role of pharmacoepidemiology in drug evaluationmartin...role of pharmacoepidemiology in drug...
TRANSCRIPT
Role of Pharmacoepidemiology in Drug Evaluation
Martin Wong MD, MPHSchool of Public Health and Primary Care
Faculty of MedicineChinese University of Hog Kong
Outline of Content• Introduction: what is pharmacoepidemiology about?
• Research: Use of pharmacoepidemiology datasets
• Contributions & Roles of pharmacoepidemiology in various areas:– Data supplementation in premarketing studies: Quantitation of the
incidence of drug effects– Discovery of undetected drug effects– Analysis of cost-effectiveness of drugs– Drug utilization patterns & adherence profiles– Assess effects of drug overdoses & reassure drug safety– Association between medication use and outcomes
• Future direction of development
What is pharmaco-epidemiology about?
• the study of the use of and the effects of drugs in large numbers of people
• applies the methods of epidemiology to the content area of clinical pharmacology– Epidemiology: methods of inquiry– Clinical pharmacology: focus of inquiry– Applies the methods of epidemiology to the content area of clinical
pharmacology
• an effective tool to capture useful data for clinicians, researchers and policy-makers
When should one perform pharmacoepidemiology studies?
• Regulatory– Earlier approval for marketing– Response to question by regulatory agency– Assist application for approval for marketing elsewhere
• Marketing– To assist market penetration by documenting the safety of the drug– To increase name recognition– To assist in repositioning of the drug– To protect the drug from accusations about adverse effects
• Legal• Clinical
– Hypothesis testing/generating
Research: Use of pharmacoepidemiology
– Becoming more important to reflect “real life clinical practice” on pharmacological effects of medications and their utilization
– What happened to the RCTs?– Are they not robust enough?

2007 Guidelines for the management of arterial Hypertension
1). the need to select higher risk patients2). uncomplicated, younger and lower risk patients were
under-represented3). not representing real clinical practice4). Prolonging the observation of patients after the end of
trials might capture more “real-life” outcomes but these can only be done in an uncontrolled manner,
– the problem of selection bias still exist.
– The Task Force for the Management of Arterial Hypertension of the European Society of Hypertension (ESH) and of the European Society of Cardiology (ESC) (2007). 2007 Guidelines for the management of arterial hypertension. European Heart Journal 28:1462- 536.
Contributions & Roles of pharmacoepidemiology in various areas:
– 1). Data supplementation in premarketing studies
– Better quantitation of the incidence of known adverse and beneficial effects
• Higher precision• In patients not studied prior to marketing e.g. the elderly,
children, in pregnant women• As modified by other drugs and other illnesses.• Relative to other drugs used for the same medication.
Contributions & Roles of pharmacoepidemiology in various areas:
2). Quantitation of the disease incidence & drug effects
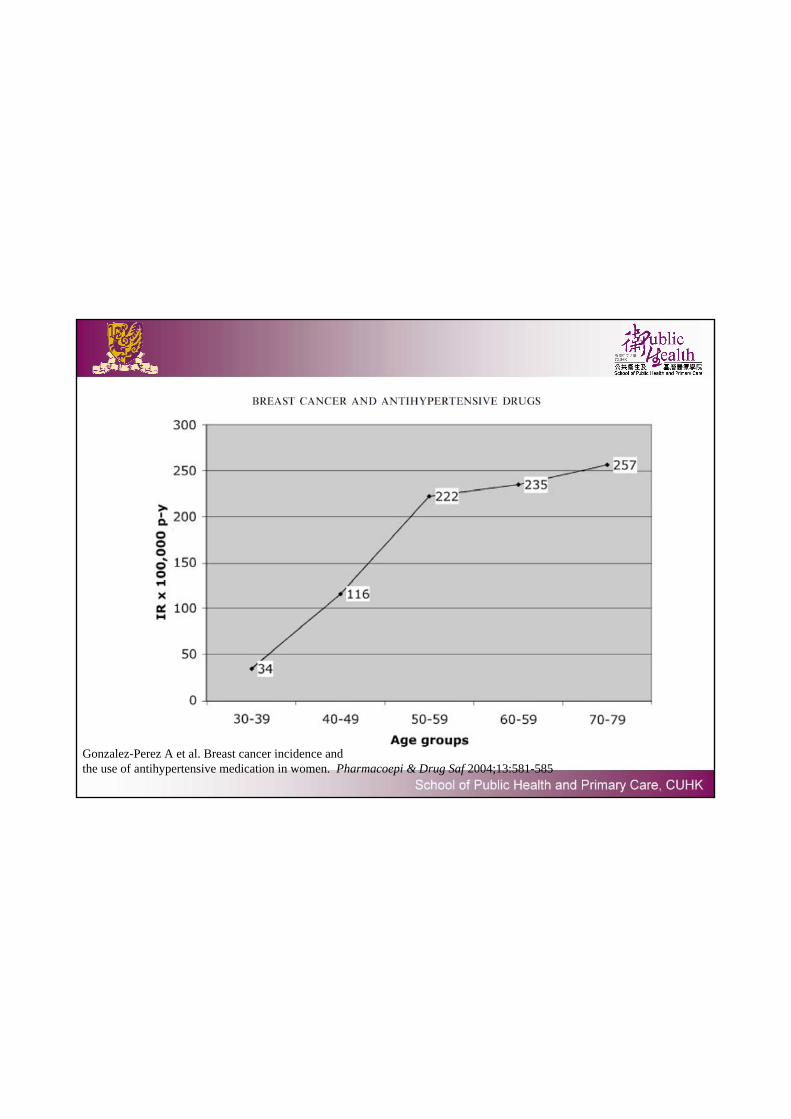
Gonzalez-Perez A et al. Breast cancer incidence and the use of antihypertensive medication in women. Pharmacoepi & Drug Saf 2004;13:581-585
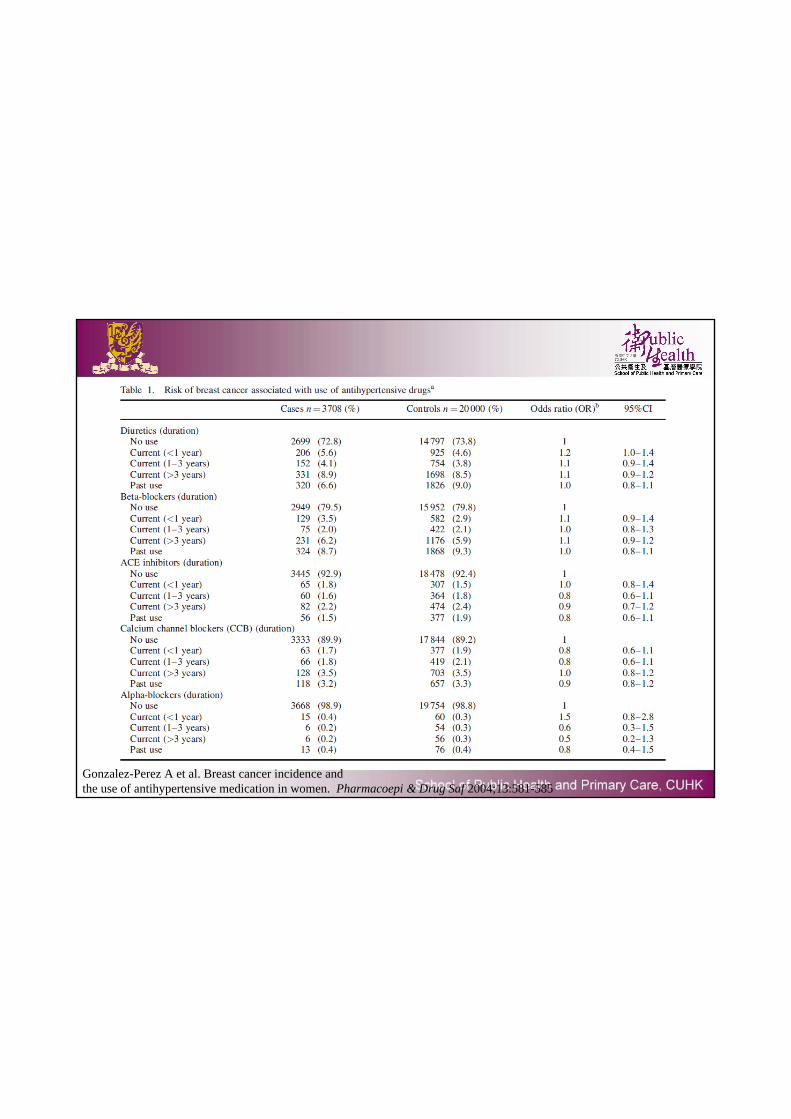
Gonzalez-Perez A et al. Breast cancer incidence and the use of antihypertensive medication in women. Pharmacoepi & Drug Saf 2004;13:581-585
Contributions & Roles of pharmacoepidemiology in various areas:
– 3). Discovery of undetected drug effects
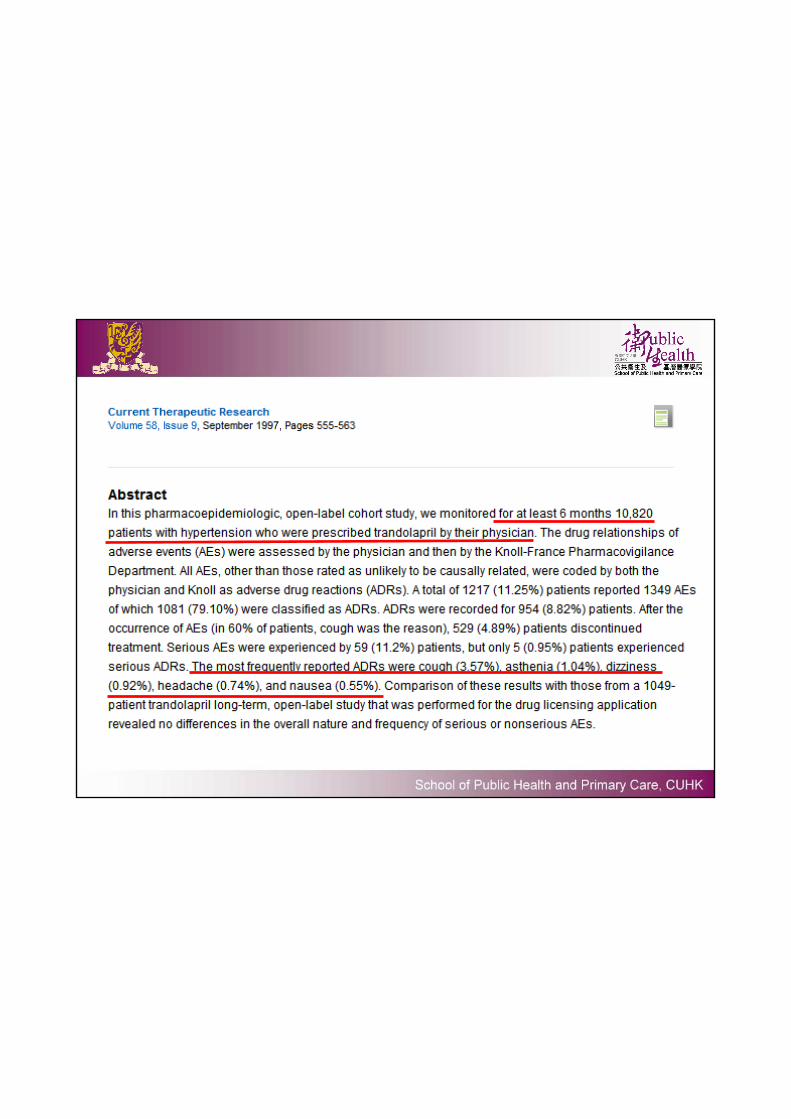
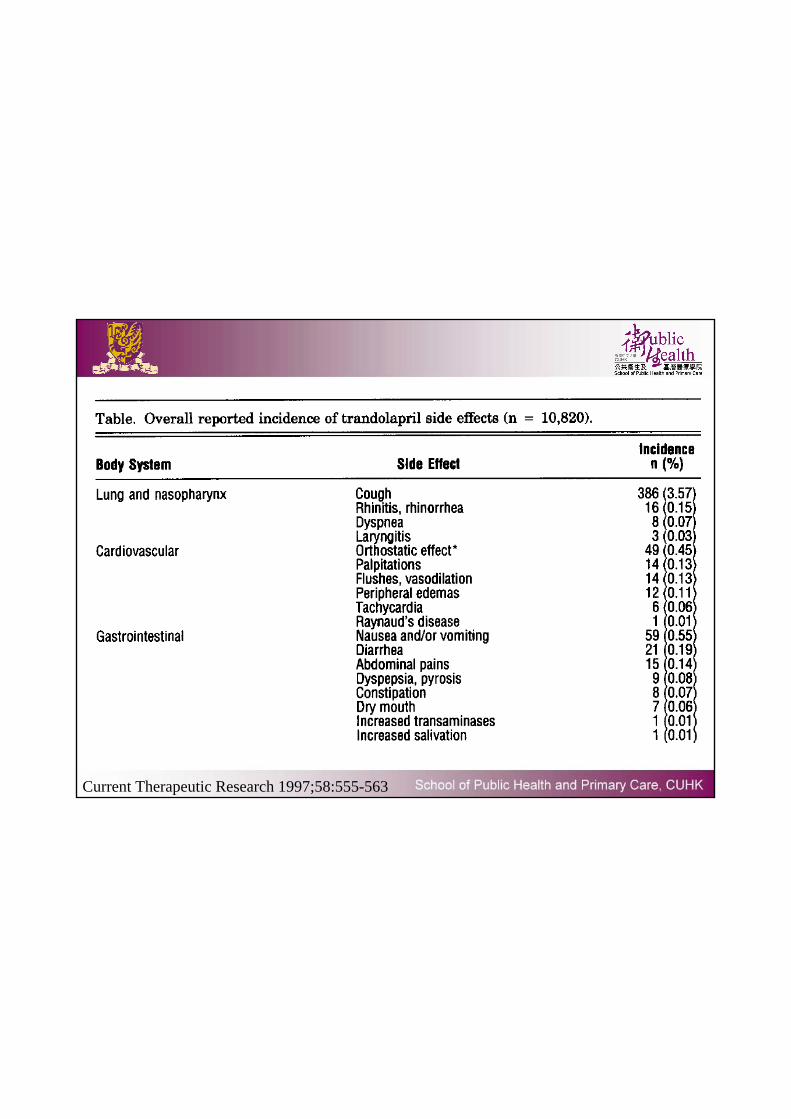
Current Therapeutic Research 1997;58:555-563
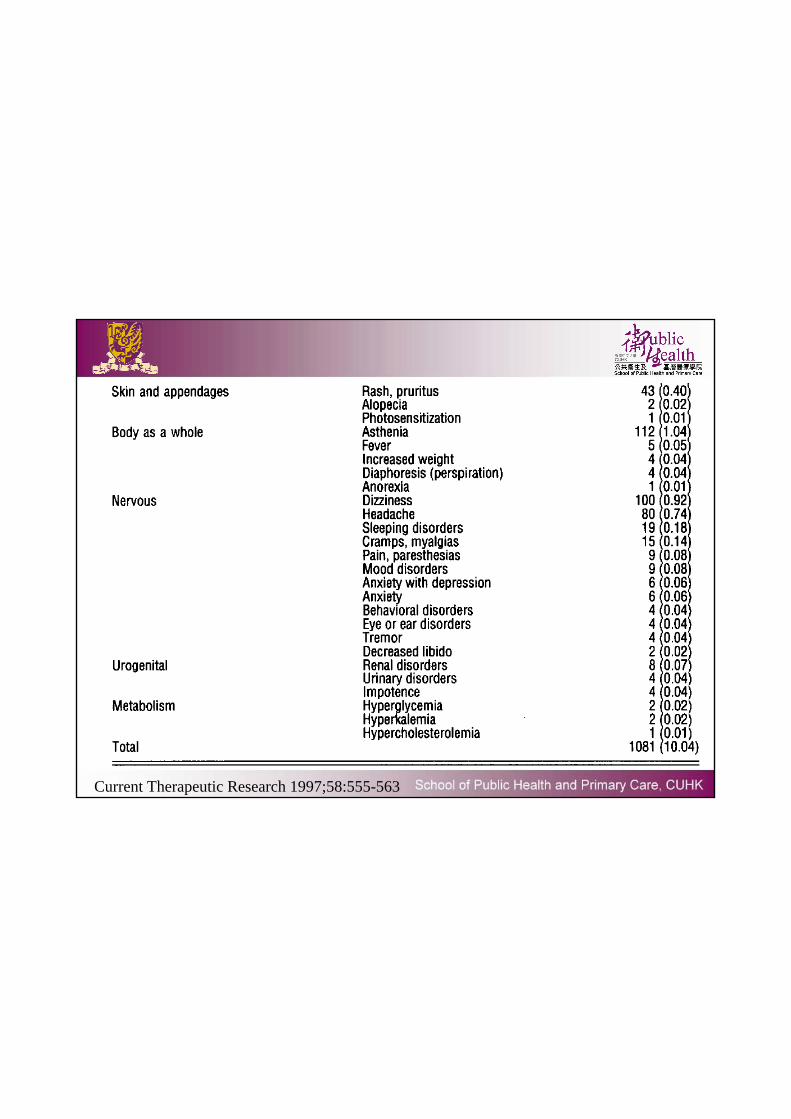
Current Therapeutic Research 1997;58:555-563
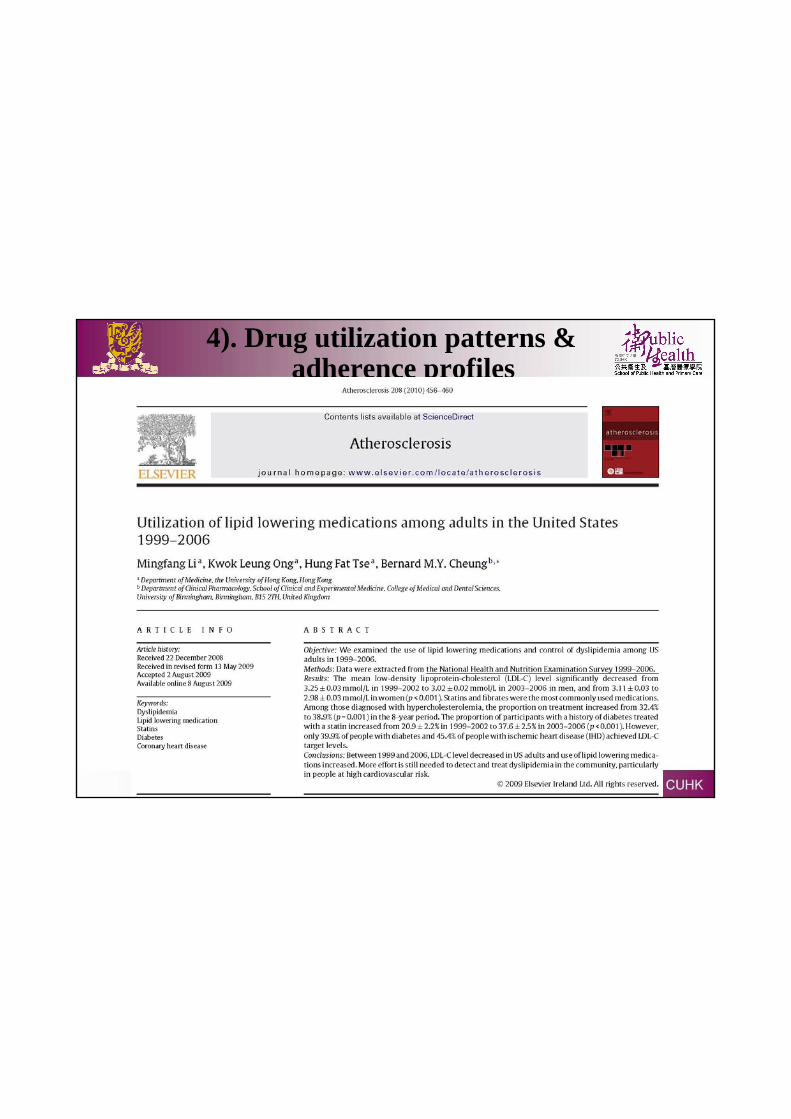
4). Drug utilization patterns & adherence profiles
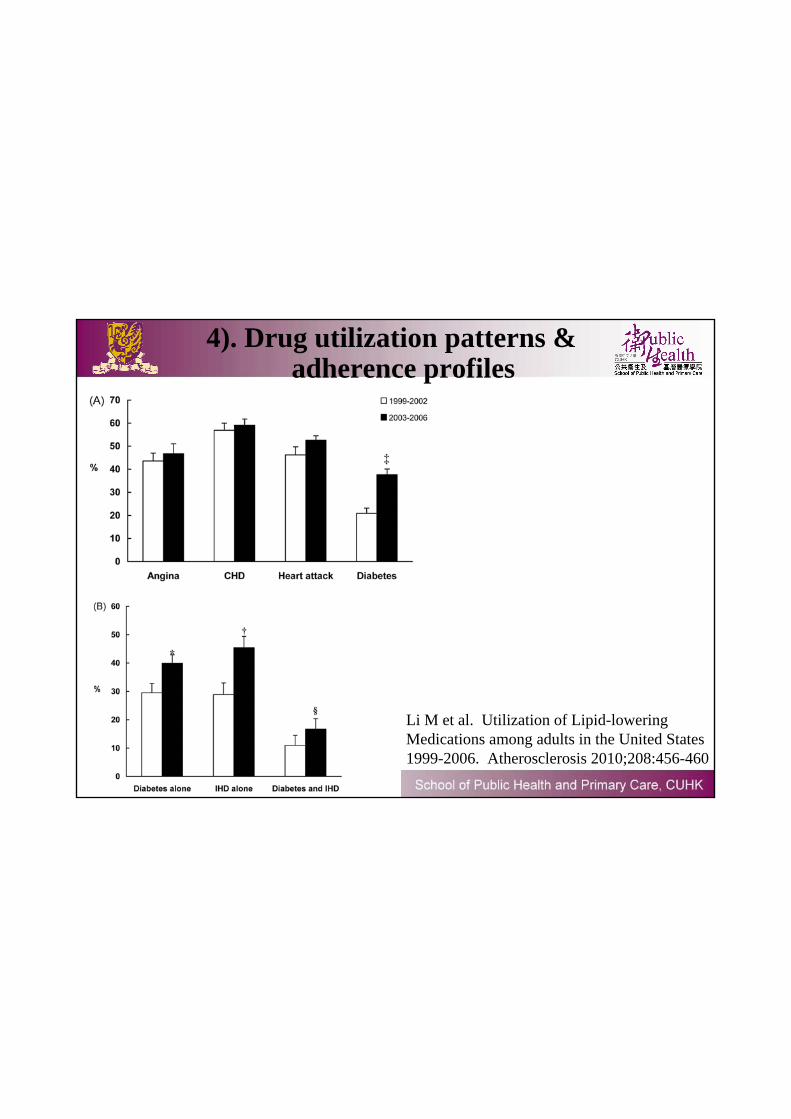
4). Drug utilization patterns & adherence profiles
Li M et al. Utilization of Lipid-lowering Medications among adults in the United States 1999-2006. Atherosclerosis 2010;208:456-460
Contributions & Roles of pharmacoepidemiology in various areas:
– 5). Assess effects of drug overdoses & reassure drug safety
Am J Cardiol 2010;106:1594-1601
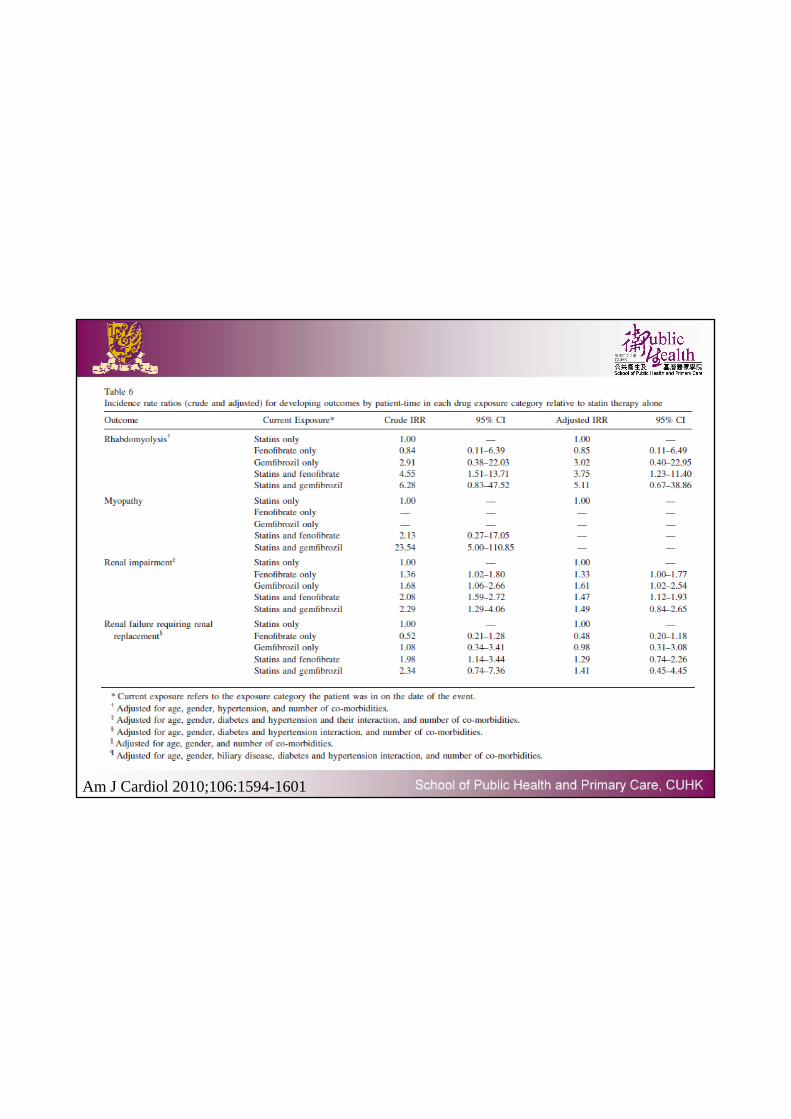
Am J Cardiol 2010;106:1594-1601
Methods
• Data Source– Electronic computerized system, Hospital Authority– included a large population of Hong Kong ~ 1.3 million– Robustness of database evaluated
• High completeness of demographic data (100%) & prescription details (99.98%)*
*Wong MCS, Jiang Y, Tang JL, Lam A, Fung H, Mercer SW, Griffiths S. Health services research in the public healthcare system in Hong Kong: An analysis of over 1 million antihypertensive prescriptions between 2004-2007 as an example of the potential and pitfalls of using routinely collected electronic patient data. BMC Health Services Research 2008;8:138
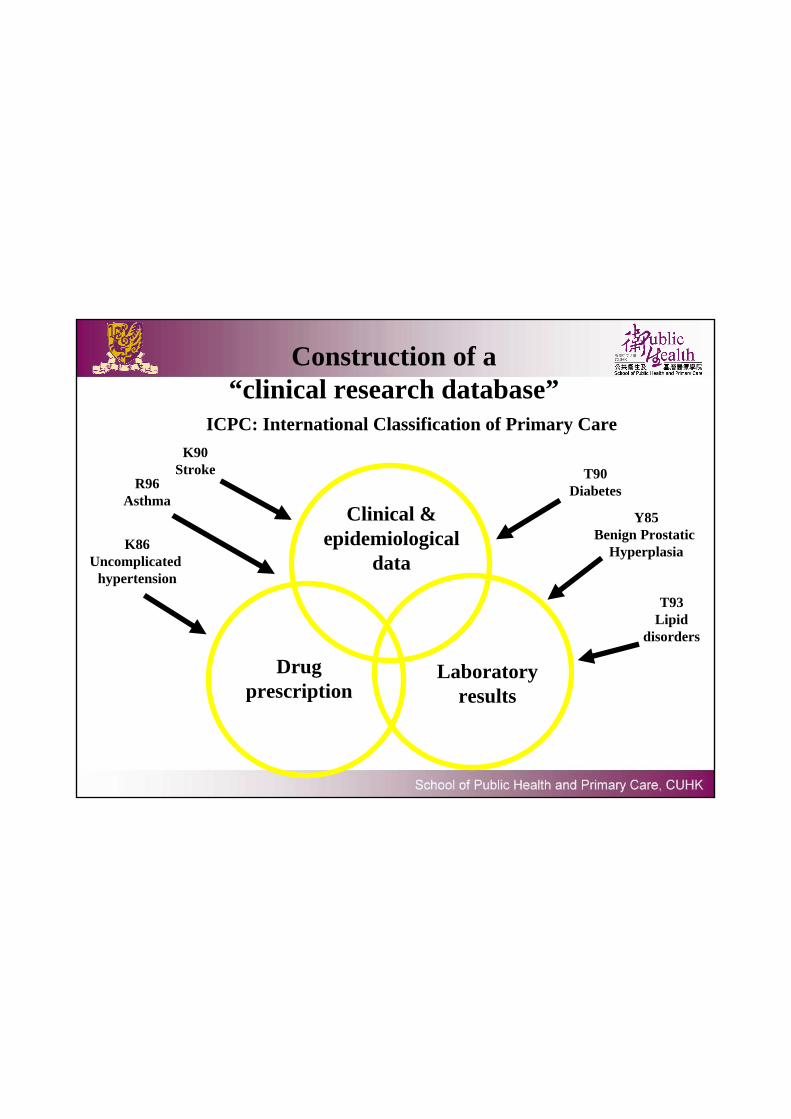
Construction of a “clinical research database”
Clinical & epidemiological
data
Drugprescription
Laboratory results
ICPC: International Classification of Primary Care
K86Uncomplicated
hypertension
T90Diabetes
T93Lipid
disorders
K90Stroke
R96Asthma
Y85Benign Prostatic
Hyperplasia
*Wong MCS, Jiang Y, Tang JL, Lam A, Fung H, Mercer SW, Griffiths S. Health services research in the public healthcare system in Hong Kong: An analysis of over 1 million antihypertensive prescriptions between 2004-2007 as an example of the potential and pitfalls of using routinely collected electronic patient data. BMC Health Services Research 2008;8:138
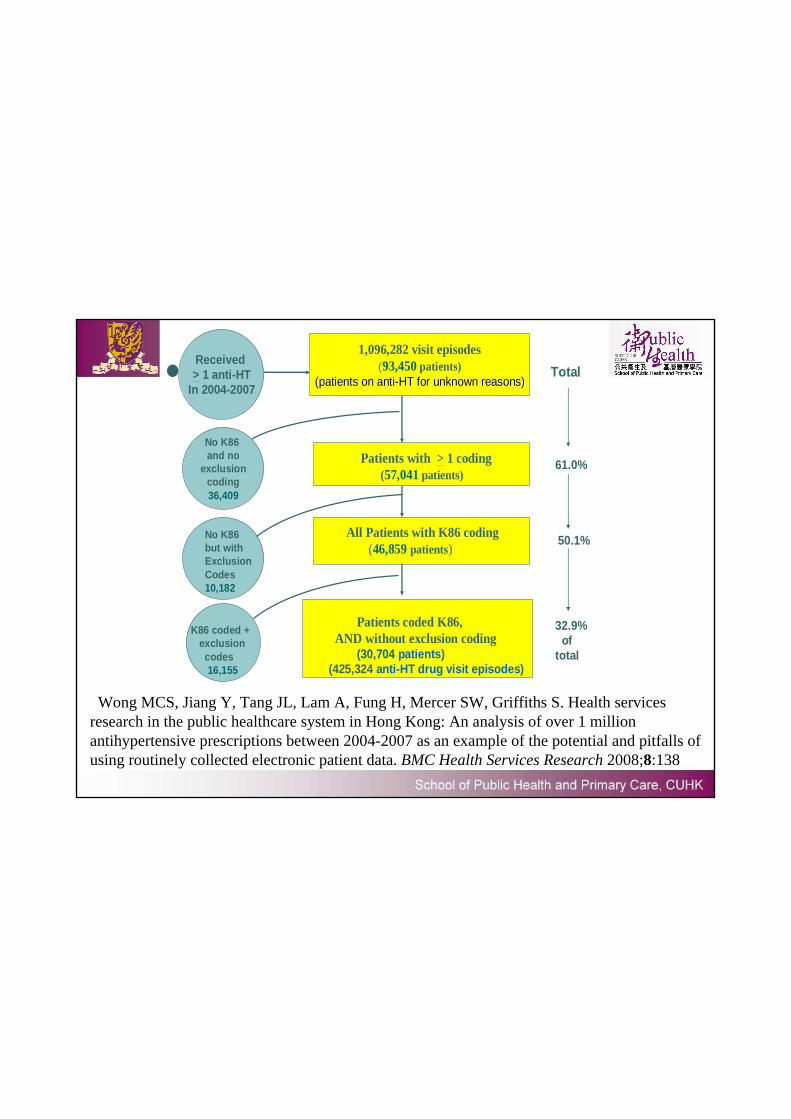
1,096,282 visit episodes(93,450 patients)
(patients on anti(patients on anti--HT for unknown reasons)HT for unknown reasons)
Received > 1 anti-HT
In 2004-2007
No K86 and no
exclusioncoding36,409
Patients with > 1 coding(57,041 patients)
Patients coded K86,AND without exclusion coding
(30,704 patients)(425,324 anti-HT drug visit episodes)
No K86but withExclusion Codes10,182
All Patients with K86 coding(46,859 patients)
K86 coded + exclusion codes16,155
Total
61.0%
50.1%
32.9%of
total
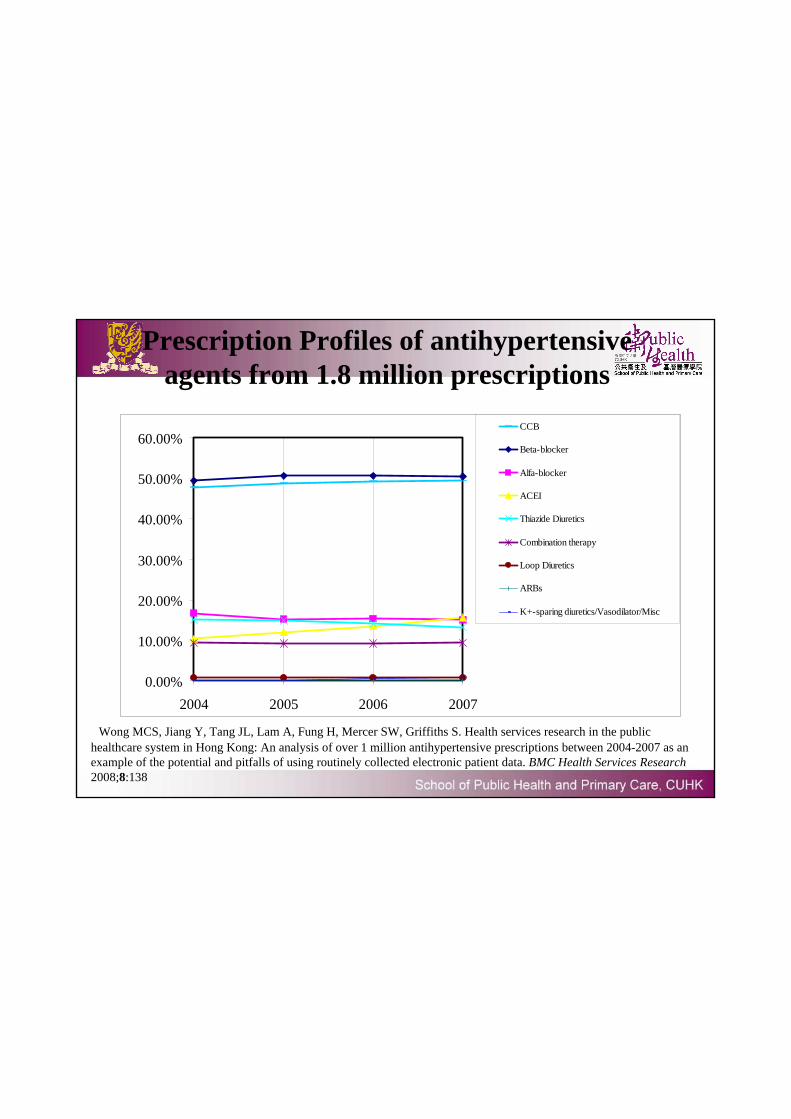
Prescription Profiles of antihypertensive agents from 1.8 million prescriptions
*Wong MCS, Jiang Y, Tang JL, Lam A, Fung H, Mercer SW, Griffiths S. Health services research in the public healthcare system in Hong Kong: An analysis of over 1 million antihypertensive prescriptions between 2004-2007 as an example of the potential and pitfalls of using routinely collected electronic patient data. BMC Health Services Research 2008;8:138
0.00%
10.00%
20.00%
30.00%
40.00%
50.00%
60.00%
2004 2005 2006 2007
CCB
Beta-blocker
Alfa-blocker
ACEI
Thiazide Diuretics
Combination therapy
Loop Diuretics
ARBs
K+-sparing diuretics/Vasodilator/Misc
Background
• International guidelines on management of arterial hypertension– Thiazide diuretics a first-line agent– JNC 7th, NICE (ESC/ISH)
• Metabolic side effects of thiazide diuretics– Includes ↓Na+ and ↓K+
– Hospital admissions & even mortality– Deters physicians from prescribing them…
Background
• The majority of reports on anti-HT & electrolytes were conducted in Caucasian countries alone– electrolyte profiles among Chinese hypertensive
patients on thiazides have been scarce and were small scale
• Ethnicity is associated with different pharmacological outcomes of antihypertensive agents – even small ethnic differences may bear substantial
health resource implications
Participants• Inclusion criteria:
– Patients who newly attended the public primary care practice & prescribed a single antihypertensive agent as the first-ever antihypertensive pharmacotherapy in the public sector during January 2004 to June 2007
– coded by physicians with ICPC K86 (uncomplicated hypertension)– had their plasma Na+ and K+ levels checked 4–16 weeks after the
prescription
• Exclusion criteria:– subjects having concomitant cardiovascular factors or clinical
conditions that could confound antihypertensive prescription choice– Discontinued or switched their drug prescription or received Na+ or
K+ supplements before electrolyte measurements
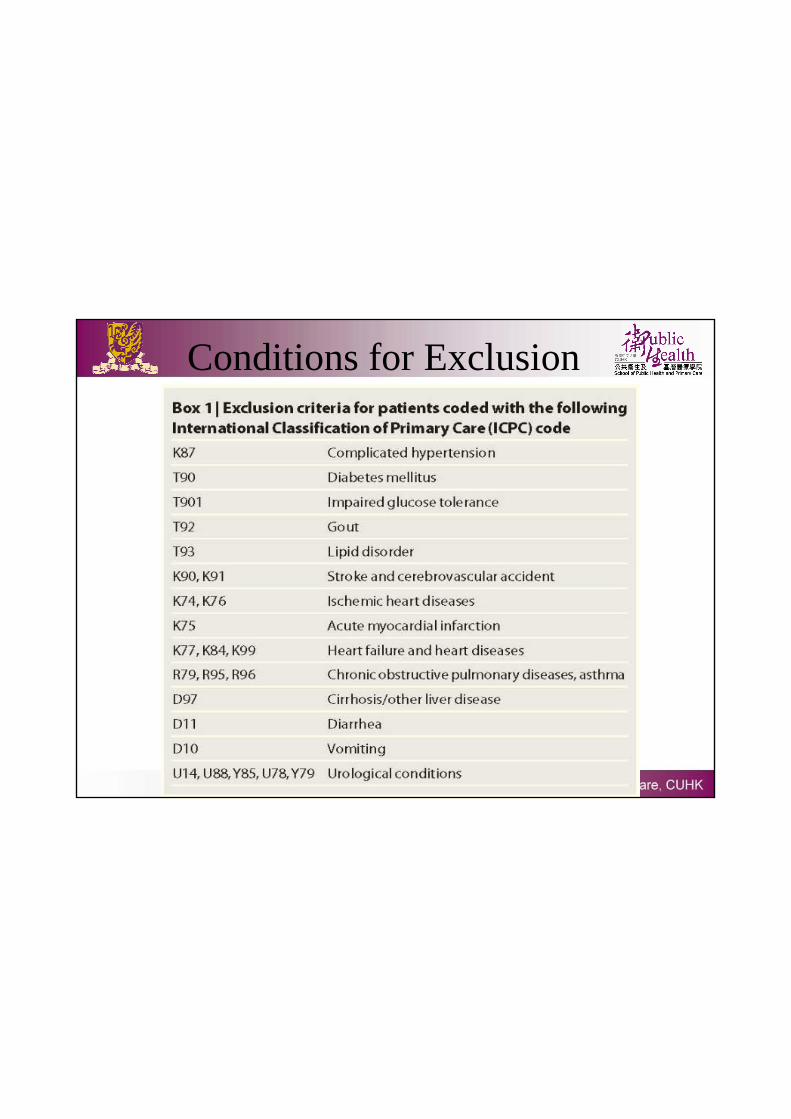
Conditions for Exclusion
Antihypertensive drug classes
• Each patient was classified into one drug group according to the prescription– BB: β-blockers, – TD: Thiazide diuretics, – CCB: Calcium channel blockers, – RAS: drugs acting on the renin–angiotensin system, and – Others (including α-blockers, potassium-sparing and
other diuretics, vasodilators, and combination therapy).
• Evaluated the dosage of each prescription qualitatively as “low,” “medium,” or “high” according to standard drug formulary.
Outcome variables• (1). the mean plasma Na+/K+ levels• (2). the proportions of patients having low (Na <135 mEq/l; K
<3.4 mEq/l), normal (Na 136–147 mEq/l; K 3.5–5.1 mEq/l), and high (Na >148 mEq/l; K >5.2 mEq/l) levels among the various drug classes.
• Independent predictors and covariates include – patients’ age, – gender, – payment status (fee waivers vs. payers; each consultation
costs US$5.77), – district of residence, – estimated GFR (in tertiles), and – the antihypertensive drug classes prescribed
Statistical Analysis
• Two multivariate regression analyses
• Binary outcome variables: ↓Na+ and ↓K+
• significant differences between districts with respect to antihypertensive prescribing,– conducted sensitivity analyses where district of
residence was included and then excluded as an independent variable, respectively, to avoid over-controlling of covariates
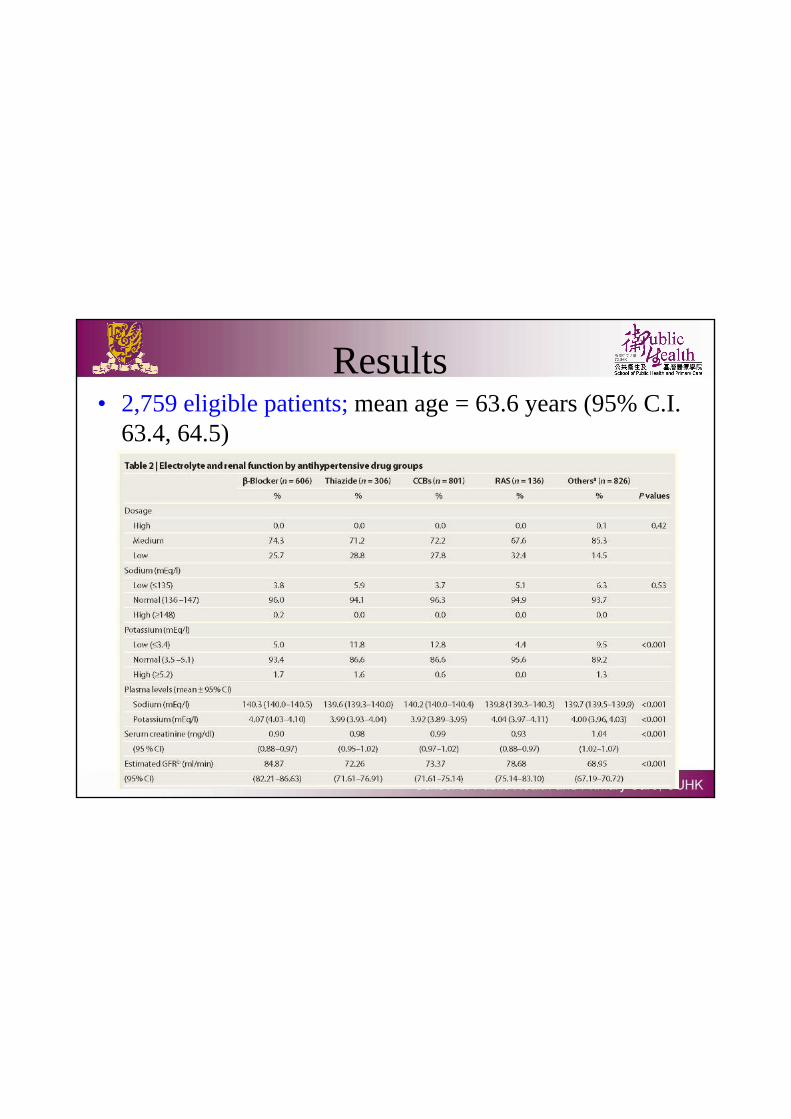
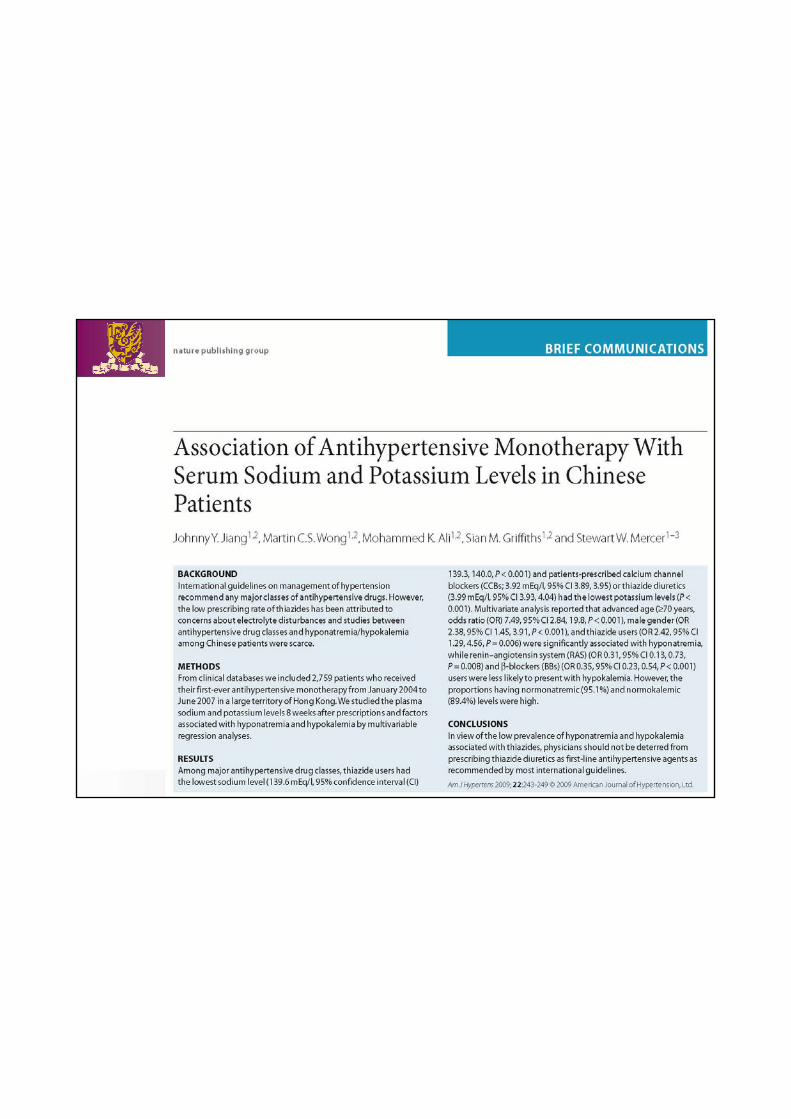
Results• 2,759 eligible patients; mean age = 63.6 years (95% C.I.
63.4, 64.5)
Major Findings• (1). Thiazide diuretics had the lowest levels of Na+; CCBs and
thiazide diuretics had the lowest levels of K when compared to other drug classes– the absolute magnitude of differences were minimal.
• (2). Factors positively associated with ↓Na+ from multivariate regression analysis
– advanced age, – male gender, – and thiazide user
• (3). RAS and BBs were less likely to present with ↓K+ when compared with CCB.
Interpretations• (1). Elderly women could have expanded fluid volume after
increased fluid intake but decreased ability to excrete free water, which might explain the higher risks of ↓Na+ among the elderly.
• (2). Male patients with advanced age should have their sodium levels monitored more closely.
• (3). Physicians should not be deterred from prescribing thiazide.
• (4). some caution is needed in prescribing thiazide and CCBs because the prevalence of ↓K+ (11.8 and 12.8%, respectively) is still not negligible
Limitations
– 1). Could the sample size be larger?
– 2). Baseline electrolyte: absent
– 3). Ethnicity: generalizability to other races?
– 4). risk association: not cause-and-effect relationship
– 5). Dietary diary & other confounders: not available
Contributions & Roles of pharmacoepidemiology in various areas:
– 6). Association between medication use and clinical outcomes
JHH 2009; 23: 735-742
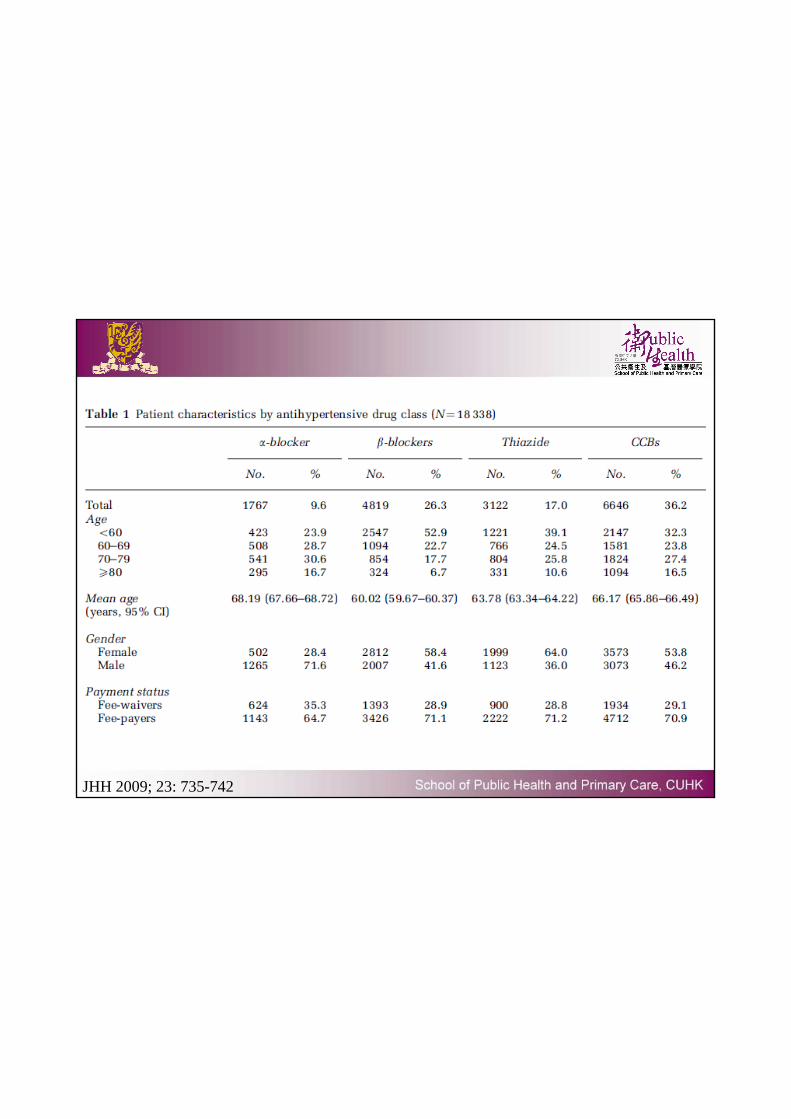
JHH 2009; 23: 735-742
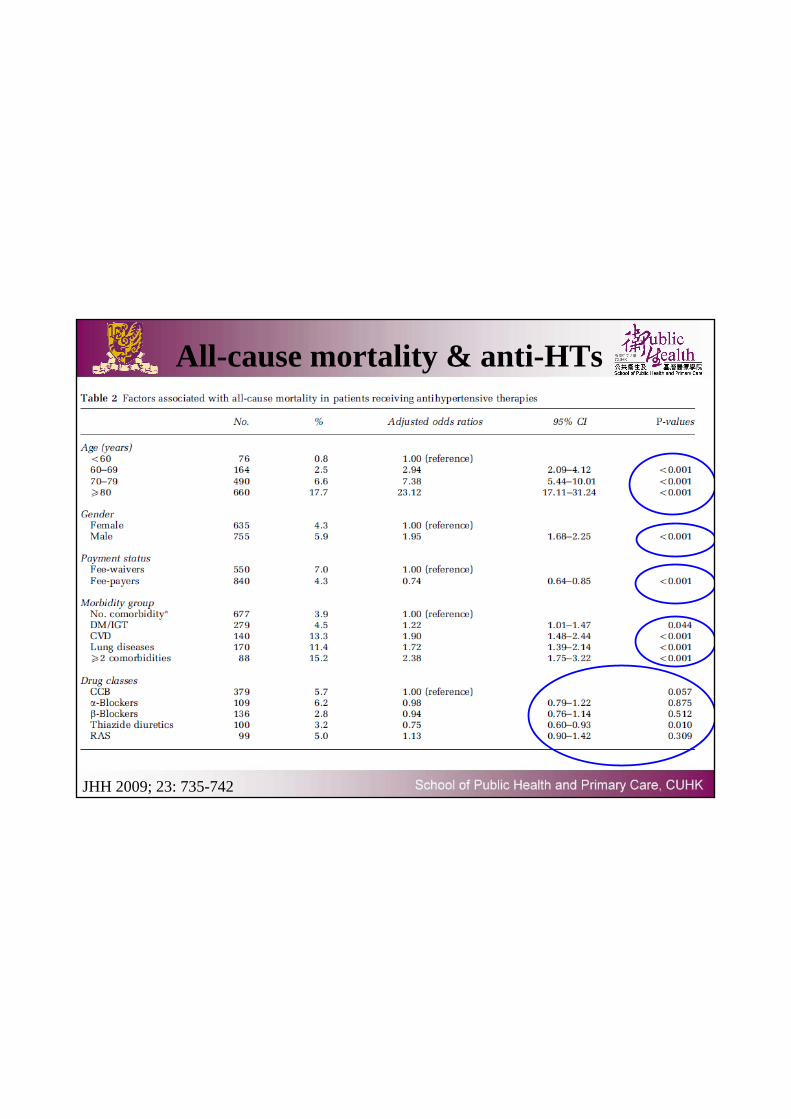
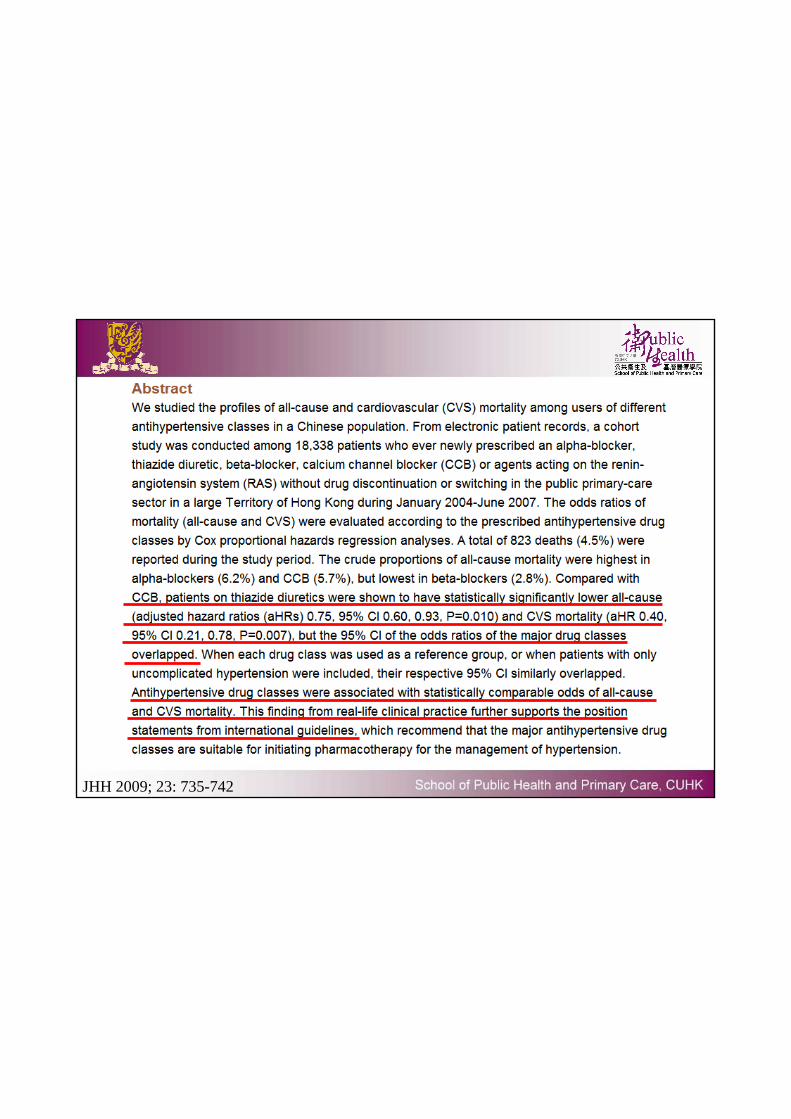
All-cause mortality & anti-HTs
JHH 2009; 23: 735-742
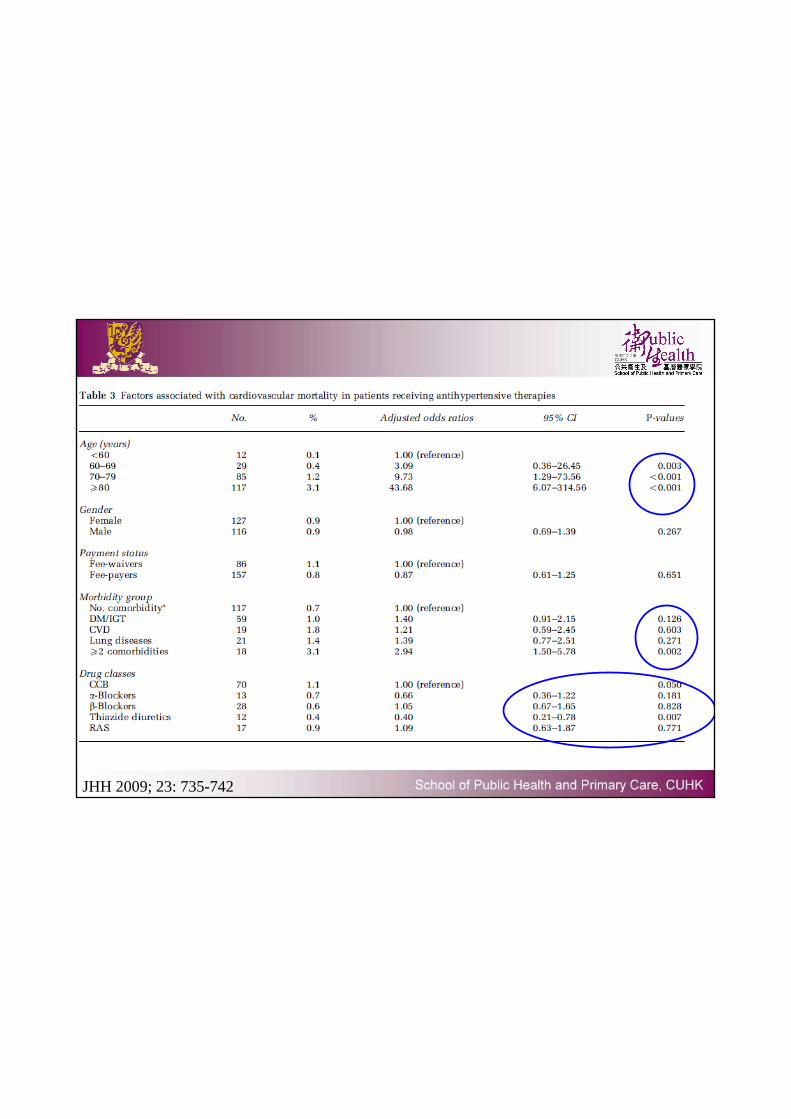
JHH 2009; 23: 735-742
JHH 2009; 23: 735-742
Contributions & Roles of pharmacoepidemiology in various areas:
– 7). Analysis of cost-effectiveness of drugs
Pharmacotherapy 1991; 11: 50-5

Future direction of development• 1). Rapid development & increased interests globally• Annual international conference on pharmacoepidemiology: attendance
50 (1980) 900 (2004)
• ISPE: 800 members from 37 countries; guidelines (2004)
• Academic Journals: Clin Pharmacol Ther. (IF: 6.961, 11/237); J Clin Epidemiol; Pharmacoepidemiol & Drug Saf.– Actively solicit pharmaco-epi studies
• ↑ number of summer programmes on pharmaco-epidemiology– Michigan SPH (10%), McGill, Erasmus U. Rotterdam, Johns Hopkins
• Initiatives from pharmaceutical companies– Forming their own pharmaco-epidemiology units
Future direction of development• 2). The academics• Methodologic advances
– Expanded use of neural networks, propensity scores, sensitivity analyses, time-varying exposures & confounder control, data mining
– Involvement of pharmacoepidemiologists into policy questions– Emergence of pharmacogenetic studies
• New content areas of interest– E.g. drug utilization, prescription profiles
• Logistical advances• Funding• Personnel
Future direction of development• 2). The academics
• Training in statistical techniques– Confounding management– Use of propensity scores
• Better use of large-scale datasets– Coding rate of HT (ICPC-2 K86)/ DM (ICPC-2 T90)– Coding rate is increasing
Future direction of development• 3). The Industry – role of pharmacoepi expanding
– Contribute to identify problems & document drug safety– Develop & evaluate risk management programme– “prophylactic” studies by manufacturers– Post-marketing studies for all newly marketed drugs for chronic
diseases– Protect major investment made in developing a new drug
• Reduce legal liability
– Pharmaceutical companies: ↑ investment in external pharmacoepidemiologic data resources
– Need adequately trained researchers with statistical skills & robust dataset
Future direction of development
• 4). The Regulatory Agencies
• Also expanding
• Postmarketing pharmaco-epi studies replacing pre-marketing phase III studies (e.g. zidovudine)
• Use of therapeutic risk management approaches – change regulation
• Increase attention to drug safety (COX-2 inhibitors; NSAIDs)
Future direction of development• 5). The law
– ↑ No. of lawsuits related to adverse drug effects
– ↑ Awareness of the legal system’s ability to obtain substantial remuneration for those suffered from adverse effects
– Financial payments: put entire drug company at risk
References
• Brian L. Strom. Pharmaco-epidemiology (4th edition), Wiley
Future direction of development
• Let’s join our hands…Thank you