivery to the cells can be
caused by:caused by:
• A. Hypoxic hypoxia – insufficient oxygenA. Hypoxic hypoxia – insufficient oxygen• B. Anemic hypoxia – insufficient red blood B. Anemic hypoxia – insufficient red blood
cellscells• C. Stagnant hypoxia – shockC. Stagnant hypoxia – shock• D. Histotoxic hypoxia – oxygen unable to D. Histotoxic hypoxia – oxygen unable to download at the celldownload at the cell• E. All of the aboveE. All of the above

Happy Thanksgiving, and thanks to Happy Thanksgiving, and thanks to you all for all your hard work.you all for all your hard work.
Provena Regional EMS StaffProvena Regional EMS Staff

AnswersAnswers 1.1. CC Part B.Part B. BB 2.2. DD Part B.Part B. AA 3.3. AA Part B.Part B. DD 4.4. BB Part B.Part B. CC 5.5. BB Part B.Part B. AA 6.6. CC Part B.Part B. AA 7.7. DD Part B.Part B. AA 8.8. DD 9.9. DD 10.10. EE