respirology and the 2008 lmcc examinations 2008 april 1 guidelines to help keep you on course peter...
TRANSCRIPT
Arterial Blood gas interpretation
pH PaCO2 PO2 on FIO2 =….
pH then PCO2 for acid-base balance – for an acute change in PCO2 of 10, the pH
goes 0.08 units in the other direction.
PCO2 and PO2 and FIO2 for gas exchange

Bicarbonate is never measured, it is calculated from the Henderson-Hesselbach equation using measured pH and paCO2
Examples of Acid-Base Imbalance:

Describe the Acid-Base Imbalance (1):
pH=7.42, PCO2=48
PaCO2 is slightly high pH is on the alkaline side of normal This is most probably a
compensated metabolic alkalosis

Describe the Acid-Base Imbalance (2):
pH=7.36, PCO2=52
PaCO2 is high
pH is normal, but on the acid side of 7.40
This is most probably a compensated
respiratory acidosis

Describe the Acid-Base Imbalance (3):
pH=7.20, PCO2=52
pH is quite acid PaCO2 is less high than you expect
for a pure respiratory acidosis, (PCO2 up by 12, pH should go down by ~ .10 units)
this is a mixed acidosis

Assessment of Gas Exchange:
Question: While breathing room air, a comatose hyperpneic youth arrives in the ER. He is pink. An ABG shows:– pH=7.15; PCO2=20, PO2=95
Acid-base status? Acute Metabolic Acidosis
Are his lungs normal? NO as A-a DO2 is

The Flow-Volume loop
A. Normal
– Identify
» 1 Peak flow rate
» 2 RV
» 3 TLC
What is B?
1
23

The Flow-Volume loop
A. Normal
B. Restrictive
C. Large airway fixed
obstruction
D. Small airways
variable obstruction
E. Extra-thoracic
variable obstruction

Exercise Testing: Stage I Screening
Quantitate exercise capacity c.f. predicted
Assess oxygen saturation on exertion Factors limiting Exercise
– Pulmonary Mechanics– Pulmonary Vascular– Cardiac or peripheral (including unfitness)– Anxiety

Inhaler Devices:
Dry powder inhalers (DPI) - (Diskus or Turbuhaler or Handihaler)
Pressurized Metered Dose Inhalers- (Freon-free) (HFA MDIs) eg Advair 250, Qvar,Salbutamol, Mometasone– pulmonary deposition may be improved– side-effects decreased
Patients still need careful instruction in the use of any inhaler device

Inhaled Steroids: (IS)
Fluticasone (Flovent) , Budisonide (Pulmicort), Ciclesonide (Alvesco)
all have similar local side effects - sore throat, thrush, dysphonia ( try a spacer and do a swish, gargle and spit) (Ciclesonide may be exception)
Enough absorption to cause bruising

Inhaled Steroids (IS): Potential side-effects if long-term, high dose therapy:
Cataracts, Osteoporosis
– osteoporosis prevention may be important with children on high dose IS, but not adults.
– Inactivity due to uncontrolled asthma promotes osteoporosis also
Delayed growth Adrenal insufficiency

Long-lasting B2 Agonists (LABAs):
Examples:– Salmeterol (Serevent) 25 ug p ii bid – Formoterol (Oxeze) 12 ug p i bid
Second-line drug for ongoing acute bronchospasm despite optimal inhaled steroids
Decreases nocturnal exacerbations Does not eliminate the need for short-acting
B2-agonists Not a rescue medication

Combination IS/LABA: Examples:
– Advair discus(fluticasone + salmeterol– Symbicort turbuhaler (budisonide +
formoterol Indication in Asthma:
– When IS in doses of 500-1000 ug/day are insufficient to eliminate frequent rescue with SABAs
Indication in COPD: – May increase interval between AECB .

Leukotriene Antagonists
Montelukast (Singulair) 10 mgm qhs Block leukotriene-derived mediators
(SRS-ALTC4 and LTD4, but not prostaglandins
Montelukast is accepted for children down to age 6 years (5 mgm strength)
It is helpful in a minority of asthmatics

Leukotriene Antagonists Role:
– a second line drug– If inhaled steroids are insufficient to control
symptoms or are contra-indicated – May help:
» ASA-sensitive individuals» restore sense of smell (Systemic distribution)» may be useful to prevent progressive asthma
Side effects - None

IgE Antagonists: Omalizumab (Xolair)
Monoclonal antibodies block action of IgE on mast cell
Effective if IgE levels are only slightly elevated (500-1200)
Monthly injection Extremely expensive ?$45,000/year Use if frequent need for oral steroids
despite optimum conventional Rx and patient has drug plan or $$$

Acute asthma, ER management
Mild: B2 agonist; start IS Moderate: add O2, oral steroids Severe: add continuous B2 aersols,
Ipatropium, 100% O2 Near death: add intubation, ventilation,
kitchen sink (Theophylline, MgSO4, Halogenated anesthetic) Discharge criteria: track record,
response to B2 agonists, prior steroids, compliance

Chronic asthma management
Minimal: B2 agonist prn. Mild: add inhaled steroids Moderate :
– Leucotriene antagonist– long lasting B2 agonist– Short course oral prednisone
Severe:– add oral steroids dose large enough, duration long
enough to return patient to “personal best”– “Bronchial barbecue”- bronchial thermoplasty
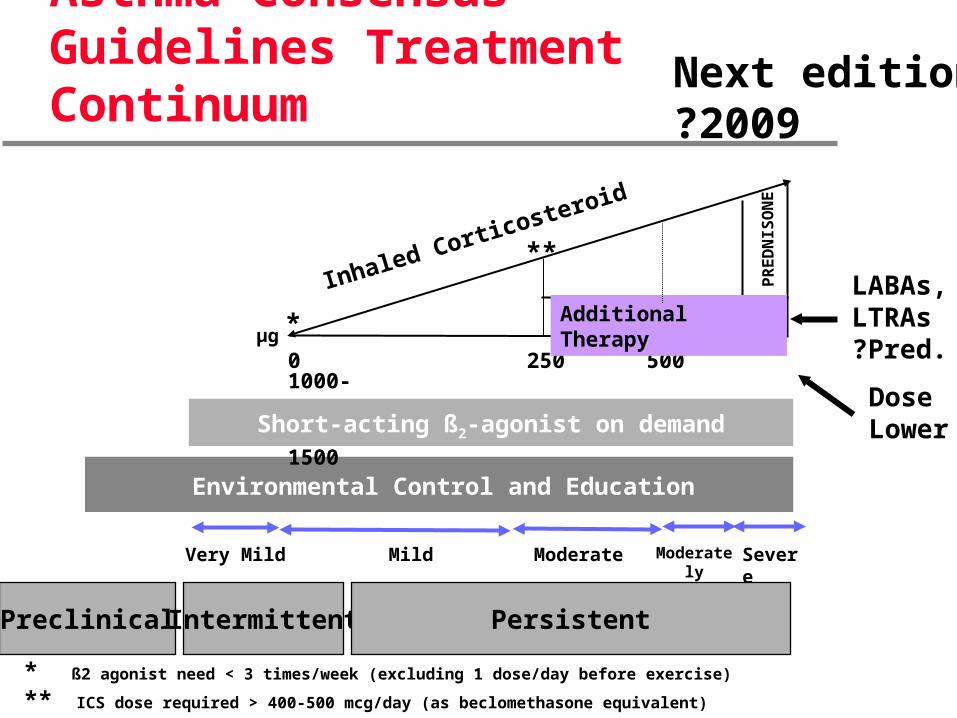
Environmental Control and Education
Short-acting ß2-agonist on demand
0 250 500 1000- 1500
µg *
**
* ß2 agonist need < 3 times/week (excluding 1 dose/day before exercise)
** ICS dose required > 400-500 mcg/day (as beclomethasone equivalent)
PR
ED
NIS
ON
E
Inhaled Corticosteroid
Asthma Consensus Guidelines Treatment Continuum
Additional Therapy
SevereModerately Severe
ModerateMildVery Mild
Next edition?2009
LABAs,LTRAs?Pred.
Dose Lower
Preclinical Intermittent Persistent

COPD
4% of Canadians 4th leading cause of death Over 40 years of age Mortality rate rising, especially for females Occasionally occupation causes COPD

COPD Guidelines
Do not screen asymptomatic smokers Assess with spirometry if symptomatic
– Cough – SOBOE– wheeze – persisting colds
FEV1/ FVC< .7
Do ABG if FEV1 <40% predicted

COPD-Assesment: (FEV1/ FVC< .7)
Mild-– SOBOE if hurrying
Moderate– Stops after walk of few
minutes Severe
– SOB on ADL– Resp failure– R CHF
Very Severe– SOB at rest
FEV1% predicted>80%
50%<80%
30%<50%
<30%

Continuum of COPD Management
CTS guidelines, Canadian Respiratory J 2008;SuppA 15:1-8

COPD- Management
Education Smoking cessation Pharmacotherapy Regular exercise is part of therapy-
Education! Inhaled steroids only for repeated
AECB responding to prednisone

Smoking Cessation
Counseling If patient is motivated to quit :
+/- Nicotine replacement (patch, gum, etc) -(doubles success)
+/- Bupropion (Zyban) start 1week prior to quit day (doubles success)
+/- Combination =4x as successful-(40%non smokers after 1 year, c.f. 10%)Champix (varenicline tartrate) –a
pseudonicotine new kid on the block

Champix (varenicline tartrate)
Pseudonicotine ..more effective than Bupropion initially Side efect nausea 15-30% Dose: (half in renal disease)
– .5 mgm qd x 3d– .5mgm bid x 4 d then D/C cigarettes– 1 mgm bid x 12 weeks
Cost: $3.37/day (~ to “patch”; c.f. $1.84/day for Zyban)

Inhaled Anti-Cholinergics: Tiotropium (Spireva)
Useful in COPD– significant increase in Vital Capacity
– may help FEV1
Supplants Ipatropium (Atrovent) as DPI No side effects (?glaucoma
exacerbation) Dose: 18 ug tablet DPI inhaled qAM via
Handihaler Not a limited use drug

COPD long-term management - continued
Bronchodilators – B2 (SABA-> LABA) – and/or Ipatropium/Tiotropium
Steroids: only 10% respond - document response! Combination IS/LABA may increase time between
exacerbations Theophyllines: popularity fluctuates Annual Influenza vaccination ? Pneumovax q 5-10 years

COPD long-term management - continued
Long-term O2 prolongs life:– if PaO2= or<55 mmHg– if SpO2= or<88%– if pulmonary hypertension,
polycythemia, nocturnal desaturation PaO2<60, SpO2<90
– Palliative grounds allowed Antibiotics for purulent bronchitis –
Trimethoprim, Tetracycline, Clavulin, Cefuroxime, Clarithromycin, respiratory quinolone

COPD long-term management - continued
Rehabilitation- exercise! (GOYA to complex)
Breathing exercises (? unproven) Surgery:
– Lung Volume reduction » extra 2 years survival
– Lung transplantation» No longer smokes» Even if alpha 1 pt.» Patient not on a ventilator» Median survival 2-4years

AECB= Acute exacerbation of Chronic Bronchitis
Over 50% associated with infections Average of 2 AECBs/year Diagnose if patient has 2 or 3 of the
following symptoms: – Increase in Dyspnea – Increase in sputum volume – Purulent sputum

Management of AECB
Usual bronchodilator Rx Prednisone 25-50 mgm x 7-14 days Antibiotics will attenuate the AECB
– Faster resolution of clinical criteria and Peak Flow Rates, reduced LOS*
– Choice based on antibiotic hx and local factors
*Anthonisen NR, et al.: Ann Intern Med 1987; 106(2):196-204.

Microbiology of AECB:Most Common Pathogens by Class
Mild COPD– H. influenzae, other Haemophilus species,
S. pneumoniae, M. catarrhalis Moderate COPD with risk factors
– Class I pathogens– Klebsiella sp.– Increased likelihood of beta-lactam-resistance
Severe COPD, – needs hospitalization– Class I and II pathogens– Increased risk of P. aeruginosa

AECB: Antibiotic Therapy
Simple– COPD mild-moderate; FEV1 >50% pred– RX: Tetra, Amoxi, Cephalosporin GI or GII, Macrolide GII
or GIII (clarithromycin or telithromycin)
Complicated– COPD severe; FEV1 <50% pred– Any of
» <4 AECB/year, Chronic O2 rx, Recent antibiotics, CAD, other chronic illness
– RX: Respiratory quinolone, (Gemflox, Levoflox, Moxiflox)
Acute on chronic respiratory failure
Determine cause– ?Pneumonia– ?AECB– ?CHF– ?Sedatives
Assess with spirometry and ABG Oxygenate temperately: avoid greed Drugs: as per asthma, plus Ipatropium
(Atrovent)

Outpatients Inpatients Nursing Home
S. Pneumoniae S. pneumoniae S. pneumoniae
H. Influenzae H. Influenzae H. Influenzae
Atypicals (2)* Atypicals (3)** Atypicals (3) **
GNR GNR**
* Atypicals (2) = M. pneumoniae, C. pneumoniae
** Atypicals (3) = M. pneumoniae, C. pneumoniae, Legionella spp.
GNR = Gram negative rods
–Pathogens in CAPPathogens in CAP
** Negated in EU guidelines

CAP: Selecting Treatment
2nd-gen. cephalosporin + macrolide
Respiratory fluoroquinolone alone or amox/clav + macrolide
S. pneumoniae, enteric Gram-negative rods (?), H. influenzae
Nursing-home residents in nursing home
Doxycycline
Amox/clav + macrolide or 2nd-gen. cephalo-sporin + macrolide
3rd-gen cephalosporin + clindamycin or metronidazole
Macrolides
Respiratory fluoroquinolone
Amox/clav +/- macro-lide, or 4th-gen. cephalosporin
– COPD (no recent anti-biotics or oral steroids within past 3 months)
– COPD (recent antibiotics or oral steroids within past 3 months)—H. influenzae & enteric Gram-negative rods
– Suspected macroaspiration—oral anaerobes
Outpatient w/ modifying factors
DoxycyclineMacrolide—Outpatient w/out modifying factors
Second-choice therapy
First-choice therapyModifying factors and/or pathogens
Type of pneumonia
Mandell LA, et al.: Can J Inf Dis 2000; 11(5):237-47. Adopted by the CIDS and the CTS
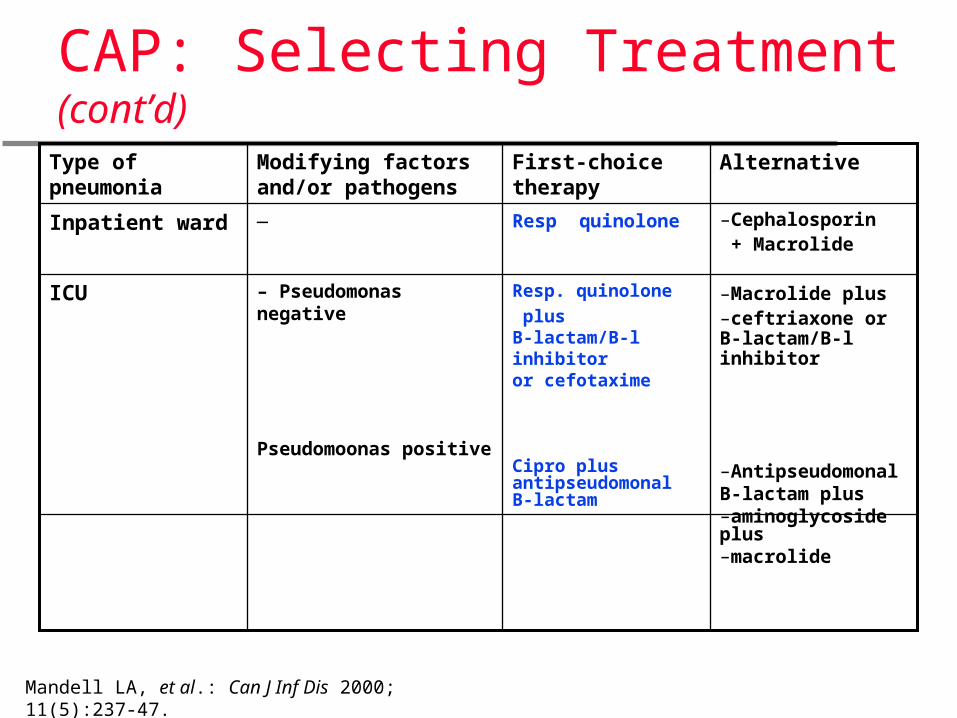
CAP: Selecting Treatment (cont’d)
Resp. quinolone
plus B-lactam/B-l inhibitor or cefotaxime
Cipro plus antipseudomonal B-lactam
– Pseudomonas negative
Pseudomoonas positive
ICU
Resp quinolone—Inpatient ward
AlternativeFirst-choice therapyModifying factors and/or pathogens
Type of pneumonia
Mandell LA, et al.: Can J Inf Dis 2000; 11(5):237-47.
–Cephalosporin + Macrolide
–Macrolide plus –ceftriaxone or B-lactam/B-l inhibitor
–Antipseudomonal B-lactam plus–aminoglycoside plus–macrolide

Pulmonary Arterial Hypertension - Classification
Ideopathic -includes Collagen vascular disease, portal hypertension, HIV, anorexogens
Secondary to Pulmonary venous hypertension - esp CHF
Hypoxemic related PAH
Thrombo-embolic PAH

Pulmonary Arterial Hypertension:Diagnosis
Unexplained exertional dyspnea Isolated impairment of DCO Exercise test Echocardiogram Specialized tests (one or more of):
– Spiral CT– V/Q scan– Pulmonary angiogram

Pulmonary Arterial Hypertension:Therapy of Primary PHtn
Refer to specialty clinic Oxygen if indicated Medications
– …Calcium channel blockers– Epoprostenol (prostacycline analog)– Bosentan (endothelin antagonist)– Sildenofil (PDE5 inhibitor)
Lung transplantation
Dyspnea management in palliation:
Reverse what can be reversed Oxygen for hypoxemia or pre-emptive Opiates -
– Morphine oral »15-120 mgm q12h »s/c route 5-10 mgm q1-6h.
– Dilaudid s/c .5-1.0 mgm q1-6h

Obstructive Sleep Apnea Syndrome
Heavy snoring Daytime hypersomnolence Obesity Other manifestations:
– Hypertension– Unexplained Cor Pulmonale– Nightmares– Impotence– Depression

Obstructive Sleep Apnea Syndrome
Diagnosis:
Sleep study or Polysomnography– EEG to stage sleep– Electro-oculography– EKG– Oronasal airflow– Respiratory effort– SpO2

Obstructive Sleep Apnea Syndrome
RDI= Respiratory disturbance index
= # of apneas or hypopneas/hrMild OSA- RDI 5-15
Moderate OSA RDI 16-30
Severe OSA RDI >30 Therapy:
– Weight reduction– CPAP / BiPAP– Mandibular Prosthesis, Tracheostomy

LMCC topics understressed
Hemoptysis:– Refer if major (>200 ml / 24 hours)– Treat the cause– Antibiotics
Pleural effusion– Treat the cause– Drain if pus– Pleurex indwelling catheter if chronic– Pleurodesis if cancer prognosis>3 months and
pleurex support not available