review article - jcp.bmj.com · ria in large numbers on the surface of gastric type epithelial...
TRANSCRIPT

J Clin Pathol 1986;39:353-365
Review article
Campylobacter pyloridis, gastritis, and pepticulcerationCS GOODWIN,* JA ARM STRONG,t BJ MARSHALL:
From the Departments of *Microbiology, tElectronmicroscopy, and tGastroenterology, Royal Perth Hospital,Western Australia
SUMMARY Campylobacter pyloridis is a spiral bacterium which was seen by histopathologists severalyears before it was cultured in 1982 in Perth, Western Australia. It has unique cellular fatty acids,predominantly tetradecanoic acid and cis- 11, 12 methylene octadecanoic acid. It also has a uniqueultrastructure which is different from that of other campylobacters. C pyloridis possesses a powerfulurease enzyme and produces large amounts of extracellular catalase. Both these features may beimportant virulence factors, allowing it to occupy a protected niche in the stomach below the mucuslayer but above the gastric mucosa. Specific lesions are found in the gastric mucosa, and ultra-structural studies show the presence of adherence pedestals identical with those found with entero-pathogenic Escherichia coli of the intestine. Histological examination of gastric biopsy tissue hasshown that C pyloridis is strongly associated with active chronic gastritis, when polymorphonuclearleucocytes are present, and is not found on normal mucosa except when a biopsy specimen fromelsewhere in the stomach shows active chronic gastritis. When patients with symptoms caused bygastritis are identified dual antibacterial treatment, combining the action of bismuth in the stomachwith a systemic antibiotic, can eradicate C pyloridis, with remission of symptoms and restorationof normal epithelial morphology. Most peptic ulcers relapse after modern acid reducing treatment,and antibacterial treatment may be beneficial in preventing relapse.
Until a microbe is cultured and characterised, histo-pathological observation of the new organism in anunexpected site remains tantalisingly incomplete. Inpatients suffering from peptic ulceration there havebeen many reports of bacteria in association with thestomach mucosa,1 3 in contrast to transient bacteriafound above the mucus layer. In 1938 Doenges4reported "spirochaetes" in the stomach in necropsyspecimens, and Freedberg and Barron in 1940 found"spirochaetes" in 13 of 35 gastrectomy specimens.Steer in 19756 described bacteria closely related to thegastric mucosa under the mucus layer in associationwith gastritis but absent from the normal stomach.The bacteria were usually "apposed to the mucus-secreting cells," and there was "at least one filumprojecting from one end of the bacterium." Ultra-structural illustrations6 7 indicated that the bacteria
Accepted for publication 20 November 1985
were spiral, but Steer did not comment on this feature.He provided convincing evidence that these bacteriawere not contaminants introduced at the time ofbiopsy and emphasised that polymorphonuclear leu-cocytes migrate through the gastric mucosa, pre-sumably in response to the bacteria. Cultures of theseendoscopic biopsy specimens yielded Pseudomonasaeruginosa,7 but this is not a spiral organism and wasalmost certainly an irrelevant contaminant. In May1983 Steer submitted an article8 with scanning elec-tron microscopic pictures of curved and spiral bacte-ria in large numbers on the surface of gastric typeepithelial cells in the pre-pyloric area of the stomachand in areas of gastric metaplasia in the duodenalbulb, but the bacteria were not associated with thesurface of intestinal type epithelial cells. They werefound in 73% of patients with duodenal ulceration.
Since 1980 curved and spiral campylobacter likebacteria had been observed by Warren in endoscopicbiopsy specimens from patients with gastritis and pep-
353
on 23 March 2019 by guest. P
rotected by copyright.http://jcp.bm
j.com/
J Clin P
athol: first published as 10.1136/jcp.39.4.353 on 1 April 1986. D
ownloaded from
354tic ulceration at the Royal Perth Hospital in WesternAustralia; the bacteria stained well by the Warthin-Starry method9 but were difficult to see with the hae-matoxylin and eosin stain. Marshall and Warren ini-tiated a prospective study in 1982 that resulted in theculture from gastric antral biopsy specimens of micro-aerophilic campylobacter like organisms with asmooth coat and sheathed flagella arising from onepole ofeach organism.10 The first 34 biopsy specimenswere cultured on standard campylobacter media andnon-selective media for 48 hours without success. Thethirty fifth specimen was incubated during the Easterholiday and was examined after five days, when aheavy growth of campylobacter like bacteria wasobserved on the non-selective medium. Subsequentspecimens yielded these bacteria after three or fourdays of incubation but only on the non-selectivemedium; contaminants often covered the plates, sothat only 11 isolations were achieved, although thebacteria were often seen in the Gram stain." Thesespiral bacteria were named Campylobacterpyloridis, l and this name has now been validated.'2C pyloridis was detected histologically in a high pro-portion of the patients with gastritis and peptic ulcer;Marshall and Warren'3 presented cogent argumentsfor the probable clinical importance of C pyloridis inthe aetiology ofpeptic ulcers when not associated withmalignancy, or non-steroidal anti-inflammatorydrugs.A careful ultrastructural study of gastritis in 1979
by Fung et all4 included an illustration of curvedbacteria, which "abutted directly on to the plasma-lemma of the mucosal lining cells, but were never seenwithin the cell," and thus were thought not to beclinically important.
In September 1983 a retrospective histologicalstudy by Rollason et all' was accepted for publica-tion; 42% of endoscopic gastric biopsy specimensshowed spiral bacteria, undoubtedly associated withgastritis. Thus in 1982 in at least three separate labo-ratories in Southampton,8 Birmingham,'5 and Perth,Western Australia9 gastric spiral bacteria were beingvisualised, but only in Perth were the organisms cul-tured." C pyloridis has now been isolated frompatients with gastritis and peptic ulcer inEngland,'6 17 Holland,'8 Germany, United States ofAmerica, Canada, Japan, and Peru.'9
Unique features of C pyloridis
Campylobacter pyloridis is a fascinating microbe in itsown right. The true spiral bacteria, which includeCampylobacter, Spirillum, and Vibrio spp must be dis-tinguished from spirochaetes, which have endoflagellaor periplasmic fibres20: these spirochaetes also includethe human rectal spirochaete2' and an organism from
Goodwin, Armstrong, Marshall
the gut of rodents.22 Analyses of C pyloridis haveyielded a DNA base composition of guanosine pluscytosine 35-8-37 1 mol percent," which is within thecampylobacter range. In contrast to nearly all othercampylobacters, however, C pyloridis possesses apowerful urease enzyme preseat in largeamounts'1823 Urea is present in food such as milk,and this would result in the organism surroundingitself with a cloud of ammonia that would effectivelyinsulate it from the lethal effects of stomach acid. Cpyloridis also possesses large amounts of extracellularsuperoxide dismutase and catalase,24 which may con-fer resistance to the oxidative killing mechanisms ofphagocytes. C nitrofigilis2' and some aquaticcampylobacters26 possess a weak urease enzyme, andother campylobacters possess smaller amounts ofextracellular or intracellular catalase.24 C pyloridisshows strong phosphatase activity in the phenol-phthalein test, in which other campylobacters includ-ing "GCLO-2", an ordinary campylobacter isolatedrarely from the stomach, are negative27; the cellularfatty acid profile of GCLO-2 resembles that of Cjejuni,27 and it may be a related biotype of Cjejuni.28
Ultrastructural appearances and chemical analysesindicate that there are fundamental differencesbetween C pyloridis and other campylobacters.29 Cpyloridis has a smooth surface with four to six uni-polar flagella of sheathed type, each with a terminalbulb; it lacks the distinct pit like depression at eachpole from which the single flagellum of other cam-pylobacters arises.29 Typically, campylobacters havea rugose cell wall, with unsheathed flagella withoutterminal bulbs.30 Terminal bulbs have been seen onthe flagella of Vibrio cholerae,3' and it seems inap-propriate to designate these terminal structures as"paddles."
It is now accepted that the cellular fatty acid com-position of bacteria is important taxonomically.32 3The major cellular fatty acids of campylobacters arehexadecanoic (16:0), octadecenoic (18:1), and hexa-decenoic (16:1).34 In contrast, the major cellular fattyacids of C pyloridis are tetradecanoic (14:0) and cis-methylene octadecanoic (19:OA), with a very smallamount of hexadecanoic.29 Recently, the cis-methylene octadecanoic acid was shown to be cis- I1,12-methylene octadecanoic,35 correcting the originalerroneous report of cis-9,10-methylene octadecanoicacid.29 Respiratory quinones are also importantchemotaxonomic markers. C pyloridis lacks themethylated menaquinone-6,27 which is found in allother campylobacters.36 Evidence that a new bacte-rial genus has been discovered will have to await stud-ies of cistron similarities,37 and it is hoped that thesewill not be delayed too long.C pyloridis is very sensitive to most antibiotics; in
liquid medium the minimum inhibitory
on 23 March 2019 by guest. P
rotected by copyright.http://jcp.bm
j.com/
J Clin P
athol: first published as 10.1136/jcp.39.4.353 on 1 April 1986. D
ownloaded from

Campylobacter pyloridis, gastritis, and peptic ulceration
concentration90 of amoxycillin is 0 25 mg/I, of benzylpenicillin 0 5 mg/I, and of erythromycin 0-25 mg/I.38Cjejuni and Cfetus are 10 to 100 times more resistantto these antibiotics.3940Growth of C pyloridis in liquid media can be
enhanced in many ways. The addition of blood willresult in a heavy growth, but high counts can also beobtained in brain heart infusion broth plus 10% horseserum plus 0 25% yeast extract, provided that thedepth of liquid is shallow.38 Satisfactory growth canalso be obtained in nutrient broth with 5% serum and0-25% yeast extract in flat sided virus containers, orwith shaking.
C pyloridis in vivo
C pyloridis can be isolated readily from endoscopicspecimens of the gastric mucosa, but in a study of 103specimens its distribution was found to be patchy.41This observation has a direct bearing on the frequencywith which C pyloridis has been alleged to occur inpatients with duodenal ulcer. Evidence for a negativefinding can only be accepted if sufficient specimenshave been taken from different areas of the stomach,at least one from the antrum and one from the body.One specimen may not show C pyloridis when it is, infact, present elsewhere in the stomach. A satisfactorymedium for the isolation of C pyloridis is brain heartinfusion agar base (Oxoid) with 7% horse blood andIsoVitalex 1% (BBL Microbiology Systems), van-comycin 6 mg/I, nalidixic acid 20 mg/l, and ampho-tericin B 2 mg/l; the plates should be undried, but theycan be kept in a plastic container at room temperaturefor up to two weeks.4' Biopsy specimens can be keptin 0 5 ml 20% glucose at 4°C for at least five hourswithout loss of viability of C pyloridis.4"The importance of C pyloridis in the aetiology of
gastritis and peptic ulcer, and the consequent possiblevalue of antibacterial treatment in the resolution ofthese conditions remains highly controversial, at leastin the minds of gastroenterologists. Microbiologistsand histopathologists have been greatly impressed bythe close association of C pyloridis with activegastritis 1315-19; activity is indicated by the presenceof polymorphonuclear leucocytes. 13 42 C pyloridis isdetected very rarely on normal mucosa and again theimportance of taking at least one specimen from theantrum has been shown in a study of 150 patients withbiopsy specimens taken from both the body and theantrum of the stomach; when C pyloridis was foundon normal mucosa in the body the other specimenfrom the antrum always showed gastritis.43 Cpyloridis may not be detected due to poor techniqueby the gastroenterologist, the microbiologist, or thehistopathologist; Marshall44 warned that false nega-tive findings can result from lignocaine being swal-
355
lowed before endoscopy, simethicone being givenbefore biopsy, cimetidine in the stomach, which isslightly active against C pyloridis38; the patient mayhave taken bismuth preparations or antibiotic drugs,biopsy forceps may have been contaminated with glu-taraldehyde, or the biopsy specimen may contain noepithelium.44 If the specimen is kept at room tem-perature for more than three hours C pyloridis mayhave died; in the laboratory the plates may not befresh enough or may be too dry, and if primary iso-lation is attempted in a carbon dioxide incubator thehumidity must be greater than 98%.4l The histo-pathologist may be unable to detect C pyloridis if thespecimen contains mainly intestinal metaplasia oracid secreting mucosa, or if the Warthin-Starry stainis poorly prepared.44
In one Dutch study of "healthy" volunteers Cpyloridis was found in some of them, but in every oneof these the gastric mucosa showed gastritis while thevolunteers without gastritis did not have Cpyloridis.45
NON-ULCER DYSPEPSIANon-ulcer dyspepsia may be broadly defined as ulcerlike symptoms in the absence of an ulcer crater. Clin-icians seem unwilling to subdivide this group ofpatients into those with histological gastritis and thosewith a histologically normal mucosa. One reason fortheir reluctance may be the poor association betweenhistological gastritis and symptoms which may beconsidered important.46 Thus, although C pyloridis isassociated with histological gastritis and is rarelyfound in normal mucosa, it may still be difficult toprovide convincing evidence that C pyloridis is apathogen, because the organism may be found in peo-ple with apparently few symptoms but with histologi-cal gastritis; and it may be absent in people who com-plain ofdyspepsia but who have a normal mucosa. Oncareful questioning of patients, however, a remark-ably consistent pattern of symptoms can be detectedin patients subsequently found to have histologicalgastritis and C pyloridis. Apart from severeindigestion or abdominal pain, these symptoms aresternal, or epigastric burning or discomfort, reflux,burping, epigastric distension, periodic nausea,flatulence,47 and halitosis. Currently, there may belittle convincing evidence that gastritis gives rise to thesymptoms of the non-ulcer dyspepsia syndrome.48Although there is no proof that duodeno-gastric bilereflux causes non-ulcer dyspepsia,49 neither can pepticulcer be ascribed to such reflux.47 The importance ofstress in the aetiology of non-ulcer dyspepsia and pep-tic ulcer is also unclear; patients with non-ulcer dys-pepsia seem to suffer no more major life event trau-mas, such as a bereavement, than controls.50Cimetidine, which inhibits gastric acid secretion, has
on 23 March 2019 by guest. P
rotected by copyright.http://jcp.bm
j.com/
J Clin P
athol: first published as 10.1136/jcp.39.4.353 on 1 April 1986. D
ownloaded from

356
been found to be no better than placebo in relievingthe symptoms of non-ulcer dyspepsia"5; nor doestruncal vagotomy, which reduces acid output, relievethese symptoms.52Endoscopy is unreliable as a means of detecting
histologically florid gastritis."4 Its main value is todetermine whether a gastric or duodenal ulcer ispresent and to obtain several specimens for histologyand microbiological processing. It is to be hoped thatdefinitive studies of the importance of C pyloridis willrely on histological evidence of the presence orabsence of active gastritis in the body or the antrumof the stomach and not on endoscopic appearances.There are clear pathophysiological differencesbetween the gastritis that accompanies a chronic ero-sion, the lesion of pernicious anaemia, the chronicgastritis which is alleged to be associated withincreasing age, and the gastritis which is associatedwith peptic ulcer.5" Non-steroidal anti-inflammatorydrugs are notorious for causing haemorrhagic ero-sions, but these lesions are not necessarily associatedwith histological active chronic gastritis.
EPIDEMIC GASTRITIS WITH HYPOCHLORHYDRIAIn 1984 one of the authors (BJM) underwent an endo-scopy and a gastric biopsy, which showed normalmucosa without bacteria. One month later 109 colonyforming units of C pyloridis in alkaline peptone waterwere swallowed, and eight days later a transientachlorhydric gastritis was experienced.54 Symptomsincluded a brief episode of non-acidic vomiting, epi-gastric distension, malaise, and severe halitosis. Onthe tenth day biopsy specimens showed active chronicgastritis with polymorphonuclear cell inflammation inthe antrum, and large numbers of C pyloridis wereseen and cultured. Electronmicroscopy showed thatthe antral epithelial cells had lost their characteristicpattern of alignment and had developed irregularbulging surfaces with depletion of microvilli and asevere reduction in the numbers of cytoplasmic mucussecretory granules. On the fourteenth day anotherbiopsy specimen was taken; Cpyloridis was not found,polymorphonuclear cells were absent, and the ultra-structural changes had partially resolved. On the sameday treatment was started with tinidazole 500 mgtwice daily, and the symptoms resolved completelywithin 24 hours of the start of this treatment.A study in Texas in 1978 of 37 healthy volunteers
participating in a study of acid secretion was associ-ated with 17 volunteers becoming rapidly and pro-foundly hypochlorhydric: nine of these had a mildillness with epigastric pain several days before hypo-chlorhydria was detected. Gastric mucosal biopsyspecimens taken from subjects during the stage ofhypochlorhydria showed severe fundal and antral gas-
Goodwin, Armstrong, Marshalltritis.55 Retrospective analysis of the histologicalspecimens showed that the volunteers with gastritiswere infected with Cpyloridis (WL Peterson, personalcommunication). Acid secretion returned to baselinelevels in 14 of 17 subjects after a mean of 26 days, andthe severity of the gastritis diminished concurrently inseven of 10 subjects on whom biopsy was seriallyperformed. The pH electrode was not sterilisedbetween measurements, and gastric juice was returnedto the stomach after being tested. Thus it would bepossible for an infective agent to have been trans-mitted via a contaminated glass electrode. Similarly,in a Canadian study of gastric secretion four out of sixpreviously healthy subjects developed hypo-chlorhydria after a transient illness: nausea, vomiting,and abdominal pain were reported.56 No endoscopicabnormality was seen at one and eight months, butbiopsy specimens showed active superficial gastritis,which resolved in one subject and became chronic intwo. As in the previous study the pH electrode was notsterilised between measurements, and the gastric juicewas returned to the stomach, because this was consid-ered to be essential to avoid aspirating antacid, whichmight have resulted in loss of buffering effect. Again,analysis of the specimens suggested that in two sub-jects spiral bacteria were present in the biopsies. Inthis Canadian report there was a suggestion that thegastritis was a response to the presence of bacteriathat colonised the stomach which had previously hada high intragastric pH. Such an argument is refuted bythe Texas report55 in which the volunteers had a nor-mal stomach pH and then developed gastritis. In gen-eral, some authorities assert that the gastritis associ-ated with Cpyloridis occurs after cimetidine treatmenthas raised the intragastric pH. Many patients withpeptic ulcer, however, have high acid output and alsohave gastritis with C pyloridis, and so again the argu-ment is refuted by the facts.
Gastric and duodenal ulceration
The pathogenesis of gastric ulcer that shows malig-nant change is not clear. Gastritis may possibly pre-cede the malignant ulcer, so that chronicinflammation induced by C pyloridis may be animportant factor in the aetiology of such an ulcer.Apart from ulcers due to non-steroidal anti-inflammatory drugs, gastric acid seems to be the mainprecipitating cause of gastric and duodenal ulcers.When acid secretion is reduced by drugs that act as H2receptor antagonists-namely, cimetidine and ran-itidine,57 or proton pump inhibitors such asomeprazole58-healing of the ulcer can be observedby endoscopy. When tissue is taken from healed duo-denal ulcers, however, most show evidence of mod-erate to severe inflammation and gastric epithelial
on 23 March 2019 by guest. P
rotected by copyright.http://jcp.bm
j.com/
J Clin P
athol: first published as 10.1136/jcp.39.4.353 on 1 April 1986. D
ownloaded from

Campylobacter pyloridis, gastritis, and peptic ukerationmetaplasia at or adjacent to the site of the ulcer.59Whitehead stated that "ulcer and gastritis are invari-ably present in the same stomach"53; the gastritisalways affects the antrum in prepyloric ulcers andextends to a larger area in body ulcers.60 There issome evidence that high gastric ulcers are always asso-ciated with gastritis in the area of stomach distal to theulcer.6' Active chronic gastritis can be one cause ofgastric ulcer,62 and gastric ulcers commonly occur ininflamed antral type mucosa.63The frequency with which C pyloridis has been
found in patients with duodenal ulceration has varied;even when tissue was taken only from the gastricantrum, 95% of 61 patients were found to have theorganism.64 In 16 patients additional specimens weretaken from the duodenum, stomach, and oesophagus;C pyloridis was identified in the duodenal mucosaproximal to the ulcer within the stomach but not in theoesophagus. Ninety four per cent of the patients withpeptic ulcer also had associated gastritis.64 The skill ofthe endoscopist in choosing correct areas to biopsyand the strictness with which a peptic ulcer is definedcould influence the final percentage of patients withulcers found to have C pyloridis. In one small study inHolland all 15 patients with duodenal ulcer and nineof 10 patients with gastric ulcer were found to have theorganism.45 In another study in which only two speci-mens were taken for histology, but not all specimenswere cultured, seven of 70 patients with duodenalulcer did not have C pyloridis, neither did 13 of the 40patients with gastric ulcer.44
Until the importance of gastritis in the pathogenesisof gastric and duodenal ulcers is clearly established,the exact place for antibacterial treatment will remainunresolved.65
Is C pyloridis a commensal, an opportunist, or aprimary pathogen?
Firstly, it should be determined whether C pyloridis isassociated with a specific lesion which can be detectedultrastructurally, and, secondly, whether or not thislesion occurs in the absence of the organism. Specificserum antibodies should be detected in patients fromwhom Cpyloridis can be cultured, and IgA antibodiesshould be found in the gastric juice of patients. Theseantibodies should be less common and at a lower titrein patients without the organism. Specific anti-bacterial treatment directed against Cpyloridis shouldalso reverse the specific lesions and relieve the symp-toms of infected patients.
Ultrastructural features of infection with C pyloridisand their reversal after treatment with antibiotics
Ultrastructural studies of antral tissue have been per-
357
formed in the Royal Perth Hospital since 1982.12Invariably, the presence of C pyloridis has been asso-ciated with a specific lesion in which C pyloridis isintimately associated with the gastric mucosa.65 Sucha lesion was found in a 64 year old woman with ahistory of "nervous dyspepsia," which had started atthe age of 18; she did not have a peptic ulcer (Fig. 1).This woman's father had also suffered from life longdyspepsia and two of three brothers had a confirmedduodenal ulcer. Her symptoms included burning epi-gastric pain after meals associated with acid reflux, afeeling of distension in the stomach after meals, noc-turnal pain with burning and nausea, and episodes ofcolic. (Interestingly, the feeling of distension could bedue to the fact that C pyloridis produces powerfulenzymes, possibly resulting in the liberation ofcarbondioxide. A controlled study of patients with duodenalulcer showed increased partial pressures of carbondioxide in the duodenum of patients after meals.66)
She underwent endoscopy, and culture of the antraltissue yielded C pyloridis. Although macroscopicallythe stomach mucosa seemed to be normal, histologyshowed the presence of severe active chronic gastritis.The patient was given tri-potassium di-citrato bis-muthate (DeNol), one tablet to be chewed an hourbefore meals and at night time: this is the same doseas is used for the treatment of duodenal ulcer. Ater 14days she was able to stop taking the antacid medica-tion and felt well. Endoscopy and biopsy wererepeated after four and eight weeks of treatment, andC pyloridis was not detected in either of the biopsyspecimens. Treatment with DeNol was then stopped,but three weeks later she again developed symptoms.At endoscopy the stomach and duodenum were againnormal, but the biopsy specimen showed activechronic gastritis and Cpyloridis. The patient was thengiven 28 days of treatment with DeNol supplementedwith amoxycillin 500 mg thrice daily from the seventhto the 28th day. Her symptoms resolved in three days.One month and six months after completing the sec-ond course of treatment biopsy was performed whichshowed a histologically normal mucosa; C pyloridiscould not be cultured. She has remained well for twoyears, has been able to eat any type of food, and hasrarely used antacids.
For the ultrastructural studies on the patient speci-mens were processed in a manner already described.29Thin sections of the antral biopsy specimen beforetreatment with bismuth was started showed consid-erable abnormalities of the mucosal ultrastructure(Fig. 1). Most notably, the flattened luminal surfacesof normal mucus secreting epithelial cells werereplaced by an irregular pattern due to dome likebulging or ragged flap like protrusion of the individ-ual epithelial cells. Partial to complete loss of surfacemicrovilli was also evident. Intracellular mucin gran-
on 23 March 2019 by guest. P
rotected by copyright.http://jcp.bm
j.com/
J Clin P
athol: first published as 10.1136/jcp.39.4.353 on 1 April 1986. D
ownloaded from

Goodwin, Armstrong, Marshall
.,
.. .. .s
ig $.: 4 >
iS .:
.. s ,'i rt:e' :: :' . :'
_ .> :.
^ ..N i::
,.; t:. ,.:f 1 ' S:snggs; ga ..... ,
*: .*vb w l\:.^
*:
.:
t£:X ;' :4fs
xe; jf4::.
.. ... .. : }! :::@ ¢@lE .. 5so
...:% .:
0'
,...*.
* ; '.s:,
.. -Kx
Fig. 1 Luminal surface of antral epithelium before treatment. Clusters of Campylobacter pyloridis lie close tobulging membranes of mucus secretory cells. Note retention of microvilli in isolated bacteria free pocket (*). M =mucin eranules (Electron microscopy.) x 5750.
t~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~.,,..~t
Mt:::t
4",..W:.,M% 4,.
-"
Are
"t, !PI-V.--71--.-,!.- .1fv.1. "'Ilv.4,S$4.-- ..
Fig. 2 Higher magnification shows intimate adherence between Campylobacter pyloridis and antral cell membrane(arrows). Cellular cytoskeleton (CS) shows random orientation. Sheathedflagellar profiles (F) and sectioned termi-nal bulb (B) are present. (Electron microscopy.) x 110000.
358
At
:.f,. za...S, .%-r-
on 23 March 2019 by guest. P
rotected by copyright.http://jcp.bm
j.com/
J Clin P
athol: first published as 10.1136/jcp.39.4.353 on 1 April 1986. D
ownloaded from
Campylobacter pyloridis, gastritis, and peptic ulceration 359
4,4~~~~~~~~~~~~~~~~~~~4
N1
~~~~~~~~~~~~~~~~~~'~~~~ ~ ~ ~ ~ ~ ~ ~ ~ ~~~Ar* ~~~~~~~Amet'~~~~~~~~~~~~~~~~~~~~~~~~~*S *~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~eIf~~~~
FW AF~~~~~~~~~4 ~~~~~, Pt 1'~~~~~~~jF-~~ ~ ~ ~ ~ ~ W
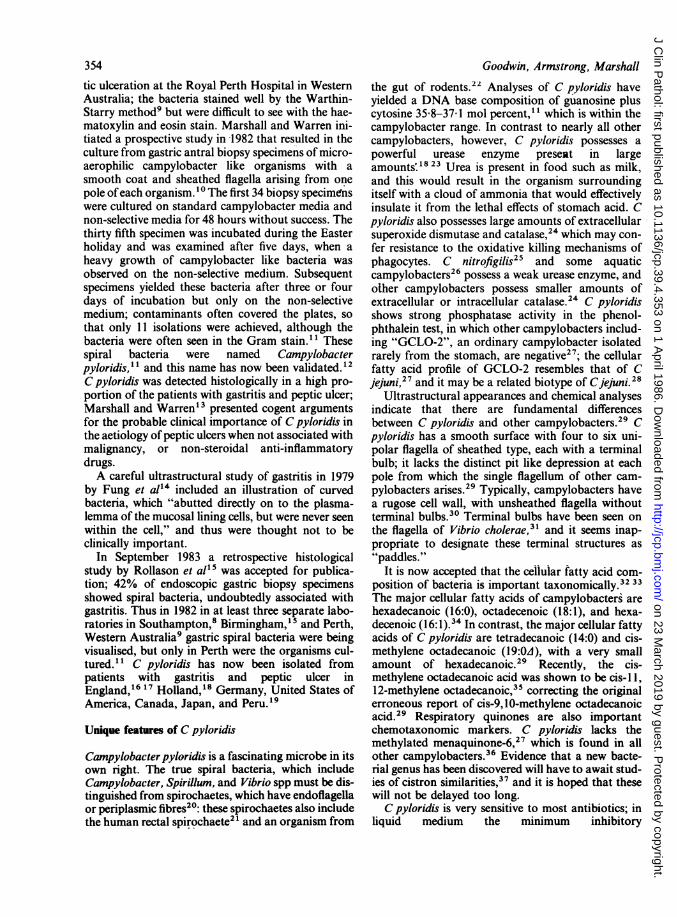
Fig. 3 Restored normal appearance of antral epithelium after four weeks of treatment with bismuth. (Electronmicroscopy.) x 2750.
4.~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~.
It~ ~ ~ ~ I
S A
j'4j
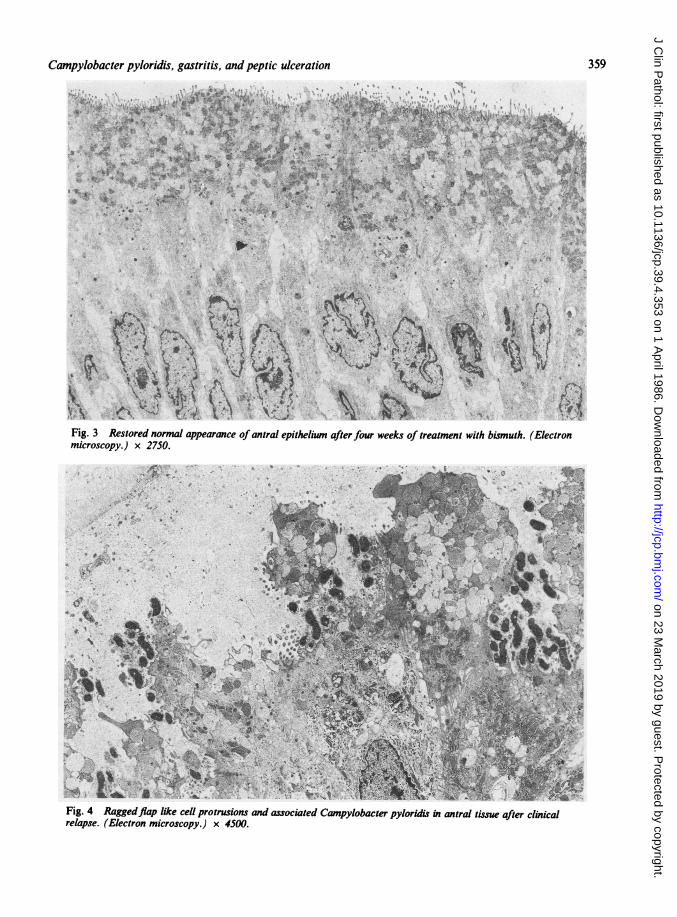
Fig. 4 Raggedflap like cell protrusions and associated Campylobacter pyloridis in antral tissue after clinicalrelapse. (Electron microscopy.) x 4500.
on 23 March 2019 by guest. P
rotected by copyright.http://jcp.bm
j.com/
J Clin P
athol: first published as 10.1136/jcp.39.4.353 on 1 April 1986. D
ownloaded from

Goodwin, Armstrong, Marshall
Fig. 5 Detail from antral speciment of normal appearance four months after completion of combined treatment.Restored microvilli have filamentous cores (arrows) entering cytoskeletal web. (Electron microscopy.) x 4S 000.
ules were depleted and often confined to apical cyto-plasmic protrusions. Intracellular oedema was promi-nent, but essential continuity of the epithelium waspreserved through junctional complexes bordering thelumen and attachment to an intact underlying basallamina. Superficial neck cells of the gastric pits weresimilarly affected, but the tubular glands themselvesseemed to be normal. A sparse infiltrate of neutrophilpolymorphs and lymphocytes was present in the lam-ina propria, and occasional neutrophils had crossedthe basal lamina to penetrate between the epithelialcells while others lay free on the luminal surface.
Large numbers of curved rod like or spiral bacteriaup to 3 pm in length and about 0 5 pm in width, weredistributed singly or in clusters over the luminal sur-face of the epithelium, including the gastric pits. Thebacteria had multiple unipolar sheathed flagella,which is characteristic of C pyloridis. They werelocated deep to the layer of gastric mucus and close tothe smooth bulging plasma membranes of the antralepithelial cells, often interspersed with remnants ofdetached microvilli. The bacteria seemed to be wellpreserved, and so presumably viable, and includeddividing forms; no preferential orientation withrespect to the epithelium was apparent; some lay endon and others lengthwise to the cell membranes.Where bacteria were numerous, cellular microvilli
were generally absent or much depleted, and points ofintimate membranous adhesion (adherence pedestals)between the outer bacterial cell wall and distinctiveconcavities of the epithelial surface were clearly visible(Fig. 2). There was local "thickening" of the cell mem-brane in the area of the adherence pedestal. No partic-ular parts of the bacteria seemed to be participatingmore fully than others in such points of adherence.High magnification showed loss of microvilli, alongwith the organised central cores of microfilaments,which normally contribute to the cytoskeleton of theapical cytoplasm. A few isolated pockets of epi-thelium, which were free of bacteria had retained theirsurface microvilli (Fig. 1). No profiles were found tosuggest bacterial intracellular penetration, orattempts by epithelial cells at phagocytic ingestion ofthe organisms; but occasional C pyloridis had beeningested by neutrophils, and such organisms appeareddegraded and non-viable. A small island of epithelialmetaplasia was found within the biopsy specimen, inwhich mucus secreting antral cells had been replacedby columnar intestinal type cells bearing a definitivebrush border. Here infestation with C pyloridisstopped, only to reappear on the far side of the meta-plastic zone; the columnar cells showed no surfacemembrane changes like those of adjacent antralmucus cells. It seems that the organisms have a predi-
360
on 23 March 2019 by guest. P
rotected by copyright.http://jcp.bm
j.com/
J Clin P
athol: first published as 10.1136/jcp.39.4.353 on 1 April 1986. D
ownloaded from

Campylobacter pyloridis, gastritis, and peptic ulceration
lection for adherence to typical mucus secreting antralepithelium.
After treatment with bismuth tablets alone theantral tissue (Fig. 3) showed an essentially normalmucosa without any spiral bacteria. Notable detailswere even alignment and general flattening of theluminal surfaces, restoration of short microvilli, and aconsiderable increase in the number ofmucin granulesin the supranuclear cytoplasm. The specimenobtained after clinical relapse showed reversal of thereparative process, with return of severe epithelialbulging or flap like protrusion and depletion of micro-villi; spiral bacteria were again present in profusion(Fig. 4). In contrast, the final specimen taken fourmonths after treatment with bismuth tablets and oralamoxycillin once again showed a normal well alignedepithelium, without any spiral bacteria. Microvilliwere fully developed for the antral cell type, eachexhibiting a prominent core of microfilaments reach-ing down into the submembranous cytoskeletal web(Fig. 5).
These ultrastructural studies of sequential speci-mens illustrate the specific lesion of C pyloridis andshow that when the bacteria were eliminated themucosa returned to normal. The pathological changesoccurred both in the initial biopsy specimen beforetreatment and after clinical relapse following inade-quate monotherapy. After completion of each treat-ment schedule there was a reversion to normal epi-thelial cell alignment and disappearance of theorganisms. These observations clearly favour a cyto-pathogenic role for C pyloridis, with mucus secretingcells as the preferential target. An identical lesion wasseen in the mucosa of a volunteer who swallowed Cpyloridis,S4 and in all our other gastric biopsies thislesion was seen only in association with C pyloridis.As C pyloridis affects gastric mucosal cells it is not
surprising that the mucus content of the mucosal cellsis greatly reduced. It can be envisaged that with amuch reduced layer of mucus the mucosal cells mightbe more susceptible to gastric acid, possibly resultingin an ulcer. Numerous compounds such as alcohol,bile salts, and salicylates directly damage the stomach:these substances increase the permeability of themucus barrier, allowing diffusion of acid into themucosa with subsequent development of hae-morrhage and mucosal erosion.6768 Whether thesecompounds pave the way for infection with Cpyloridis or whether they further weaken the mucosalprotection after C pyloridis has caused gastritis andallow an ulcer to form is not yet clear. The layer ofgastric mucus in the stomach almost certainly has amajor role in protecting gastric epithelium from gas-tric acid.69 The depth of mucus gel is an importantconsideration in terms of mucosal protection, becausebelow a minimum depth luminal acid entering the gel
will overwhelm the bicarbonate secreted by themucosa. 9 It is of great interest that C pyloridis main-tains its motility in highly viscous material such asmethyl cellullose, in which Escherichia coli becomesimmobile.70
SIMILARITY BETWEEN LESIONS CAUSED BY CPYLORIDIS AND THOSE CAUSED BYENTEROPATHOGENIC ESCHERICHIA COLIEnterotoxigenic E coli produce toxins, and otherstrains of E coli invade the mucosa. The pathogenesisof disease caused by enteropathogenic E coli, how-ever, was obscure until Cantey and Blake7" describeda strain of E coli (RDEC-1) in 1977, which reliablyproduced diarrhoea in rabbits without producing tox-ins or invading the mucosa. Subsequently, a few iso-lates of enteropathogenic E coli (EPEC) were shownto produce a small amount of shiga enterotoxin.72Ultrastructural studies ofE coli 015 (RDEC-1) infec-tion in rabbits have shown specific lesions associatedwith the close adherence of the bacteria to the mucosaof the ileum, caecum, and colon. The microvilli aredestroyed and disappear, and the bacteria rest onextrusions of epithelial cell plasma membrane, whichcan be seen to cup the bacteria, and which have beentermed "adherence pedestals."73 - 75 Although thebacteria do not invade cells, degenerative changes areseen in cells with many adherent bacteria. An identicalultrastructural lesion has been observed in a rectalbiopsy specimen from an infant with diarrhoea associ-ated with E coli 0119.76 Similar adherence pedestalsand ultrastructural changes have been reported ingnotobiotic piglets with enteritis due to EPEC77;polymorphonuclear leucocytes, plasma cells, andmacrophages had infiltrated the mucosa and sub-mucosa. Another organism that produces a similarlesion, and probably associated diarrhoea, isCryptosporidium.72Our ultrastructural studies of C pyloridis here and
elsewhere1 2 have shown a similar picture, with adher-ence of C pyloridis to the mucosa, depletion of micro-villi, disruption of submembranous cytoskeletal sup-porting microfilaments, and the development ofadherence pedestals. The selectivity of the bacterialattachment is shown by sparing of metaplastic intes-tinal type columnar epithelium surrounded byaffected antral mucus secretory cells. There was noevidence of epithelial cytolysis or intracellular para-sitism. Mechanisms underlying the cytopathic effectshave yet to be determined.
This ultrastructural evidence militates against thehypothesis that Cpyloridis is associated with gastritismerely by colonising the mucosa after inflammationhas occurred. The presence and precise location of Cpyloridis in intimate relation to antral epitheliumshowing obvious changes, both at an initial case
361
on 23 March 2019 by guest. P
rotected by copyright.http://jcp.bm
j.com/
J Clin P
athol: first published as 10.1136/jcp.39.4.353 on 1 April 1986. D
ownloaded from

362
presentation and after clinical relapse, together withthe reversion to epithelial normality and disap-pearance of organisms after completion of each treat-ment schedule, are findings that clearly favour apathogenic role for this organism. The return ofinflammation and bacteria after monotherapy withDeNol would indicate that not all the organisms wereeliminated. Support is given to this conclusion by areport from Holland, in which three patients whorelapsed after monotherapy with DeNol or an anti-biotic were subjected to endoscopic biopsies, and Cpyloridis was cultured after relapse. The strains wereanalysed by Hind III restriction endonuclease anal-ysis. Each strain produced a different profile from theother strain, but the isolate obtained after relapse wasidentical with the isolate obtained before treatment.78This indicated relapse rather than reinfection. In ourpatient treated concurrently with DeNol and a sys-temic antibiotic, however, the organism seems to havebeen completely eradicated and the patient hasremained well for two years.
Immune responses to Campylobacter pyloridis
Methods of measuring antibodies to C pyloridis havevaried considerably. Complement fixation titres arehigher in patients with gastritis than in patients with-out gastritis, in blood donors, and in antenatalpatients. 17 A passive haemagglutination test has beendescribed briefly.79 Using this method 20% (216) ofblood donors were found to have antibody to Cpyloridis and these donors had more abdominal symp-toms than the antibody negative donors. Passive hae-magglutination, however, is not an easily standard-ised test and other workers have not found the testreliable (J Eldridge, personal communication).Enzyme linked immunosorbent assay (ELISA) is awell established method, but in some brief publishedreports the antigen used was a sonicate of Cpyloridis,80 or organisms killed by whole formalin.43In a study conducted in Melbourne it was reportedthat IgG antibody to C pyloridis was lower in"healthy" people than in patients with peptic ulcer.80In that study, however, histological data were notreported, and commenting on it Rathbone et a143emphasised that C pyloridis correlated very stronglywith gastritis, but the relation of C pyloridis to pepticulcer was probably due to coexistent antral gastritis.Thus the Melbourne study reported relatively highantibody titres in a few children but no histologicaldata on these patients. Rathbone et a143 reported con-siderably raised IgG and IgA serum antibody titres inpatients from whom Cpyloridis was cultured, but IgMtitres were similar in groups positive or negative forthe bacteria. They also detected IgA antibody againstC pyloridis in the gastric juice of most colonised
Goodwin, Armstrong, Marshall
patients, which was undetectable in normal subjects.If IgA antibody is not present in other transudatessuch as saliva then the local antibody response in thestomach would provide further evidence for a patho-genic role of the organism in chronic gastritis.
In the case of C jejuni ELISA results in infectedpatients were most reliable when an acid-glycineextract of the organism was used.8" Such an antigenis difficult to prepare for C pyloridis but is now inroutine use at the Royal Perth Hospital; in bacterianegative patients very low titres of polyclonal anti-body are found, but in most bacteria positive patientshigh titres are present (authors' personal obser-vations).
Antibacterial treatment directed against C pyloridis
Although peptic ulcers are readily healed with acidreducing drugs, after such treatment is stopped therate of relapse may reach 100% in patients followedup for two years.82 Marshall et al44 showed thatC pyloridis could be found in inflamed mucosa adja-cent to a duodenal ulcer and they presented con-vincing arguments for the clinical importance ofC pyloridis in gastritis and peptic ulceration notcaused by non-steroidal anti-inflammatory drugs. Astudy by McClean et al83 of the reports of ulcerrelapse following different treatments showed thattreatment with cimetidine produced higher rates ofrelapse than treatment with tri-potassium di-citratobismuthate, or other "mucosal-protection agents".They also suggested84 that cimetidine may promoteulcer relapse by raising intragastric pH to provide anideal growth environment for bacteria.The response of our patient (Figs. 1-4) showed that
bismuth is antibacterial to C pyloridis but inadequateon its own to eradicate the organism. Treatment withamoxycillin alone is also usually followed by relapseand reappearance of the organism.78 This is not sur-prising, considering the sequestered niche whereC pyloridis is found, below the mucus layer but abovethe gastric mucosa. By using combination treatment,however, similar to that described above, Marshall85was able to eradicate the bacterium in 15 of 17patients with duodenal ulcer as assessed by repeatbiopsy one month after treatment had been stopped.Thus treatment with both bismuth and a systemicantibiotic may be required to eradicate the organism.At present the optimum length of treatment is notknown, nor whether C pyloridis can developresistance to an antibacterial drug during treatment.Controlled trials showing healing of the ulcer withantibiotics have already been reported; met-ronidazole, which was active against 80% of isolatesof C pyloridis in Perth47 has been reported to healpeptic ulcers,86 as has furazolidone.87 88
on 23 March 2019 by guest. P
rotected by copyright.http://jcp.bm
j.com/
J Clin P
athol: first published as 10.1136/jcp.39.4.353 on 1 April 1986. D
ownloaded from
Campylobacter pyloridis, gastritis, and peptic ulceration
Until the natural history of gastritis and its relationto peptic ulceration is fully understood, it will beimpossible to plan the most rational treatment.65Conventional treatment regimens, which concentrateonly on the immediate healing of a macroscopic ulcercrater, are clearly defective if they do not cure thedisease, in addition to which they must be continuedindefinitely. It is also illogical to confine treatmentthat relieves ulcer type symptoms to patients withulcer craters. Many patients without an ulcer haveidentical symptoms associated with an identical histo-logical lesion (active chronic gastritis), affecting largeareas of their gastroduodenal mucosa. These patientsmust be more carefully studied and their symptomsevaluated as part of the spectrum of ulcer disease.Antibacterial treatment of all symptomatic patientswith confirmed C pyloridis infection and patients witha high titre of antibodies to the organism must becarefully evaluated.
Future developments
C pyloridis has not been cultured from any organother than the stomach in man, nor from the environ-ment, and such studies will be eagerly awaited. Salivafrom 33 patients with gastritis did not yieldC pyloridis (authors' personal observations).C pyloridis is a fascinating new spiral organism thatwill be studied for its own sake. Already several of itsfeatures have been found to be unique-its cellularfatty acids, ultrastructure, and enzyme qualities. Astudy of cistron similarities should be made to deter-mine whether it should remain in the genus Cam-pylobacter, or be the first member of a new genus. Theimportance ofC pyloridis as a human pathogen, how-ever, will need to be proved in great detail to satisfygastroenterologists. We hope that the importance of ahistological diagnosis rather than the macroscopicappearance at endoscopy will be accepted as a basison which to assess the pathogenicity ofC pyloridis. Asthe pathogenic mechanisms of enteropathogenic Ecoli are more fully delineated they may indicate whichavenues should be studied for C pyloridis, which hasan identical method of mucosal adherence to that ofEPEC. Serological tests of patients and controls mustbe undertaken with a clearly defined antigen and fullassessment of all factors, which might show that asupposed control was, in fact, a patient. The role ofantibacterial medicine in the long term treatment ofpeptic ulceration and gastritis will require doubleblind placebo controlled prospective trials, which areno doubt already being undertaken around the world.C pyloridis could be described as "a galactic intruderinto gastroenterology". If and when it is finallyaccepted as a pathogen by practising clinicians andsurgeons then no doubt more microbiology laborato-
363
ries will be required to isolate this organism fromgastric biopsy specimens and perhaps other sources,and advice on antibacterial treatment will be sought.Immunoblot techniques may show the importance ofdifferent antigens in patients and healthy contacts,and those antigens which would be candidates for avaccine may be delineated. C pyloridis is to beadmired for its parasitism of a unique niche, where it"4grazes" on the microvilli of cells which have thecapacity for rapid regeneration, thus providing newpasture: because the underlying cells are not invadedthe host will continue to live. Possibly, our modernstressful civilisation induces people to develop pepticulceration, from which a few of the hosts do perish.Modern medicine has been kind to C pyloridis, how-ever, in that the current antacids such as cimetidineand ranitidine alleviate the most serious symptomsand concomitantly make the stomach a more pleasantplace in which C pyloridis can multiply.
Within the symptom complex of gastritis and pepticulceration more study must be given to the cause ofsymptoms. Thus some duodenal ulcers give rise tovery few symptoms until an episode of bleedingoccurs. After acid reducing treatment duodenal ulcerscan reappear without symptoms. Are the symptoms ofpeptic ulcer due to the ulcer itself or to concomitantgastritis? Patients with asymptomatic but bleedingulcers may have less gastritis than patients with ahighly inflamed gastric antrum but no duodenal ulcer.
Studies of acute transient gastritis should include anattempt to detect the presence ofC pyloridis by biopsyor brushing of the gastric mucosa. Osler describedsuch a condition89 54 and we have referred to twosmall outbreaks.55 56 Possibly, acute achlorhydricgastritis may be an unrecognised common minor ill-ness, but if it leads to the more serious disorders asso-ciated with chronic gastritis then detailed examinationof vomit from such cases, and even gastric biopsy willbe warranted.The presence of C pyloridis infection in apparently
healthy subjects will continue to be problematical forthose who maintain that the bacterium is a pathogen.Like most other chronic infections, however, such astuberculosis, the success of C pyloridis as a pathogenmay be partly due to the fact that it often induces arelatively asymptomatic but nontheless infectious car-rier state.
We acknowledge the gastroenterological help of DrsTom Waters and Chris Sanderson and the histologicalexpertise of Dr R Warren. We thank Mrs Faye Cov-erley for indefatigable secretarial help and Mr SHWee and Mrs Elizabeth Blincow for expert technicalhelp. We acknowledge the financial support of theNational Health and Medical Research Council andthe Royal Perth Hospital Research Foundation. As
on 23 March 2019 by guest. P
rotected by copyright.http://jcp.bm
j.com/
J Clin P
athol: first published as 10.1136/jcp.39.4.353 on 1 April 1986. D
ownloaded from

364
research on C pyloridis is at an early stage some refer-ences are to letters, journals, and abstracts. In severalcases, however, we have seen submitted manuscriptsthat give full details of the studies, and we thank thoseauthors.
References
1 Bottcher. Dorpater Medicinische Zeitschrift 1874;5:148.2Rosenow EC, Sandford AH. The bacteriology of ulcer of the stom-
ach and duodenum in man. J Infect Dis 1915;17:210-26.3Applemans R, Vassiliadis P. Etude sur la flore microbienne des
ulcers gastro-duodeneaux et des cancers gastriques. Revue Beigedes Sciences Medicales 1932;4:198-203.
4Doenges JL. Spirochaetes in the gastric glands of Macacus rhesusand humans without definite history of related disease. Proc SocExp Med Biol 1938;38:536-8.
sFreedburg AS, Barron LE. The presence of spirochaetes in humangastric mucosa. American Journal of Digestive Diseases1940;7:443-5.
6Steer HW. Ultrastructure of cell migration through the gastricepithelium and its relationship to bacteria. J Clin Pathol1975;28:639-46.
7 Steer HW, Colin-Jones DG. Mucosal changes in gastric ulcerationand their response to carbenoxolone sodium. Gut 1975;16:590-7.
'Steer HW. Surface morphology of the gastroduodenal mucosa induodenal ulceration. Gut 1984;25:1203-10.
9Warren JR. Unidentified curved bacilli on gastric epithelium inactive chronic gastritis. Lancet 1983;i:1273.
Marshall BJ. Unidentified curved bacilli on gastric epithelium inactive chronic gastritis. Lancet 1983;i: 1273-5.
" Marshall BJ, Royce H, Annear DI, et al. Original isolation ofCampylobacter pyloridis from human gastric mucosa. MicrobiosLetters 1984;25:83-8.
12Anonymous. Validation of publication of new names and newcombinations previously effectively published outside the IJSB.Int J Syst Bacteriol 1985;85:223-5.
13 Marshall BJ, Warren JR. Unidentified curved bacilli in the stom-ach of patients with gastritis and peptic ulceration. Lancet1984;i:131 1-4.
4Fung WP, Papadimitriou JM, Matz LR. Endoscopic, histologicaland ultrastructural correlations in chronic gastritis. Am J Gastro-enterol 1979;71:269-79.
5Rollason TP, Stone J, Rhodes JM. Spiral organisms in endoscopicbiopsies of the human stomach. J Clin Pathol 1984;37:23-6.
McNulty CAM, Watson DM. Spiral bacteria of the gastricantrum. Lancet 1984;i:1068-9.
17 Jones DM, Lessells AM, Eldridge J. Campylobacter like organismson the gastric mucosa: culture, histological, and serological stud-ies. J Clin Pathol 1984;37:1002-6.
18Langenberg ML, Tytgat GNJ, Schipper MEI, Rietra PJGM,Zanen HC. Campylobacter like organisms in the stomach ofpatients and healthy individuals. Lancet 1984;i: 1348.
Pearson AD, Skirrow MB, Lior H, Rowe B, eds. Campylobacter IIIProceedings ofthe third international workshop on Campylobacterinfections. London: Public Health Laboratory Service,1985:158-194.
20Hovind-Hougen K. Determination by means of electron micro-scopy of morphological criteria of value for classifications ofsome spirochaetes, in particular treponemes. Acta Pathol Micro-biol Scand 1976;255:20-2.
21 Hovind-Hougen K, Birch-Andersen A, Henrik-Nielsen R, et al.Intestinal spirochetosis: morphological characterization and cul-tivation of the spirochaete Brachyspira aalborgi gen. nov. sp.nov. J Clin Microbiol 1982;16:1127-36.
22 Phillips MW, Lee A. Isolation and characterization of a spiralbacterium from the crypts of rodent gastrointestinal tX4s. ApplEnviron Microbiol 1983;45:675-83.
Goodwin, Armstrong, Marshall
23Owen RJ, Martin SR, Borman P. Rapid urea hydrolysis by gastriccampylobacters. Lancet 1985;i: 11.
24Lior H, Johnson WN. Catalase, peroxidase and superoxide dis-mutase activities in campylobacter spp. In: Pearson AD, SkirrowMB, Lior H, Rowe E, eds. Campylobacter III: proceedings ofthethird international workshop on Campylobacter infections. Lon-don: Public Health Laboratory Service, 1985:226-7.
2SMcClung CR, Patriquin DG, Davis RE. Campylobacternitrofigilis sp. nov., a nitrogen-fixing bacterium associated withroots of Spartina altemiflora Loisel. Int J Syst Bacteriol1983;33:605-12.
26Bolton FJ, Holt AV, Hutchinson DN. Urease-positive thermo-philic campylobacters. Lancet 1985;i:1217-8.
"Goodwin S, Blincow E, Armstrong J, McCulloch R, Collins D.Campylobacter pyloridis is unique: GCLO-2 is an ordinary cam-pylobacter. Lancet 1985;ii:38-9.
Steele TW, Lanser JA, Sangster N. Nitrate-negativecampylobacter-like organisms. Lancet 1985;i:394.
Goodwin CS, McCulloch RK, Armstrong JA, Wee SH. Unusualcellular fatty acids and distinctive ultrastructure in a new spiralbacterium (Campylobacter pyloridis) from the human gastricmucosa. J Med Microbiol 1985;19:257-67.
30Pead PJ. Electron microscopy of Campylobacter jejuni. J MedMicrobiol 1979;12:383-5.
31 Rowles CR, Parton R, Jeynes MH. Some aspects of the cell wallsof Vibrio spp. In: Fuller R, Lovelock DW, eds. Microbial ultra-structure. London: Academic Press, 1976;109-15.
32Lechevalier MP. Lipids in bacterial taxonomy-a taxonomist'sview. CRC Critic Rev Microbiol 1977;5:109-210.
33Lambert MA, Huckman-Brenner FW, Farmer JJ, Moss CW.Differentiation of Vibrionaceae species by their cellular fattyacid composition. Int J Syst Bacteriol 1983;33:777-91.
34 Curtis MA. Cellular fatty acid profiles ofcampylobacters. MedLabSci 1983;40:333-48.
3S Hudson MJ, Wait R. Cellular fatty acids of Campylobacter specieswith particular reference to Campylobacter pyloridis. In: Pear-son AD, Skirrow MB, Lior H, Rowe B, eds. Campylobacter III:third internafuonal workshop on Campylobacter infections. Lon-don: Public Health Laboratory Service, 1985:198-9.
36 Collins MD, Costas M, Owen RJ. Isoprenoid quinone compositionof representatives of the genus Campylobacter. Arch Microbiol1984;137:168-70.
37Gillis M, De Ley J. Intra- and intergeneric similarities of the ribo-somal ribonucleic acid cistrons of Acetobacter and Glu-conobacter. Int J Syst Bacteriol 1980;30:7-27.
38 Goodwin CS, Blake P, Blincow E. The minimum inhibitory andbactericidal concentrations of antibiotics and anti-ulcer agentsagainst Campylobacter pyloridis. J Antimicrob Chemother (inpress).
39Shanker S, Sorrell TC. Susceptibility of Campylobacter jejuni totwenty-three antimicrobial agents. Pathology 1983;15:61-3.
40 Chow AQ, Patten V, Bednorz D. Susceptibility of Campylobacterfetus to twenty-two antimicrobial agents. Antimicrob AgentsChemother 1978;13:416-8.
41 Goodwin CS, Blincow ED, Warren JR, Waters TE, Sanderson CR,Easton L. Evaluation of cultural techniques for isolating Cam-pylobacter pyloridis from endoscopic biopsies of gastric mucosa.J Clin Pathol 1985;38:1127-31.
42 Whitehead R, Truelove SC, Gear MWL. The histological diagnosisof chronic gastritis in fibreoptic gastroscope biopsy specimens. JClin Pathol 1972;25:1-l1.
43 Rathbone BJ, Wyatt JL, Worsley BW, Trejdosiewicz LK, HeatleyRV, Losowsky MS. Immune response to Campylobacterpyloridis. Lancet 1985;i:1217.
"Marshall BJ, McGechie DB, Rogers PA, Glancy RJ. Pyloric cam-
pylobacter infection and gastroduodenal disease. Med J Aust1985;142:439-44.
4STytgat GNJ, Langenberg ML, Rauws E, Rietra PJGM.Cainpylobacter-ike organisms (CLO) in the human stomach.Gastroenterology 1985;88:1620.
on 23 March 2019 by guest. P
rotected by copyright.http://jcp.bm
j.com/
J Clin P
athol: first published as 10.1136/jcp.39.4.353 on 1 April 1986. D
ownloaded from
Campylobacter pyloridis, gastritis, and peptic ulceration'6Siurala M, Varis KV. Gastritis. In: Sircus W, Smith AN, eds.
Scientific foundations ofgastroenterology. London: William Hei-nemann, 1980:357-69.
Marshall BJ. Nervous dyspepsia. Med J Aust 1985;142:704.48Talley NJ. The pathogenesis of non-ulcer dyspepsia. Med J Aust
1985;143:173.49 Hughes K, Robertson DAR, James WB. Duodenogastric reflux in
normal and dyspeptic subjects. Clin Radiol 1982;33:461-6.50Talley NJ, Piper DW. Is stress a factor in non-ulcer dyspepsia-a
preliminary report. Gastroenterology 1985;88:1608.51Talley NJ Piper DW. Double-blind crossover study of cimetidine
and pirenzepine in non-ulcer dyspepsia. Gastroenterology1985;88:1608.
52Christiansen J, Aagaard P, Koudahl G. Truncal vagotomy anddrainage in the treatment of ulcer-like dyspepsia without ulcer.Acta Chir Scand 1975;139:173-5.
S3Whitehead R. Gastritis. In: Mucosal biopsy of the gastrointestinaltract. 3rd ed. London: Saunders, 1985:41.
S4 Marshall BJ, Armstrong JA, McGechie DB, Glancy RJ. Attemptto fulfil Koch's postulates for pyloric campylobacter. MedJ Aust1985;142:436-9.
s Ramsay EJ, Carey KV, Peterson WL, et al. Epidemic gastritis withhypochlorhydria. Gastroenterology 1979;76:1449-57.
56 Gledhill T, Leicester RJ, Addis B, et al. Epidemic hypochlorhydria.Br MedJ 1985;290:1383-6.
S7 Legerton CW. Duodenal and gastric ulcer healing rates: a review:Am J Med 1984;77:2-7.
S8Prichard PJ, Rubinstein D, Jones DB, et al. Double blind compara-tive study of omeprazole 10 mg and 30 mg daily for healingduodenal ulcers. Br Med J 1985;290:601-3.
"Fullman G, Van Deventer C, Schneidman D, Walsh J, ElashoffJ,Weinstein W. "Healed" duodenal ulcers are histologically ill.Gastroenterology 1985;88: 1390.
"Gear MWL, Truelove SC, Whitehead R. Gastric ulcer and gas-
tritis. Gut 1971;12:639-45.61Tatsuda M, Okuda S, Tamura H, Taniguchi H. Endoscopic diag-
nosis of early gastric cancer by the endoscopic Congo red-methylene blue test. Cancer 1982;50:2956-60.
62 Mackay IR, Hislop IG. Chronic gastritis and gastric ulcer. Gut1966;7:228-33.
63 Schrager J, Spink R, Mitra S. The antrum in patients with duo-denal and gastric ulcers. Gut 1967;8:497-508.
64 Lambert JR, Dunn KL, Eaves ER, Korman MG, Hansky J, Pink-ard KIJ. Pyloric CLO in the human stomach. Med J Aust1985;143:174.
6SGoodwin CS, Armstrong JA. Will antibacterial chemotherapy beefficacious for gastritis and peptic ulcer? J Antimicrob Chemother1986;17: 1-4.
66Rune SJ. Acid-base parameters of duodenal contents in man.
Gastroenterology 1972;62:533.67Davenport HW. Salicylate damage to the gastric mucosal barrier.
N Engl J Med 1967;276:1307-12."Davenport HW. Destruction of the gastric mucosal barrier by
detergents and urea. Gastroenterology 1968;54:174-81.Allen A, Garner A. Mucus and bicarbonate secretion in the stom-ach and their possible role in mucosal protection. Gut1980;21:249-62.
70Hazell SL, Lee A. The adaption ofmotile strains ofCampylobacterpyloridis to gastric mucus and their association with gastricepithelial intercellular spaces. In: Pearson AD, Skirrow MB,Lior H, Rowe B, eds. Campylobacter 111: proceedings ofthe thirdinternational workshop on Campylobacter infections. London:Public Health Laboratory Service, 1985:189-191.
71Cantey JR, Blake RK. Diarrhoea due to Escherichia coli in therabbit. A novel mechanism. J Infect Dis 1977;135:454-62.
7'Guerrant RL. Microbial toxins and diarrhoeal diseases: intro-duction and overview. In: Ciba Foundation Symposium 112.Microbial toxins and diarrhoeal disease. London: Pitman,1985:1-13.
'3Takeuchi A, Inman LR, O'Hanley PD, Cantey JR, Lushbaugh
365
WB. Scanning and transmission electron microscopic study ofEscherichia coli 015 (RDEC-1) enteric infection in rabbits.Infect Immun 1978;19:686-94.
74 Cantey JR, Lushbaugh WB, Inman LR. Attachment of bacteria tointestinal epithelial cells in diarrhea caused by Escherichia colistrain RDEC-1 in the rabbit: stages and role of capsule. J InfectDis 1981;143:219-30.
7S Cantey JR. The rabbit model of Escherichia coli (strain RDEC-I)diarrhea. In: Boedeker EC, ed. Attachment of organisms to thegut mucosa, Florida: CRC Press, 1984:40-7.
76Rothbaum RJ, McAdams AJ, Giannella R, Partin JC. A clinico-pathologic study of enterocyte adherent Escherichia coli: a causeof protracted diarrhea in infants. Gastroenterology 1982;83:441.
"Tzipori S, Robins-Browne RM, Gonis G, Hayes J, Withers M,McCartney E. Enteropathogenic Escherichia coli enteritis: eval-uation of the gnotobiotic piglet as a model of human infection.Gut 1985;26:470-8.
78Langenberg ML, Rauws EAJ, Schipper MEI, et al. The pathogenicrole of Campylobacter pyloridis studied by attempts to eliminatethese organisms. In: Pearson AD, Skirrow MB, Lior H, Rowe B,eds. Campylobacter III: proceedings of the third internationalworkshop on Campylobacter infections. London. Public HealthLaboratory Service, 1985:162-3.
Marshall BJ, Francis G, McGechie D. Correlation between symp-toms of dyspepsia and Campylobacter pyloridis serology inWestern Australian blood donors. In: Pearson AD, Skirrow MB,Lior H, Rowe B, eds. Campylobacter 111: proceedings of the thirdinternational workshop on Campylobacter infections. London:Public Health Laboratory Service, 1985:118-9.
80Kaldor J, Tee W, McCarthy P, Watson J, Dwyer B. Immuneresponse to Campylobacter pyloridis in patients with pepticulceration. Lancet 1985;i:921.
81 Svedheim A, Gunnarsson H, Kaijser B. Diffusion-in-gel enzymelinked immunosorbent assay for routine detection of IgG andIgM antibodies to Campylobacter jejuni. J Infect Dis1983;148:82-92.
82Bardhan K, Cole DS, Hawkins BW, Franks CR. Does treatmentwith cimetidine extended beyond initial healing of duodenalulcer reduce the subsequent relapse rate? Br Med J1982;284:621-23.
83 McLean AJ, Harrison PM, Ioannides-Demos L, Byrne AJ,McCarthy P, Dudley FJ. The choice of ulcer healing agentinfluences duodenal ulcer relapse rate and long-term clinicaloutcome. Aust NZ J Med 1985;15:367-74.
8McLean AJ, Harrison PN, loannides-Demos LL, Byrne AJ,McCarthy P, Dudley FJ. Microbes, peptic ulcer, and relapserates with different drugs. Lancet 1984;ii:525-6.
Marshall BJ, McGechie DB, Armstrong JA, Francis G. The anti-bacterial action of bismuth: early results of antibacterial regi-mens in the treatment of duodenal ulcer. In: Pearson AD, Skir-row MB, Lior H, Rowe B, eds. Campylobacter III: proceedingsof the third international workshop on Campylobacter infections.London: Public Health Laboratory Service, 1985:165-6.
86Shirokova KI, Filomonov RM, Poliakova LV. Metronidazole inthe treatment of peptic ulcer. Klin Med (Mosk) 1981;59:48-50.
87 Zheng ZT, Wang ZY, Chu YX, et al. Double-blind short-term trialof furazolidone in peptic ulcer. Lancet 1985;i: 1048-9.
88Zhao H-Y, Li G, Guo J, et al. Furazolidone in peptic ulcer. Lancet1985;ii:276-7.
89Osler W, McRae T. Disease of the stomach. In: The principles andpractice of medicine. New York: Appleton, 1920.
Requests for reprints to: Professor C Stewart Goodwin,Head, Department of Microbiology, Royal Perth Hospital,Box 2213 G.P.O., Perth, Western Australia 6001.
on 23 March 2019 by guest. P
rotected by copyright.http://jcp.bm
j.com/
J Clin P
athol: first published as 10.1136/jcp.39.4.353 on 1 April 1986. D
ownloaded from