s 08-cartin-ceba effusion confusion.ppt - mayo clinic ... · thoracentesis in one week b. admit...
TRANSCRIPT

Effusion Confusion
5th Annual Acute Care of the Complex Hospitalized Patient for Advanced Practitioners
Scottsdale, Arizona, February 2016
Rodrigo Cartin‐Ceba, MD, MSc
Mayo Clinic Arizona
©2010 MFMER | slide‐1
Disclosures
• Nothing to disclose
©2010 MFMER | slide‐2

Objectives
Understand the following:• Types of pleural effusions and common
etiologies• Work-up of pleural effusions• Treatment of pleural effusions
Question 1What is the only known land mammal with no
pleura?
A. Elephant
B. Lion
C. Humans with Trisomy 18
D. Giraffe
E. Platypus

PLEURA
Visceral pleura lines the lungParietal pleura lines the chest wall/diaphragmSingle layer of mesothelial cellsLoose connective tissue, vesselsElastic fibersPleural space: between visceral and
parietal pleura

Pleura
Visceral Pl
Parietal Pl
Pleural Space
Functions of the pleura
• Allows extensive movement of the lung relative to the chest wall
• Visceral pleura provides mechanical support
• Route by which edema escapes the lung
PLEURAL EFFUSION
Abnormal collection of fluid in the pleural spaceFluid formation is affected by:
Hydrostatic pressuresPermeability of pleural vesselsOsmotic pressures
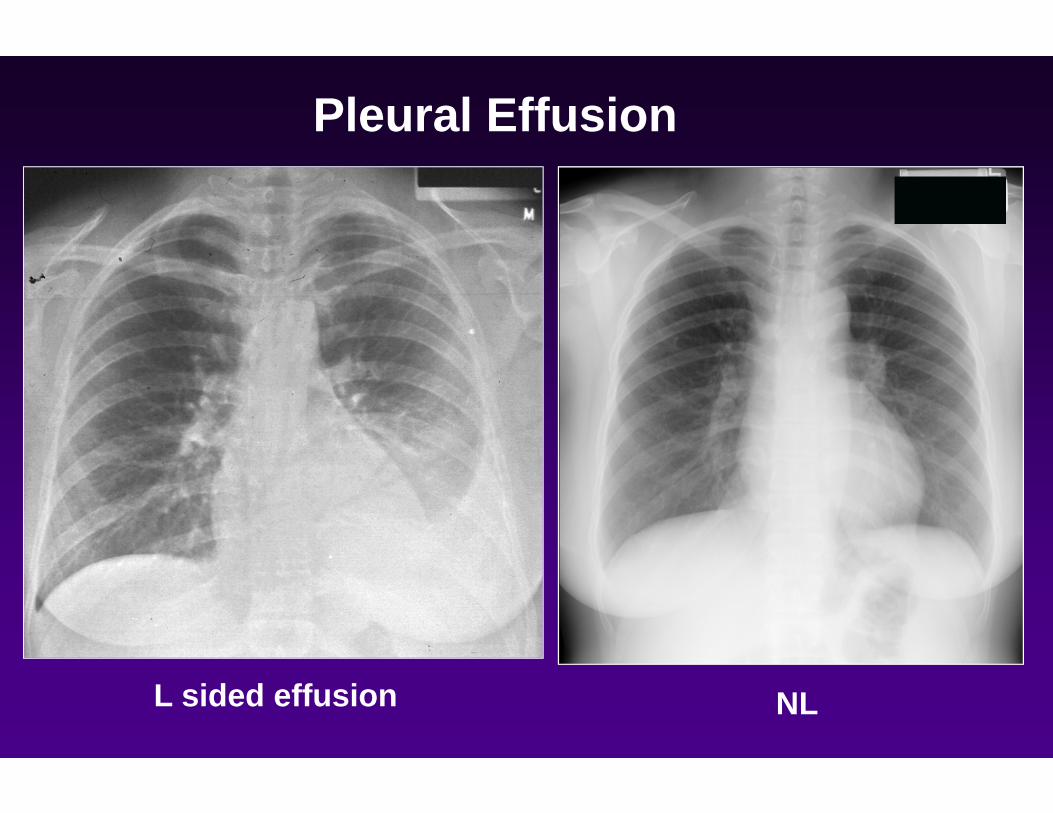
Pleural Effusion
L sided effusion NL
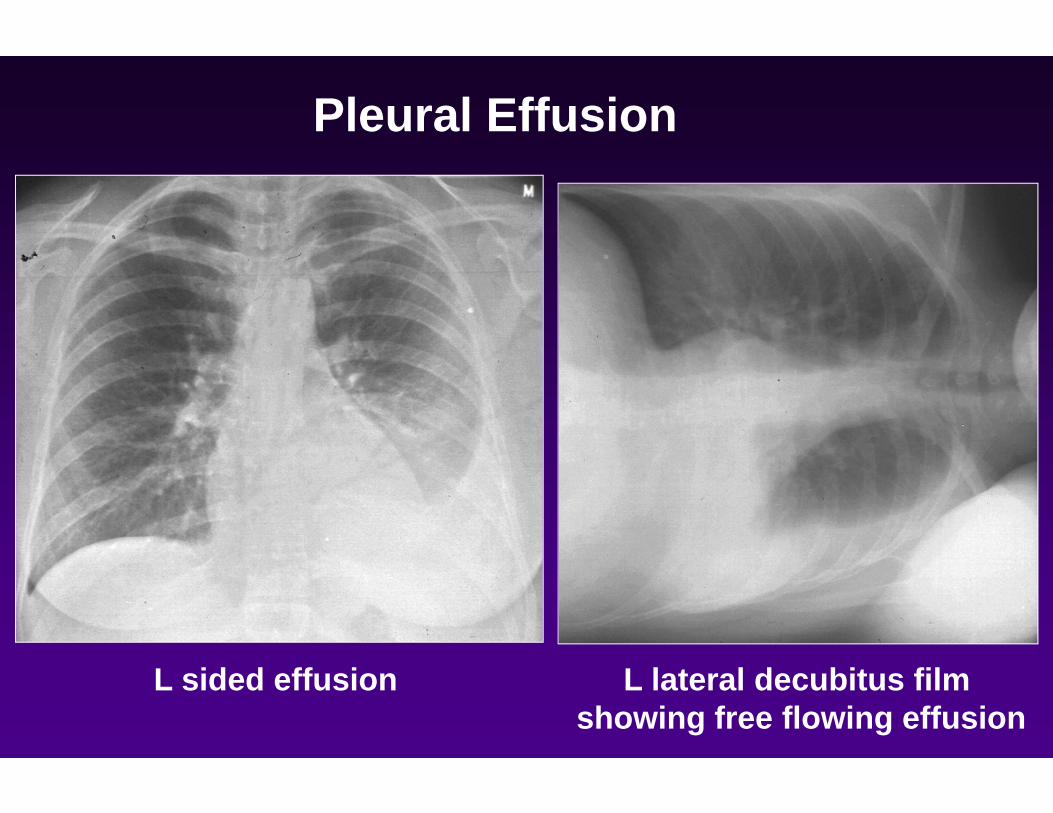
Pleural Effusion
L sided effusion L lateral decubitus film showing free flowing effusion

Pleural Effusion
Lateral view showinga blunted costophrenic angle
NL lateral view showinga sharp CP angle
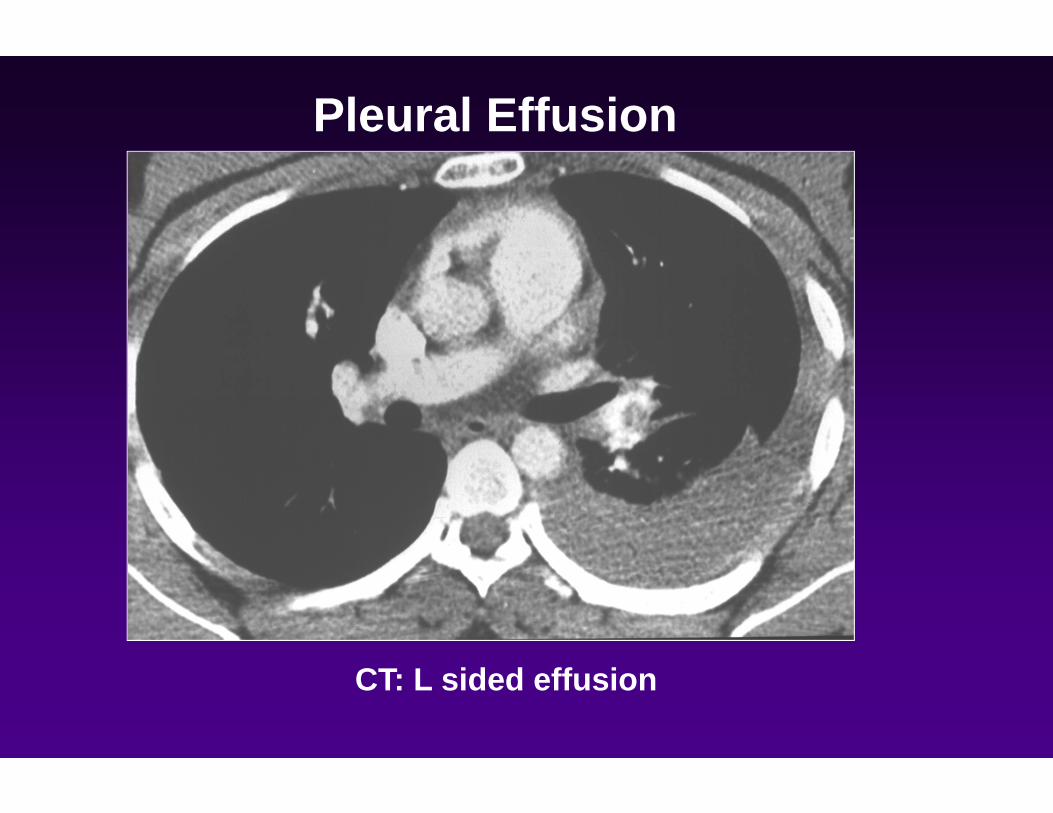
Pleural Effusion
CT: L sided effusion
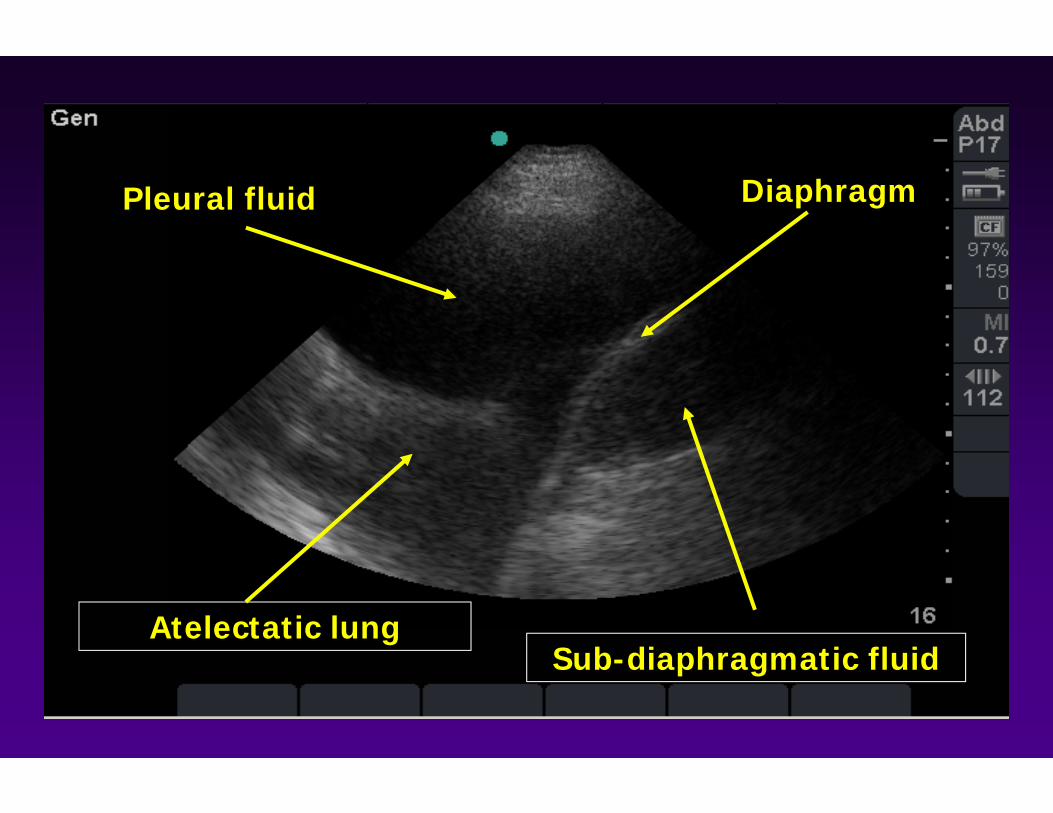
DiaphragmPleural fluid
Atelectatic lungSub-diaphragmatic fluid

Pleural Effusion Appearance
chyloushemorrhagic Serous
Question 2What is the most common cause of pleural effusion?
A. Cirrhosis
B. Cancer
C. Pneumonia
D. Heart Failure
E. Rheumatoid arthritis

Light RW. N Eng J Med 2002;346:1971-77
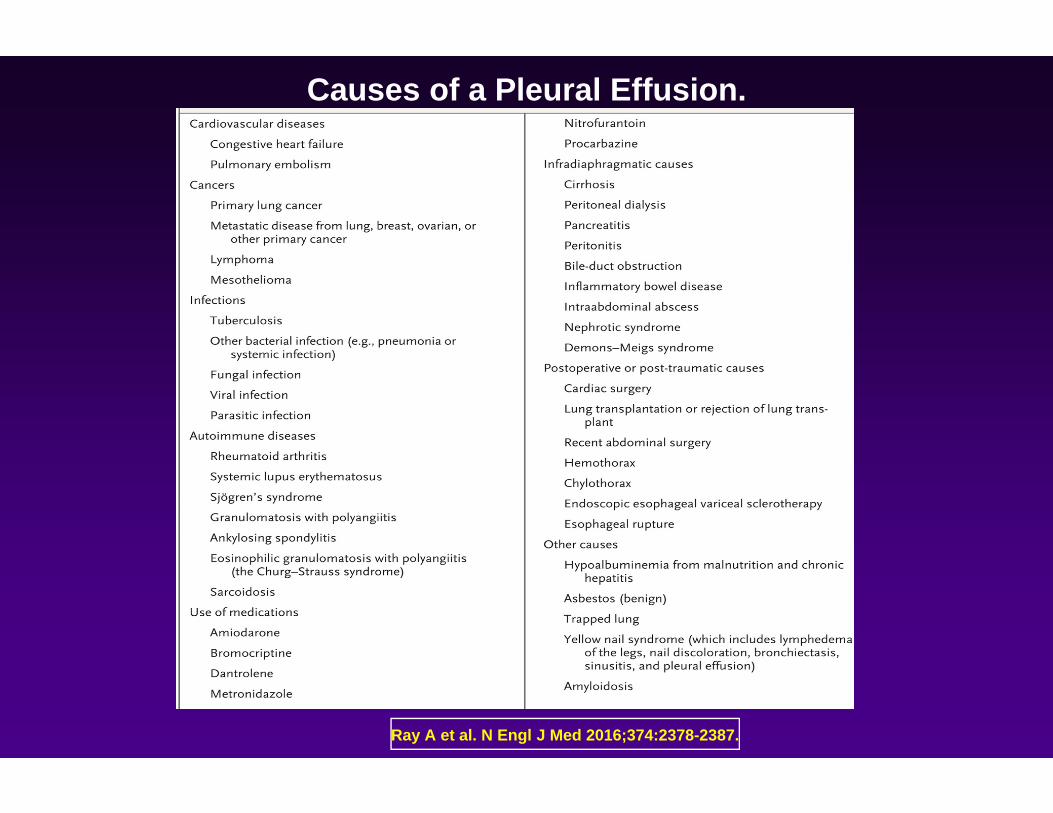
Ray A et al. N Engl J Med 2016;374:2378-2387.
Causes of a Pleural Effusion.

Exudate or Transudate?

Sahn SA. Am J Med Sci 2008;335:7-15
Diagnoses that can be established “definitively” by pleural fluid analysis

Question 3
• 36 y/o female presents with cough and mild dyspnea x 3 weeks.
• Seen by PCP 5 days ago and prescribed levofloxacin
• Denies fevers, chest pain, sputum, hemoptysis.
• PMHx: Nephrolithiasis treated previously with lithotripsy
• Meds: Tylenol as needed
• Exam: Afebrile, HR 98, 128/72, 94% (RA)
• CV: normal, no edema, flat neck veins
• Lungs: decreased BS Left base, adjacent crackles

Question 3What test would you request?
A. Chest CT scan
B. Chest ultrasound with thoracentesis
C. Pulmonary function testing
D. PET scan
E. Echocardiogram
Question 4What would you order on Pleural Fluid Analysis?
A. LDH, Albumin, Lipid analysis, cultures, glucose
B. Albumin, LDH, cholesterol, adenosine deaminase
C. LDH, Total Protein, Beta-2-transferrin, creatinine
D. LDH, Total Protein, pH, cultures, cytology, glucose, cell count
E. Anti-myocardial antibody, LE cells, RF, CRP, hematocrit, cell count

Light RW. N Eng J Med 2002;346:1971-77
Sensitivity of Tests to Distinguish Exudative from Transudative Effusions

Light RW. N Eng J Med 2002;346:1971-77
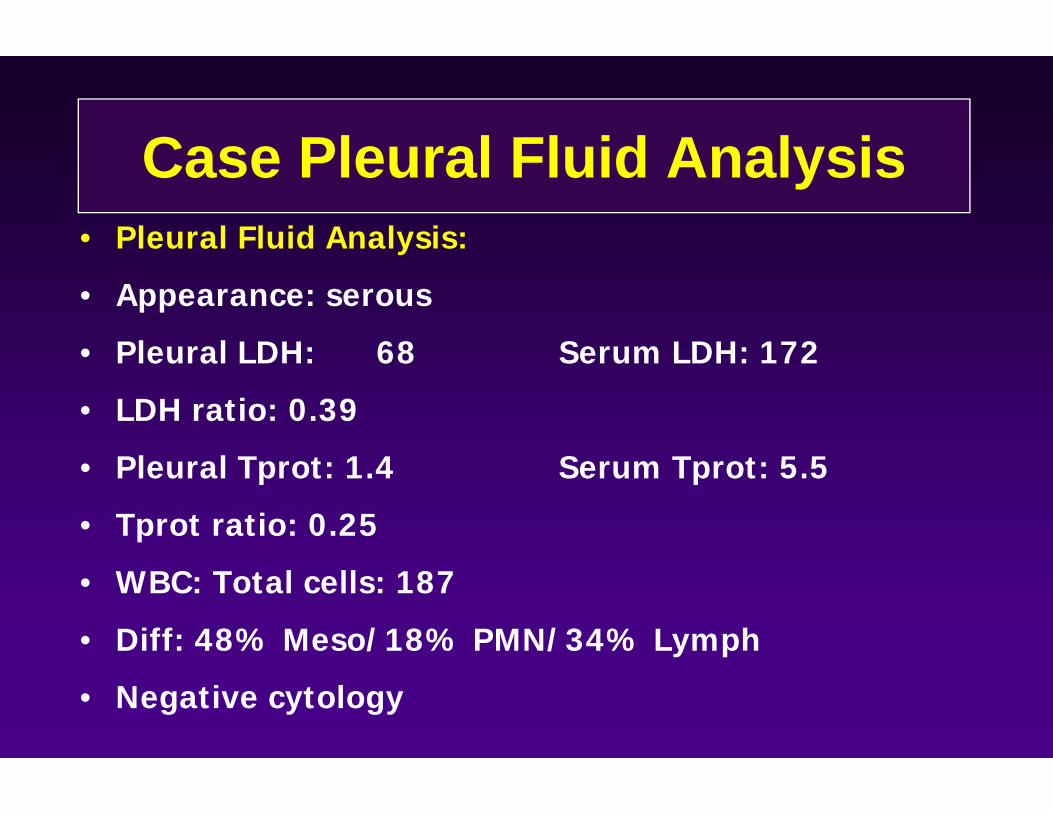
Case Pleural Fluid Analysis• Pleural Fluid Analysis:
• Appearance: serous
• Pleural LDH: 68 Serum LDH: 172
• LDH ratio: 0.39
• Pleural Tprot: 1.4 Serum Tprot: 5.5
• Tprot ratio: 0.25
• WBC: Total cells: 187
• Diff: 48% Meso/18% PMN/34% Lymph
• Negative cytology
Question 5Based on preliminary results, the most likely diagnosis is:
A. Parapneumonic effusion
B. Hepatic hydrothorax
C. Tuberculous effusion
D. Malignant pleural effusion
E. Chylothorax
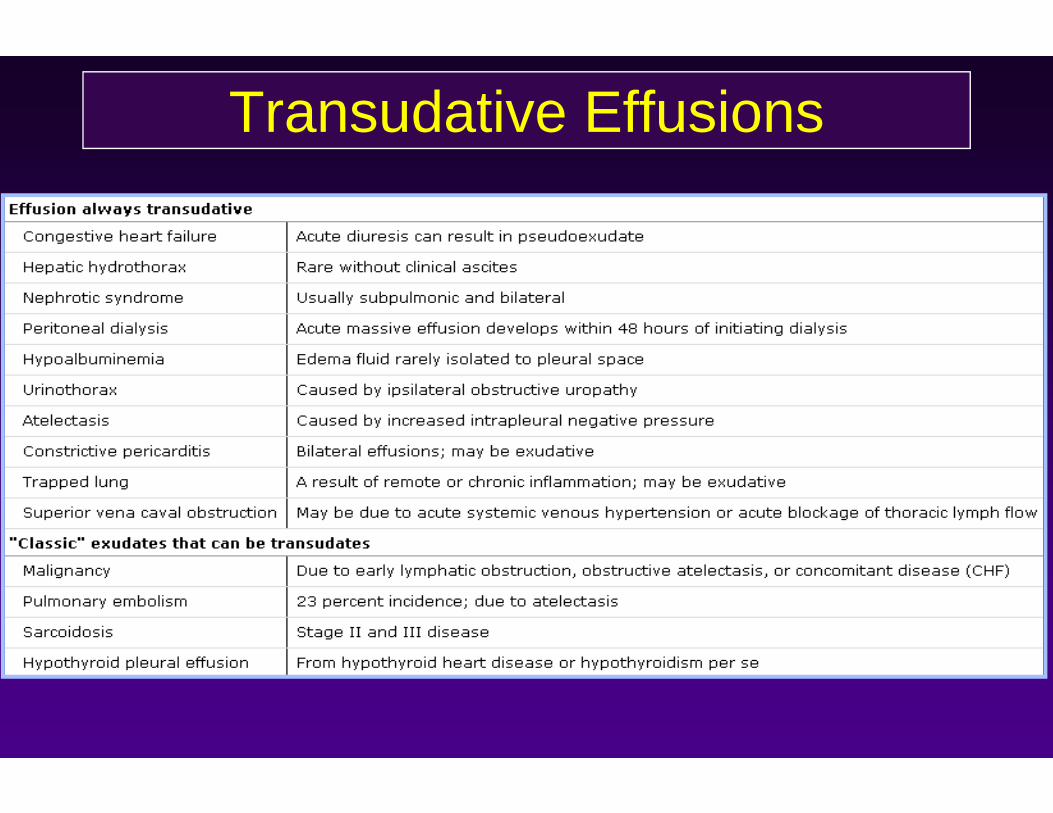
Transudative Effusions

Back to the case
Pleural Fluid Analysis:
• pH: 6.4 Glucose: 48
• Gram Stain: (-) Culture: NG

Question 6What additional tests might you add?
A. Adenosine Deaminase
B. LE cells
C. Beta-2-transferrin
D. Pleural and serum creatinine
E. Albumin
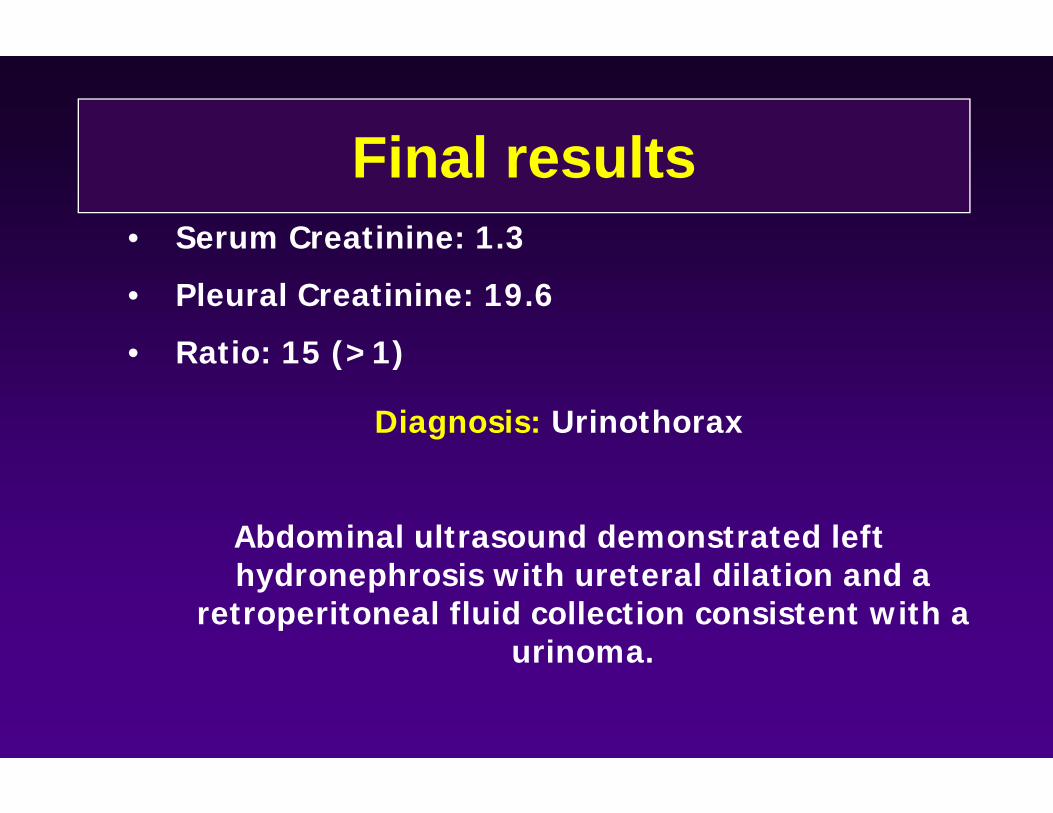
Final results• Serum Creatinine: 1.3
• Pleural Creatinine: 19.6
• Ratio: 15 (>1)
Diagnosis: Urinothorax
Abdominal ultrasound demonstrated left hydronephrosis with ureteral dilation and a
retroperitoneal fluid collection consistent with a urinoma.

Transudative Pleural Effusions1. Typically serous in appearance.
2. Caused by an imbalance of hydrostatic and oncotic forces.
3. Most commonly caused by CHF, less commonly due to hepatic or renal failure.
4. Least likely causes are urinothorax of duropleural fistula (although both can be definitively diagnosed by PFA).
5. Infrequently (3-10%) transudative effusions are malignant.
Question 7
• A 57-year-old male presented with dyspnea and dry cough, no fever
• Prior smoker (45 pack-years) • He was a construction worker and
specialized in insulation• No medications• No significant FHx

• ExamNormotensive, HR:92, SpO2 96% (RA)Lungs: decreased breath sounds right base to
mid lungENT: normalCV: normalNo L/AAbdomen benignNo edema
Question 7
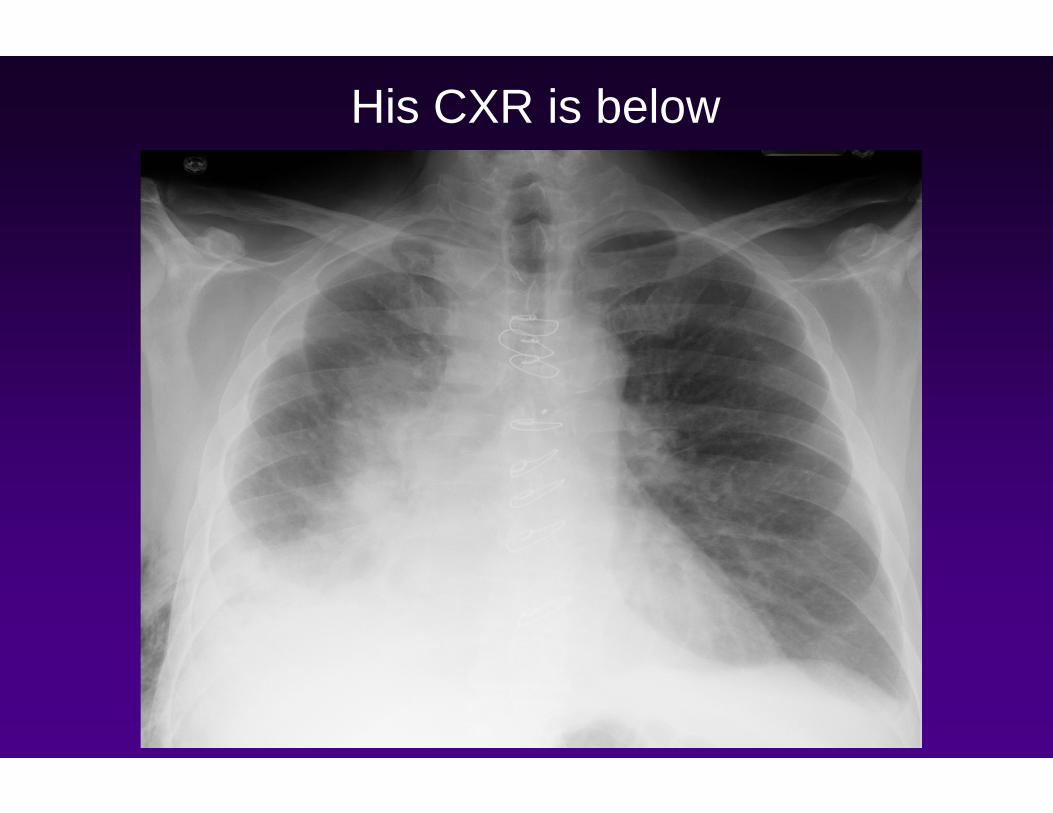
His CXR is below

Question 7
• He underwent three thoracenteses that showed an exudative effusion with lymphocytic predominance, normal pH and glucose, cultures and cytology were negative.
• US and CT of the Chest were done:

DiaphragmPleural fluid
Fibrin stranding

Bloody pleural effusion
Causes of Bloody Pleural Fluid
1. Malignancy
2. Benign Asbestos Pleural Effusion (BAPE, may also see elevated eosinophil count in 30%)
3. Post-cardiac injury syndrome
4. Pulmonary infarction
5. Trauma (especially if anticoagulated)
6. True hemothorax
7. Catamenial hemothorax

Question 7
What is the most appropriate next step:A. Repeat thoracentesisB. Aggressive diuresisC. Placement of an indwelling catheter
(Pleurx catheter)D. Thoracoscopic pleural biopsy
Question 8What is the most likely diagnosis?
A. Empyema
B. Congestive heart failure
C. Hemothorax
D. Malignant pleural effusion
E. IBD-associated lymphocytic pleuritis
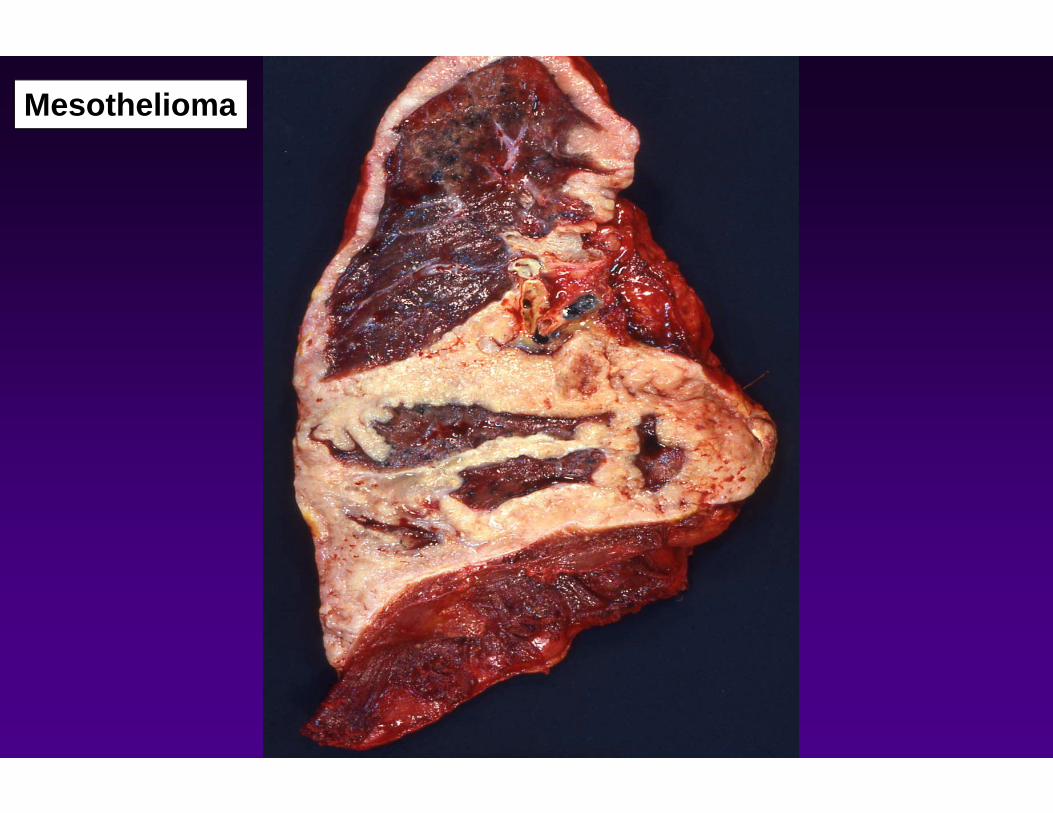
Mesothelioma
Pleural fluid cytology1. Positive 40-50% on first thoracentesis.
2. Yield improves with serial thoracenteses up to three (60% by third tap).
3. Yield does not increase with larger volume of pleural fluid tested.
4. Most common malignant etiologies: #1 lung, #2 breast, #3 lymphoma.
5. Should be sent:
A. All unilateral and bilateral effusions with normal heart size.
B. Patients over 40 or with risk factors
C. Etiology unclear
Exudative Pleural Effusions1. Appearance varies and may be helpful diagnostically.
2. Caused by inflammation and/or lymphatic obstruction.
3. Tend to be unilateral.
4. Massive effusions usually the result of carcinoma with contralateral shift seen typically in non-lung primary, no shift typically with lung primary of mesothelioma.
5. Whereas low pH (<7.3) or glucose (<60) in transudate is seen only in urinothorax, with exudate is seen in empyema, malignancy, esophageal rupture, RA/SLE pleuritis, tuberculous effusion.

Last case
• 72 y/o never smoker with h/o DM and GERD is evaluated in the ER due to progressive dyspnea, fever, chills and productive cough.
• Prescribed amoxicillin 4 days ago by her PCP but no improvement
• Medications: Metformin and ranitidine• PE: febrile, tachycardic, normotensive,
decreased BS in the right base

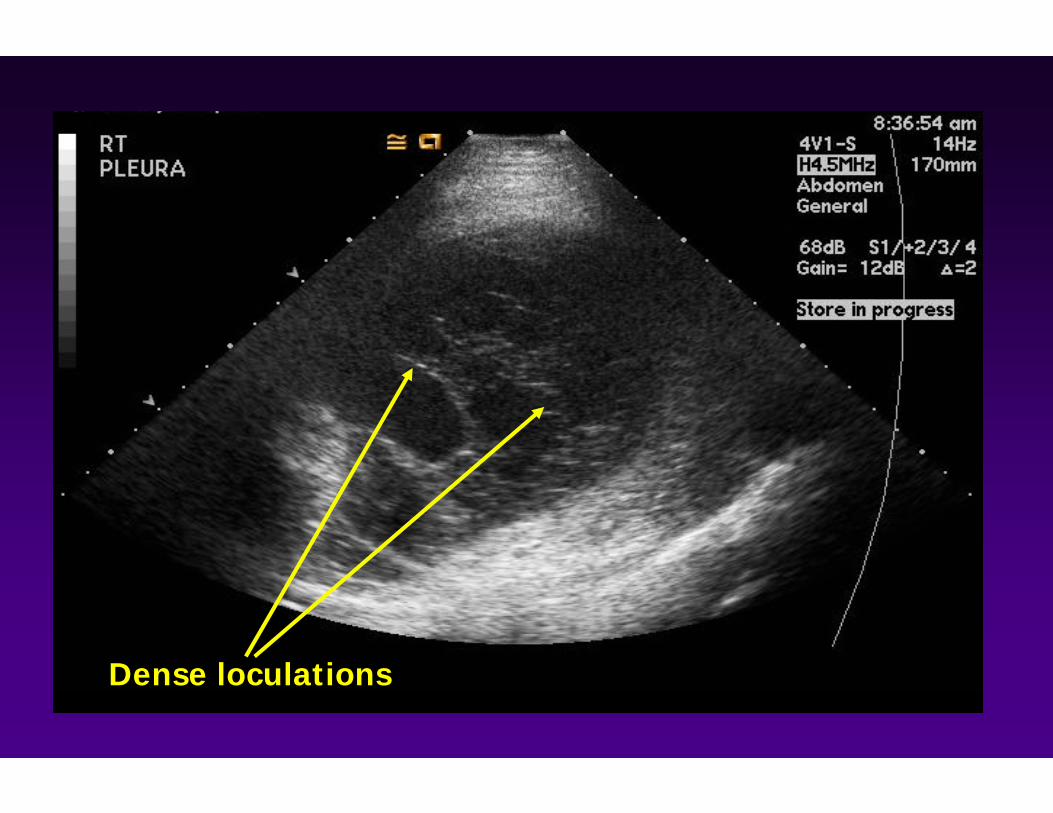
Dense loculations

Cloudy, greenish-yellow in color.
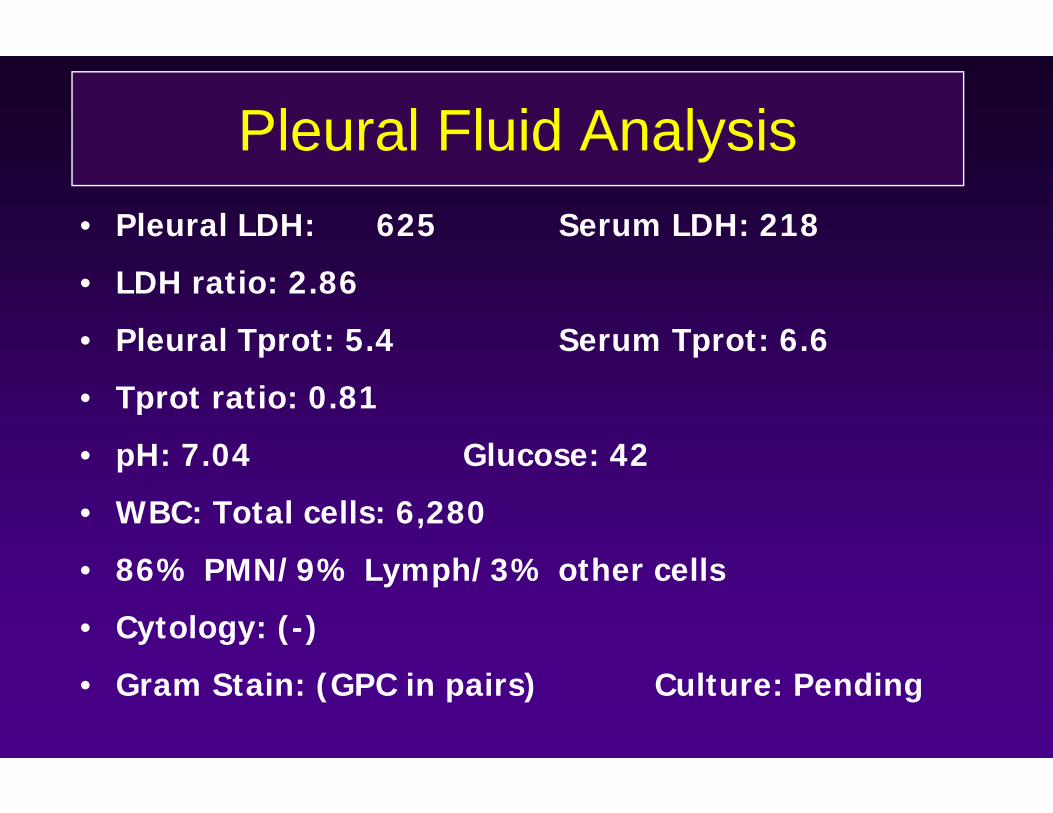
Pleural Fluid Analysis• Pleural LDH: 625 Serum LDH: 218
• LDH ratio: 2.86
• Pleural Tprot: 5.4 Serum Tprot: 6.6
• Tprot ratio: 0.81
• pH: 7.04 Glucose: 42
• WBC: Total cells: 6,280
• 86% PMN/9% Lymph/3% other cells
• Cytology: (-)
• Gram Stain: (GPC in pairs) Culture: Pending
Question 9What would you recommend to do in this case?
A. Schedule repeat chest ultrasound and thoracentesis in one week
B. Admit patient immediately, broaden antibiotics, place a chest tube on the right, consider intrapleural thrombolysis
C. Start patient on oral levofloxacin at 750mg/day and follow-up in three days
D. Outpatient follow-up with thoracic surgery to consider decortication electively.
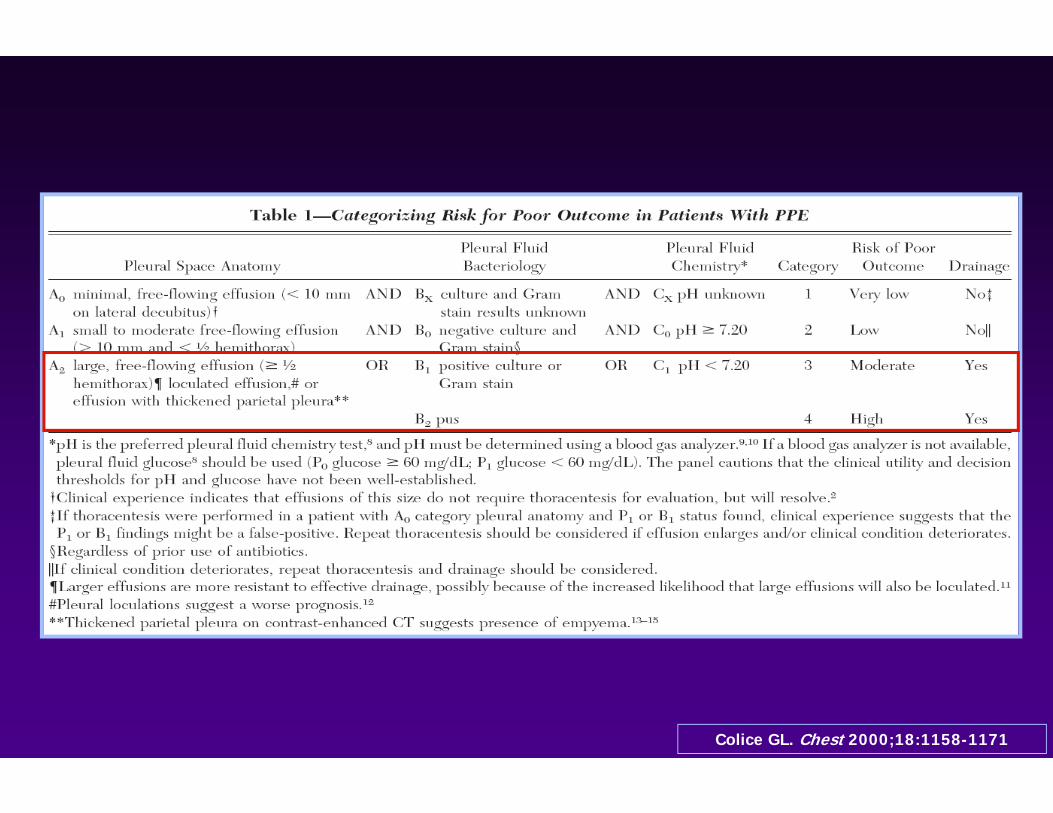
Colice GL. Chest 2000;18:1158-1171

• Intrapleural t-PA–DNase therapy improved fluid drainage in patients with pleural infection and reduced the frequency of surgical referral and the duration of the hospital stay
• Treatment with DNase alone or t-PA alone was ineffective.

Management of Plural Effusion
• Depends on the etiology: treat underlying cause
• Most of the data available are from malignant pleural effusions
• Serial thoracenteses, talc pleurodesis, abrasion pleurodesis and indwelling pleural catheter are the most common options

Pleural catheter for malignant effusion


Indwelling pleural catheters:
• Afford excellent symptom control• Appear cost effective in comparison to pleurodesis up to 6 months of therapy
• Generally can be placed in outpatient setting• Result in spontaneous pleurodesis in approximately 50% of all patients at 30‐50 days, 70% at 90 days in those fit for pleurodesis
• Appear to decrease subsequent hospitalization days relative to pleurodesis

Summary1. Light’s Criteria (pLDH/sLDH >0.6, pTProt/sTProt >0.5,
pLDH > 2/3 ULN serum LDH) is most sensitive method of identifying exudate
2. Specificity suffers especially in patients on diuretics. In that case, albumin gradient </= 1.2 is more specific.
3. CHF/liver disease/nephrotic syndrome most common transudates
4. Most common causes of exudates include infection, malignancy and inflammatory conditions
5. In complicated parapneumonic effusions, indication for drainage: pH <7.2, glucose < 60, loculations, positive gram stain
[email protected]©2010 MFMER | slide‐60