response adaptive randomization in clinical trials - cctst kim 2011-06-17.pdf · response adaptive...
TRANSCRIPT

Response Adaptive Randomization in Clinical Trials
Mi-Ok Kim
Associate Professor of PediatricsDiv. of Biostatistics and Epidemiology
CCHMC, UC College of MedicineSupported by CCTST Method Grant
June 17th, 2011
?Statistical Heresy

When info. is available,
• Shall we use it? – Yes.
• What about if the information is from an ongoing clinical trial and we consider using the information to change some aspects of the trial under way? – No.


A Dilemma Faced by Dr. Chmielowski
• Mr. McLaughlin: the experimental drug stopped the growth of the tumor.
• Mr. Ryan: chemotherapy, priori known ineffective, could not hold back the tumors.
• Mr. Ryan is highly likely to benefit from the experimental drug yet would not be allowed to switch as it would muddy the trial’s results.

Conflicts of Convent. Design w Ethics
• Why wouldn’t Mr. Ryan be allowed to cross-over to the experimental drug?
• Why hadn’t Mr. Ryan be given a greater than 50:50 chance of being assigned to the experimental drug?

Outline
• Response Adaptive Design– Frequentist/Bayesian Approach
• Early Immunomodulator Trt Use in Pediatric Ulcerative Colitis Patients– Motivation
– Logistical & Statistical Issues
– Simulation Results
• Conclusion

Response Adaptive Randomization (RAR)
• Skews alloca. prob. away from equal alloca. over the course of a trial to favor the better orbest performing trt arm adaptively based on resp. data accrued thus far w/o undermining the validity and integrity of the trial
• Allocation prob. are adapted “by design”, not on “ad hoc” basis.
• Same inference procedure works as with a fixed (non-adaptive) design

Randomized Play-the-Winner
Success
FailureSuccess

Doubly Biased Coin Design
• Pick a target allocation – E.g) Minimizing the expected total # of failures
• True unknown. • Use estimates based on available data
successively over the course of a trial.
CT
T
ppp
CT pp ,


How to compare different designs?
Suppose a target allocation probability is given & the sample size is fixed:
The power increases as the variance of the sample allocation ratio gets smaller (Hu & Rosenberger, 2003)


Ped. U Colitis Pts
• Current trt regimens are far from optimal.– Up to 45% on corticosteroid (CS) 1yr after Dx.
– Up to 26% receiving colectomy within 5yrs post Dx
– No guidance as to who shall receive IM therapy, not 5-ASA monotheray, the least toxic UC drug
• PROTECT: observational study that aims to– Est. the success rate of standardized therapeutic
protocol
– Develop a prediction model
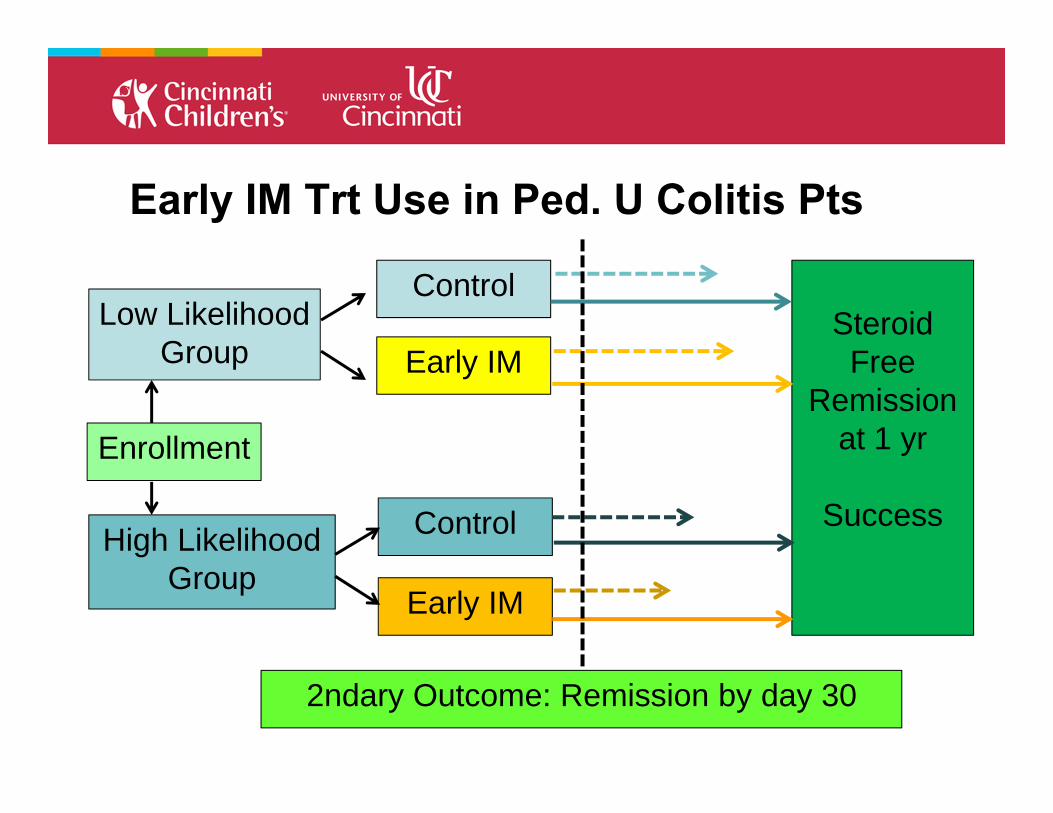
Early IM Trt Use in Ped. U Colitis Pts
Enrollment
High Likelihood Group
Early IM
Control
Early IM
Control
Low Likelihood Group
SteroidFree
Remission at 1 yr
Success
2ndary Outcome: Remission by day 30

Doubly Biased Coin Design
• Pick a target allocation – Urn model
• Estimate the unknown based on available data
%3.58)1()1(
1
CT
C
ppp
CT pp ,

Issues in Implementing an RAR Design
1. Delay in the response
2. Heterogenous pt population • Okay.
• DABCD (Duan and Hu, 2007), Urn model (Bai & Hu, 1999, 2005), Drop-the-loser rule (Zhang, et. al., 2007)
• Okay. Update when resp. become available.
• DABCD (Hu et al., 2007), Urn model (Bai et al., 2002; Hu and Zhang, 2005), Drop-the-loser rule (Zhang, et. al., 2007)

Issues in Implementing an RAR Design
1. Delay in the response
2. Heterogenous pt population • Use the short-term Seconndary endpoint as a
strata variable.
• Use the Kaplan-Meier estimator to incorporate the delayed (or unavailable) responses & to update based on all available data.

Proposed Method
1. “Standard” Method: Primary Only / Primary + Secondary
2. K-M Method: Primary Only / Primary + Secondary
Heterogeneous delays are okaySimulation – Use the Ped. IBD Collaborative
Research Group Registry (n=353)

0 50 100 150 200
0.45
0.50
0.55
0.60
Low Likelihood Group, Long Delay
Patient number in the order of entry
Mea
n %
Pat
ient
s as
sign
ed to
the
TRT
grou
p
"Standard" methodK-M method

0 50 100 150 200
0.45
0.50
0.55
0.60
High Disk, Short Delay, n=228
Patient number in the order of entry
Per
cent
age
of p
atie
nts
assi
gned
to th
e tre
atm
ent g
roup
Standard methodProposed method
Low likelihood Group, Short Delay
K-M method

1 9 19 31 43 55 67 79 91 104 119 134 149 164 179 194 209
0.2
0.3
0.4
0.5
0.6
0.7
0.8
"Standard" Method, Long Delay
Patient number in the order of entry
% P
atie
nts
assi
gned
to th
e TR
T gr
oup
Primary only

1 9 19 31 43 55 67 79 91 104 119 134 149 164 179 194 209
0.2
0.3
0.4
0.5
0.6
0.7
0.8
"Standard" Method, Long Delay
Patient number in the order of entry
% P
atie
nts
assi
gned
to th
e TR
T gr
oup
1 9 19 31 43 55 67 79 91 104 119 134 149 164 179 194 209
0.2
0.3
0.4
0.5
0.6
0.7
0.8
Primary onlyPrimary+Secondary

Results (2000 simulated data replicates)
N ≈ 228(0.5 vs 0.3)
Fixed
Primary Only Primary + Secondary
“Standard” K-M “Standard” K-M
90.8 (80.7%) 93.1 (80.3%) 94.7 (80.7%) 92.9 (78.8%) 94.8 (79.5%)
99.7 (91.6%) 103.4 (88.7%) 101.8 (94.0%) 104.7 (93.5%)

Bayesian Approach
• Prior knowledge about parameters + Data = Posterior knowledge about parameters
• Prior for rate of success stratified by the secondary endpoint.
• Require more extensive pre-trial research to appropriately design the approach with acceptable operating characteristics

Bayesian Approach
• When the priors are appropriately specified, may perform better.

When Bayesian approach may help?
• When there exist sufficient priori info. on which to base a relatively strongly informative prior – may bring substantially greater gain.
• Continuous assessment of trt effects is natural. Easier to incorporate early stopping rules and multiple hypotheses. • Testing a drug in genetically defined many sub-
patient populations
• Testing many drugs with limited resources

Conclusion
• Response adaptive randomization is a well-established randomization method that increases pt benefit without undermining the validity or integrity of clinical trials.
• RAR can be applied for delayed responses, while maintaining the benefits of the adaptive design.
• Bayesian approach can be more beneficial

• Ms. Chunyan Liu (DBE)• Dr. Jack J. Lee (MD Anderson)• Dr. Feifang HU (Univ. of Virginia)• Dr. Lee Denson (Direct Inflammatory Bowel
Disease Center at CCHMC)• the Ped. IBD Collaborative Research Group
• Dr. Lili Ding (DBE) – Adaptive Dose Finding • Ms. Yangqing Hu – Covariate Adaptive
Randomization Design

References• Hu, F. and Rosenberger, W.F. (2003). Optimality, variability, power:
Evaluating response-adaptive randomization procedures for treatment comparisons. Journal of the American Statistical Association, 98, 671-678.
• Hu, F. F., L. X. Zhang, et al. (2008). Doubly adaptive biased coin designs with delayed responses. Canadian Journal of Statistics-Revue Canadienne De Statistique 36(4): 541-559.
• Bai, Z., Hu, F. and Rosenberger, W.F. (2002). Asymptotic properties of adaptive designs for clinical trials with delayed response. Ann. Statist. Vol 30, No 1, 122-139.
• Hu, F. and Zhang, L.X. (2004). Asymptotic normality of adaptive designs with delayed response. Bernoulli. 10, 447-463.
• Zhang, L.-X., Chan, W.S., Cheung, S.H., Hu, F.A generalized drop-the-loser urn for clinical trials with delayed responses. (2007) Statistica Sinica, 17 (1), pp. 387-409.

• Duan, L. L. and F. F. Hu (2009). Doubly adaptive biased coin designs with heterogeneous responses. Journal of Statistical Planning and Inference 139(9): 3220-3230.
• Bai, Z. D. and Hu, Feifang (1999) Asymptotic theorems for urn models with nonhomogeneous generating matrices. Stochastic Processes and their applications, Vol. 80, 87-101.
• Bai, Z. D. and F. F. Hu (2005). Asymptotics in randomized URN models. Annals of Applied Probability 15(1B): 914-940.
• Hu, F. and W. F. Rosenberger (2006). The theory of response-adaptive randomization in clinical trials. Hoboken, N.J., Wiley-Interscience.
References