sedation policy lpch 6 11
TRANSCRIPT

This policy applies to: Lucile Packard Children’s Hospital
Date Written or Last Revision:JUNE 2011
Name of Policy: Sedation Policy
Page 1 of 24 Departments Affected: All Departments
Contents: I. Purpose II. Policy: III. Definitions: A. Minimal Sedation B. Moderate Sedation C. Deep Sedation D. Anesthesia IV. Equipment V. Medication VI. Process/Procedures Moderate vs Deep Sedation: A. Locations B. Process 1. Pre-procedure Physician Responsibility 2. Pre-procedure Nursing Responsibility 3. Intra-procedure Monitoring and Care Requirements 4. Post-procedure Monitoring and Care Requirements 5. Management of Emergency Situations VI. Requirements: A. Credentialing B. Personnel C. Ongoing Performance Improvement and Outcomes Measurement VII. Related Documents VIII. Appendices I. PURPOSE
The administration of drugs to produce sedation can have the unintended effect of compromising a patient's protective reflexes, therefore this policy and procedure are intended create the framework and outline the operational requirements to facilitate a standardized approach to provide patients at Packard with the benefits of sedation/analgesia while minimizing the associated risks. For the purposes of this document, a clear distinction has been made between “minimal,” “moderate,” and “deep” sedation, but moving from a state of consciousness to deep sedation and further to general anesthesia is a continuum. This continuum depends on individual response, age, health status, and drug combinations used.

This policy applies to: Lucile Packard Children’s Hospital
Date Written or Last Revision:JUNE 2011
Name of Policy: Sedation Policy
Page 2 of 24 Departments Affected: All Departments
II. POLICY STATEMENT
Administration of any drug or drugs to sedate a patient in association with a procedure requires implementation of the sedation policy.
III. DEFINITIONS
A. Minimal sedation/analgesia: A drug-induced state during which patients remain conscious and
respond to verbal commands. Although cognitive function and coordination may be impaired, consciousness, ventilatory and cardiovascular functions are unaffected. Gag reflex and other protective airway reflexes are maintained. This state may be referred to as “anxiolysis.”
B. Moderate sedation/analgesia: A drug-induced depression of consciousness during which patients
respond purposefully to verbal commands, either alone or accompanied by light tactile stimulation. No interventions are required to maintain a patent airway, and spontaneous ventilation is adequate. Gag reflex and other protective airway reflexes are maintained. Cardiovascular function is usually maintained. Reflex withdrawal from a painful stimulus is not considered a purposeful response.
C. Deep sedation/analgesia: A drug-induced depression of consciousness during which patients
cannot be easily aroused but respond purposefully following repeated or painful stimulation. The ability to independently maintain ventilatory function may be impaired, and gag reflex and other protective airway reflexes may be impaired or absent. Patients may require assistance in maintaining a patent airway and spontaneous ventilation may be inadequate. Gag reflex and other protective airway reflexes may be impaired. Cardiovascular function is usually maintained. Reflex withdrawal from a painful stimulus is not considered a purposeful response.
This policy applies to: Lucile Packard Children’s Hospital
Date Written or Last Revision:JUNE 2011
Name of Policy: Sedation Policy
Page 3 of 24 Departments Affected: All Departments
D. Anesthesia: A drug-induced loss of consciousness during which patients are not
arousable, even by painful stimulation. The ability to independently maintain ventilatory function is often impaired. Patients often require assistance in maintaining a patent airway, and positive pressure ventilation may be required because of depressed spontaneous ventilation or drug-induced depression of neuromuscular function. Gag reflex and other protective airway reflexes are absent. Cardiovascular function may be impaired.
IV. EQUIPMENT
A. Use equipment that monitors and measures the following 1. Respiratory rate 2. Heart rate 3. EKG 4. Blood Pressure 5. Blood Oxygen saturation 6. ET CO2 levels (for patients receiving moderate or deep sedation) B. Emergency equipment immediately available: 1. Code cart 2. Suction equipment (wall suction or portable suction generator,
suction canister, suction tubing, tonsil-tip or Yankauer suction, red rubber catheters, or the equivalent, sterile tracheal suction catheters)
3. Self-inflating manual resuscitation bag and mask 4. Oral and Nasopharyngeal Airways, endotracheal tubes,
laryngoscopes of appropriate sizes, and a qualitative or quantitative CO2 detection device.
V. Medication A. Moderate Sedation: Includes medications as ordered for sedation
(Refer to LPCH Housestaff Manual) B. Deep Sedation: includes medications as listed in LPCH housestaff
manual C. For the purpose of procedural sedation, drugs that are anesthetic
agents, such as propofol (Diprivan®), and ketamine (Ketalar®), etc., must be administered by an appropriately credentialed anesthesiologist, or by a credentialed physician using a written protocol that has been approved by the Sedation Committee (see Appendix E).

This policy applies to: Lucile Packard Children’s Hospital
Date Written or Last Revision:JUNE 2011
Name of Policy: Sedation Policy
Page 4 of 24 Departments Affected: All Departments
VI. PROCESS/PROCEDURE
LOCATIONS: Sedation for procedures will be completed whenever possible in locations as specified in the Location Matrix for Sedation at LPCH (See appendix F) These standards apply to all LPCH patients in all locations where invasive and/or diagnostic procedures are performed under sedation, with the following clarifications: A. Locations staffed by Anesthesiologists: When general anesthesia, regional anesthesia, or sedation is
administered by an anesthesiologist at LPCH or SHC, at a minimum the sedation policy will apply, but may be augmented by the policies of the Department of Anesthesia, pertinent to specific locations.
B. Pediatric, Cardiovascular, and Neonatal Intensive Care Units: 1. When patients who are not intubated or mechanically ventilated
receive sedation for any procedure, the provisions of the Sedation Policy will apply.
2. When patients who are intubated and currently receiving sedation require a deeper level of sedation in order to have a procedure performed, the documentation requirements of the Sedation Policy will apply, including the need for obtaining consent.
3. The provisions of the Sedation Policy do not apply to patients who are administered sedatives either by continuous infusion or by intermittent boluses for the purpose of maintaining a continuously sedated state to facilitate mechanical ventilation or other routine ICU therapy that does not itself require an informed consent.
PROCESS

This policy applies to: Lucile Packard Children’s Hospital
Date Written or Last Revision:JUNE 2011
Name of Policy: Sedation Policy
Page 5 of 24 Departments Affected: All Departments
The standards below apply to the administration of moderate sedation and deep sedation. Note that the standards for practitioner presence and practitioner completion of preparation and evaluation differ for moderate and deep sedation. These standards do not apply to the administration of minimal sedation (e.g. anxiolysis). Moderate Sedation: requires either a physician credentialed in moderate sedation, or a moderate sedation credentialed physician assistant or nurse practitioner, working under a protocol with the supervision of a responsible physician. Deep Sedation: requires an intensive care physician credentialed for deep sedation or an anesthesiologist A. Pre-Procedure Practitioner Responsibility: 1. Ensure there is a complete History and Physical Examination
documented as specified in the hospital bylaws. Complete and document a pre-procedure assessment, with a focus on the following elements of the H&P, within 48 hours of the planned sedation:
a. History: (1) Acute and chronic medical problems (2) History of adverse reactions to anesthesia or
sedative medication, potential risks or problems (3) Allergies (4) History of airway anomalies (see Appendix A) (5) Any history of apnea (6) Current medications (6) Recent dosing of sedative and/or opioid
medications (7) Last food and fluid intake b. Physical Examination: (1) Airway evaluation (2) Cardiovascular evaluation (3) Pulmonary evaluation (4) the patient's general condition/neurologic status c. Assign American Society of Anesthesiologists Physical
Status (see Appendix B)

This policy applies to: Lucile Packard Children’s Hospital
Date Written or Last Revision:JUNE 2011
Name of Policy: Sedation Policy
Page 6 of 24 Departments Affected: All Departments
2. For a patient with unstable or poorly controlled systemic disease or organ dysfunction (ASA 3), obtain a consultation with a member of one of the following departments or divisions as appropriate to the child’s underlying disease state and condition:
a. Department of Anesthesia b. Division of Critical Care c. Division of Pediatric Cardiology d. Division of Neonatology 3. Referral to, or consultation by, the Department of Anesthesia is
required for ASA Physical Status 4 or 5 patients (see Appendix B) and all patients with congenital or acquired airway abnormalities (see Appendix A), unless under the care of an intensivist or a neonatologist in an intensive care environment.
4. Practitioner responsible for and ordering sedation must obtain and document informed consent for sedation.
5. Establish and document a plan for sedation, and write or enter orders in the Electronic Health Record for 1. NPO status, (See Appendix C), 2. sedative medications, and 3. intravenous access if required.
6. Immediately prior, within 1 hour, of administering the sedation, review and reassess the following:
a. the pre-sedation assessment b. sedation plans c. current patient condition including recent dosing of sedative and
opioid medications and last food and fluid intake d. Document this reassessment

This policy applies to: Lucile Packard Children’s Hospital
Date Written or Last Revision:JUNE 2011
Name of Policy: Sedation Policy
Page 7 of 24 Departments Affected: All Departments
B. Pre-Procedure Nurse Responsibility 1. Initiate the pre-procedure checklist and Universal Protocol, located
in the Ad Hoc charting section of the Electronic Health Record. Satellite units will document on the paper Pre-Procedure Checklist form. Outpatients also require the short form nursing assessment and nursing history.
2. Notify the manager if the appropriately trained staff is not available or if additional medical evaluation is required.
3. If an outpatient, ensure that the patient has transportation home and will be accompanied by a responsible adult.
4. Verify that a completed history, physical, pre-sedation assessment, and sedation informed consent are documented. Also if needed, consultation from an anesthesiologist or appropriate intensive care or cardiology specialist. (See A. 2. and 3 above)
5. Confirm and document NPO status. If not in compliance with guidelines, notify the responsible physician, physician’s assistant, or nurse practitioner.
6. Assess and document the pre-sedation condition of the patient using the ‘Recovery Scoring Tool’ on the paper or Interactive Flowsheet. This includes:
a. Baseline Level of consciousness b. Baseline Level of pain c. Baseline Sp02 d. Baseline capillary refill e. Baseline level of nausea or vomiting 7. Document baseline vital signs in the Interactive Flowsheet 8. Ensure that patients have patent IV access; mandatory for those
undergoing deep sedation, suggested for all patients undergoing sedation but at the discretion of the attending physician or practitioner ordering the sedation
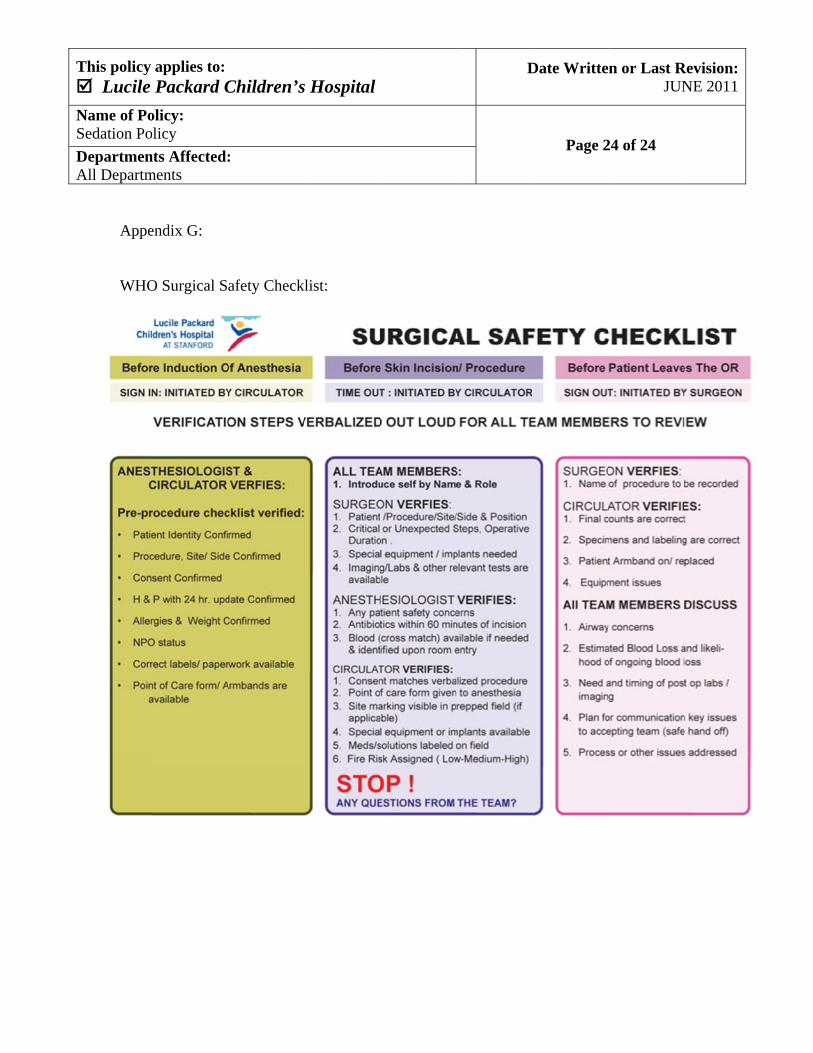
9. Ensure that the "Pediatric WHO Checklist" is completed prior to initiation of the procedure and documented on the Universal Protocol (See appendix G).
C. Intra-Procedure Monitoring and Care Requirements (also see Appendix D)
1. Continuous observation and monitoring of the patient during administration of sedation for:
a. Airway patency and respiratory rate (including ETCO2 value for moderate and deep sedation)

This policy applies to: Lucile Packard Children’s Hospital
Date Written or Last Revision:JUNE 2011
Name of Policy: Sedation Policy
Page 8 of 24 Departments Affected: All Departments
b. Hemoglobin oxygen saturation and pulse rate using pulse oximetry
c. Electrocardiogram d. Level of consciousness e. Occurrence of adverse reactions 2. Intermittent blood pressure monitoring as follows: a. For moderate sedation: measurement and documentation
on the interactive flowsheet of blood pressure after administering the sedative drugs, and intermittent monitoring of blood pressure as follows:
(1) Blood pressure will be recorded every 15 minutes except for the following patients, for whom blood pressure will be recorded every 5 minutes:
(a) Patients with a history of hypertension, whether treated or not at the time of the procedure
(b) Patients who have had a renal transplant (c) Patients with acquired or congenital heart
disease (d) Patients with a history of cardiac arrhythmias (e) Patients who have or are at risk for
dehydration. (f) Patients less than 52 weeks Post-conceptional
age (g) Patients with a history of sleep apnea b. For deep sedation: measurement and documentation on
the paper or interactive flowsheet of blood pressure after administering the sedative drugs, and intermittent monitoring of blood pressure every 5 min.
3. Documentation will be made of observations and monitoring, the names, dosage, route, and time of all drugs administered and patient’s response to medication on the paper or interactive flowsheet and MAR
4. If the MD administers a medication during the procedure, the nurse must document the medication administration on the paper or electronic MAR noting the name of the MD who administered the medication in the ‘Performed By’ field.
This policy applies to: Lucile Packard Children’s Hospital
Date Written or Last Revision:JUNE 2011
Name of Policy: Sedation Policy
Page 9 of 24 Departments Affected: All Departments
5. Documentation for patients receiving sedation or anesthesia by an anesthesiologist will comply with Anesthesia Department processes
6. The practitioner responsible for the sedation must be immediately available during the administration of the sedative medication, or designate another qualified practitioner who will be so available. The identity and beeper number and/or direct phone link for the responsible practitioner must be communicated to the nurse administering the sedation.
7. If deep sedation is planned, a responsible physician must be present, with no other conflicting immediate responsibilities.
D. Post-Procedure Monitoring and Care Requirements 1. A practitioner, credentialed in sedation, a. Must remain immediately available throughout the recovery period b. If the patient requires reversal medications and/or does not meet
discharge criteria within 1 hour of admission to recovery, the practitioner must evaluate the patient and order their discharge to the next appropriate level of care.
c. If no recovery (PACU) or sedation-level-2 competent nursing staff is available, a practitioner credentialed in sedation will remain with the patient until he/she is recovered.
2. A nurse, recovery (PACU) or sedation-level-2 competent, will remain with the patient through the recovery period and complete the following:
a. Using the same protocol as during the procedure, continually assess and monitor the patient for a minimum of 30 minutes post-procedure, and continue until the patient meets the following post-procedure discharge criteria. (see appendix D for frequency of monitoring required during recovery from sedation) .
b. The following criteria indicate that the patient has recovered sufficiently to safely return home if an outpatient, or if an inpatient, to return to pre-procedure level of care.
i. Able independently to maintain an airway ii. SpO2 at the patient’s baseline level iii. Stable cardiovascular status. An adequate post-procedure
blood pressure must be recorded. iv. Easily aroused, able to talk (if age appropriate), or is at
pre-procedure baseline level of consciousness v. If reversal agent given, monitor for 1 hour before
discharge. vi. For outpatients:

This policy applies to: Lucile Packard Children’s Hospital
Date Written or Last Revision:JUNE 2011
Name of Policy: Sedation Policy
Page 10 of 24 Departments Affected: All Departments
(1) The patient’s discharge from the hospital must be ordered by a physician, or meet established discharge criteria.
(2) A responsible adult must be present to escort the patient home.
(3) The patient or parent/guardian must be given written post-procedure instructions.
c. Document the post-procedure assessment using the ‘Recovery Scoring Tool’ located on the paper or Interactive Flowsheet. If the patient does not return to the documented baseline assessment within one hour, continue to monitor frequently and notify the MD.
d. For infants receiving sedation, please see the LPCH Policy on Admission of Infants after Anesthesia or Sedation
E. Management of Emergency Situations 1. Any practitioner ordering, responsible for, or supervising a trainee
ordering or responsible for sedation, and any practitioner monitoring the patient must be competent to institute appropriate emergency care if the patient’s airway, breathing, or circulation becomes compromised.
2. Immediately report all untoward effects (e.g. respiratory or hemodynamic instability, adverse reaction to drugs, altered level of consciousness, prolonged drug effect, etc.) to the responsible practitioner and intervene as ordered by the responsible practitioner.
3. If a patient’s condition deteriorates, STAT page or call the direct contact phone line for the responsible practitioner; consider calling the rapid response or code team if appropriate.
4. For urgent or emergent assistance for patients receiving sedation or anesthesia by an anesthesiologist, emergency protocols delineated in the perioperative policies and procedures will apply.
VII. Staffing Requirements
Individuals ordering, administering, and/or supervising moderate and/or deep sedation must be qualified and have the appropriate credentials to manage patients at whatever level of sedation is achieved, either intentionally or unintentionally. Residents ordering sedation must be supervised by an attending physician who is also credentialed to manage that planned level of sedation.

This policy applies to: Lucile Packard Children’s Hospital
Date Written or Last Revision:JUNE 2011
Name of Policy: Sedation Policy
Page 11 of 24 Departments Affected: All Departments
A. Physician, Physician’s Assistant, and Nurse Practitioner Competency
Requirements Privileges for Minimal Sedation: 1. Completion of a sedation teaching module. 2. Successful completion of a written examination to test the
knowledge of medications being given, and principles of physiologic monitoring including the interpretation of ECG and arrhythmia recognition.
Privileges for Moderate Sedation 1.
Must meet all Criteria for Minimal Privileges
2. Demonstration of sedation and airway skills supervised by anesthesiologist or intensive care physician credentialed for deep sedation: may take place in simulated environment with infant sized simulation equipment or in operating/sedation environment with a patient.
Privileges for Deep Sedation
1. Must meet all criteria for Moderate Sedation 2. Must be board certified or in active participation in pediatric critical
care, or adult critical care, or board certified or board eligible in anesthesiology
Physician Trainees 1.
must meet all criteria for minimal sedation
2. must be immediately supervised by physician credentialed in the level of sedation/anesthesia planned for the procedure
B. Nursing Competency Requirements:
Only RNs who complete Sedation Level II competency may administer minimal or moderate sedation at LPCH. To achieve Sedation Level II, the RN must complete:
1. The Sedation Level I Health Stream training module and post-test on an annual basis

This policy applies to: Lucile Packard Children’s Hospital
Date Written or Last Revision:JUNE 2011
Name of Policy: Sedation Policy
Page 12 of 24 Departments Affected: All Departments
2. The Sedation Level II validation of sedation skills through supervised demonstration. Validation of skill will be completed through a simulation-based training and testing curricula or by observation of skill by a Sedation Level II competent RN.
C. Personnel 1. Responsible practitioner: Each patient undergoing sedation must
have a credentialed practitioner immediately available to respond to adverse events occurring during the sedation or during recovery from sedation. The responsible practitioner must have at a minimum competency-based education, training, and experience in evaluating patients before moderate or deep sedation and anesthesia, and in performing moderate or deep sedation, including rescuing patients who slip into a deeper than desired level of sedation or analgesia. This includes the following:
a. Moderate sedation: qualification to rescue patients from deep sedation, and competence to manage a compromised airway and provide adequate oxygenation and ventilation.
b. Deep sedation: qualification to rescue patients from general anesthesia and are competent to manage an unstable cardiovascular system as well as a compromised airway and inadequate oxygenation and ventilation.
2. Designated sedation monitor: A designated physician, physician’s assistant, nurse practitioner, RN, or licensed practitioner other than the person performing the procedure must be present to administer sedative drugs, observe the patient, measure and document the required physiologic parameters throughout the procedure, and assist in any supportive or resuscitative measures as required.
3. Medication administration:
a. A physician, physician's assistant, nurse practitioner, or RN may administer the medications used for minimal or moderate sedation.
b. A physician, or CRNA must either administer medications for deep sedation, or be present to give directed order for specific doses of medications to be given.

This policy applies to: Lucile Packard Children’s Hospital
Date Written or Last Revision:JUNE 2011
Name of Policy: Sedation Policy
Page 13 of 24 Departments Affected: All Departments
VIII. Performance Improvement:
Å. There will be periodic quality management evaluations of policy compliance, performance and outcome.
B. Related to sedation, all reported adverse events or adverse drug reactions will be reviewed; in addition, items to be reviewed, tracked, or audited will include cases in which the following occur:
1. Administration of naloxone, flumazenil,
epinephrine, or atropine.
2. Manual intervention to support airway or breathing
3. Unplanned admission to a higher level of care,
including unplanned admission of an outpatient
4. Cancellation of a procedure due to unsuccessful
sedation.
5. Cardiopulmonary resuscitation
6. Death.
IX. RELATED DOCUMENTS
LPCH Policies and Bylaws that May Apply to Sedation Cases A. Universal Protocol: Verification of Patient Identity, Correct Surgical Site
and Time Out
B. Discharge by Criteria, Outpatients and PACU Transfers Only
C. Code Blue Management
D. Anesthesia; Intra-Operative Care and Monitoring
E. Informed Consent Policy
F. Protocol for use of intravenous anesthetic agents by Critical Care Medicine physicians to facilitate procedures in non-intubated patients.

This policy applies to: Lucile Packard Children’s Hospital
Date Written or Last Revision:JUNE 2011
Name of Policy: Sedation Policy
Page 14 of 24 Departments Affected: All Departments
G. Housestaff Manual: Medications H. Policy : Admission of Infants after Anesthesia and Sedation
IX. APPENDICES
A. Example of Airway Assessment for Sedation and Analgesia B. American Society of Anesthesiologists Physical Status (PS) Classifications C. NPO Policy D. Intra-procedure Monitoring Requirements E. Request for Sedation Strategy That Differs from Sedation Policy F. Matrix for Sedation Locations at LPCH G. Pediatric WHO Checklist
X. DOCUMENT INFORMATION
A. Legal Authority/References 1. American Academy of Pediatric Dentistry (1997). Guidelines for
the elective use of pharmacologic conscious sedation and deep sedation in pediatric dental patients. Pediatric Dental Journal. 19:48-52.
2. American Academy of Pediatric Dentistry (1985). Guidelines for the elective use of conscious sedation, deep sedation, and general anesthesia in pediatric patients. Committee on Drugs Section on Anesthesiology. Pediatrics, 76(5) 317-321
3. American Academy of Pediatrics Committee on Drugs (1992). Guidelines for monitoring and management of pediatric patients during and after sedation for diagnostic and therapeutic procedures. Pediatrics 89:1110-1115.
4. American College of Emergency Physicians. (1998)Clinical policy for procedural sedation and analgesia in the emergency department Annals of Emergency Medicine 31 663-677.
5. American Dental Society of Anesthesiologists (1998). A. D. S. A. guidelines of intra-operative monitoring of patients undergoing conscious sedation, deep sedation and general anesthesia. Journal of Connecticut State Dental Association 62:210-211.

This policy applies to: Lucile Packard Children’s Hospital
Date Written or Last Revision:JUNE 2011
Name of Policy: Sedation Policy
Page 15 of 24 Departments Affected: All Departments
6. American Medical Association Council on Scientific Affairs: The use of pulse oximetry during conscious sedation (1993). JAMA 270:1463-1458.
7. American Society of Anesthesiologists (1996). Practice guidelines for sedation and analgesia by non-anesthesiologists. Anesthesiology 84:459-471.
8. American Society of Anesthesiologists.(2009) Standards: Continuum of Depth of Sedation/Definition of General Anesthesia and Levels of Sedation/analgesia. Accessed at: http://www.asahq.org/publicationsAndServices/standards/20.pdf
9. Chudnofsky CR (1997). Safety and efficacy of flumazenil in reversing conscious sedation in the emergency department; Emergency medicine conscious sedation study group. Academic Emergency Medicine. 4:944-50.
10. Coté CJ, et al. (2000). Adverse Sedation Events in Pediatrics: A critical Incident analysis of contributing factors. Pediatrics 105:805-14.
11. Coté CJ: Sedation for the pediatric patient (1994). Pediatric Clinics of North America 41: 31-58.
12. Holzman RS, et al. (1994). Guidelines for the sedation by non-anesthesiologists during diagnostic and therapeutic procedures. Journal of Clinical Anesthesia 6; 265-76.
13. Kao et al. (1999). A survey of post-discharge side effects of conscious sedation using chloral hydrate in pediatric CT and MR imaging. Pediatric Radiology. 29:287-90.
14. Macpherson CF, Lundblad LA (1997). Conscious sedation of pediatric oncology patients for painful procedures: development and implementation of a clinical practice protocol. Journal of Pediatric Oncology Nursing. 14:33-42.
15. Malviya S et al. (1997). Adverse events and risk factors associated with the sedation of children by nonanesthesiologists. Anesthesia & Analgesia 85:1207-13.
16. Mayers, DJ, et al. (1991). Chloral hydrate disposition following single-dose administration to critically ill neonates and children. Developmental Pharmacology and Therapeutics 16: 71-7.
17. Morton NS, et al. (1998). Development of a selection and monitoring protocol for safe sedation of children. Pediatric Anesthesia 8:65-8.

This policy applies to: Lucile Packard Children’s Hospital
Date Written or Last Revision:JUNE 2011
Name of Policy: Sedation Policy
Page 16 of 24 Departments Affected: All Departments
18. National Institutes of Health (1985). Consensus conference – anesthesia and sedation in the dental office Journal of American Medical Association 254:1073-1076.
19. Nelson, Jr. MD (1994). Commentary: Guidelines for the monitoring and care of children during and after sedation for imaging studies. American Journal of Radiology 160: 581-582.
20. Pediatric Committee of the American College of Emergency Physicians.(1994) Pediatric analgesia and sedation. Annals Emergency Medicine February 23: 237-250.
21. Somerson SJ, et al. (1995). Insights into conscious sedation. American of Journal of Nursing 95(6) 26-33,
22. Strain, et al. (1986). Administration of intravenous pentobarbital sodium for sedation in pediatric CT. Radiology 161:105-108.
23. Yaster M, et al. (1997). The Pediatric Pain and Sedation Handbook. St. Louis, MO: Mosby-Yearbook, Inc.
B. Author/Original Date LPCH Sedation Committee; 5/04 C. Distribution and Training Requirements 1. This policy resides in the Patient Care Manual of Lucile Packard
Children’s Hospital. Web URL: https://intranet.lpch.org/formsPoliciesReferences/policies/hospitalWide/ patientCare/sedationPolicy.html
2. New documents or any revised documents will be distributed to Patient Care Manual holders. The department/unit/clinic manager will be responsible for communicating this information to the applicable staff.
D. Review and Renewal Requirements This policy will be reviewed and/or revised every three years or as required
by change of law or practice. E. Review and Revision History 1/05; 11/06, Stephanie Martian, RN, Clinical Transformation, 09/07 E. Krane, 05/10 A. Honkanen, 6-2010, 6/2011 F. Approvals Sedation Committee; 11/06

This policy applies to: Lucile Packard Children’s Hospital
Date Written or Last Revision:JUNE 2011
Name of Policy: Sedation Policy
Page 17 of 24 Departments Affected: All Departments
Medical Executive Committee: 01/07; 10/11 Clinical Practice Committee; 1/07, 05/10
This document is intended for use by staff of Stanford Hospital & Clinics and/or Lucile Packard
Children’s Hospital. No representations or warranties are made for outside use.
Not for outside reproduction or publication without permission. Appendix A:
Example of Airway Assessment for Sedation and Analgesia
A. History 1. Previous problems with anesthesia or sedation 2. Stridor, snoring, or sleep apnea 3. Dysmorphic facial features (e.g. Pierre-Robin syndrome, Trisomy
21) 4. Advanced rheumatoid arthritis
B. Physical examination 1. Habitus - Obesity (especially involving the neck and facial
structures) 2. Head and neck - Short neck - Limited neck extension - Decreased hyoid-mental distance (<3cm in an adult) - Neck mass - Cervical spine disease or trauma - Tracheal deviation 3. Mouth - Small opening (< 3cm in an adult) - Protruding incisors - Loose or capped teeth - High arched palate - Macroglossia - Tonsillar hypertrophy - Uvula obscured by base of tongue or tonsils

This policy applies to: Lucile Packard Children’s Hospital
Date Written or Last Revision:JUNE 2011
Name of Policy: Sedation Policy
Page 18 of 24 Departments Affected: All Departments
4. Jaw - Micrognathia - Retrognathia - Trismus - Significant malocclusion
Appendix B:
American Society of Anesthesiologists Physical Status (PS) Classifications
PS-1: A healthy patient without illness or disease
PS-2: A patient with localized disease or a systemic disease in good control
(examples: VSD without CHF, juvenile onset diabetes mellitus in good control, asymptomatic reactive airway disease, localized or systemic infection under treatment)
PS-3: A patient with systemic disease that is not controlled
(examples: VSD with CHF, cystic fibrosis, cyanotic congenital heart disease, uncontrolled hypertension, infection with fever or sepsis)
PS-4: A patient with a localized or systemic disease that represents an immediate threat to life; a patient who is not expected to survive without the planned procedure
(examples: acute or end-stage organ failure, hypotension or shock, DKA, coma of any cause)
PS-5: A moribund patient who is not expected to survive with or without the planned procedure.
E: Added to above classifications to designate an unplanned emergency procedure (example: PS-2E)

This policy applies to: Lucile Packard Children’s Hospital
Date Written or Last Revision:JUNE 2011
Name of Policy: Sedation Policy
Page 19 of 24 Departments Affected: All Departments
Appendix C:
NPO Policy
All patients should be NPO prior to moderate and/or deep sedation, and should not have any risk factors for aspiration. The use of sedation must be preceded by an evaluation of food and fluid intake. For infants and children over 3kg in weight, minimum NPO* intervals are: A. > 8 hours for heavy solids B. > 6 hours for milk, formula, barium contrast, light solids C. > 4 hours for breast milk D. > 2 hours for clear liquids E. Pregnant and postpartum women require special consideration regarding
NPO* status; the minimum times above may be inadequate to assure gastric emptying
F. Patients with various medical conditions may require longer NPO times to ensure adequate gasric emptying; times will be adjusted at the discretion of the anesthesiologist or physician administering sedation as required.
For infants under 3kg in weight, the minimum NPO* interval depends upon routine feeding frequency: A. > than the usual duration between feedings for formula, breast milk,
barium contrast, etc. For example, if a former premature weighing 2 kg is fed formula or breast milk every 3 hours, then NPO time must be > 3 hours.
B. Formula and breast milk and fluids may be administered to the jejunum through a stoma, other than the nose or mouth continuously
* NPO here indicates nothing by mouth, nasogastric tube, or gastrostomy tube. Please note that the above instructions are meant to guide the practitioner. Many patients have special needs and these must be considered in regard to preparing them for anesthesia and / or sedation. The anesthesia nurse practitioner or the anesthesia resident (after 5pm ) should be consulted for questions related to NPO instructions.

This policy applies to: Lucile Packard Children’s Hospital
Date Written or Last Revision:JUNE 2011
Name of Policy: Sedation Policy
Page 20 of 24 Departments Affected: All Departments
Appendix D: Intraprocedure Sedation Level Recovery Parameter Minimal Moderate Deep Continuous Observation
Continuous Pulse Oximetry
Continuous ECG ETCO2 Blood Pressure q-15 min
Blood Pressure q-5 min
Documentation q5m
Documentation q15m

This policy applies to: Lucile Packard Children’s Hospital
Date Written or Last Revision:JUNE 2011
Name of Policy: Sedation Policy
Page 21 of 24 Departments Affected: All Departments
Appendix E:
Request for Sedation Strategy That Differs from Sedation Policy
The introduction of a new sedation technique or procedure that differs from this policy that improves the quality of care for patients, or the use of anesthetic agents such as propofol, ketamine, sodium thiopental, or etomidate for sedation, requires that a written request be formally submitted to the Sedation Committee. The following information and criteria must be included in a department's or division's request. Requests may be submitted to the Sedation Committee Chair via the LPCH Medical Staff Office 1. Names of supervising physician(s). 2. Location of the practice change. 3. Procedures for which the new procedure will be used. 4. Desired level of sedation. 5. Patient inclusion/exclusion criteria. 6. Proposed regimen: drug(s), dosage(s), route, and frequency of
administration. 7. Education plan for staff responsible for drug administration. 8. Desired outcome and monitoring plan: a. Purpose statement including pertinent background information. b. How will you measure an improvement over current practice?
(1) Include a summary of baseline measures that will be used to
determine the effectiveness of the changes (i.e. chart review of x patients).
(2) Specify the desired goal and outcome. 9. Results: Data must be presented to the Committee 6 months after
implementation.
All aspects of the current policy will apply unless a specific change in practice is proposed within the request. The Sedation Committee will review the request at its next quarterly meeting and notify the department/division of the Committee's decision in writing. All requests will be approved for a 6-month pilot period, after which pilot results must be presented to the Committee for final review and approval.

This policy Lucile
Name of PoSedation PoDepartmenAll Departm
AppeRequ
applies to: Packard C
olicy: olicy nts Affected:ments
endix F: Matuirements
Children’s
:
trix for Seda
s Hospital
ation Requireements and L
D
Locations
Date Writte
Page 2
n or Last RJUN
22 of 24
Revision:NE 2011

This policy Lucile
Name of PoSedation PoDepartmenAll Departm
AppeLocat
applies to: Packard C
olicy: olicy nts Affected:ments
endix F. (contions
Children’s
:
nt.):
s HospitalDDate Writte
Page 2
n or Last RJUN
23 of 24
Revision:NE 2011
This policy Lucile
Name of PoSedation PoDepartmenAll Departm
Appe WHO
applies to: Packard C
olicy: olicy nts Affected:ments
endix G:
O Surgical S
Children’s
:
afety Check
s Hospital
klist:
DDate Writte
Page 2
n or Last RJUN
24 of 24
Revision:NE 2011