second edition d second e d it ion community-based...
TRANSCRIPT

COM M U N I T Y-BA SE D
PA RT ICI PATORY HEALTH RESEARCH
S e c o n d E d i t i o n
E D I T O R S
DANIEL S. BLUMENTHAL
RALPH J. DICLEMENTE
RONALD L. BRAITHWAITE
SELINA A. SMITH
BLU
ME
NT
HA
L
DIC
LE
ME
NT
E
BR
AIT
HW
AIT
E
SMIT
H
CO
MM
UN
ITY
-BA
SE
D
PA
RT
ICIP
AT
OR
Y
HE
AL
TH
RE
SEA
RC
HSecond Edition
9 780826 193964
ISBN 978-0-8261-9396-4
11 W. 42nd StreetNew York, NY 10036-8002 www.springerpub.com
“The editors of this book bring together in one place both a description of epidemio-logical methods and a discussion of community-level issues. It is a volume that will prove useful to those who wish to conduct contemporary community-based research.”
–Praise for the First Edition from the ForewordDavid Satcher, Former Surgeon General of the United States
This second edition of a highly regarded textbook on the foundations of and strategies for achieving fertile community-based health care research has been completely revised and updated. It now includes new chapters on translating research into practice, evaluat-ing research, and applying community-based participatory research (CBPR) principles to service, education, and evaluation. The book also updates a crucial chapter on the voices of community stakeholders and an important study of the ethical issues surrounding the Tuskegee Syphilis Study. Edited by renowned professors of community-based research, the text is distinguished by its how-to approach and focus on practical research methods.
The text discusses the unique challenges of conducting CBPR and addresses ways to build and sustain community partnerships. It explores ethical issues regarding health care research, includes input from community stakeholders, and describes national and interna-tional support for CBPR. Research methods covered include qualitative studies, surveys, and intervention trials. Applications of CBPR illustrate how to translate research into practice and community-based participatory approaches to service, education, and evaluation.
The second edition includes new chapters on:
� Building and sustaining researcher/community partnerships� National and international investments in and support for CBPR� Surveys and methods for conducting CBPR� Translating research into practice� Community-based participatory approaches to service, education, and evaluation
COM M U N I T Y-BA SE D PA RT ICI PATORY HEALTH RESEARCH
Issues, Methods, and Translation to Practice
Issues, Methods, and Translation to Practice
S e c o n d E d i t i o n
E D I T O R S
DANIEL S. BLUMENTHAL, MD, MPH, RALPH J. DICLEMENTE, PhD,
RONALD L. BRAITHWAITHE, PhD, SELINA A. SMITH, PhD, MDiv

COMMUNITY-BASED PARTICIPATORYHEALTH RESEARCH
Daniel S. Blumenthal, MD, MPH, is a graduate of Oberlin College and the School of Medicineat the University of Chicago. He completed his residency in pediatrics at Charity Hospital ofNew Orleans (Tulane Division) and received his master of public health degree from EmoryUniversity. He is board certified in both pediatrics and preventive medicine. He has servedas a VISTA volunteer physician in Lee County, Arkansas; as an Epidemic IntelligenceService officer with the Centers for Disease Control and Prevention in Atlanta; and as amedical epidemiologist with the World Health Organization Smallpox Eradication Programin India and Somalia. He was on the faculty of the Emory University School of Medicineand has been at Morehouse School of Medicine (MSM) since 1980, where he served as foundingchair of the Department of Community Health and Preventive Medicine from 1984 to 2009.He is currently associate dean for community health. He is a recipient of the Georgia PublicHealth Association’s Sellers-McCroan Award “for outstanding achievement and service toGeorgia in public health.” He was named the Outstanding VISTA Volunteer of the 1960s.He received a “Shining Light” Award from the Georgia Association for Primary HealthCare and the Leonard Tow Humanism in Medicine Award from MSM. He was the 2010 reci-pient of the Duncan Clark Award from the Association for Prevention Teaching and Research,the association’s highest award.
Ralph J. DiClemente, PhD, is Charles Howard Candler professor of public health and associ-ate director, Emory/Atlanta Center for AIDS Research. He holds concurrent appointments asprofessor in the Emory University School of Medicine, the Department of Pediatrics, in the Div-ision of Infectious Diseases, Epidemiology, and Immunology, and the Department of Medicine,in the Division of Infectious Diseases, and the Department of Psychiatry. He was most recently,chair, Department of Behavioral Sciences and Health Education at the Rollins School of PublicHealth, Emory University. Dr. DiClemente was trained as a health psychologist at the Univer-sity of California San Francisco where he received his PhD in 1984 after completing a master ofscience in behavioral sciences at the Harvard School of Public Health and his undergraduatedegree at the City University of New York.
Ronald L. Braithwaite, PhD, is a professor in the Departments of Community Health and Pre-ventive Medicine, Family Medicine, and Psychiatry at Morehouse School of Medicine. He has aPhD in educational psychology from Michigan State University. He currently serves as thedirector of the Center of Excellence for Health Disparities Research and core research directorof the Prevention Research Center at Morehouse School of Medicine. He carried out postdoc-toral studies at Howard University, Yale University, and the University of Michigan School ofPublic Health and Institute for Social Research. He is also a visiting professor in the School ofMedicine at the University of Cape Town. His research involves HIV and substance use inter-vention studies with juveniles and adults in correctional systems. He has widely publishedpapers in education and health journals and is the coeditor of Health Issues of IncarceratedWomen; Health Issues in the Black Community (first, second, and third editions); coauthor ofPrison and AIDS: A Public Health Challenge, and Building Health Coalitions in the Black Community.
Selina A. Smith, PhD, MDiv, has worked in cancer and community-based participatoryresearch for the past 19 years. She holds a bachelor of science in food and nutrition fromFlorida State University, a master of science from Florida International University, and a doc-torate in human nutrition, Howard University. She also earned a master of divinity degreefrom Emory University in 2005. Her specific areas of research include translational research,health disparities research, cancer epidemiology, and cancer control and prevention. Beforejoining the faculty of Morehouse School of Medicine’s (MSM) Department of CommunityHealth and Preventive Medicine in 1998, Dr. Smith was a faculty member at the Universityof Miami School of Medicine and Georgetown University College of Medicine. She currentlyserves as deputy director of the MSM Cancer Research Program and principal investigator ofthe MSM component of the MSM/TU/UAB Cancer Center Partnership. She is also lead prin-cipal investigator on the Efficacy-to-Effectiveness Translation of an Educational Program toIncrease Colorectal Cancer Screening study.
COMMUNITY-BASED PARTICIPATORY
HEALTH RESEARCH
ISSUES, METHODS, AND TRANSLATION
TO PRACTICE
SECOND EDITION
Daniel S. Blumenthal, MD, MPH
Ralph J. DiClemente, PhD
Ronald L. Braithwaite, PhD
Selina A. Smith, PhD, MDiv
Editors

Copyright # 2013 Springer Publishing Company, LLC
All rights reserved.
No part of this publication may be reproduced, stored in a retrieval system, or transmitted inany form or by any means, electronic, mechanical, photocopying, recording, or otherwise,without the prior permission of Springer Publishing Company, LLC, or authorization throughpayment of the appropriate fees to the Copyright Clearance Center, Inc., 222 Rosewood Drive,Danvers, MA 01923, 978-750-8400, fax 978-646-8600, [email protected] or on the Web atwww.copyright.com.
Springer Publishing Company, LLC11 West 42nd StreetNew York, NY 10036www.springerpub.com
Acquisitions Editor: Sheri W. SussmanProduction Editor: Joseph StubenrauchComposition: Techset
ISBN: 978-0-8261-9396-4e-book ISBN: 978-0-8261-9397-1
13 14 15 / 5 4 3 2 1
The author and the publisher of this Work have made every effort to use sources believed to bereliable to provide information that is accurate and compatible with the standards generallyaccepted at the time of publication. The author and publisher shall not be liable for any special,consequential, or exemplary damages resulting, in whole or in part, from the readers’ use of, orreliance on, the information contained in this book. The publisher has no responsibility for thepersistence or accuracy of URLs for external or third-party Internet websites referred to in thispublication and does not guarantee that any content on such websites is, or will remain,accurate or appropriate.
Library of Congress Cataloging-in-Publication Data
Community-based participatory health research : issues, methods, and translation to practice /edited by Daniel S. Blumenthal . . . [et al.]. — 2nd ed.
p. ; cm.Includes bibliographical references and index.ISBN 978-0-8261-9396-4 — ISBN 978-0-8261-9397-1 (e-book)I. Blumenthal, Daniel S.[DNLM: 1. Community-Based Participatory Research. 2. Community-Institutional
Relations. 3. Research Design. W 84.3]204′.47—dc23
2012046370
Special discounts on bulk quantities of our books are available to corporations,professional associations, pharmaceutical companies, health care organizations, and otherqualifying groups. If you are interested in a custom book, including chapters from morethan one of our titles, we can provide that service as well.
For details, please contact:Special Sales Department, Springer Publishing Company, LLC11 West 42nd Street, 15th Floor, New York, NY 10036-8002Phone: 877-687-7476 or 212-431-4370; Fax: 212-941-7842E-mail: [email protected]
Printed in the United States of America by Gasch Printing.

The editors would like to acknowledge, and dedicate this book to,the many communities with which we have partnered in
conducting projects over the years. We hope that the work thatwe have done together has resulted in improved health and
quality of life in those communities.


CONTENTS
Contributors ixForeword Regina M. Benjamin, MD, MBA, Eighteenth U.S. Surgeon
General xiiiPreface xv
Part I: Issues
1. Community-Based Participatory Research: An IntroductionDaniel S. Blumenthal, Ernest Hopkins III, and Elleen Yancey 1
2. Building Partnerships in Community-Based Participatory ResearchJames P. Griffin, Jr., Elleen Yancey, andElizabeth Armstrong-Mensah 19
3. Community-Based Participatory Research Use or Abuse: TheU.S. Public Health Service Syphilis Study at TuskegeeRueben C. Warren, Bailus Walker, Jr., Lanice C. Middleton,and Louis A. Rabb 35
4. A View From the Community: African American, Hispanic, andAfrican Immigrant PerspectivesFred Murphy, Andrea Hinojosa, and Sirad Osman 51
5. Public and Private Investments and Resources for Community-BasedParticipatory ResearchMichelle C. Kegler, Diane Fletcher, Sally Honeycutt,and Amanda Wyatt 79
Part II: Methods
6. Qualitative Research in CBPRFleda M. Jackson, Ama Saran, Patricia Graham Johnson,and Selma J. Morris 111
vii

7. Survey Planning and Implementation in the Context of CBPRRobert M. Mayberry, Pamela Daniels, Anya Bazzell, Fengxia Yan,Robina Josiah Willock, and Barbara Mack 131
8. Intervention Trials in Community-Based Participatory ResearchScott D. Rhodes, Stacy Duck, Jorge Alonzo, Mario Downs, andRobert E. Aronson 157
9. Translating Research to PracticeSelina A. Smith and Daniel S. Blumenthal 181
10. Community-Based Participatory Approaches to Service:Lessons LearnedMary Langley, Roland Bernard Welmaker, Sr., Alice Jackson,and Angela M. Mack 195
11. Community-Based Approaches to EducationMeryl McNeal, Daniel S. Blumenthal, Kendrea Williams Pierson,Chad Hale, and Theresa Rogers 215
12. Community-Based Participatory Approaches to EvaluationTabia H. Akintobi, Jennie C. Trotter, Donoria Evans, Nastassia Laster, andTarita Johnson 231
Index 263
viii Contents

CONTRIBUTORS
Tabia H. Akintobi, PhD, MPH, Research Associate Professor, CommunityHealth and Preventive Medicine; Director, Prevention Research Center, MorehouseSchool of Medicine, Atlanta, GA
Jorge Alonzo, JD, Project Manager, Department of Social Sciences and HealthPolicy, Wake Forest School of Medicine, Winston-Salem, NC
Elizabeth Armstrong-Mensah, PhD, Instructor, Community Health and PreventiveMedicine, Morehouse School of Medicine, Atlanta, GA
Robert E. Aronson, DrPH, MPH, Associate Professor, Department of PublicHealth Education, School of Health and Human Performance, University ofNorth Carolina at Greensboro, Greensboro, NC
Anya Bazzell, MPH, Morehouse School of Medicine, Atlanta, GA
Daniel S. Blumenthal, MD, MPH, Professor, Community Health and PreventiveMedicine, Morehouse School of Medicine, Atlanta, GA
Pamela Daniels, MBA, MPH, PhD, Research Assistant Professor, CommunityHealth and Preventive Medicine, Morehouse School of Medicine, Atlanta, GA
Mario Downs, Project Coordinator, Department of Social Sciences and HealthPolicy, Wake Forest School of Medicine, Winston-Salem, NC
Stacy Duck, BS, Executive Director, Chatham Social Health Council, Silver City, NC
Donoria Evans, MPH, Assistant Director, Evaluation, Community Health andPreventive Medicine; and Prevention Research Center, Morehouse School ofMedicine, Atlanta, GA
Diane Fletcher, MA, BSN, RN, Chief Executive Officer, Cancer Coalition of SouthGeorgia, Albany, GA
James P. Griffin, Jr., PhD, Research Associate Professor, Community Health andPreventive Medicine, Morehouse School of Medicine, Atlanta, GA
Chad Hale, Executive Director, Georgia Avenue Community Ministry, Atlanta, GA
ix

Andrea Hinojosa, Executive Director, Southeast Georgia Communities Project,Lyons, GA
Sally Honeycutt, MPH, Evaluation Team Lead, Emory Prevention Research Center,Rollins School of Public Health, Emory University, Atlanta, GA
Ernest Hopkins III, Phoenix Foundation, Atlanta, GA
Alice Jackson, BS, ICPS, Program Coordinator, Community Health and PreventiveMedicine, Morehouse School of Medicine, Atlanta, GA
Fleda M. Jackson, PhD, MS, Senior Fellow, National Center for Health BehavioralChange, Morgan State University, Baltimore, MD
Patricia Graham Johnson, MSW, Retired Director, Office of Alumnae Affairs,Spelman College, Atlanta, GA
Tarita Johnson, MSW, Junior Deputy Director, Wholistic Stress Control Institute,Incorporated, Atlanta, GA
Michelle C. Kegler, DrPH, MPH, Director, Emory Prevention Research Center,Associate Professor, Department of Behavioral Sciences and Health Education,Rollins School of Public Health, Emory University, Atlanta, GA
Mary Langley, PhD, MPH, RN, ICPS, Director, Health Promotion Resource Center,Associate Professor, Community Health and Preventive Medicine, MorehouseSchool of Medicine, Atlanta, GA
Nastassia Laster, MPH, ORISE Fellow, Office of Public Health Preparedness andResponse, Centers for Disease Control and Prevention, Atlanta, GA
Angela M. Mack, BS, Executive Director, Lamar Co. Activity Center, Inc.,Barnesville; Program Coordinator, Health Promotion Resource Center, MorehouseSchool of Medicine, Atlanta, GA
Barbara Mack, Community Health Worker, Morehouse School of Medicine,Atlanta, GA
Robert M. Mayberry, MS, MPH, PhD, Research Professor, Community Health andPreventive Medicine, Morehouse School of Medicine, Atlanta, GA
Meryl McNeal, PhD, MA, Professor, Community Health and Preventive Medicine,Morehouse School of Medicine, Atlanta, GA
Lanice C. Middleton, Tuskegee, AL
Selma J. Morris†
Fred Murphy, MSPHyg, MPIA, Executive Director, Lifelong Health, Inc., Rex, GA
†Deceased.
x Contributors
Sirad Osman, PhD, New Americans Community Services, St. Paul, MN
Kendrea Williams Pierson, MA, Atlanta, GA
Louis A. Rabb, BA, MA, MHA, Tuskegee, AL
Scott D. Rhodes, PhD, MPH, Professor, Department of Social Sciences andHealth Policy, Section on Infectious Diseases, Wake Forest School of Medicine,Winston-Salem, NC
Theresa Rogers, Volunteer Health Coordinator, Saint Anthony of Padua CatholicChurch, Atlanta, GA
Ama Saran, PhD, MSW, Senior Fellow, National Center for Health BehavioralChange, Morgan State University, Baltimore, MD
Selina A. Smith, PhD, MDiv, Professor, Community Health and PreventiveMedicine, Morehouse School of Medicine, Atlanta, GA
Jennie C. Trotter, MEd, Executive Director and Founder, Wholistic Stress ControlInstitute, Incorporated, Atlanta, GA
Bailus Walker, Jr., PhD, MPH, Professor of Environmental and OccupationalMedicine and Toxicology, Howard University College of Medicine, Washington, DC
Rueben C. Warren, DDS, MPH, DrPH, MDiv, Professor of Bioethics, TuskegeeUniversity, Director of the National Center for Bioethics in Research and HealthCare, Tuskegee, AL
Roland Bernard Welmaker, Sr., MSLS, PhD, Librarian/Archivist/ResearchInstructor, Community Health and Preventive Medicine, Morehouse School ofMedicine Library, Atlanta, GA
Robina Josiah Willock, MPH, PhD, Instructor, Community Health and PreventiveMedicine, and Research Associate, Clinical Research Center, Morehouse School ofMedicine, Atlanta, GA
Amanda Wyatt, MPH, Research Project Coordinator, Emory Prevention ResearchCenter, Rollins School of Public Health, Emory University, Atlanta, GA
Fengxia Yan, MD, MS, Assistant Professor, Clinical Research Center, MorehouseSchool of Medicine, Atlanta, GA
Elleen Yancey, PhD, Associate Clinical Professor, Community Health andPreventive Medicine, Morehouse School of Medicine, Atlanta, GA
Contributors xi


FOREWORD
Community-based participatory research (CBPR) has become the preferredmodel for conducting research in communities. Most scientists whoconduct such research now recognize that working in partnership withthe community is preferable, and more ethical, than conducting researchon a community. Involving the community directly in a research projectoften results in better research and offers the researcher smoother sailingin carrying out the project. In addition, CBPR provides low-income andminority communities a voice and a capacity that they have not had inthe past. There are now several textbooks that provide guidance on con-ducting CBPR, including this one.
As Surgeon General of the United States, I direct a number of pro-grams aimed at encouraging Americans to avoid tobacco, engage in phys-ical activity, consume more nutritious diets, and protect their health inother ways. We need more effective methods to persuade, motivate, andenable individuals and communities to adopt these healthier lifestyles,and it is through CBPR that we will be able to discover these methods.
The United States Public Health Service, through several HHSagencies, has recognized the growing importance of the CBPR approach,and has funded a number of research centers and individual projects toconduct CBPR. For instance, the Centers for Disease Control and Preven-tion (CDC) supports 37 Health Promotion and Disease Prevention ResearchCenters (PRCs) at schools of public health and medical schools acrossthe country. These centers focus primarily on CBPR and conduct avariety of projects, funded by the CDC, as well as other agencies that usethis approach.
The National Institute on Minority Health and Health Disparities(NIMHD), one of the National Institutes of Health (NIH), has funded a sub-stantial number of projects under its CBPR initiative on reducing and elim-inating health disparities. This initiative has three phases, including a
xiii

3-year planning grant, a 5-year intervention grant, and a 3-year informationdissemination grant. Hence, a single project may be funded for up to 11years. This initiative is unique not only in the potential duration ofsupport for a project, but also in the opportunity it provides the communityto identify the topic to be researched.
Since 2004, the Office of Behavioral and Social Science Research(OBSSR) at NIH has issued several Funding Opportunity Announcements(FOAs) on community participation in research, with funding from severalof the NIH institutes. These FOAs have primarily solicited applications forR01 grants, the most rigorous and competitive of NIH awards, indicatingNIH recognition that CBPR can be as scientifically sound as any othertype of research. And the most recent FOAs specify that applicationsshould target the medically underserved, recognizing the importance ofthis type of research in reducing and eliminating health disparities.
These and other initiatives that promote CBPR are what is needed inorder to find practical and effective strategies to change our national healthcare focus from one of sickness and disease to one of wellness and preven-tion. By improving the health of individuals and communities, we canbecome a more healthy and fit nation.
Regina M. Benjamin, MD, MBAEighteenth U.S. Surgeon General
xiv Foreword

PREFACE
This is the second edition of a book that was first published in 2004. The titleof the first edition was Community-Based Research for Health. Since that time,community-based participatory research (CBPR)—which was barely men-tioned by name in the first edition—has clearly emerged as the model ofchoice for conducting research in communities.
After a slow start, CBPR has been gaining currency as a researchapproach since the middle of the first decade of the 21st century. APubMed search using the term “community-based participatory research”turns up 2,333 citations (through November 2012), with the first appearingin 1989. The figure below demonstrates how the number of CBPR publi-cations has grown from 2001 through 2012.
Interestingly, the figure takes the form of a typical sigmoid growthcurve common to many biological phenomena. After a lengthy lag phase,
Number of publications identified with the search term“community-based participatory research” on PubMed, 2001–2012
xv

the publication rate had an exponential “growth spurt” from 2007 to 2010,and then returned to a rate of growth similar to the initial phase.
One of the guiding principles of CBPR is that the community shouldbe a partner in every phase of a research project—from defining theproblem to be researched to disseminating the results of the study. Wehave taken the principle one step further, and added “to writing thebook about CBPR.” Hence, most chapters in this book have one or morecommunity partners—that is, community representatives without aca-demic positions—as coauthors. One chapter (Chapter 4, “A View Fromthe Community: African American, Hispanic, and African ImmigrantPerspectives”) was entirely written by community representatives. Wehave also included case studies in most of the chapters in an effort todemonstrate how the principles of CBPR can be, and have been, put touse in the real world.
In a past era, we often heard references to a “community laboratory”or a “community classroom.” Sometimes we still hear those references.However, we believe that the community is not a laboratory; to view itthat way reduces the people who live there to the status of guinea pigs.Similarly, we do not subscribe to the view of the community as a classroom;this approach reduces the people who live in the community to the status ofprops for a teaching exercise. The third leg of the academic “stool” (besidesresearch and education) is service, and in the same spirit, we recognize thatthe community is not a charity case; this view robs people of their dignity.
Rather, in research, education, or service, the community should be apartner, with benefits accruing to both the academic and communitymembers of the partnership. Since the principles of partnership apply toeducation and service as well as research, we have included chapters oncommunity-based participatory education and community-based partici-patory service. And since evaluation is important in all three domains,we have included a chapter on community-based participatory evaluation.
This is a volume on both “issues” and “methods.” The issues sectionfocuses on principles and perspectives that are always “on the table” in anydiscussion of CBPR. The methods section provides practical guidelines forconducting CBPR using a variety of research designs. In any edited work,there is the potential for discontinuity, but as editors, we hope that we haveproduced an integrated volume that will help the student, the researchscientist, or the interested citizen understand and apply the principles ofcommunity-based participatory research.
Daniel S. Blumenthal, MD, MPHRalph J. DiClemente, PhD
Ronald L. Braithwaite, PhDSelina A. Smith, PhD, MDiv
xvi Preface

CHAPTER ONE
COMMUNITY-BASED PARTICIPATORY RESEARCH:AN INTRODUCTION
Daniel S. Blumenthal, Ernest Hopkins III, and Elleen Yancey
In this chapter, we first consider community-based research generally, andthen turn our attention to community-based participatory research.
COMMUNITY-BASED RESEARCH
Community-based research (whether “participatory” or not) is scientificinquiry involving humans that takes place in the community—that is,outside of the laboratory, hospital, or clinic setting. It is the “fourth estate”of research, assuming its station relatively recently alongside basic, clinical,and health services research. It guides public health workers engaged inimproving the health of populations, just as traditional clinical researchguides the actions of clinicians in caring for individual patients.
Beyond the aspect of location, community-based research is definedby several other concepts:
Prevention focus: Community-based research may describe the epide-miology of a disease or condition, identify risk factors, or test ahealth promotion intervention, but (unlike laboratory- or hospital-/clinic-based research) it does not generally evaluate new modes oftherapy. Health problems can be identified and assessed on acommunity-wide basis; prevention-related interventions or policiescan be tested across a community; but, in general, treatment ofdisease can only be delivered and evaluated on an individual basis.
Population centered: Community-based research focuses on a popu-lation rather than on individuals. The population that is the unitof interest may be a geographically defined community, a groupwith a common personal characteristic (i.e., age, race, sex, occu-pation), or a group with a common modifiable risk factor (i.e.,tobacco use, risky sexual behavior). If the study involves a healthpromotion intervention, the intervention may be directed at one
1

individual at a time, but the analysis is still done by considering thepopulation as a whole.
Multidisciplinary approach: The methods of community-based researchinclude those of the biomedical sciences, the behavioral sciences,and the social sciences, and approaches from more than onediscipline are often combined in a single project. Typically themembers of a research team will represent a number of disciplines.This sometimes leads scientists whose perspectives encompass asingle discipline to view community-based research as lackingrigor, but well-conducted community-based research is as rigorousas any other type of well-conducted research.
Participants continue their usual activities: Participants in community-based research must be reached where they live or work—in theirnatural surroundings. This means that they may be exposed to avariety of confounding influences. For instance, adolescents partici-pating in a school-based trial of an intervention to prevent tobaccouse may also see antismoking messages on television and billboardsand may receive tobacco-related information in church, in after-school activities, or elsewhere. If smoking rates decline, it may bedifficult to identify the cause or causes. This is unlike the situationof the laboratorian, whose subjects may live in a cage or a Petridish, and unlike that of the clinical trials specialist, who can befairly certain that his/hers is the only experimental drug beingadministered to the subject.
Motivation to participate may be low: Taking part in a prevention-oriented research project often represents a low priority for poten-tial participants. Their incentive to participate is quite differentfrom that of ill persons in a therapeutic trial or even an etiologicstudy. This is especially the case in a low-income community,where top priority is assigned to finding the means to pay therent or put a meal on the table. Consequently, attrition rates maybe high in community-based studies (Blumenthal, Sung, Williams,Liff, & Coates, 1995).
COMMUNITY-BASED PARTICIPATORY RESEARCH: THE BASICS
The contemporary approach to community-based research does not coun-tenance conducting research on a community, or even in a community, butrather with a community, in a partnership arrangement. Ideally, the com-munity in which the research is to be conducted will participate togetherwith the academic or government research team in every phase of theresearch: identifying the problem to be investigated, defining the researchquestion, developing the protocol, conducting the study, analyzing thedata, and disseminating the results. This approach to research is commu-nity-based participatory research, or CBPR.
2 I: Issues
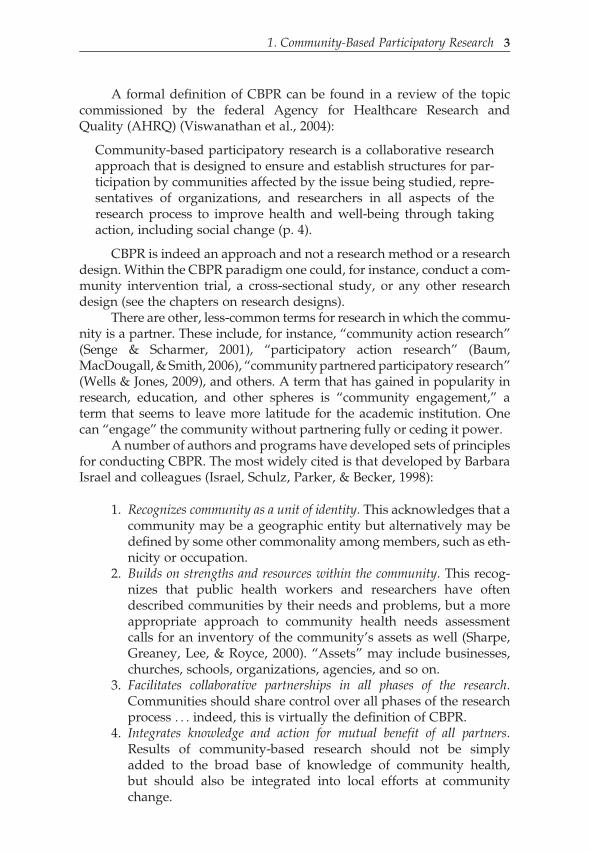
A formal definition of CBPR can be found in a review of the topiccommissioned by the federal Agency for Healthcare Research andQuality (AHRQ) (Viswanathan et al., 2004):
Community-based participatory research is a collaborative researchapproach that is designed to ensure and establish structures for par-ticipation by communities affected by the issue being studied, repre-sentatives of organizations, and researchers in all aspects of theresearch process to improve health and well-being through takingaction, including social change (p. 4).
CBPR is indeed an approach and not a research method or a researchdesign. Within the CBPR paradigm one could, for instance, conduct a com-munity intervention trial, a cross-sectional study, or any other researchdesign (see the chapters on research designs).
There are other, less-common terms for research in which the commu-nity is a partner. These include, for instance, “community action research”(Senge & Scharmer, 2001), “participatory action research” (Baum,MacDougall, & Smith, 2006), “community partnered participatory research”(Wells & Jones, 2009), and others. A term that has gained in popularity inresearch, education, and other spheres is “community engagement,” aterm that seems to leave more latitude for the academic institution. Onecan “engage” the community without partnering fully or ceding it power.
A number of authors and programs have developed sets of principlesfor conducting CBPR. The most widely cited is that developed by BarbaraIsrael and colleagues (Israel, Schulz, Parker, & Becker, 1998):
1. Recognizes community as a unit of identity. This acknowledges that acommunity may be a geographic entity but alternatively may bedefined by some other commonality among members, such as eth-nicity or occupation.
2. Builds on strengths and resources within the community. This recog-nizes that public health workers and researchers have oftendescribed communities by their needs and problems, but a moreappropriate approach to community health needs assessmentcalls for an inventory of the community’s assets as well (Sharpe,Greaney, Lee, & Royce, 2000). “Assets” may include businesses,churches, schools, organizations, agencies, and so on.
3. Facilitates collaborative partnerships in all phases of the research.Communities should share control over all phases of the researchprocess . . . indeed, this is virtually the definition of CBPR.
4. Integrates knowledge and action for mutual benefit of all partners.Results of community-based research should not be simplyadded to the broad base of knowledge of community health,but should also be integrated into local efforts at communitychange.
1. Community-Based Participatory Research 3
5. Promotes a co-learning and empowering process that attends to socialinequalities. Researchers and community members learn fromeach other. Moreover, researchers recognize the inherent inequal-ity among themselves and community members and attempt toaddress this factor by sharing information, decision-makingpower, resources, and support.
6. Involves a cyclical and iterative process. This cycle proceeds from part-nership development and maintenance through communityassessment, problem definition, development of research method-ology, data collection, analysis and interpretation, disseminationof results, determination of action and policy implications,taking action, and establishing mechanisms for sustainability. Byimplication, the process would then start over.
7. Addresses health from both positive and ecological perspectives. Theformer is the more limited model of health that emphasizes phys-ical, mental, and social well-being. The latter recognizes the role ofeconomic, cultural, historical, and political factors.
8. Disseminates findings and knowledge gained to all partners. Thisemphasizes sharing the results of the research with communitypartners in understandable language and includes the need forconsulting with participants prior to submission of manuscriptsfor publication, acknowledging the contributions of participants,and developing coauthored publications when appropriate.
9. Involves a long-term commitment by all partners. A true partnershipdoes not dissolve because a 3-year grant has come to an end.The partnership continues even in the absence of funding; the part-ners may search for new funding while continuing unfoundedactivities.
Others sets of principles include:
B A 23-item checklist by which CBPR grant applications can bereviewed and rated (Green et al., 1995)
B Eleven “critical elements” in the AHRQ review cited earlier(Viswanathan et al., 2004)
B Ten “Principles of Good Community–Campus Partnerships”developed by the organization Community-Campus Partnershipsfor Health (Community–Campus Partnerships for Health, 1997)
B Thirteen values for community-engaged research and 12 criteriafor grant applications for research involving communities, devel-oped by the National Institutes of Health’s Council of Public Repre-sentatives (Ahmed & Palermo, 2010).
Hence, for the researcher seeking to conduct CBPR, there is no dearth ofguiding principles. There are, however, a substantial series of challenges
4 I: Issues

in translating those principles into action. Some of the specific challengesare discussed later in this chapter.
Notwithstanding the plethora of principles, CBPR rests on two mainpillars (Blumenthal, 2011). The first is ethical and responds to a history ofexploitation of communities—especially minority and low-income com-munities—in the name of research. The most notorious U.S. example isthe Tuskegee Syphilis Study (see Chapter 3) but the residents of many com-munities can recall university researchers who came to conduct interviewsor take samples and then vanished. The academics presumably published,won grants, and were promoted, while the research subjects and their com-munities received no benefit.
The second pillar—community empowerment—has domestic rootsthat lie in the principle of “maximum feasible community participation”that guided the poverty programs of the late 1960s and early 1970s. Initiat-ives such as Headstart and community health centers had, and still have,community-majority governing bodies. This represented recognition ofthe fact that low-income communities rarely have any control over the pro-grams that impact their lives—schools, medical facilities, public housing,and so on. If these communities can gain a modicum of power over theseimportant aspects of their lives, the argument goes, they will be better-positioned to address the social determinants of health (Marmot, 2011)and break the “cycle of poverty:” Poverty begets powerlessness, which inturn begets poverty.
COMMUNITY-BASED RESEARCH ANDCOMMUNITY INVOLVEMENT
New Paradigms
Traditionally, the relationship between health professional and patient/client has reflected a substantial power differential; a patient has beenexpected to follow “doctor’s orders.” This has been equally true regardlessof whether the interaction was around practice or research.
Now, both medical care and research are undergoing a transform-ation. Many patients expect that their physicians will include them as part-ners in the therapeutic relationship, sharing information on the risks andbenefits of treatment options so that physician and patient can develop amanagement plan together (Sandman & Munthe, 2010). In clinical research,individual participants (the term “subjects” is losing favor) must be fullyinformed of the potential risks and benefits of the research and must givetheir consent in writing to participate. At each institution receivingfederal research funds, an Institutional Review Board (IRB) must reviewevery proposed research project to ensure that it meets all ethical standards.Although a set of federal regulations (Code of Federal Regulations, 2009)laying out these requirements has existed since the mid-1970s, it is onlyin recent years that it has been well-enforced.
1. Community-Based Participatory Research 5

In the fields of public health and community-based research, thepatient, client, or participant is the community, and a similar shift in the pro-fessional–client paradigm is underway. Public health workers are now lesslikely to view the community as a population that must be immunizedand sanitized, and much more likely to recognize it as a partner anda participant in promoting its own health. This is especially true in commu-nity-based research, where both ethics and research rigor demand that thecommunity serve as a partner. Of course, federally funded community-based research is subject to the same ethical requirements as other researchinvolving humans and must be approved by the appropriate IRB.
Community-based research often takes place in minority and otherdisadvantaged communities, and this is likely to become an even more fre-quent venue in the future as research scientists address racial and ethnichealth status disparities. These are often powerless communities that areaccustomed to being the purported beneficiaries of health and social pro-grams over which they have no control. Organized to participate withpublic health workers and researchers as partners in finding better waysto improve their health, they can become empowered to take action onother issues, such as education, transportation, or housing. These are alsopublic health issues; in fact, these “social determinants of health” (includ-ing employment, income, and socioeconomic status) are recognized ashaving a far greater impact on community health than does medical care(Marmot, 2011). Hence, CBPR can help a community address those socialdeterminants. It is unique in that the process of research (not just theoutcome) can benefit the participating community.
Levels of Community Participation
Typically, community leaders are convened as an “advisory board” to offerinput to researchers on a research agenda or on a particular project.Depending on the researchers’ approach, this can be a meaningful or asham relationship. Hatch, Saran, Presley-Cantrell, and Mallory (1993)identified four levels or models of community participation. At the firstlevel, the persons consulted by the researchers are at the periphery of thecommunity, often working for human service agencies and living outsidethe community. In this model, community residents are unaware of thepurpose of the research and have no influence on its design.
At the second level, the project’s advisors are leaders drawn fromorganizations and churches within the community, but the researchersretain total control of the project. In this model, there is community invol-vement, but it is passive.
At the third level, community leaders are asked not only for endorse-ment of the project, but for guidance in hiring community residents toserve as interviewers, outreach workers, and so on. This model is “commu-nity based but not community involved, since community members do
6 I: Issues
not contribute to the design of the research nor do they have a significantrole in interpreting findings.” This model may also offer potential for mani-pulation of the community, since those hired may essentially becomepatronage workers.
The fourth level both involves and empowers the community. In it,community representatives are first among equals in defining the researchagenda, identifying the problem to be studied, analyzing its contributoryfactors, and proposing possible solutions. The community “negotiates, asa collaborator, the goals of the study, the conduct of the study, and theanalysis and use of study findings.”
At this fourth level, there are likely to be conflicts and differencesbetween the researchers and the community. The challenge to the research-ers is to negotiate these differences and to build a trusting relationship withthe community rather than to search for another, more compliant, venue inwhich to implement their plans. This relationship between community andresearcher is the most difficult to attain but one that is most conducive toconducting effective and ethical CBPR.
COMMUNITY ORGANIZING FOR PARTNERSHIPDEVELOPMENT
Several models offer guidance for partnering with the community as part ofa community health planning (not necessarily research) process. Theseinclude, for instance, the World Health Organization’s “Healthy Commu-nities” Program (Hancock, 1993) and the Centers for Disease Control’s“Planned Approach to Community Health” (PATCH) (Goodman, Steckler,Hoover, & Schwartz, 1993). Braithwaite, Murphy, Lythcott, and Blu-menthal (1989) describe a model of “community organization and develop-ment for health promotion” that borrows from the “empowermenteducation” approach of Paulo Freire (1968). Freire’s writings are oftencited as forming much of the philosophical basis for CBPR.
Braithwaite et al. list seven steps in the model as guidance to healtheducators or community organizers:
1. Learning the community layout: Entry to the community should bepreceded by a study of community geography, health statusmeasures, and so on.
2. Learning the community ecology: This includes identifying placeswhere people congregate, as well as meeting community leadersand “gatekeepers” and learning their relationship to each other.
3. Community entry process: The process must be negotiated with gate-keepers, and the community organizer must be “validated” by theformal and informal community networks.
4. Building credibility: Tangible resources, such as jerseys for a neigh-borhood football team, are helpful at this step.
1. Community-Based Participatory Research 7
5. Development of a community coalition board: The board described inthis step is one that is consumer dominated (at least 60%) butalso includes academic, agency, and organizational representa-tives as well as elected officials.
6. Conducting a community needs assessment: This involves a survey orsimilar methods to identify those health issues felt by communityresidents to be most important. In the context of a research initiat-ive, this step might be titled “establishing a research agenda.”
7. Planning the intervention: Again, in the context of a research initiat-ive, this would be “planning the research project.” Implicit is the needto provide feedback on the results of the project or the interventionto the community.
PRINCIPLES FOR WORKING WITH COMMUNITIES
Among the guidelines and principles mentioned earlier, those developed byCommunity–CampusPartnerships for Health (1997) areworthreproducinghere.These are straightforward and apply regardless of whether the academic–community partnership is focused on research, education, or service:
1. Partners must agree on missions, goals, and outcomes.2. Partners should have mutual trust, respect, and commitment.3. Partnerships need to build on identified strengths and assets.
Instead of approaching a community-based partnership solelyby itemizing all of the problems that the community faces, the part-ners should also identify their strengths and assets.
4. Good partnerships should have clear communication among part-ners and transparency in the decision-making process.
5. Partnerships evolve using feedback to, among, and from allpartners.
6. Roles, norms, and processes for the partnerships should evolvefrom the input and agreement of all partners. Partnerships needa governance structure that establishes a common understandingof how to proceed.
7. Successful partnerships have relationships with local leaders andfunding agencies.
8. Effective partnerships use existing structures, such as schools andworksites, to incorporate solutions into their mission.
HEALTH DISPARITIES AND HEALTH EQUITY
CBPR represents an attempt to bringing equity to the research enterprise. Itis understandable, then, that most CBPR is focused on bringing equity tohealth—that is, to reducing or eliminating the gaping disparities that arereflected in racial and ethnic health status indices.
Table 1.1 illustrates these disparities.
8 I: Issues

It seems clear from the table that it is the African American populationthat is most severely affected by health disparities. Black mortality rates arethe highest of any racial or ethnic group for every important cause of death,with rates that exceed the lowest rates by factors ranging from a bit lessthan 2 to over 30. However, every group is affected by one or another dis-parity; for instance, Asians have unusually high rates of hepatitis B infec-tion and liver cancer (with the former largely responsible for the latter).
Some Challenges in Conducting CBPR
For the research scientist wishing to pursue CBPR, there are several chal-lenges unique to this research approach (Blumenthal, 2011):
B Maintaining credibility: CBPR is potentially vulnerable to criticismfrom both fellow researchers in the field and from more traditionalresearch scientists. From the former may come the charge that theresearch is not sufficiently community participatory—that it doesnot adhere sufficiently to the many published principles for part-nering with communities and conducting CBPR. From the lattermay come the charge that the research is not sufficiently rigor-ous—that it compromises science in the interest of providing com-munity service. While these criticisms may have validity inindividual cases, there is no reason why an academic–communityteam cannot conduct research that is scientifically rigorous while atthe same time adhering to the principles of good partnerships.
B Time constraints: CBPR may take longer to achieve outcomes thando more traditional research models, and certainly longer thanmost laboratory research. The partnership-building process itselfmay take a year or more. For the junior faculty member on a time-table for promotion, this may prove daunting. Negotiations with
Table 1.1 Mortality Rates by Racial/Ethnic Group, Age Adjusted Deaths/100,000 Population
Cause of Death Black White Hispanic NativeAmerican
Asian
All 1,006.2 777.8 579.5 652.9 436.7
Heart disease 308.4 239.2 180.5 157.4 134.6
Cancer 238.8 195.6 128.4 125.4 113.6
Stroke 76.3 54.6 41.3 47.5 47.7
Diabetes 49.5 22.2 35.6 43.2 17.4
Homicide 21.0 2.8 7.3 8.4 2.9
AIDS 22.5 2.1 5.8 2.2 0.8
Source: Health, United States (2009).
1. Community-Based Participatory Research 9
the department chair or with the promotion and tenure committeemay be needed; some institutions have adjusted their promotionrequirements (Calleson, Jordan, & Seifer, 2005; Steiner, Calleson,Curtis, Goldstein, & Denham, 2005).
B IRB review: Faculty conducting CBPR often complain that IRBs donot understand this research approach and erect needless road-blocks and delays—for instance, by requiring detailed consentdocuments for seemingly minimal-risk projects. In fact, themission of IRBs is to protect individual research participantsrather than communities (Code of Federal Regulations, 2009). Thesolution at the institutional level may lie in IRB education, or eventhe creation of a special IRB to review community-based research.
CULTURAL COMPETENCE IN COMMUNITY-BASED RESEARCH
Partnering or creating a coalition with a community presupposes that theresearcher is competent to communicate and interact with persons whoare part of the community’s culture; that is, the researcher should be cultu-rally competent. Cultural competence begins with understanding the con-cepts of culture, values, beliefs, and ethnicity, from both the individual andorganizational systems perspectives. It is important to understand theimpact and influence of cultural competence on one’s own cultural perspec-tive as it relates to community-based research. A dictionary definition ofculture is “the customary beliefs, social forms, and material traits of aracial, religious, or social group” (Merriam-Webster, 2012). Cultureshapes how people experience their world and make decisions on qualityof life and work (Health Resources and Services Administration, 1998).
Values are abstract concepts of worth. They are not initially an indi-vidual’s own concepts, but are social products of what has been taughtor imposed upon the person and slowly, over time, internalized. As anindividual matures and/or is exposed to other values, he or she mayconsciously adopt the value or may discard or modify it to fit his or herown perspectives.
Beliefs are structures of values, common language and similar lifeexperiences shared within a culture. Ethnicity refers to groups of peoplegenerally believed to be biologically related and who share a uniquesocial and cultural heritage.
Most definitions of cultural competence describe an increased culturalawareness and knowledge and a change in attitude. The concept is multi-faceted; researchers and practitioners must view it broadly in order toassimilate it and put it into practice. Cross, Bazon, Dennis, and Isaacs(1989) have developed the following definition of cultural competencethat contains the essential principles:
A set of attitudes, skills, behaviors, and policies that enable organiz-ations and staff to work effectively in cross-cultural situations.
10 I: Issues
It reflects the ability to acquire and use knowledge of the health-related beliefs, attitudes, practices, and communication patterns ofclients and their families to improve services, strengthen programs,increase community participation, and close the gaps in healthstatus among diverse population groups. Cultural competence alsofocuses attention on population-specific issues including health-related beliefs and cultural values (the socioeconomic perspective),disease prevalence (the epidemiological perspective), and treatmentefficacy (the outcome perspective).
According to the National Center for Cultural Competence (2000),cultural competence requires that organizations:
B Have a defined set of values and principles, and demonstrate beha-viors, attitudes, policies, and structures that enable them to workeffectively cross culturally.
B Have the capacity to (1) value diversity, (2) conduct self-assessment, (3) manage the dynamics of difference, (4) acquireand institutionalize cultural knowledge, and (5) adapt to diversityand the cultural contexts of the communities they serve.
B Incorporate the above in all aspects of policy making, adminis-tration, practice, and service delivery, and involve systematicallyconsumers, key stakeholders, and communities.
A culturally competent system acknowledges and incorporates, at alllevels, the importance of culture, the assessment of cross-cultural inter-actions, vigilance toward the dynamics that result from cultural differ-ences, expansion of cultural knowledge and adaptation of services, andresearch and prevention models to meet culturally unique needs. Culturalcompetence is a developmental process and should be viewed as a goal thatinstitutions, agencies, and individuals strive to achieve.
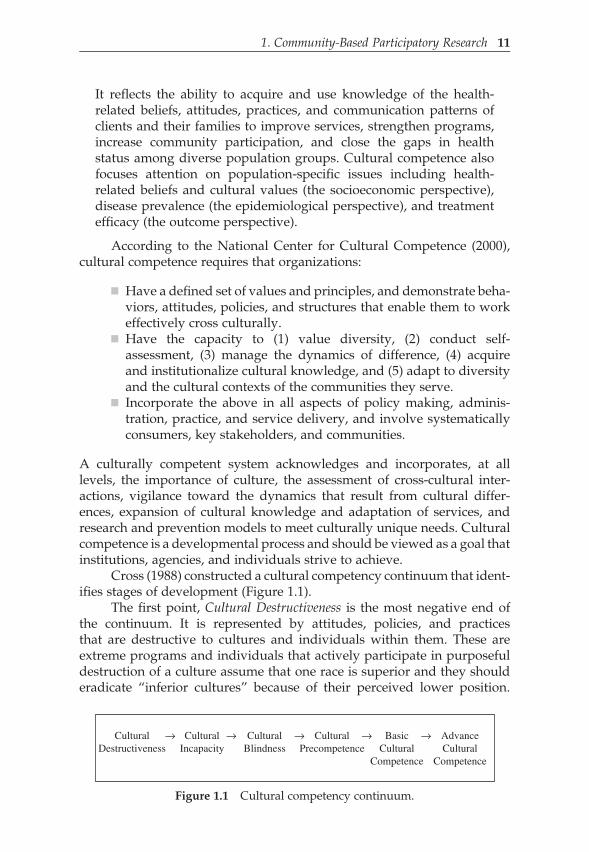
Cross (1988) constructed a cultural competency continuum that ident-ifies stages of development (Figure 1.1).
The first point, Cultural Destructiveness is the most negative end ofthe continuum. It is represented by attitudes, policies, and practicesthat are destructive to cultures and individuals within them. These areextreme programs and individuals that actively participate in purposefuldestruction of a culture assume that one race is superior and they shoulderadicate “inferior cultures” because of their perceived lower position.
CulturalDestructiveness
→ CulturalIncapacity
→ CulturalBlindness
→ CulturalPrecompetence
→ BasicCultural
Competence
AdvanceCultural
Competence
→
Figure 1.1 Cultural competency continuum.
1. Community-Based Participatory Research 11

These entities are actively involved in services that deny people access totheir natural helpers or healers. They remove children from their familiesbased on race or ethnicity and risk the well-being of minority individualsin social or medical experiments without their knowledge or consent.
Cultural Incapacity, the second point on the continuum, does notincorporate intentional cultural destructiveness, but rather a lack of capac-ity to work effectively with diverse groups. There is extreme bias and thebelief in racial superiority of the dominant group. Frequently there is a dis-proportionate application of resources, support of racist policies, mainten-ance of stereotypes, and lower expectation of minorities.
At the third point, Cultural Blindness, research is conducted and healthservices provided with the intent of being unbiased. Cultural blindnessleads one to believe that culture makes no difference, for example, “allpeople are the same.” Research and health services approaches tradition-ally used by the dominant culture are universally applied. Cultural blind-ness ignores the cultural strengths of individuals and groups andencourages assimilation into the majority culture. Minorities are viewedfrom the cultural deprivation model that asserts problems are the resultof inadequate resources rather than cultural differences.
Cultural Pre-Competence, point four, implies movement toward com-petence. Weaknesses are recognized and attempts to improve practicesand increase knowledge are made. There is a danger of “tokenism,”however, as systems attempt to explore more culturally competent pro-cesses. Precompetent entities often lack information on what is possibleand how to proceed. These systems and individuals are characterized bythe desire to practice culturally competent services and a commitment tothe rights of individuals.
Point five, Basic Cultural Competence, is characterized by acceptance ofand respect for difference, continuing self-assessment regarding culture,and careful attention to the dynamics of difference. There is a continuousexpansion of cultural knowledge and resources and a variety of adaptationsto research and health services, adjusting and creating new models in orderto address more effectively the needs of multiple populations.
Advanced Cultural Competence, point six, is the most positive end of thecontinuum. It is characterized by holding culture in high esteem andseeking to add to the knowledge base of cultural competence by conduct-ing culture-based research, examining intra-cultural phenomena asopposed to comparison research, which compares minority populationsto the dominant population.
There are three primary arenas of change where development can andmust occur if there is to be a movement toward cultural competence: (1)Attitudes change to become less ethnocentric and biased; (2) policieschange to become more flexible and culturally impartial; and (3) practiceschange to become more congruent with the culture(s) with which the inter-action is based.
12 I: Issues

CULTURALLY COMPETENT RESEARCH
Culturally competent research should encompass the following com-ponents: awareness and acceptance of cultural differences; awareness ofone’s own cultural values; understanding of the dynamics of difference;basic knowledge about the culture of the population involved in theresearch; knowledge of the research participants’ environment; ability toadapt research methods, evaluation, and data collection; and analysis tofit the participants’ cultural context.
In addition to the characteristics of culturally competent research,there are five elements that characterize the culturally competent researcher.
1. Acknowledges cultural differences and becomes aware of howthey affect the research process. The researcher should develop adual perspective, that is, an understanding of his or her ownculture and appreciation of differences among others.
2. Recognizes the influence of one’s own culture on perspectives.Acknowledges how cultural norms and values have shapedday-to-day behaviors and have been reinforced by families,peers, and social institutions.
3. Understands and accepts the dynamics of difference. Whenresearchers of one culture interact with and collect data from par-ticipants of another culture, both groups bring their own historyand the influence of current political and socioeconomic powerrelationships to the research interaction.
4. Makes a conscious effort to understand the meaning of the datawithin his or her own cultural context as well as that of the partici-pants. Qualitative research methods often effectively enhance theinterpretation of quantitative data. Interview and focus groupscan be utilized to effectively clarify survey results, providingin-depth perspectives to unanswered questions. It is important tounderstand what symbols are meaningful and what they meanto research participants, how health is defined and how peergroup and family group networks are configured.
5. Knows where and how to obtain detailed information regardingthe culture of populations involved in the research. Gainsenough knowledge to know how to seek information, what infor-mation to seek, and how to apply it effectively.
Culturally competent research strengthens the effectiveness of researchers,health care providers, and health service systems by providing them withaccurate information to improve their work. It also empowers diverse com-munities by equipping them with the knowledge and skills to understandhealth care issues and to intervene on their own behalf (National Center forCultural Competence, 2000).
1. Community-Based Participatory Research 13

SUMMARY
Community-based research is the force that propels modern public health.Advances against the most important causes of morbidity and mortality inindustrial societies and, hence, major gains in life expectancy, will dependon scientific advances at the community level. Moreover, improvements inpublic health at the community level offer the best chance of reducing oreliminating racial and ethnic health status disparities.
It is now widely accepted that the appropriate and ethical way toconduct research in communities is through community-based participatoryresearch—that is, by partnering with the community and involving it atevery step of the way. In this way, exploitation of communities isaverted, just as unethical exploitation of individual research participantsis averted by treating them as partners in research.
CBPR relies on the same scientific principles as other types ofresearch. The processes by which hypotheses are developed and testedand considerations of study design are similar in any type of research.There is, however, an important set of considerations that apply uniquelyto community-based research. These include the principles that governrelationships between researchers and communities and the principles ofcultural competence that prepare researchers to create the community part-nerships needed to conduct community-based research.
CASE STUDY
THE EXPERIENCE OF PARTNERING WITH ACADEMIA
by Ernest Hopkins III
This is a case study of partnering community and academia, havinga mutual interest in research and the dissemination of informationinto communities at risk.
Engaging the idea of participating in research was certainly not new tome, having been diagnosed with a life-threatening chronic illness in1984. The experience first starts with open-mindedness, a willingnessto be a part of something unknown, different, challenging, impactingyou or your community. Having some experience working withothers as a leader in the HIV community opened doors and opportu-nities to expand interest in local research. I was introduced to theAtlanta Clinical and Translational Science Institute (ACTSI)/Commu-nityEngagementResearchProgram(CERP)byalong-timecommunityactivist/advocate who was already involved in participatory research.The activist was Linda Felix, who requested my participation during a
(continued)
14 I: Issues

CERP Steering Board meeting. After attending several meetings ledby community members, I committed to becoming a community part-ner and a marriage between community and academia was made.
Our CERP introduced me to several researchers that appealed to ourinterests particularly in the area of HIV prevention education and out-reach. Our organization has had to develop relationships that fosterresearch and the dissemination of information to under-served, mar-ginalized, at-risk communities. The relationship between communityand academia has worked for me and my organization (The PhoenixGroup Foundation, Inc.) only in the sense of having developed anetwork of academic scholars and researchers who are willing tohelp my community address health disparities. Within our first yearparticipating in the ACTSI/CERP Steering Board, we have hadseveral opportunities to apply for small mini-grants to initiateresearch led educational programming in our local HIV community.
The researcher, Gale Newman, PhD, Department of Microbiology,Biochemistry, and Immunology, Morehouse School of Medicine,focusing on the study of HIV-associated neuropathy, collaboratedwith me and my organization initially to disseminate prevention edu-cation for HIV positives at risk of renal (kidney) disease. The researchfindings and data are to be shared with the community. Havingworked with a researcher has allowed us to examine weaknessesand strengths internally within our organization, which has per-mitted us to strengthen our capacity to disseminate information toour communities served and to also be a better partner in the partici-patory research community.
We found some principal keys to success in developing ourresearch relationship:
Listening: Is one of the most important keys; it requires bothparties to communicate and develop understanding. The lis-tening success key is important to building the “relationship”that’s needed to promote the dissemination of researchinformation.
Teamwork: Good teamwork is essential to creating the commu-nity/academic relationship. Teamwork is working togetherfor a common cause, to reach a goal collectively. The team-work key promotes collaboration among researchers andcommunity members; it helps to support effective outcomesthat impact underserved populations.
Collaboration: Collaboration is a major success key for buildingeffective academic and community relationships for partici-patory research. It was essential for our organization to use
(continued)
1. Community-Based Participatory Research 15

our listening skills to be able to collaborate with others. Col-laborating is essential to maximizing impact and having suc-cessful outcomes to affect communities with high levels ofhealth disparities.
Our organizational experience with community participatoryresearch has been attainable only because of these keys to success.
REFERENCES
Ahmed, S. M., & Palermo, A. S. (2010). Community engagement in research: Frame-works for education and peer review. American Journal of Public Health, 100(8),1380–1387.
Baum, F., MacDougall, C., & Smith, D. (2006, October). Participatory action research.Journal of Epidemiology and Community Health, 60(10), 854–857.
Blumenthal, D. S. (2011). Is community-based participatory research possible? AmericanJournal of Preventive Medicine, 40, 386–389.
Blumenthal, D. S., Sung, J., Williams, J., Liff, J., & Coates, R. (1995). Recruitment andretention of subjects for a longitudinal cancer prevention study in an inner-cityBlack community. Health Services Research, 30, 197–205.
Braithwaite, R. L., Murphy, F., Lythcott, N., & Blumenthal, D. S. (1989). Communityorganization and development for health promotion within an urban Black commu-nity: A conceptual model. Health Education, 20(5), 56–60.
Calleson, D. C., Jordan, C., & Seifer, S. D. (2005, April). Community-engaged scholarship:Is faculty work in communities a true academic enterprise? Academic Medicine, 80(4),317–321.
Code of Federal Regulations, Title 45 Part 46: Protection of Human Subjects. RevisedJanuary 15, 2009. Available at http://www.hhs.gov/ohrp/humansubjects/guidance/45cfr46.html
Community–Campus Partnerships for Health. (1997). Principles of good community–campus partnerships. Retrieved from http://depts.washington.edu/ccph/principles.html#principles
Cross, T. L. (1988). Services to minority populations: Cultural competence continuum.Focal Point, 3(1), 1–2.
Cross, T., Bazon, B., Dennis, K., & Isaacs, M. (1989). Towards a culturally competent systemof care, (l). Washington, DC: Georgetown University Child Development CenterCASSP Technical Assistance Center.
Freire, P. (1968). Pedagogy of the oppressed. New York: Continuum, 2007 (first published inPortuguese, first English translation 1970).
Goode, T., Harrisone, S., Sandman, L., & Munthe, C. (2010, March). Shared decisionmaking, paternalism and patient choice. Health Care Analysis, 18(1), 60–84.
Goodman, R. M., Steckler, A., Hoover, S., & Schwartz, R. (1993, January–February). Acritique of contemporary community health promotion approaches: Based on aqualitative review of six programs in Maine. American Journal of Health Promotion,7(3), 208–220.
Green, L. W., George, M. A., Daniel, M. et al. (1995). Guidelines and categories for classifyingparticipatory research projects in health promotion (pp. 43–50). Ottawa, Ontario: RoyalSociety of Canada. Retrieved from www.lgreen.net/guidelines.html
Hancock, T. (1993, Spring). The evolution, impact and significance of the healthy cities/healthy communities movement. Journal of Public Health Policy, 14(1), 5–18.
16 I: Issues

Hatch, J., Moss, N., Saran, A., Presley-Cantrell, L., & Mallory, C. (1993). Communityresearch: Partnership in black communities. American Journal of Preventive Medicine,9(6 Suppl), 27–31; 23, 2001.
Health Resources and Services Administration, Bureau of Primary Health Care, U.S.Department of Health and Human Services. (1998). Cultural competence: A journey.
Israel, B. A., Schulz, A. J., Parker, E. A., & Becker, A. B. (1998). Review of communitybased research: Assessing partnership approaches to improve public health.Annual Reviews in Public Health, 19, 173–202.
Marmot, M. (2011, October 1). Global action on social determinants of health. Bulletin ofthe World Health Organization, 89(10), 702.
Merriam-Webster. Retrieved June 28, 2012, from http://www.merriam-webster.com/medical/culture
National Center for Cultural Competence. (2000, Summer). Cultural competence in primaryhealth care: Partnerships for a research agenda (Policy Brief No. 3). Washington, DC:National Center for Cultural Competence.
Senge, P., & Scharmer, O. (2001). Community action research. In P. Reason, &H. Bradbury (eds), Handbook of action research (pp. 238–250). Thousand Oaks, CA:Sage Publications.
Sharpe, P. A., Greaney, M. L., Lee, P. R., & Royce, S. W. (2000, March–June).Assets-oriented community assessment. Public Health Report, 115(2–3), 205–211.
Steiner, B. D., Calleson, D. C., Curtis, P., Goldstein, A. O., & Denham, A. (2005, April).Recognizing the value of community involvement by AHC faculty: A case study.Academic Medicine, 80(4), 322–326.
Viswanathan, M., Ammerman, A., Eng, E. et al. (2004). Community-based participatoryresearch: Assessing the evidence. Evidence Report/Technology Assessment No. 99(Prepared by RTI—University of North Carolina Evidence-based Practice Centerunder Contract No. 290-02-0016). AHRQ Publication 04-E022-2. Rockville, MD:Agency for Healthcare Research and Quality.
Wells, K., & Jones, L. (2009, July 15). Commentary: “Research” in community-partnered,participatory research. Journal of the American Medical Association, 302(3), 320–321.
1. Community-Based Participatory Research 17
