sars situation in guangdong and hospital infection control xiaoping tang, m.d, ph.d guangzhou no. 8...
TRANSCRIPT

SARS Situation in GuangdongSARS Situation in Guangdong and Hospital Infection Control and Hospital Infection Control
Xiaoping Tang, M.D, Ph.D
Guangzhou No. 8 People’s Hospital

Number Of SARS Patients and HCW Infection (AS of 8/7/2003) Cases Death (%) HCW(%) Last Report
Global 8422 916 11 1725(20) 7.13
China(Main) 5327 349 7 1002(19) 6.25
Guangdong 1512 58 4 346(23) 6.25
Hongkong 1755 300 17 386(22) 5.31
Taiwan 665 180 27 86(13) 6.15Canada 251 41 17 108(43) 6.12Singapore 283 33 14 97(41) 5.05


Foshan Cases
In November, 2002 A cluster of 5 cases of
Pneumonia from one family were hospitalized, 2 developed to RF
( First case : onset time Nov 16 )
Large shadows in Lungs No Response to
Antibiotics X-Ray

Heyuan Cases
• Mr. Huang, a restaurant cook, got sick on Dec.10 in Shenzhen
• admitted to Heyuan 1st Hospital on Dec.15, 2002
• A cluster of cases including 8 HCW happened
First case in Heyuan

Zhongshan Cases
• January 20, 20 cases were reported to Guangdong Health Bureau.
• Jan. 21, experts from Guangzhou, Foshan, Heyuan and China CDC had consultation together.


Guangzhou Super-spreader

90


Total Patients Received
• 1st patients: Feb 2, 2003
• Total : 413 probable & suspect cases
(262 confirmed )

5
118142
109
2743 52 47
30 33 3313
2 10
50
100
150
Number of Pati ents i n Hospi tal

Male 124
Female 138
Age 2-89 years old
average 41±18
SARS contacting history 175 (67.3%)
Incubation period 1-14 d
average 4.5 d
General Information

Clinical features (%) Hong KongLee et al(n=138)
TorontoBooth et al (n=144)
Hong KongPeiris et al
(n=50)
GuangzhouZhang et al
(n=260)
SingaporeHsu et al
(n=20)
Fever 100 99.3 100 100 100
Chills/rigor 73.2 27.8 74 51.2 15
Myalgia 60.9 49.3 54 26.5 45
Cough 57.3 69.4 62 72.7 75
Dyspnoea -- 41.7 20 75.4 40
Headache 55.8 35.4 20 26.5 20
Dizziness 42.8 4.2 12 46.5 --
Sputum 29.0 4.9 -- 11.5 --
Diarrhoea 19.6 23.6 10 24.2 25
Nausea & vomiting 19.6 19.4 20 -- 35
Sore throat 23.2 12.5 20 -- 25
Malaise -- 31.2 50 24.6 45
Presenting Symptoms

Laboratory Findings (1)
Leucocyte >10 ×109/L 38 (14.6%)
4.0~10 ×109/L 146 (56.2%)
< 4.0 ×109/L 76 (29.2%)
< 2.0 ×109/L 35 (13.5%)
Lymphocyte < 1.5 ×109/L 226 (86.9%)
Platelet < 10 ×109/L 25 (9%)
the lowest 2.5 ×109/L
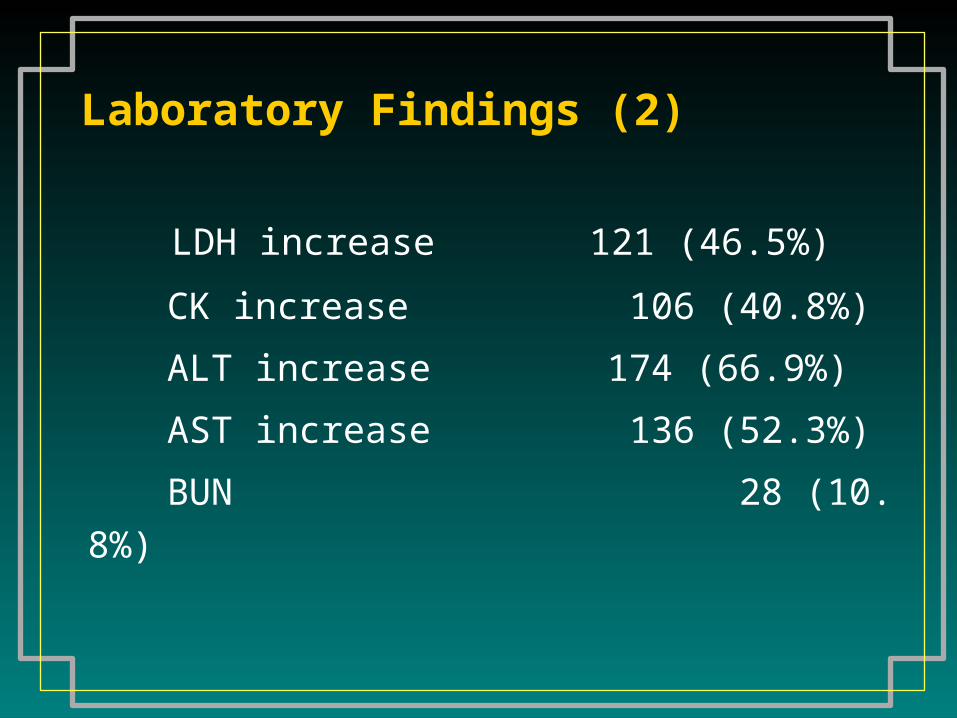
Laboratory Findings (2)
LDH increase 121 (46.5%)
CK increase 106 (40.8%)
ALT increase 174 (66.9%)
AST increase 136 (52.3%)
BUN 28 (10.8%)

CD4 + lymphocyte 475.6 ± 405.2/ul
< 400/ul 56/93 (60.2%)
< 200/ul 30/93 (32.3%)
the lowest 23/ul
SO2 < 95% 101 (38.8%)
Laboratory Findings (3)Laboratory Findings (3)

1527
787633
954
551
371472
244 202
0
200
400
600
800
1000
1200
1400
1600
1800
2000
2200
CD3+ CD4+ CD8+
Normal
Mild
Severe
T Lymphocyte Subtypes (1)
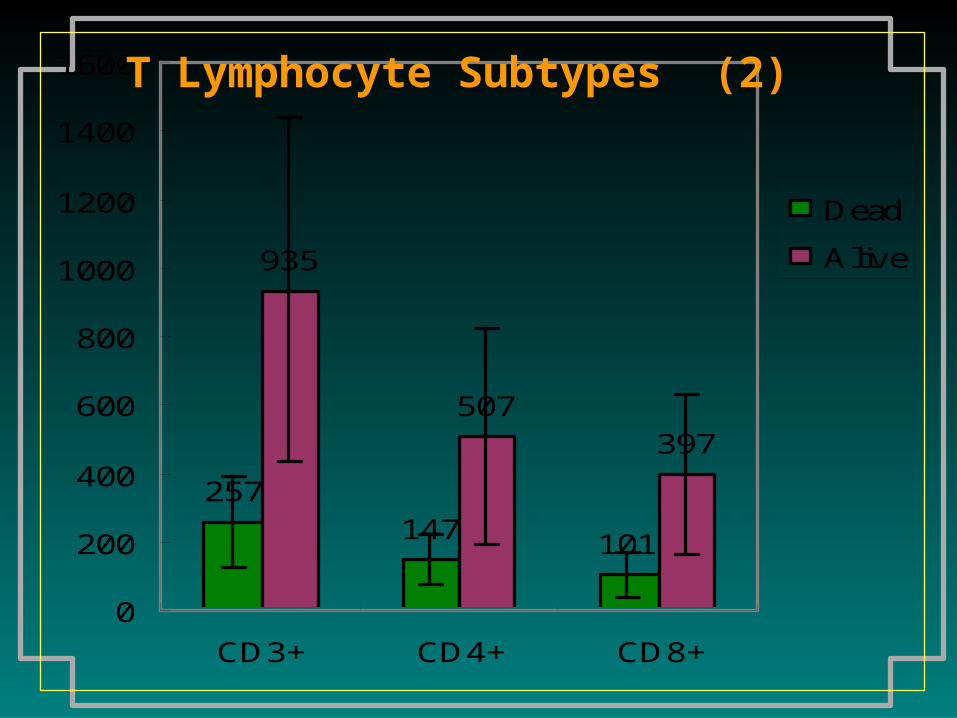
257147 101
935
507397
0
200
400
600
800
1000
1200
1400
1600
CD3+ CD4+ CD8+
Dead
Alive
T Lymphocyte Subtypes (2)

Chest X-ray
Interstitial damage 184 (70.7%)
Small patch-like or spotty shadow 195 (75%)
Large patch-like shadow 161 (61.9%)
Reticular opacities 93 (35.8%)
Both lung involvement 192 (73.8%)

Management
• Oxygen taking
• Antibiotics: empirically
• Anti-viral reagents : Ribavirin
• Glucocorticoid (Methyprednisolone)
• Artificial Ventilator support
Corticosteroid Management
Early systemic corticosteroid administrationAutopsy showed: hyalinization of airway basal membrane, alveolar fibrosis (similar to ARDS)
Indication:
High fever>3 days
Chest X ray deteriorates progressively

Dose of methylprednisolone in Guangzhou No.8 Hosp
• Dose of MP 140±123mg/d (40~500mg/d)
• Duration 14±12 days
• N=54

No-invasive Positive Pressure Ventilation (CPAP/BiPAP)
Indications:
1. RR>30times/min ;
2.SaO2< 93% when taking
oxygen 3-5L/min
3 、 Difficulty in breathing
No.8 Hosp. N=54/262
Average time of hospitalization
Common type 13.8 ± 3.5 d
Severe type 28.4 ± 10.3 d
Fatality rate 4.2% (12/260)
Prognosis
Mortality in Guangzhou
Total cases 1274
Dead 46 3.61%
70% (892 cases) with IgG titer 4 times higher than normal
Mortality 46/892 = 5.16%5.16%

Low mortality in Guangdong (why?) (1)
• Misdiagnosis
• Less worse epidemics
– Peak < 60 newly diagnosed pts/day
• Age distribution ?
• Fewer patients with underlying diseases?

Low mortality in Guangdong (why?) (2)
• Critical Cases
• Medical staff
• Guideline - better efficacy with combined man
agement (lower dose corticosteroid +CPAP/Bi
PAP)
referred to well-equipped referred to well-equipped
and well-trained hospitalsand well-trained hospitals

Distribution of death relating to age (n=931)
Age
(yrs)<15 15-20 20-30 30-40 40-50 50-60 60-70 >70 Total
Case 12 47 287 255 161 82 50 37 931
Death 0 0 1 5 13 5 7 4 35
% 0 0 0.4 2.0 8.1 6.1 14 11 3.7

Underlying Disease relating to death (n=931)
Total With underlying disease
No underlying disease
Case 931 190 (20.4%) 741 (79.6%)
Death 35 15 20
% 3.7 7.9 2.7
Underlying diseases—Diabetes, COPD, chronic asthma, cancer, chronic renal disease, hypertension, pulmonary TB, chronic hepatitis, chronic heart failure, etc

A comparison of Intubation Rate and Crude Fatality Rate in SARS patients
NNCPAPCPAP
(BiPAP)(BiPAP)IntubationIntubation FatalityFatality
Hong Kong 175535
(2.0%)
246
(14.0%)
300
(17.1%)
Guangzhou 528122
(23.1%)
39
(7.4%)
29
(5.5%)
P
(X2 test)
<0.001
(228.3)
<0.001
(16.3)
<0.001
(43.6)

Hospital Infection Control

Number Of SARS Patients and HCW Infection (AS of 8/7/2003) Cases Death (%) HCW(%) Last Report
Global 8422 916 11 1725(20) 7.13
China(Main) 5327 349 7 1002(19) 6.25
Guangdong 1512 58 4 346(23) 6.25
Hongkong 1755 300 17 386(22) 5.31
Taiwan 665 180 27 86(13) 6.15Canada 251 41 17 108(43) 6.12Singapore 283 33 14 97(41) 5.05



Medical Staff Infection in Our Hospital
• Total 20 (8 doctors, 12 nurses)
• Happened during the time when there
were most patients ( from Feb. 12 to
Feb.19 )
• All recovered

After Bitter Experiences
More Strict Hospital Preventive
Measures were Taken by Medical Staff




Separated Fever Clinic










Thank You !