resting state fmri changes during spinal cord stimulation chima o.oluigbo, md, amir abduljalil, phd,...
TRANSCRIPT

Resting state fMRI changes during Spinal Cord Stimulation
Chima O.Oluigbo, MD, Amir Abduljalil, PhD, Xiangyu Yang, PhD, Andrew Kalnin, MD,
Michael V. Knopp, MD, PhD, Ali R. Rezai, MDCenter for Neuromodulation, Departments of
Neurosurgery and Radiology, Wexner Medical Center at The Ohio State University Hospital

Disclosure
• No personal disclosures
• Funding by Medtronic

Farmer et al. Neuroscience Letters 520 (2012): 197-203
• 70 million Americans, $150 billion per annum, • Develop innovative therapies • New methods to evaluate and characterize pain• Cerebral “signature” for pain perception and
modulation• Neural network changes – depression, addiction
Background – Chronic Pain

Resting State fMRI • Allows interrogation of myriad functional systems without the constraints of a priori hypothesis
• Imaging the brain during rest reveals large-amplitude spontaneous low-frequency (<0.1 Hz) fluctuations
• Temporally correlated across functionally related areas
• “Functional connectome”• Default mode network
Medial prefrontal cortex (MPC)
Posterior cingulate/Precuneus (PCC)
Lateral parietal cortex (LPC)
DEFAULT MODE NETWORK

Clinical model – Neuropathic extremityClinical model – Neuropathic extremitypain and spinal cord stimulationpain and spinal cord stimulation

Design Overview
• OSU IRB approved research study• 7 patients• Thoracic epidural SCS in place for treatment of
CRPS or neuropathic leg pain following FBSS involving one or both lower extremities

Pre-Imaging Clinical evaluation
• Determine stimulation parameters associated with:
1. SCS Perception threshold
2. “Optimal” pain reduction
3. Uncomfortable stimulation threshold
Pain QuantificationPain Quantification
Pain quantification was based on the Visual-Analog Scale (VAS) and the measure of percentage change in pain (∆P%) was determined as follows:
∆P% = 100x (POFF – PON)/POFF
where PON is the VAS pain rating as reported by the subject during stimulation while POFF is the pain rating reported with the stimulator switched OFF.

MRI safety
• Under OSU IRB approved research study, modeling analysis and laboratory measurements were performed
• Determined that the Neuromodulation devices would perform safely under the restrictions of this particular research protocol, MRI equipment, and implant restrictions.
• Note: cannot be extrapolated to other studies or other systems

fMRI protocol• 7 subjects• 1 control – 5 sessions of resting fMRI on different days• Resting state fMRI• 3 T Achieva Philips scanner, transmit /receive head coil. • Functional EPI images acquisition: isotropic spatial resolution of 3 mm,TR/TE
2000/30 ms, 80° flip angle, 80×80 matrix size, 35 slices. • B0 field map and a high resolution 3D T1 weighted image also acquired: TR/TE
7.9/3.7 ms, 1×1×1 mm3 voxel resolution. • Image analysis using FSL (FMRIB Software) and AFNI (NIMH/NIH) tools. • Functional images were motion corrected, smoothed (5 mm3) and band-pass
filtered (0.005<f<0.1 Hz).
– 10 minutes scans– Simulation
• Off• Low• Optimum• High
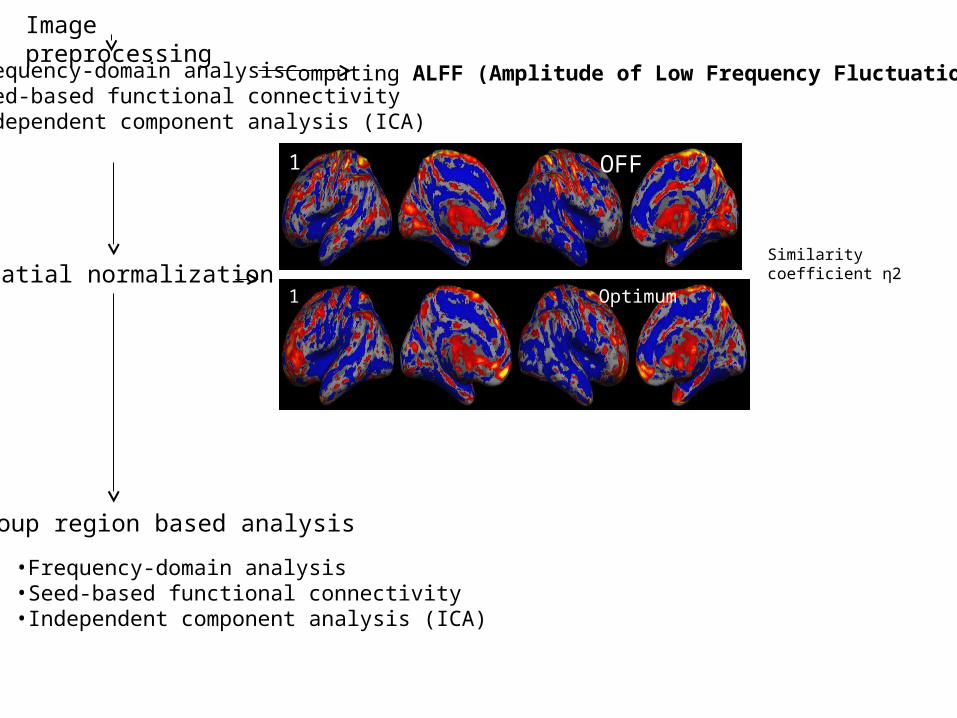
Image preprocessing
Computing ALFF (Amplitude of Low Frequency Fluctuation)
Spatial normalization
Group region based analysis
OFF
Optimum
1
1
Similarity coefficient η2
•Frequency-domain analysis•Seed-based functional connectivity•Independent component analysis (ICA)
•Frequency-domain analysis•Seed-based functional connectivity•Independent component analysis (ICA)

Results 1: Pain change calculations
Subject ∆P% (Optimum) ∆P% (Supra-optimal)
1 40% 100%
2 0% -16.6%
3 29.4% 41.2%
4 71.4% 71.4%
5 50% 57.1%
6 27% 63.6
7 75% 100%
∆P% = 100x (POFF – PON)/POFF

Frequency Domain Analysis – Amplitude of Low Frequency Fluctuation(ALFF)
• ALFF represents the average amplitude in the low-frequency band (0.01–0.08 Hz).
• Reflects the intensity of regional spontaneous brain activity
• Calculated by averaging the square root of the power spectrum of a given low-frequency BOLD time course across the frequencies filtered
• The fALFF shows the ratio of power spectrum of low-frequency (0.01-0.08 Hz) to that of the entire frequency range. It is inverse to ALFF

Chronic pain – Stimulator OFF (Group summation, n = 7)
Normal control (n = 5)
ALFF
-4.5 4.5

Normal control
Chronic pain – Stimulator OFF (Group summation)
fALFF
-4.5 4.5
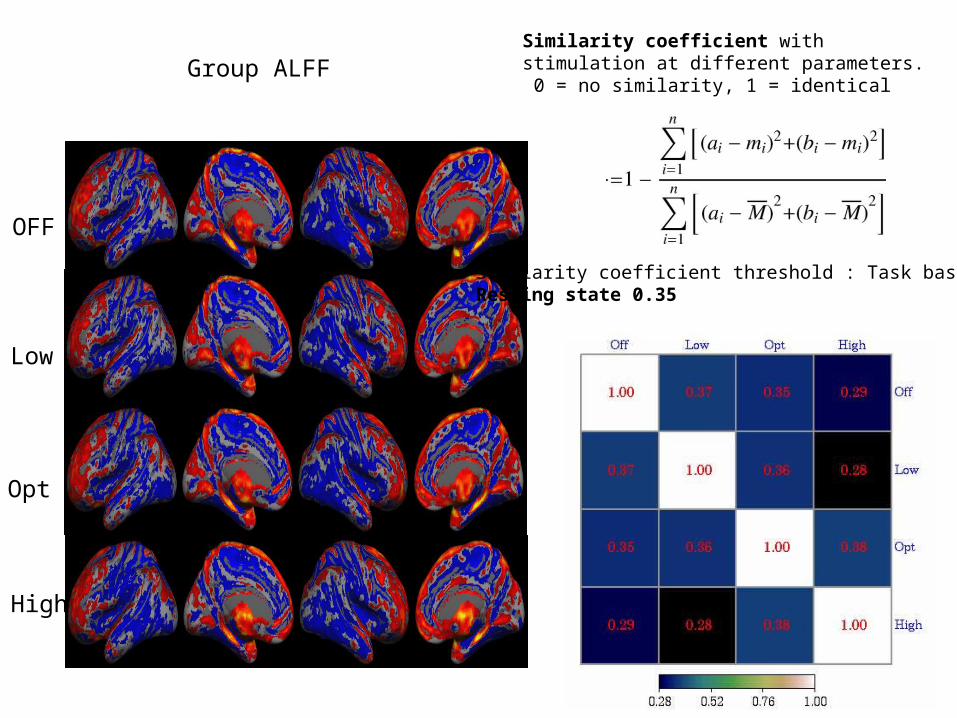
Similarity coefficient with stimulation at different parameters. 0 = no similarity, 1 = identical
OFF
Low
Opt
High
Group ALFF
Similarity coefficient threshold : Task based 0.5Resting state 0.35

Global Similarity coefficient 0 = no similarity, 1 = identical
Threshold ≤ 0.35

Seed based correlation analysis
Involves the a priori selection of a voxel, cluster or atlas region and then calculate whole-brain, voxel-wise functional connectivity maps of co-variance with the seed region.

Pain related seeds
R DLPFC (right dorsolateral prefrontal cortex) 44 36 20
L DLPFC (left dorsolateral prefrontal cortex) -34 31 34
FMC (Frontal medial cortex = Medial orbitofrontal) 0 42 -18
LFI (Left orbital frontoinsula = Left anterior insula) -32 24 -10
RFI (Right orbital frontoinsula = Right anterior insula) 38 26 -10
LAccu (Left nucleus accumbens) -10 12 -8
RAccu (Right nucleus accumbens) 10 10 -8
LAmyg (Left amygdala) -20 -6 -20
RAmyg (Right amygdala) 28 -6 -20
LPIN (Left posterior insula) -39 -24 16
RPIN (Right posterior insula) 38 14 6
RACCX (Right Anterior Cingulate Cortex) = RCC 6 38 14
LACCX (Left Anterior Cingulate Cortex) -2 36 6
Task positive seeds
IPS (Interparietal sulcus) -38 -46 54
FEF (Frontal eye field) 26 -12 50
MT (Middle temporal) -46 -68 -2
Default Mode Network Seeds
MPF (Medial prefrontal cortex) -2 46 -16
PCC (Posterior cingulated / precuneus) -4 -50 40
LP (Lateral parietal cortex) -46 -68 36
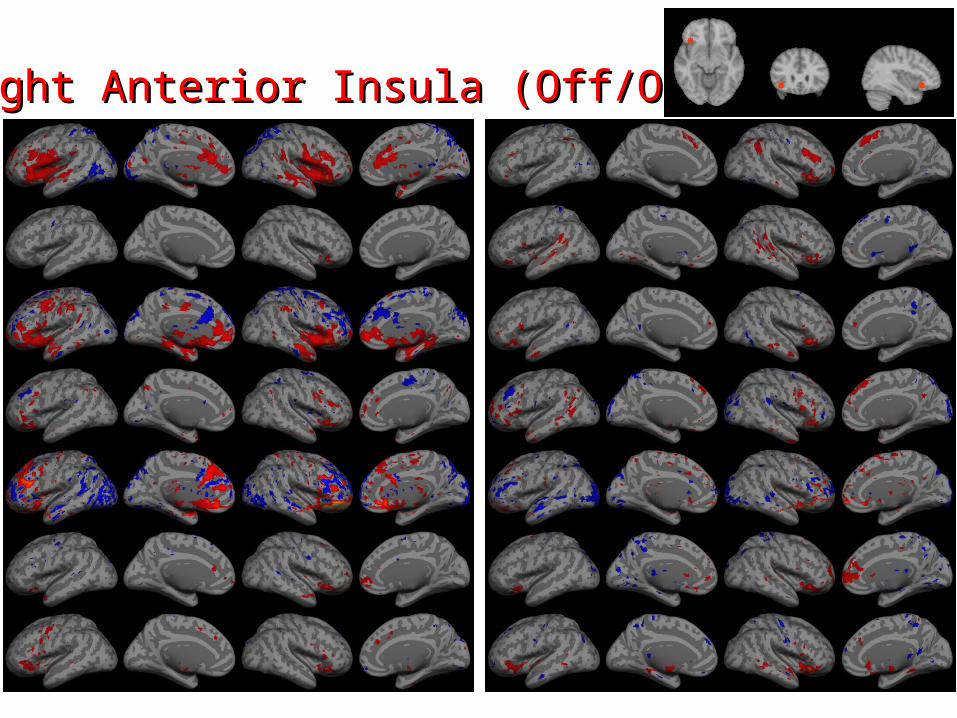
Right Anterior Insula (Off/Opt)Right Anterior Insula (Off/Opt)
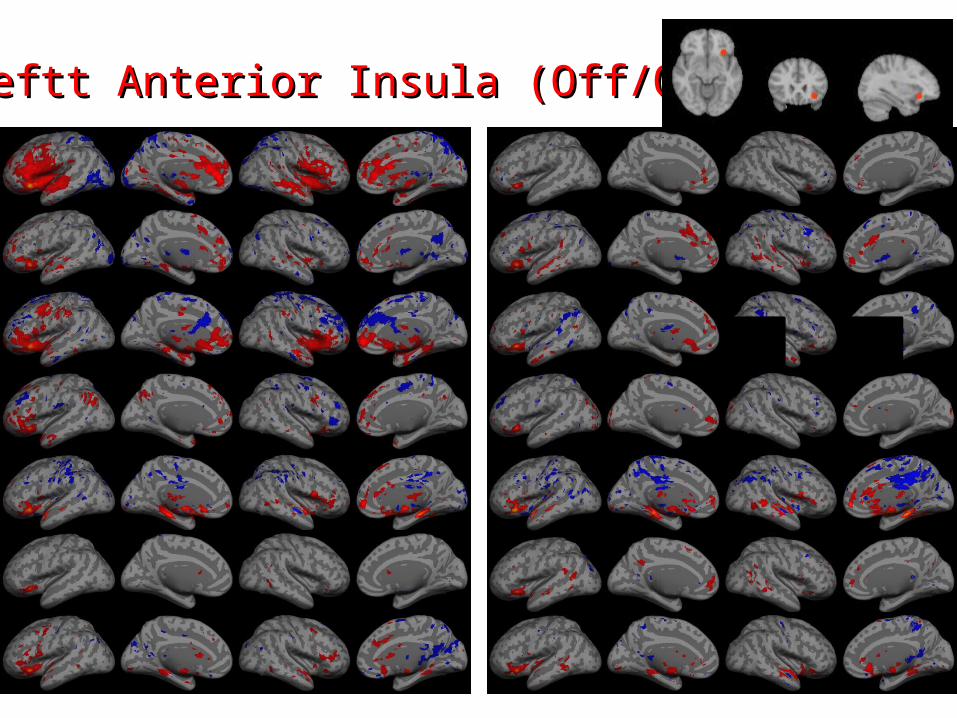
Leftt Anterior Insula (Off/Opt)Leftt Anterior Insula (Off/Opt)
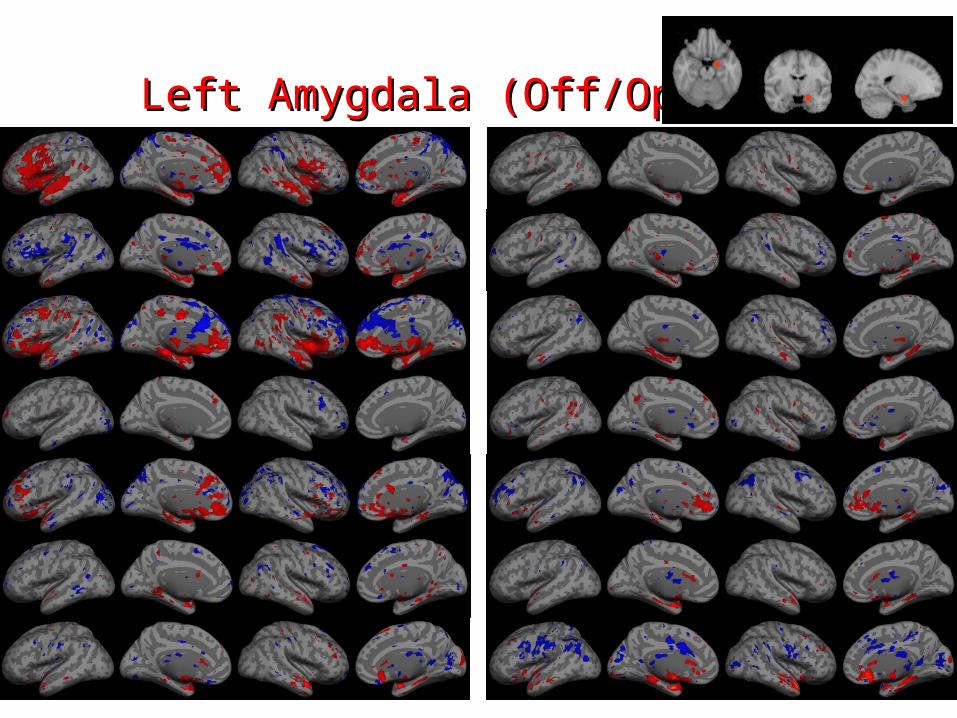
Left Amygdala (Off/Opt)Left Amygdala (Off/Opt)
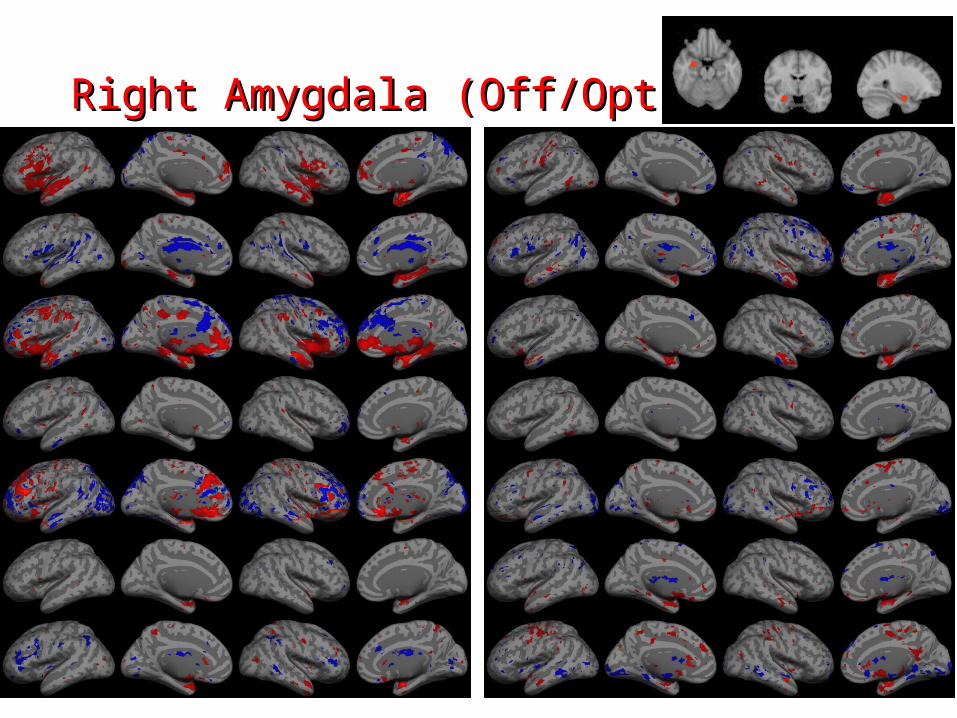
Right Amygdala (Off/Opt)Right Amygdala (Off/Opt)

Structural Equation Modeling (SEM)
• Causality modeling approach
• Provide measure of effective connectivity
• Model driven (ie ROI dependent)
• Provide confirmation for hypothesis testing
• SEM does not prove causation

Group OffGroup Off
**
* **

Group LowGroup Low

Group OptimumGroup Optimum

Group HighGroup High

Farmer et al. Neuroscience Letters 520 (2012): 197-203

Conclusions• SCS influences supraspinal (cerebral) pain
neuromodulation – indirect / direct• Pain control during spinal cord stimulation is
associated with change in connectivity between anterior insula (and amygdala) and components of the default mode network (DMN)
• ALFF in the region of the DMN is lower in patients with chronic pain compared to control.
• Spatially correlated fluctuations in resting state fMRI signals may be a neuroimaging surrogate for higher order pain perception and its modulation in chronic pain states

Thank you