results of a phase 1 trial of treg ... - tract therapeutics
TRANSCRIPT

Results of a Phase 1 Trial of Treg Adoptive Cell Transfer (TRACT) in De Novo Living Donor Kidney Transplant
Recipients
A Skaro, A LeFever, J Mathew, L Gallon, J Hie, C
Hansen, D Stare, G Johnson, J Leventhal
June 13, 2016
ATC Boston MA
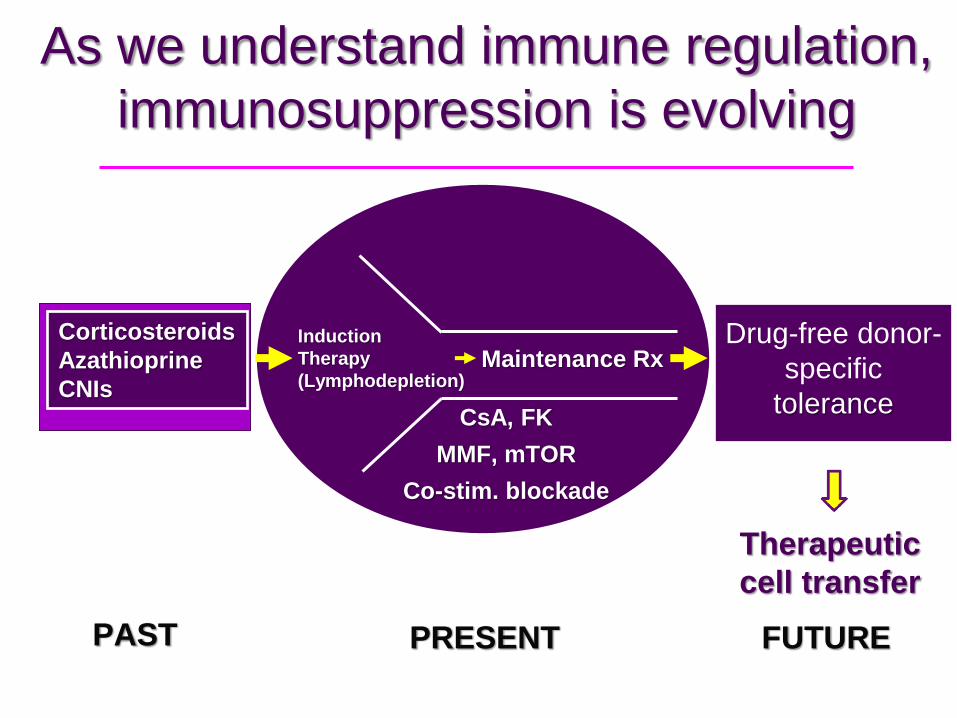
As we understand immune regulation,
immunosuppression is evolving
Induction
Therapy
(Lymphodepletion) Maintenance Rx
CsA, FK
MMF, mTOR
Co-stim. blockade
PRESENT
Corticosteroids
Azathioprine
CNIs
Drug-free donor-
specific
tolerance
PAST FUTURE
Therapeutic
cell transfer

Cell Therapies being considered for Tolerance Induction
HSC to induce chimerism
HSC to induce immunomodulation
Regulatory T cells Dendritic cells (DC)
Mesenchymal Stem Cells (MSC)
Apoptotic Cell Delivery (ECDI, ECP)
Future possibilities Combination of cell types (HSC + Treg)
Single vs multiple infusions
Derived from the thymus and/or
peripheral tissues
Demonstrated to broadly control T cell
reactivity.
Control immune responsiveness to
alloantigens
Contribute to operational tolerance in
transplantation models
Regulatory CD4+CD25+FoxP3+ T cells
Wood KJ and Sakaguchi S. Nat Rev Immunol. 2003 Mar;3(3):199-210.

Tregs in transplantation: clinical evidence
Higher circulating numbers of Tregs in tolerant kidney transplant recipients
Increased numbers of Tregs in tolerant liver transplant recipients
Improved outcomes in stem cell transplant patients receiving infusion of expanded Tregs
Sagoo P, Perucha E, Sawitzki B, et al. Development of a cross-platform biomarker signature to detect renal transplant tolerance in humans. J Clin Invest 2010; 120:1848. Wood KJ, Regulatory T. cells in transplantation. Transplant Proc 2011; 43: 2135. Leventhal JR, Mathew JM, Salomon DR, et al. Am J Transplant. 2016 Jan;16(1):221-34. Nonchimeric HLA-Identical Renal Transplant Tolerance: Regulatory Immunophenotypic/Genomic Biomarkers Sawitzki B, Brunstein C, Meisel C, et al. Prevention of graft-versus-host disease by adoptive T regulatory therapy is associated with active repression of peripheral blood Toll-like receptor 5 mRNA expression. Biol Blood Marrow Transplant. 2014 Feb;20(2):173-82.
5

Lymphodepletion maximizes efficacy of Treg therapy
0
20
40
60
80
100
0 14 28 42 56 70 84 98
Days Post-Transplantation
% G
ra
ft S
urv
iva
l
No nTreg
TGF-β/IL-2 nTreg
RA/TGF-β/IL-2 nTreg
TSA/RA/TGF-β/IL-2 nTreg
Lymphodepletion to reduce numbers of circulating effector T cells
may be an important adjunct to the use of Tregs as a cellular
therapy in organ transplantation

Design: Single center, open label, nonrandomized
Objectives: Determine the safety of using expanded Treg Adoptive
Cell Transfer (TRACT).
Investigating whether TRACT leads to transplant
rejection/allosensitization and/or nonspecific
immunosuppression
Performing limited immune monitoring.
Methodology: dose escalation of expanded autologous nTregs in
experimental arm (0.5, 1, 5 & x109 cells/subject , n=3 in each tier)
Primary Outcome Measure: Patient and Graft survival @ 1year
A PHASE 1 TRIAL OF
TREG ADOPTIVE CELL TRANSFER (TRACT)
IN LIVING DONOR KIDNEY TRANSPLANT RECIPIENTS

Inclusion Criteria
Patients males or females age 18-65 years.
No prior organ transplant.
Patients who are single-organ recipients (kidney only).
Women of childbearing potential must have a negative
serum pregnancy test and agree to use a medically
acceptable method of contraception throughout the
treatment period.
Recipient is able to understand the consent form and
give written informed consent.
Exclusion Criteria 1. Known sensitivity or contraindication to Sirolimus, tacrolimus or MMF.
2. Patient with significant or active infection.
3. Patients with a positive flow cytometric crossmatch using donor lymphocytes and
recipient serum.
4. Patients with PRA >20%.
5. Patients with current or historic donor specific antibodies.
6. Body Mass Index (BMI) of < 18 or > 35.
7. Patients who are pregnant or nursing mothers.
8. Patients whose life expectancy is severely limited by diseases other than renal disease.
9. Ongoing active substance abuse, drug or alcohol.
10. Major ongoing psychiatric illness or recent history of noncompliance.
11. Significant cardiovascular disease (e.g.):
• Significant non-correctable coronary artery disease;
• Ejection fraction below 30%;
• History of recent myocardial infarction.
12. Malignancy within 3 years, excluding non-melanoma skin cancers.
13. Serologic evidence of infection with HIV or HBVsAg positive.
14. Patients with a screening/baseline total white blood cell count < 4,000/mm3; platelet
count < 100,000/mm3; triglyceride > 400 mg/dl; total cholesterol > 300 mg/dl.
15. Investigational drug within 30 days prior to transplant surgery.
14. Anti-T cell therapy within 30 days prior to transplant surgery.

Summary of Enrolled Subjects
PCKD – polycystic kidney disease
HTN – hypertension
FSGS – focal segmental glomerulosclerosis
Subject
#
Subject
Initials
Gender Age at
Transplant
Race Cause of ESRD
1 ECW Male 52y 1m Black HTN/FSGS
2 L-N Female 28y 9m White FSGS
3 A-O Male 47y 8m Hispanic/Latino PCKD
4 J-R Male 30y 3m Hispanic/Latino Membranous
Nephropathy
5 JTM Male 53y 0m White HTN
6 V-P Female 24y 6m Native
Hawaiian /
Pacific Islander
Lupus
7 KMG Male 37y 2m White IgA Nephropathy
8 K-G Male 62y 3m White PCKD
9 B-G Female 57y 7m White PCKD

Pretransplant collection of
recipient lymphocytes via leukopheresis;
cryopreservation of cells (1 week -
1year Pretransplant)
Day 0: Living Donor Kidney Transplant:
Alemtuzumab Induction, Tacrolimus and Mycophenolate
based IS; conversion from Tac to Sirolimus
Day +30
Initiate isolation and expansion of
autologous Tregs; infusion of expanded
cells Day +60; protocol biopsy at 3 months and 1 year
post-Tx
Clinical Protocol
Isolation and Manufacture of Autologous Polyclonal Tregs
Leukopheresis of recipient pre-transplant
Immunomagnetic selection of Tregs
(CD8,CD19 negative depletion, CD25 positive
selection) from cryopreserved “raw product”
Ex vivo culture and expansion of Tregs
In process testing of expanded cells for
phenotype, function, and sterility

Release Criteria for expanded Tregs
>70% cell viability
CD4+/CD25+ > 70%; CD8+.CD19+ <10%
endotoxin < 5 EU/kg
gram stain negative; aerobic, anaerobic and
fungal sterility
mycoplasma negative
residual bead count <3,000 beads per 108 cells
>50% suppression at a 1:2 Treg:Teffector cell
ratio in a mixed lymphocyte reaction
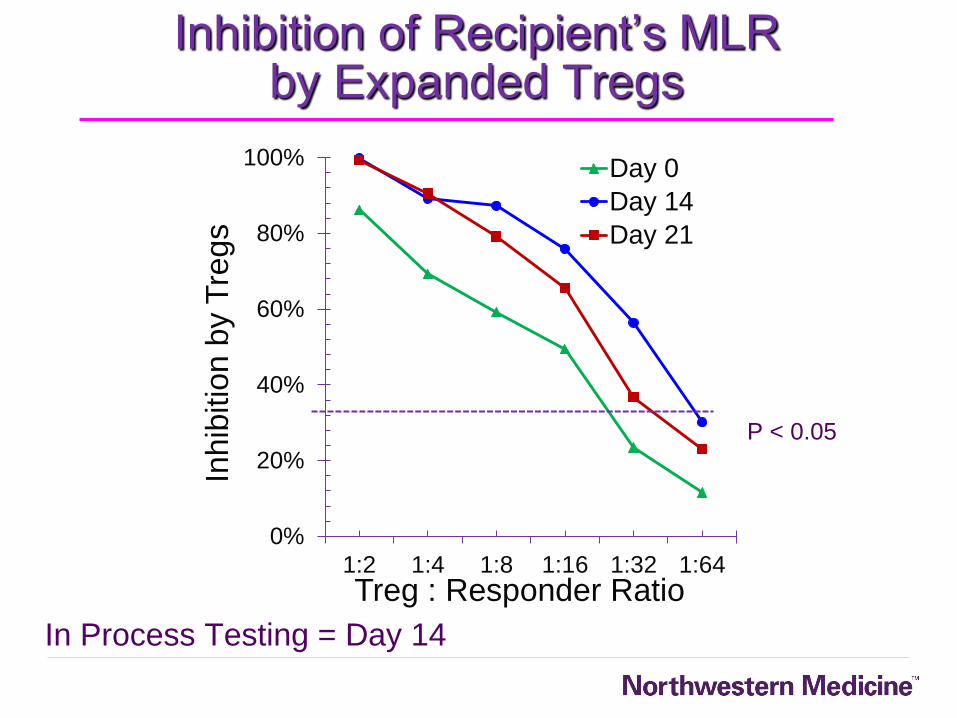
0%
20%
40%
60%
80%
100%
1:2 1:4 1:8 1:16 1:32 1:64
Inhib
itio
n b
y T
regs
Treg : Responder Ratio
Day 0
Day 14
Day 21
Inhibition of Recipient’s MLR by Expanded Tregs
In Process Testing = Day 14
P < 0.05
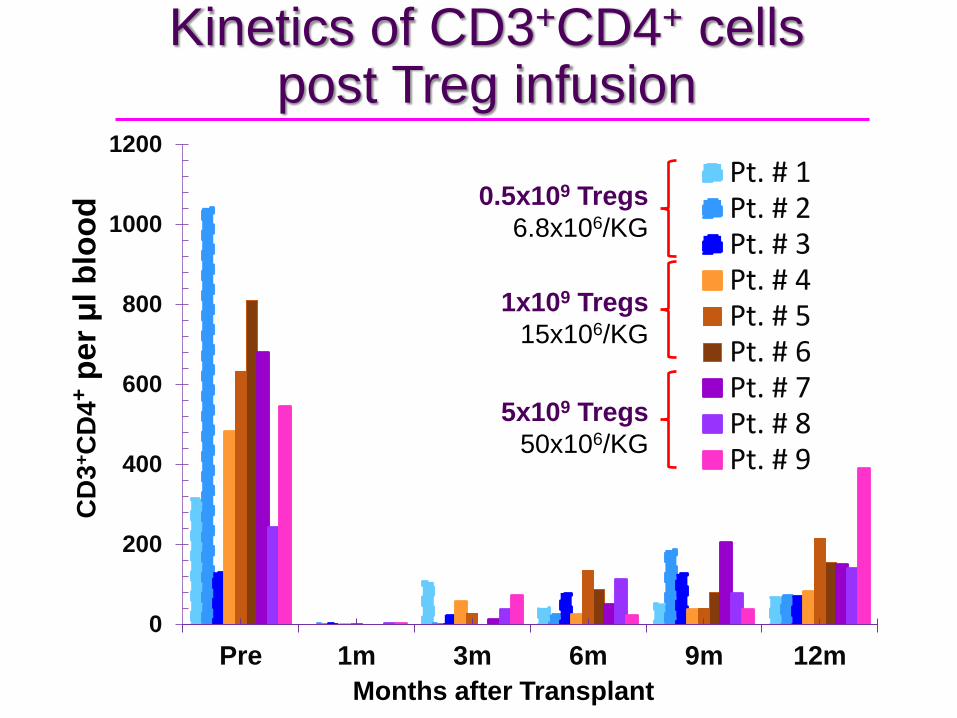
Kinetics of CD3+CD4+ cells post Treg infusion
0
200
400
600
800
1000
1200
Pre 1m 3m 6m 9m 12m
Pt. # 1Pt. # 2Pt. # 3Pt. # 4Pt. # 5Pt. # 6Pt. # 7Pt. # 8Pt. # 9
CD
3+C
D4
+ p
er μ
l b
loo
d 0.5x109 Tregs
6.8x106/KG
1x109 Tregs
15x106/KG
5x109 Tregs
50x106/KG
Months after Transplant

0
5
10
15
20
25
Pre 3m 6m 9m 12m
Pt. #1
Pt. #2
Pt. #3
Pt. #4
Pt. #5
Pt. #6
Pt. #7
Pt. #8
Pt. #9
Fo
ld C
han
ge f
rom
Pre
-Tx i
n
% o
f C
D4
+C
D127
- CD
25
hig
hF
oxP
3+
Cell
s
TRACT
Increased circulating Tregs post Treg infusion
0.5x109 Tregs 6.8x106/KG
1x109 Tregs 15x106/KG
5x109 Tregs 50x106/KG
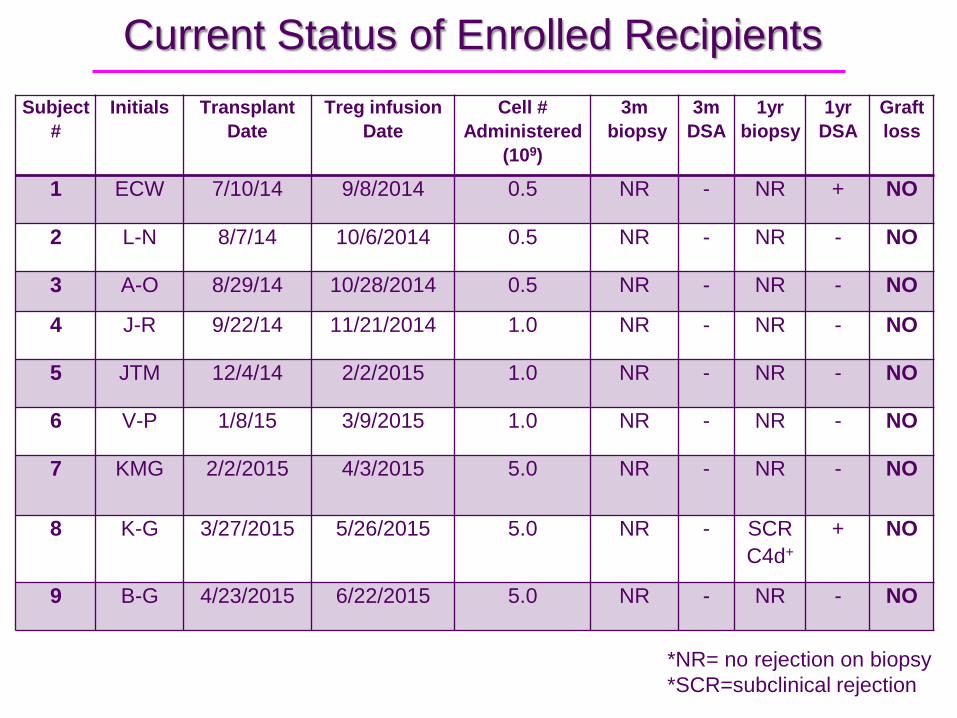
Current Status of Enrolled Recipients
Subject
#
Initials Transplant
Date
Treg infusion
Date
Cell #
Administered
(109)
3m
biopsy
3m
DSA
1yr
biopsy
1yr
DSA
Graft
loss
1 ECW 7/10/14 9/8/2014 0.5 NR - NR + NO
2 L-N 8/7/14 10/6/2014 0.5 NR - NR - NO
3 A-O 8/29/14 10/28/2014 0.5 NR - NR - NO
4 J-R 9/22/14 11/21/2014 1.0 NR - NR - NO
5 JTM 12/4/14 2/2/2015 1.0 NR - NR - NO
6 V-P 1/8/15 3/9/2015 1.0 NR - NR - NO
7 KMG 2/2/2015 4/3/2015 5.0 NR - NR - NO
8 K-G 3/27/2015 5/26/2015 5.0 NR - SCR
C4d+
+ NO
9 B-G 4/23/2015 6/22/2015 5.0 NR - NR - NO
*NR= no rejection on biopsy
*SCR=subclinical rejection

Summary & Conclusions
Efficient expansion of Tregs from cryopreserved leukopheresis product from all recipients met release criteria
No infusion related serious adverse events (5 x 109 poly Tregs are safe)
No evidence of over immunosuppression (opportunistic infections)
Post-infusion protocol biopsies at 3 months have been normal
Serial immunophenotypic analysis of subjects shows a sustained increase in circulating Tregs following Treg infusion
Data support the design and initiation of a Phase 2 trial
FDA approval for Phase 2 trial secured

Woman’s Board of Northwestern Memorial Hospital
John & Lillian Mathews Regenerative Medicine Endowment
Miltenyi BioTec
National Kidney Foundation of Illinois
TRACT Therapeutics Inc.
Jessica Heinrichs
Acknowledgements

Thank you

Questions?
Results of Phase 1 Trial of Treg Adoptive Cell Transfer in Living Donor Kidney Transplant Recipients

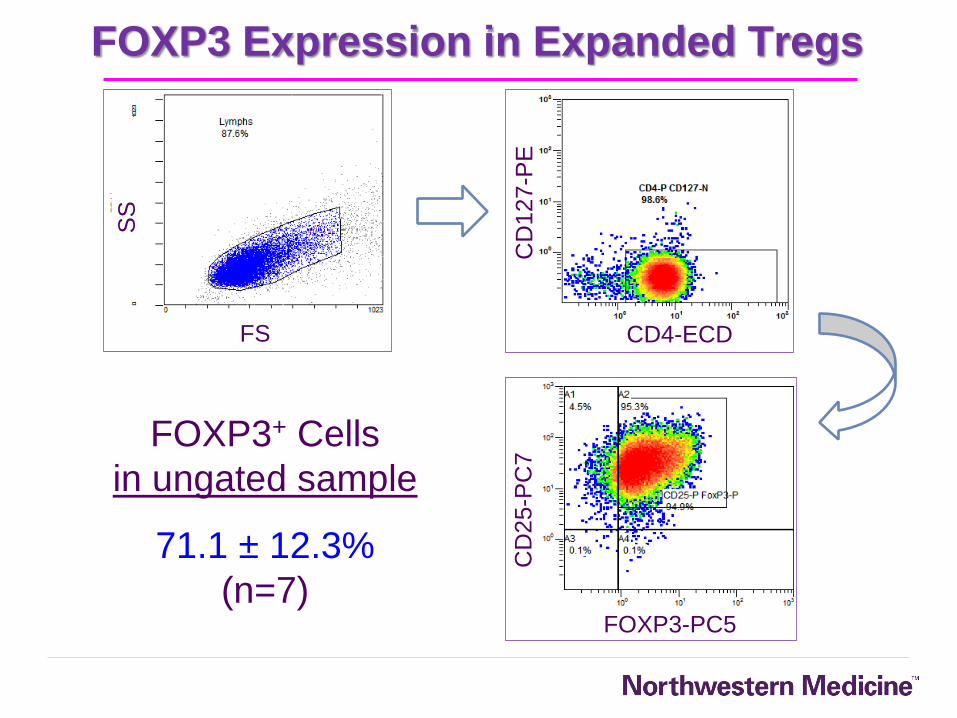
FOXP3 Expression in Expanded Tregs
SS
FS
CD
127-P
E
CD4-ECD
CD
25-P
C7
FOXP3-PC5
FOXP3+ Cells
in ungated sample
71.1 ± 12.3%
(n=7)