riding the current: upstream and downstream approaches · pdf fileapproaches to implement...
TRANSCRIPT

Riding the Current: Upstream and Downstream
Approaches to Implement Adult Immunization
Strategies
Paul Nguyen Community Health Partnership
Connie Chung-BohlingCalifornia Department of Public Health

Session Agenda• Overview of Adult Immunization Project
• Adult Immunization Practices Survey
o Clinic Workflow, Practices, and Barriers
o Electronic Health Records (EHR) and California
Immunization Registry (CAIR) Use and Barriers
o Reimbursement
o Review of Barriers and Solutions
• Community Health Partnership
o Implementation of Adult Immunization Program
• Vaccines for Adults (VFA) Program
2

Learning Objectives• Identify specific health care settings where
uninsured adults are more likely to seek services
• List at least two barriers and their solutions in
adopting the standards for adult immunization
practices into clinical workflows
• Describe current best practices to increase adult
immunizations in a selection of FQHCs and
community health centers
3

Vaccine Coverage in CA, by Year
4
0% 20% 40% 60% 80% 100%
Pneumococcal, age ≥65
Pneumococcal 18-64 yrs, high
risk
Tdap ≥18 yrs
Zoster
Coverage (%)
2013
2014
2015
Healthy People 2020 Goal
Data Source: Centers for Disease Control and Prevention (CDC) BRFSS 2013-2015 https://www.cdc.gov/vaccines/imz-managers/coverage/adultvaxview/data-reports/general-population/index.html

Vaccine Coverage, by race/ethnicity, California 2015
5
25%
59%
37%
36%
66%
31%
35%
76%
34%
39%
75%
46%
0% 20% 40% 60% 80% 100%
Pneumococcal 18-64 yrs
Pneumococcal, age ≥65
Tdap ≥18 yrs
Coverage (%)
White
Other/Multiple
Black
Hispanic
Healthy People 2020 Goal
Vaccine Coverage %’s among Hispanics and Blacks are consistently lower compared to that among Whites
Data Source: Centers for Disease Control and Prevention (CDC) BRFSS 2015 https://www.cdc.gov/vaccines/imz-managers/coverage/adultvaxview/data-reports/general-population/index.html

Project OverviewAdult Immunization Grant FQHCs
o Improve adult immunization standards in California
o Components
• FQHCs
• VFA Program
• Pharmacies
• Healthcare Systems
o Consortium of Community Health Centers and FQHCs in San Mateo and Santa Clara Counties
o Pilot Health Centers (3)
• Implement strategies to increase adult immunizations
• Share lessons learned
6

Adult Immunization Standards
• ASSESS immunization status of all patients at every clinical encounter
• Strongly RECOMMEND vaccines that patients need
• ADMINISTER needed vaccines or REFER your patients to a vaccination provider
• DOCUMENT vaccines received by your patients
7

Survey MethodsHealthcare delivery sites Survey Details
• Gather data on current immunization practices within the consortium by administering a survey
• Distributed to 10 member health organizations – 9 respondentso 34 health care delivery
sites
• Respondents: Medical Directors, MD, RN, MA, Billing staff
8
Limitations• No validation
• Low sample size
• Respondents mostly Medical Directors
9

Clinic Workflow and Practices
Survey Results
10

Routine Immunizations Programs
Do your clinics routinely assess, recommend, and administer?
11
All
All
Some
Some
No
No
0
1
2
3
4
5
6
7
8
9
Pneumococcal and Hep B Tdap and Flu
Diabetes Pregnancy
# M
emb
er H
ealt
h O
rgan
izat
ion
s
N = 9

Standing Orders
Health Providers who Assess Health Providers who Administer
12
MD or
NP
PA
CNW
RN
MA
None
NP
PA
CNW
RN
MA
LVN
None
N = 9
Which healthcare providers within your clinics assess (and which administer) adult immunizations for patients under standardized procedures / protocols or standing orders, if any?

Staff and Clinic Workflow
Strategies Barriers
• Patient registry or panel
management
• EHR guidelines/protocols
• Routine screening at
every appointment
• Clinician and staff
education
• Standing orders
• Huddle sheet, chart
“scrubs” or reviews
• Vaccine purchase and
administration cost
• Implement standing
order protocols
• Continued education
to providers
13

EHR and CAIR UseSurvey Results
14

EHR Use
15
0 2 4 6 8
Remind/Recall Patients
Run Coverage Reports
Decision Support
Provide Prompts
Print Records
Manage Inventory
# ResponsesN = 9
Clinics use NextGen or eClinicalWorks

CAIR Use
16
0 1 2 3 4 5 6 7 8 9
Shot history
Decision Support
Manage Inventory
List for Reminder/Recall
# Responses
N = 9
29 of 34 clinics use CAIR

CAIR UseMajor Barriers Major Needs
• Limited staffo Data entry into CAIR
o Double data entry into EHR and CAIR
o Check CAIR for immunization status
o Set up data exchange
• Usabilityo Concerns about
incomplete immunization histories
o Unsure about usability
o Clinic uses EHR immunization record module
• Data exchange
support
o Support to transfer
records from EHR to CAIR
o Set up EHR to interface
with CAIR
o Interpreting and
resolving error messages
to improve data quality
• Additional Staff
o Help with data entry
• CAIR Staff Training
17

ReimbursementSurvey Results
18
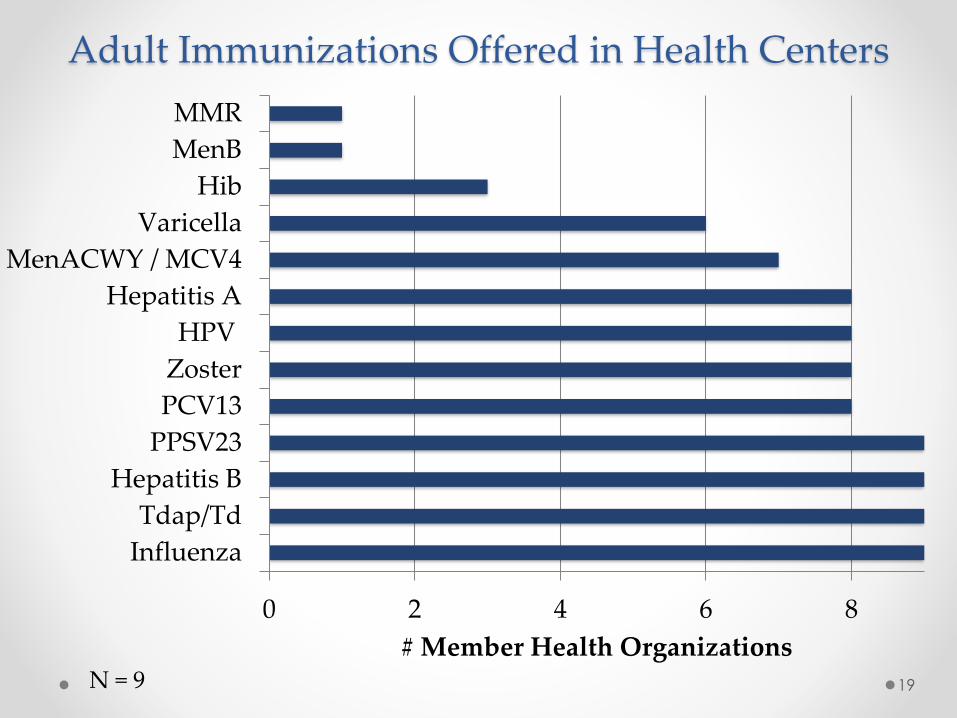
Adult Immunizations Offered in Health Centers
19
0 2 4 6 8
Influenza
Tdap/Td
Hepatitis B
PPSV23
PCV13
Zoster
HPV
Hepatitis A
MenACWY / MCV4
Varicella
Hib
MenB
MMR
# Member Health OrganizationsN = 9

ReimbursementDo payments meet the cost of vaccines and their
administration?
20
0 1 2 3 4 5 6 7 8 9
No Response
No
Yes
No Response
No
Yes
Ad
min
istr
atio
nV
acci
ne
# Member Health OrganizationsN = 9
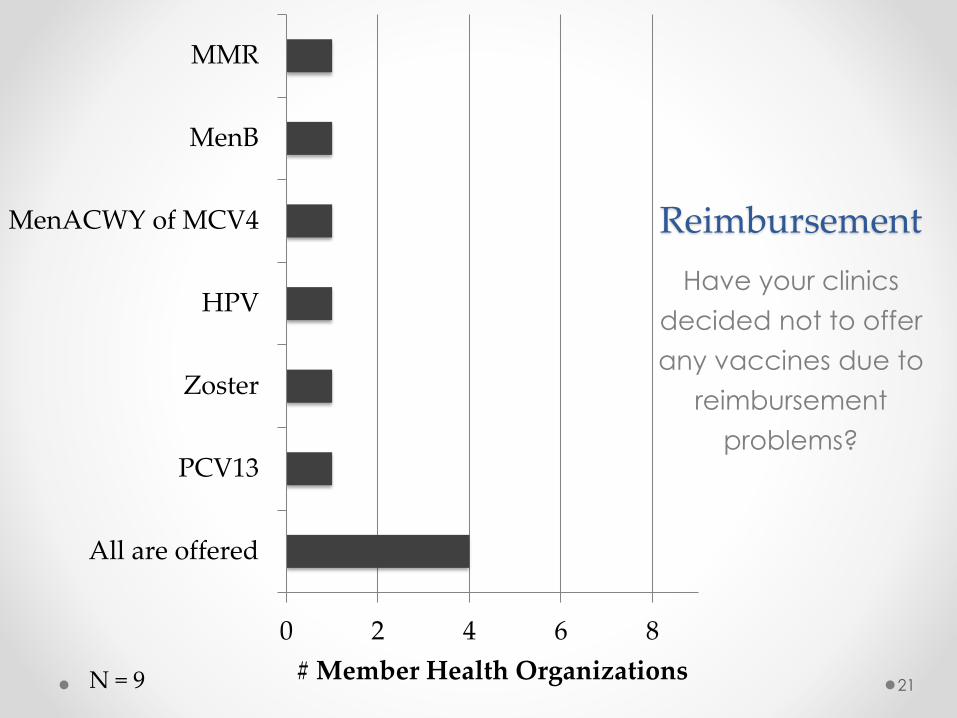
Reimbursement
Have your clinics
decided not to offer
any vaccines due to
reimbursement
problems?
21
0 2 4 6 8
All are offered
PCV13
Zoster
HPV
MenACWY of MCV4
MenB
MMR
# Member Health OrganizationsN = 9

ReferralsIf unable to provide immunizations on-site, do your clinics:
Refer patients to another provider for
immunization?
Find out if the referral was successful
and patient was immunized?
22
0 2 4 6 8
No Response
No
Yes
0 2 4 6 8
No Response
No
Yes
Refer to: travel clinic, pharmacy, LHD Unsure of vaccine availability at other clinicsOnly if patient brings back documentationLoss to follow-upPatient may decline vaccineN = 9

Barriers Solutions
• Clinic Flow
• Patient Panels & Team Based Care
• Standing Orders
Staffing/Workflow
• Data exchange support and collaboration
• Data driven improvementEHR/CAIR Use
• VFA Program
• Policy Interventions Reimbursement
23

Introduction to CHP
• Community Health Partnership, Inc. (also known as "CHP") was founded in 1993 in response to community concern for the viability of community-based, primary care health centers.
• CHP is 1 of 19 Community Health Center Associations in California. CHP represents 9 Community Health Center (CHC) organizations with 39 clinical sites in Santa Clara and San Mateo Counties. Our member CHC serve 176,348 patients in 2015, 2/3 or which are below 200% of the federal poverty level.
Criteria for Selecting Pilot Organization
• Has Electronic Medical Record system that is uploading
data to California Immunization Registry (CAIR)
• Has a significant number of prenatal patients annually
• Has a significant number of uninsured patients annually
• Is a participant of the Vaccine For Adult (VFA) Program
• Has an active vaccination program

Pilot Organization Demographics
4%
6%
11%
2%
5%
19%
17%
25%
10%
0% 5% 10% 15% 20% 25% 30%
Under 1 year
1 - 4 years
5 - 12 years
13 - 14 years
15 - 19 years
20 - 34 years
35 - 44 years
45 - 64 years
65 and over
AGE DISTRIBUTION
Male
37%
Female
63%
GENDER DISTRIBUTION

Pilot Organization Demographics
Medicare 3%
Medical 65%
Private insurance 2%
Other 1%
uninsured 29%
Coverage Data by Payer, SHC
Medicare
Medical
Privateinsurance
Other
uninsured

ApproachThe 10 Building Blocks of High Performing Primary Care
- Tom Bodenheimer, MD
The Bodenheimer model has been adopted by Community Health
Partnership as a framework for helping our member Health Centers
transform to becoming a High Performing
Primary Care Practice.
To improve immunization rates CHP focused
on the 4 foundational building blocks of
engaged leadership, data-driven
improvement, empanelment,
and team-based care.
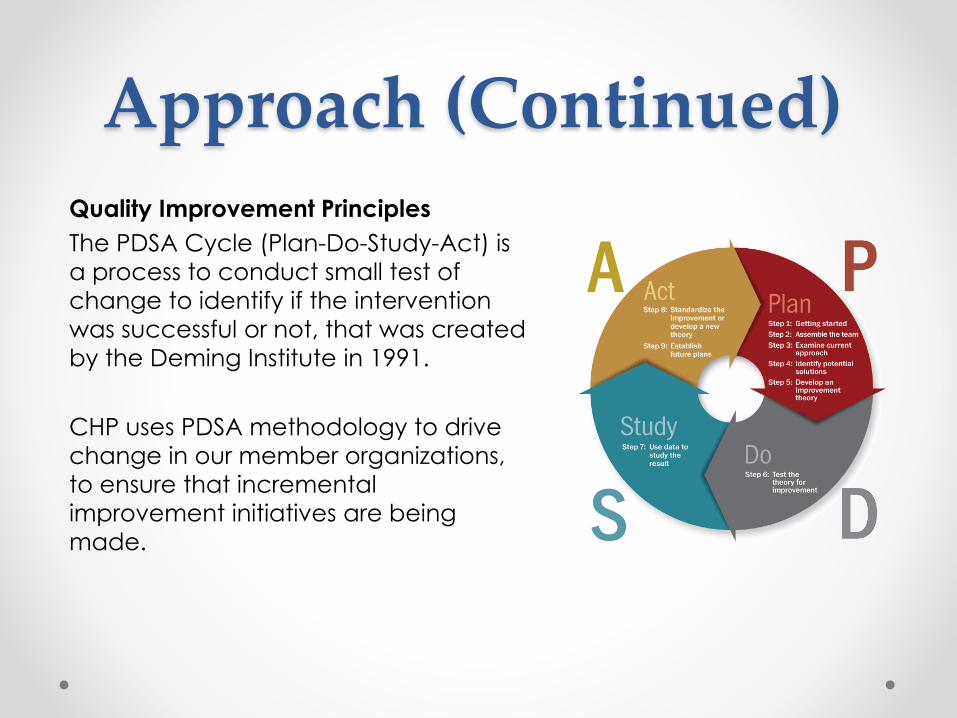
Approach (Continued)Quality Improvement Principles
The PDSA Cycle (Plan-Do-Study-Act) is
a process to conduct small test of
change to identify if the intervention
was successful or not, that was created
by the Deming Institute in 1991.
CHP uses PDSA methodology to drive
change in our member organizations,
to ensure that incremental
improvement initiatives are being
made.

Baseline 2016 Immunization Rates
Pilot Health Center
11%
17%14%
21%
13%
70% 70%
90%
30%
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
Influenza 18+ Influenza 65+ Pneumococal Zoster Tdap
MayView Immunization Rates 2016 (January -September)
CY 2016 (January - September) HP 2020 Goal

Barriers Identified From Pilot• Lack of inventory management process
• Lack of standard clinical workflows
• Understanding of Immunization Coverage
• No Culture of Data Sharing
• Access to complete immunization records
• Patient Panels are not in place for proper
care management

Engaging Leadership
Barriers & Strategy:➢ Lack of inventory management process
▪ Review job descriptions and redefined roles for Lab
Technicians to lead handling of vaccine inventory.
➢ Lack of standard clinical workflows
▪ Developed standing orders for medical assistants to conduct
initial assessment of patient immunization gaps and report to
Provider for approval.
▪ PDSA – Pilot standing order with selected Provider/Medical Assistant dyad.
➢ Understanding of Immunization Coverage
▪ Coordinated CDPH VFA Program training for clinical staff to
understand vaccine coverage.

Data Driven Improvement
Barriers & Strategy:➢ No Culture of Data Sharing
▪ Developed data wall to post immunization rates data for staff
and patient
▪ Data for project is shared with staff at monthly all staff meeting
➢ Staff not comfortable with identifying Immunization Gaps
▪ Implement Care Guidelines to provide Medical Assistance with
clinical decision support to identify patient immunization gaps.
➢ Access to Incomplete Immunization Records
▪ “No record, No shot” – If patients are not able to provide proof
of immunizations or if immunization records can not be read or
translated then staff are trained to proceed as if the
immunization did not occur and proceed to immunize and
document in patients chart.

Empanelment
Barriers & Strategy:➢ Patient Panels are not in place for proper care management
▪ CHP provided training to Pilot Health Center Staff:
▪ Develop Provider Panels
▪ Review Patient Health Registries
▪ Training to conduct Care Team Huddles to identify
immunization gaps prior to shift
Team-Based Care
Barriers & Strategy:➢ Lack of standard clinical workflows
▪ Using standing orders and implementation of care guidelines
to help Support Staff identify patient immunization gaps during
office visits and report to Provider for approval.