series editors kaija vasala medica a - oulu
TRANSCRIPT

ABCDEFG
UNIVERS ITY OF OULU P.O.B . 7500 F I -90014 UNIVERS ITY OF OULU F INLAND
A C T A U N I V E R S I T A T I S O U L U E N S I S
S E R I E S E D I T O R S
SCIENTIAE RERUM NATURALIUM
HUMANIORA
TECHNICA
MEDICA
SCIENTIAE RERUM SOCIALIUM
SCRIPTA ACADEMICA
OECONOMICA
EDITOR IN CHIEF
PUBLICATIONS EDITOR
Senior Assistant Jorma Arhippainen
University Lecturer Elise Kärkkäinen
Professor Hannu Heusala
Professor Olli Vuolteenaho
Senior Researcher Eila Estola
Information officer Tiina Pistokoski
University Lecturer Seppo Eriksson
Professor Olli Vuolteenaho
Publications Editor Kirsti Nurkkala
ISBN 978-951-42-8873-9 (Paperback)ISBN 978-951-42-8874-6 (PDF)ISSN 0355-3221 (Print)ISSN 1796-2234 (Online)
U N I V E R S I TAT I S O U L U E N S I S
MEDICA
ACTAD
D 983
ACTA
Kaija Vasala
OULU 2008
D 983
Kaija Vasala
MATRIX METALLOPROTEINASEMMP-2 AND MMP-9 AND THEIR INHIBITORS TIMP-1 AND TIMP-2 IN BLADDER CARCINOMA
FACULTY OF MEDICINE,INSTITUTE OF CLINICAL MEDICINE, DEPARTMENT OF ONCOLOGY AND RADIOTHERAPY,UNIVERSITY OF OULU


A C T A U N I V E R S I T A T I S O U L U E N S I SD M e d i c a 9 8 3
KAIJA VASALA
MATRIX METALLOPROTEINASE MMP-2 AND MMP-9 AND THEIR INHIBITORS TIMP-1 AND TIMP-2IN BLADDER CARCINOMA
Academic Dissertation to be presented, with the assentof the Faculty of Medicine of the University of Oulu, forpublic defence in Auditorium 7 of Oulu UniversityHospital, on October 31st, 2008, at 12 noon
OULUN YLIOPISTO, OULU 2008

Copyright © 2008Acta Univ. Oul. D 983, 2008
Supervised byProfessor Taina Turpeenniemi-Hujanen
Reviewed byDocent Hanna MäenpääProfessor Teuvo Tammela
ISBN 978-951-42-8873-9 (Paperback)ISBN 978-951-42-8874-6 (PDF)http://herkules.oulu.fi/isbn9789514288746/ISSN 0355-3221 (Printed)ISSN 1796-2234 (Online)http://herkules.oulu.fi/issn03553221/
Cover designRaimo Ahonen
OULU UNIVERSITY PRESSOULU 2008

Vasala, Kaija, Matrix metalloproteinase MMP-2 and MMP-9 and their inhibitorsTIMP-1 and TIMP-2 in bladder carcinomaFaculty of Medicine, Institute of Clinical Medicine, Department of Oncology and Radiotherapy,University of Oulu, P.O.Box 5000, FI-90014 University of Oulu, Finland Acta Univ. Oul. D 983, 2008Oulu, Finland
AbstractBladder cancer when superficial has a good prognosis but it has a high recurrence risk and about10–15% of the superficial carcinomas will progress into muscle invasive or metastatic type. Themost powerful factor for predicting the behavior of bladder carcinoma is the stage of the tumor.Invasion to the lamina propria increases the risk of recurrence and progress to muscle-invasivetumor. Also grade of the tumor and tumor multiplicity associates with high risk for recurrence.New markers are still needed to find those patients who need more and better treatments to avoidthe recurrence and progress. The need for new non-invasive markers to diminish the need forfrequent cystoscopy in follow-up is also obvious.
Gelatinases MMP-2 and MMP-9 are known to associate to tumor invasion and progression.Also their tissue inhibitors TIMP-1 and TIMP-2 take part in these diversified processes andmetastasis formation. In the present work the expression and clinical value of gelatinases MMP-2and MMP-9 and their tissue inhibitors TIMP-1 and TIMP-2 were evaluated in bladder carcinoma.Primary tissue samples of 121 patients were analyzed for expression of MMP-2 and/or MMP-9using immunohistochemistry. The serum samples of 87 patients who were treated in the OncologyDepartment of Oulu University Hospital were collected and studied with ELISA. The controlgroup consisted of 44 healthy volunteers.
Overexperssion of MMP-2 protein correlated significantly to disease-specific survival andshowed an independent prognostic value as a biomarker. High MMP-9 expression insteadcorrelated to favorable overall survival of bladder cancer patients. Circulating proMMP-2, TIMP-2 and MMP-2:TIMP-2 complex levels were lower in cancer patients than in healthy volunteers incontrol group. High levels of all these three markers correlated with better prognosis in bladdercancer patients.
Keywords: bladder cancer, ELISA, invasion, prognostic marker, survival, MMP-2


"When life has gotten too serious we need to laugh, when we forget to laugh, life becomes too serious"
To Anni and Pentti

6

7
Acknowledgements
This present thesis project has been carried out at the Department of Oncology and Radiotherapy, University of Oulu, during the years 1998–2008.
First, I wish to express my sincere gratitude to my supervisor, Professor Taina Turpeenniemi-Hujanen, Head of the Department of Oncology and Radiotherapy, for giving me this opportunity to learn scientific research and introduce me the field of matrix metalloproteinase. Her knowledge and positive attitude has been a great help for me during all these years.
I express me special appreciation to docent Paavo Pääkkö for his encouraging attitude and fruitful collaboration in the field of pathology. It was joyful to watch beautiful immunohistochemical staining together.
I am most grateful to the reviewers’ docent Hanna Mäenpää, M.D., Ph.D and Professor Teuvo Tammela, M.D., Ph.D, for their careful revision of my thesis and valuable advice. I am also grateful to Mr. Risto Bloigu for advice in the statistical analyses and to Mrs. Anna Vuolteenaho, for correction of language and Mr. Kari Moilanen for helping to collect patients’ clinical data.
I wish to warmly thank my dear colleagues and all the staff at the Department of Oncology and Radiotherapy for their friendship during these many years I have been months away from clinical work.
I warmly thank all my research group colleagues, docent Ulla Puistola, docent Anne Talvensaari-Mattila, Ph.D Anne Väisänen, Ph.D Outi Kuittinen, Ph.D Henni Ruokolainen, Ph.D Marita Rauvala, Ph.D Paula Kuvaja, M.D. Sanna Hoikkala, M.D. Heli Pennanen, M.D. Milla Määttä, M.D. Maria Honkavuori and Sina Santala for their support and friendship during sunny and cloudy days. I am also mostly grateful to the laboratory staff Mrs. Kaisu Järvenpää, Mrs. Anne Bisi and Mrs. Tarja Raaska for their excellent work and companionship. With you I have been able to laugh in rainy days.
I wish to thank my dearest friend Annimaiju Pudas for everlasting friendship which has been lasted since we were four years old. I love you! I owe my thanks to – Mrs. Anna-Kaisa Lappi and Mrs. Kaisu Clarot and – to all of my friends for their tremendous support and friendship.
I also give my warmest thanks to my dear sister Mrs. Maija Liisa Peltokorpi and her dear family for support and love. My mother-in-low Mrs. Raili Vasala has been a grate help during all this years, so thank you.
Finally I wish to thank my husband Antti and our children, Aappo, Lauri and Emma. You are my sunshine. Without you life would be boring and empty.

8
This study was financially supported by the Cancer Society of Northern Finland and the Finnish Society for Therapeutic Radiology and Oncology, which are gratefully acknowledged.
Oulu, May 2008

9
Abbreviations
BCG Bacillus Calmette-Guérin BM basement membrane CSS cause-specific survival DFS disease-free survival DSS disease-specific survival DNA deoksiribonucleic acid ECM extracellular matrix EGF epidermal growth factor EGFR epidermal growth factor receptor EIA enzyme immune assay ELISA enzyme-linked immune assay FGF fibroblast growth factor GC gemcitabine-cisplatin IH immunohistochemistry kDa kilodalton MMP matrix metalloproteinase mRNA messenger ribonucleic acid MT-MMP membrane-type matrix metalloproteinase MVAC metotrexate-vinblastine-adriamycin-cisplatin OS overall survival PBS phosphate-buffered saline PCR transcriptase-polymerase chain reaction PDGF platelet derived growth factor PR partial response RB retinoblastoma RECK reversion-inducing cysteine-rich protein with kazal motifs ROC receiving operating characteristics RR risk ratio SD stable disease SH zinc-interacting thiol group TCC transitional cell carcinoma TFPI tissue factor inhibitor TGF transforming growth factor TIMP tissue inhibitor of matrix metalloproteinase TNF tumor necrosis factor

10
TNM Tumor-Node-Metastasis TUR transurethral resection UICC International Union Against Cancer VEGF vascular endothelial growth factor WHO World Health Organization

11
List of original articles
This thesis is based on following articles, which are referred to in the text by their Roman numerals:
I Vasala K, Pääkkö P & Turpeenniemi-Hujanen T (2003) Matrix metalloproteinase-2 immunoreactive protein as a prognostic marker in bladder cancer. Urology 62: 952–957.
II Vasala K & Turpeenniemi-Hujanen T (2007) Serum tissue inhibitor of metalloproteinase-2 (TIMP-2) and matrix metalloproteinase-2 in complex with the inhibitor (MMP-2:TIMP-2) as prognostic markers in bladder cancer. Clin Biochem 40(9–10): 640–644.
III Vasala K, Pääkkö P & Turpeenniemi-Hujanen T (2008) Matrix metalloproteinase 9 (MMP-9) immunoreactive protein in urinary bladder cancer: A marker of favorable prognosis. Anticancer Res 28(3B): 1757–1761.
IV Vasala K, Kuvaja P & Turpeenniemi-Hujanen T (2008) Low circulating levels of proMMP-2 are associated with adverse prognosis in bladder cancer. Tumor Biol 29: 279–286.

12
13
Contents
Abstract Acknowledgements 7 Abbreviations 9 List of original articles 11 Contents 13 1 Introduction 15 2 Review of literature 17
2.1 Bladder cancer......................................................................................... 17 2.1.1 Epidemiology and risk factors...................................................... 17 2.1.2 Diagnosis and staging................................................................... 18 2.1.3 Prognostic factors ......................................................................... 19 2.1.4 Treatment of bladder cancer ......................................................... 20
2.2 Tumor invasion and metastasis ............................................................... 22 2.3 Gelatinases and their natural tissue inhibitors......................................... 24
2.3.1 The matrix metalloproteinase (MMP) gene family ...................... 24 2.3.2 Matrix metalloproteinase-2 and -9 ............................................... 26 2.3.3 Regulation of gelatinase activity .................................................. 29 2.3.4 The prognostic role of gelatinases and their inhibitors in
cancer patients .............................................................................. 30 2.3.5 Tissue inhibitors of metalloproteinases in bladder cancer............ 31
3 Aims of the present study 35 4 Materials and methods 37
4.1 Patients and tissue and serum samples.................................................... 37 4.2 Immunohistochemistry............................................................................ 37
4.2.1 Immunohistochemical staining..................................................... 37 4.2.2 Evaluation of the immunostaining................................................ 38
4.3 Enzyme-linked immunoassay ................................................................. 38 4.4 Statistical analysis ................................................................................... 40 4.5 Ethical aspects......................................................................................... 40
5 Results 41 5.1 Tumor tissue expression of MMP-2 and MMP-9 immunoreactive
protein in bladder carcinoma (I, III)........................................................ 41 5.2 Comparison of the levels of circulating MMP-2, TIMP-2 and
MMP-2:TIMP-2 complex in patients and controls (II, IV)..................... 41

14
5.3 Correlation of the MMP-2, MMP-9, TIMP-2 and MMP-2:TIMP-2 complex immunoreactive proteins with the traditional clinico-pathological markers ............................................................................... 43 5.3.1 Tissue immunoreactive proteins for MMP-2 and MMP-9
(I, III) ............................................................................................ 43 5.3.2 Circulating immunoreactive proteins for MMP-2, MMP-9,
TIMP-1, TIMP-2 and MMP-2:TIMP-2 complex (II, IV) ............. 44 5.4 The prognostic value of tumor tissue gelatinases and their tissue
inhibitors in bladder cancer ..................................................................... 45 5.4.1 Tissue MMP-2 and MMP-9 as prognostic markers (I, III) ........... 45 5.4.2 Circulating proMMP-2, TIMP-2 and MMP-2:TIMP-2
complex as prognostic markers in bladder cancer (II, IV) ........... 48 6 Discussion 51
6.1 The prognostic value of MMP-2 and MMP-9 immunoreactive protein in bladder carcinoma................................................................... 51 6.1.1 MMP-2 ......................................................................................... 51 6.1.2 MMP-9 ......................................................................................... 52
6.2 The prognostic role of circulating MMP-2, its inhibitor TIMP-2 and their complex (MMP-2:TIMP-2) in bladder cancer ......................... 54 6.2.1 MMP-2, TIMP-2 and MMP-2:TIMP-2 complex in bladder
cancer patients and in healthy controls......................................... 54 6.2.2 MMP-2 ......................................................................................... 54 6.2.3 TIMP-2 ......................................................................................... 55 6.2.4 MMP-2:TIMP-2 ........................................................................... 56
7 Conclusions 57 References 59 Original articles 73

15
1 Introduction
Bladder cancer is a worldwide health problem, causing an estimated 375,000 bladder cancer cases annually. It is more common in industrial countries than in developing countries, and 77% of the tumors occur in men. (Parkin et al. 2005) The incidence of bladder cancer has been rising gradually in recent years (Finnish Cancer Registry 2007). Bladder cancer is especially common in eastern and southern European countries as well as in Denmark, where smoking has been common. Chronic infection with Schistostoma hematobium explains partly the high prevalence of bladder cancer, particularly the squamous cell type, in Africa and the Middle East (Parkin et al. 2005). The majority, 90–95%, of the bladder carcinomas are urothelial carcinomas (transitional cell carcinomas, TCC). About 75% of the bladder cancer cases are superficial, and most of them invade only the superficial mucosa and are usually well differentiated. Recurrence risk is at its highest during the first year after treatment, being over 80%. About 10–15% of the superficial bladder carcinomas will progress into muscle invasive or metastatic type. According to different studies, the 5-year overall survival rate for patients with muscle invasive disease after radical cystectomy is about 50%. (Stein et al. 2001; Cheng et al. 2000)
There are many markers associating with the progression of bladder carcinoma, such as depth of invasion, stage, grade and multiplicity. Unfortunately they are inaccurate, which is why more clinical prognostic markers are needed.
Matrix metalloproteinases are a family of endopeptidases that are capable of degrading most components of the extracellular matrix (ECM) (Steteler-Stevenson et al. 1993; Nagase & Woessner 1999). Of them, gelatinase-A (MMP-2) and gelatinase-B (MMP-9) are able to degrade extracellular matrix protein, including type IV collagen. Gelatinases have been linked to cell invasion and the process of metastasis (Stetler-Stevenson 2001). Tissue inhibitors of matrix metalloproteinases (TIMPs) take part in the regulation of MMPs. TIMP-1 and TIMP-2 are known inhibitors of MMP-2 and MMP-9, but can also take part in the activation of MMPs. (Gomez et al. 1997) They are capable of acting as growth factors and take part in angiogenesis and apoptosis as regulators (Fassina et al. 2000).
The present study was designed to evaluate the expression and prognostic value of gelatinases and their tissue inhibitors in bladder cancer. These markers were studied in both tumor tissue and serum samples from bladder cancer patients.

16
17
2 Review of literature
2.1 Bladder cancer
Bladder cancer is the ninth most common cancer when combining both sexes. Among men it is the forth and among female the eight most common malignancy in the Western world. (Parkin et al. 2005) In Finland in the year 2006, there were 864 bladder cancer cases (Cancer Registry in Finland1). The incidence rate was higher among males compared with the female population, 13 per 100,000 and 1.3 per 100,000, respectively (Cancer Registry in Finland). The median age at diagnosis is 65 to 70 years in Western countries (Parkin et al. 2005).
2.1.1 Epidemiology and risk factors
Cigarette smoking is the most well-established risk factor for bladder cancer. Smokers seem to have a four times higher risk for developing bladder cancer than non-smokers (Table 1). Ex-smokers’ risk is about two times higher compared to non-smokers (Zeegers et al. 2004; Bjerregaard et al. 2006).
Table 1. Smoking and bladder cancer (modified from Kirkali et al. 2005).
Risk factors
Cigarette smoking increases bladder cancer risk 2- to 4-fold
30–50% of all bladder cancer is caused by cigarette smoking
Latency period is approximately 20–30 years
Quitting smoking → risk decreases immediately
Unfiltered cigarettes increase the risk 35–40% vs. filtered cigarettes
Pipe/cigar smoking → higher risk? (inhalation pattern)
Snuff or chewing tobacco→ no elevated risk
It is not known exactly how the bladder carcinogenesis works in smokers. Of the agents that are present in tobacco smoke the aromatic amines are primary carcinogens for bladder cancer (Marcus et al. 2000; Gurigliano et al. 1996). N-acetylation is mainly regulated by enzyme NAT2 and lack of two functional NAT2 alleles confers the slow acetylation phenotype (Ross et al. 1996). It has been shown that slow acetylators have an elevated cancer risk (Marcus et al. 2000).
1http://www.cancerregistry.fi
18
Occupation seems to be the second most important risk for bladder cancer. It has been estimated that occupational exposure explains the etiology for 20% of all bladder cancer cases (Vineis et al. 1991). Individuals belonging to high-risk population are painters, metal, textile and electrical workers. A minor risk is observed among miners, transport operators, excavating-machine operators as well as concierges and janitors. (Kogevinas et al. 2003)
There are different opinions concerning total fluid consumption and bladder cancer risk. It seems that total fluid intake is not associated with elevated bladder cancer risk (Zeegers et al. 2001). The relation between coffee drinking and the risk of bladder cancer has often been studied. There seems to be a weak correlation between coffee drinking and bladder cancer risk even after adjustment for age, sex and smoking (Negri et al. 2001).
Cyclophosphamid, an alkylating agent used in the treatment of malignant neoplasms, and radiotherapy both increase the risk of bladder cancer (Brenner et al. 2006; Kaldor et al. 1995).
2.1.2 Diagnosis and staging
In about 80% of the cases, hematuria is the first sign of bladder cancer. Hematuria can be either gross or microscopic (Amling 2001). The cornerstone for diagnosis is cystoscopy. During cystoscopy, random biopsies or transurethral resection (TUR) are performed. TUR is diagnostic but also therapeutic.
The majority, 90–95%, of bladder carcinomas are urothelial carcinomas. One third of urothelial carcinomas may contain squamous cell, spindle cell or adenocarcinomatous elements (Braud et al. 2002). Pure squamous cell carcinoma, adenocarcinoma and small-cell carcinoma are rare. About 75% of the bladder cancer cases are superficial and most of them invade only the superficial mucosa and are usually well differentiated. Recurrence risk is at its highest during the first year after treatment, being over 80%. About 10–15% of the superficial bladder carcinoma cases will progress into muscle invasive or metastatic type. (Braud et al. 2002)
Staging of bladder cancer is done once the diagnosis is confirmed. Its role is important when determining the prognosis and optimal treatment. Staging is usually done according to the International Union Against Cancer (UICC) classification system (Hermanek et al. 2002) (Table 2). The staging is used in bladder carcinomas but not in papillomas. Physical examination, imaging and endoscopy are needed to assess the TNM (tumor – node – metastasis) categories.

19
The depth of the invasion determines the T category: a T4 tumor invades other organs such as the prostate, uterus, vagina or the abdominal wall. The staging of lymph-node involvement is determined by the number and size of the lymph nodes. Together, tumor size, nodal involvement and distant metastasis determine the stage (I, II, III or IV). The grading of bladder cancer is done according to the World Health Organization reference center (Mostofi 1973) (Table 3).
Table 2. TNM classification of bladder tumors (modified from UICC TNM classification).
TNM class Definition/invasion level
Ta Non-invasive papillary
Tis In situ “flat tumor”
T1 Subepithelial connective tissue
T2 Muscularis (tumor invades muscle)
T2a Inner half (tumor invades superficial muscle)
T2b Outer half (tumor invades deep muscle)
T3 Beyond muscularis (tumor invades perivesical tissue)
T3a Microscopically
T3b Macroscopically (extravesical mass)
T4 Tumor invades other organs
T4a Prostate, uterus, vagina
T4b Pelvic wall, abdominal wall
N1 Single ≤ 2cm
N2 Single > 2 to 5cm, multiple ≤ 5cm
N3 > 5cm
M0 No distant metastasis
M1 Distant metastasis
Table 3. 1973 World Health Organization (WHO) classification for grading of papillary urothelial neoplasm of the bladder (modified from Mostofi 1973).
Grade Histologic features
Grade 1 carcinoma Tumors with the least degree of cellular anaplasia compatible with diagnosis of
malignancy
Grade 2 carcinoma Histologic features between grades 1 and 2
Grade 2 carcinoma Tumors with the most severe degrees of cellular anaplasia
2.1.3 Prognostic factors
The tumor stage is known to be the most powerful effector of the prognosis. The first ones that found the association between the depth of invasion and tumor

20
progression were Jewett and Strong in 1946. This fact has later been proven in many studies (Pagano et al. 1987; Ozen et al. 1986). Invasion to lamina propria increases the risk of recurrence and progress to muscle-invasive tumors (Kimeney et al. 1993). Higher tumor grade associates with an increased risk of recurrence and muscle invasion (Parmar et al. 1989; Kiemeney et al. 1993). Also tumor multiplicity associates with a higher risk for recurrence and shortens the time to the first recurrence (Fosså et al. 1985; Kimeney et al. 1993).
Mutations of the p53 gene are common genetic defects in human cancers. In some studies, p53 mutation correlates strongly with higher grade and stage in urothelial carcinomas (Habuchi et al. 1992). Shortened survival has been seen in patients with altered p53 expression (Esrig et al. 1994). On the other hand, p53-changes are related to tumors with aggressive potential (Soini et al. 1993). In a meta-analysis that included 117 studies of p53 in bladder cancer it could be seen that changes in p53 are only weakly related to higher recurrence rate, progression and mortality in bladder cancer (Malats et al. 2005).
Other tumor-suppressor molecules, such as pRB (retinoblastoma), also associate with poorer tumor-free survival rate (Logothesis et al. 1992). Several other proliferation and metastasis-associated molecules such as EGFR, e-cadherin, cyclin p21, Kip1 and apoptosis-related molecules have also shown potential prognostic value when recurrence rate, metastatic potential of bladder carcinoma and survival of bladder cancer patients have been studied (Habuchi et al. 2005).
2.1.4 Treatment of bladder cancer
Superficial bladder cancer
The standard treatment of the superficial bladder cancer is transurethral resection (TUR). In TUR the endoluminal lesion and the underlying muscle forming the bladder wall is removed. The pathologist gives the depth of the invasion in order to determine the final treatment modality. Superficial bladder cancers usually have a low grade and the prognosis is good. The 5-year survival rate is expected to be as high as 95%, although the recurrence rate is more than 80% in the first year after diagnosis and about 10–15% of the diseases will progress into muscle-invasive or metastatic disease (Cheng et al. 2000; Stein et al. 2001). The majority, 90–95%, of the bladder carcinomas are urothelial carcinomas. One third of

21
urothelial carcinomas may contain squamous cell, spindle cell or adenocarcinomatous elements. Of the bladder cancer 5–6% is squamous cell carcinoma, adenocarcinoma and small-cell carcinoma are rare (Braud et al. 2002). It is shown that intravesical therapy can reduce the recurrence rate of superficial bladder cancer (Kaasinen et al. 2003; Lamm 2000). In some studies this treatment also seems to enhance the overall survival (Herr et al. 1995). The most powerful drugs used in therapy are Bacillus Calmette-Guérin (BCG), epirubicin and mitomycin C. Radical cystectomy is recommended for the high-risk patients with multifocal grade 3 tumors. Despite intravesical therapy, a radical cystectomy is also recommended with tumor recurrence. Cystectomy may be contraindicated due to patients’ high age or poor medical condition. In these cases radical radiotherapy may be considered as a treatment option.
Muscle-infiltrative bladder cancer
Radical cystectomy is the standard treatment for muscle-invasive bladder cancer (Herr et al. 2001). Surgery offers long-term survival for patients with muscle-invasive bladder cancer. Tumor size and margin status, stage and lymph node status determine the prognosis (Cheng et al. 2000). Extended pelvic lymphadenectomy during radical cystectomy provides improved prognostic information and probably survival benefit for patients with advanced or lymph node positive bladder carcinoma (Leissner et al. 2000).
After cystectomy the 5-year survival rate in muscle-invasive bladder cancer is about 50%, including all stages in different series. Both neo-adjuvant and adjuvant therapy have been studied in many trials. Randomized trials have shown a modest survival benefit with the use of cisplatin-based neo-adjuvant or adjuvant chemotherapy (Winquist et al. 2004; Sternberg et al. 2005).
There are also some studies showing that chemoradioterapy with cisplatin-based chemotherapy after transurethral surgery can be an alternative to cystectomy. In non-randomized phase I/II trials it seems that long-term survival is same in both groups. (Kaufman et al. 2000; Shipley et al. 2002)
Metastatic bladder cancer
Systemic chemotherapy is the only treatment that may result in long-term survival in some patients with metastatic bladder carcinoma. In the 1980s the combination of methotrexate, vinblastine, adriamycin and cisplatin (MVAC) was introduced,

22
and it was shown to increase the short-term survival rate of patients with advanced cancer, median survival being 13 months (Sternberg et al. 1985). Since then no chemotherapy combination has been found to be able to increase the survival. The combination of gemcitabine and cisplatin (GC) has proven to be effective and less toxic than MVAC (von der Maase et al. 2000). There is a need to develop new, better agents for the treatment of bladder carcinoma patients, especially for those renal function or overall health is not suitable for cisplatin-based chemotherapy. Regimens like inhibitors of epidermal growth factors (EGF), inhibitors of vascular endothelial growth factors (VEGF), antifolate agents, vinflunine (a vinca alkaloid) and bortezomid, a specific inhibitor of the 20S proteosome, are under clinical trials. We will see in the future whether some of them are more effective and less toxic than MVAC or GC in metastatic bladder cancer, and whether there are patient groups among metastatic bladder cancer patients that could benefit from the use of these agents.
2.2 Tumor invasion and metastasis
The ability to invade to other tissues and spread to distant organs is characteristic for cancer cells. The extracellular matrix (ECM) is the first barrier that cancer cells must cross in order to metastasize. First they pass through the epithelial basement membrane; after that the cancer cells must invade into the surrounding stroma. Thereafter they enter blood vessels or lymphatics and extravasate to distant organs to make new proliferating tumors. (Kleiner & Stetler-Stevenson 1999; Egeblad & Werb 2002) (Fig. 1) This process is composed of degradation of ECM and cell adhesion, but also angiogenesis in the early stages of tumor development (Liotta et al. 1980; Turpeenniemi-Hujanen et al. 1985; Tryggvasson et al. 1993).

23
Fig. 1. MMPs in tumor progression (modified from Nelson et al. 2000).
MMPs are thought to facilitate invasion and metastasis by degradation of ECM components. MMPs also mediate the activation of growth factors, suppression of tumor cell apoptosis, and destruction of chemokine gradient development by host immune response or the release of angiogenic factors. (Egeblad & Werb 2002; Hojilla et al. 2003) MMPs can also target substrates and influence the apoptotic process, which is also important for tumor prognosis (Witty et al. 1995). Basement membrane undergoes constant remodeling, and MMPs have a central role in maintaining the integrity of the ECM by removing undesired proteins (Kleiner & Stetler-Stevenson 1999). Other groups that are significant in protein degradation are aspartate and cysteine-dependent proteinases as well as serine proteinases. Aspartate and cysteine-dependent proteinases are mainly involved in the intracellular proteolysis, and serine and matrix metalloproteinases in extracellular proteolysis. (Curran & Murray 1999)

24
2.3 Gelatinases and their natural tissue inhibitors
2.3.1 The matrix metalloproteinase (MMP) gene family
Matrix metalloproteinases constitute a family of 25 zinc-dependent proteolytic enzymes, which are capable of degrading the extracellular matrix (ECM). 24 of the MMPs have been found among vertebrates and 23 in humans (Visse & Nagase 2003). There are some major similarities in the structure of all members of the MMP family (Table 3). They all have an N-terminal signal sequence followed by a propeptide domain and a catalytic domain. The catalytic domain contains the zinc-binding motif. Most of the MMPs, with the exception of MMP-7, MMP-23 and MMP-26, have a hemopexin/vitronectin-like domain with a role in binding of TIMP. (Visse & Nagase 2003; Sternlicht & Werb 2001) (Fig. 2) MMPs can be divided into six subgroups: collagenases, gelatinases, stromelysins, matrilysins, membrane-type MMPs (MT-MMPs) and non-classified MMPs such as MMP-12, which is essential for macrophage migration. (Visse & Nagase 2003)

25
Table 4. Matrix metalloproteinases and their substrates (modified from Nagase, Visse & Murphy 2006; Visse & Nagase 2003).
Enzyme MMP Main substrates
Collagenase-1 MMP-1 types I, II, III, IV, VII, VIII and X collagen, gelatin, entactin, perlecan,
laminin, casein, proMMP-1, -2, -9
Gelatinase-A MMP-2 gelatin, types I, III, IV, VII, X, and XI collagen, elastin, fibrinogen,
laminin, aggregan, vitronectin, decorin, plasminogen
Stromelysin-1,
Transin-1
MMP-3 aggregan, laminin, gelatin, fibronectin, types III, IV, V, IX, X, XI and
XVIII collagen
Matrilysin-1 MMP-7 fibronectin, laminin, gelatin, aggregan, types I, IV, IX, X, XI and XVIII
collagen
Collagenase-2
Neutrophil
collagenase
MMP-8 types I, II, III, VI and X collagen, gelatin, entactin, aggregan, tenascin,
proMMP-8
Gelatinase-B MMP-9 gelatin, types I, IV, VII, X, XI and XVIII collagen, elastin, laminin,
fibronectin, vitronectin, proMMP-2, -9
Stomelysin-2,
Transin-2
MMP-10 types I, III and IV collagen, gelatin, elastin, proMMP-1,-8,-10
Stromelysin-3 MMP-11 fibronectin, laminin, aggregan, gelatin
Macrophage
elastase,
metalloelastase
MMP-12 elastin, types I and IV collagen, fibronectin, laminin, proteoglycans,
fibrinogen
Collagenase-3 MMP-13 types I, II, III, VII, X and XVII collagen, gelatin, entactin, tenascin,
aggregan
MT1-MMP MMP-14 types I, II and III collagen, gelatin, laminin, aggregan, proMMP-2, -13
MT2-MMP MMP-15 proteoglycans, proMMP-2
MT3-MMP MMP-16 type III collagen, fibronectin, proMMP-2
MT4-MMP MMP-17 gelatin, fibrinogen, proMMP-2
Collagenase-4
(Xenopus)
MMP-18 types I, II and III collagen, gelatin
Stomelysin-4 MMP-19 types I and IV collagen, gelatin, laminin, tenascin
Enamelysin MMP-20 amelogenin, aggregan, laminin
XMMP (Xenopus) MMP-21 gelatin
CMMP (Chicken) MMP-22 gelatin, casein
Ca-MMP
(Cysteine array)
MMP-23 gelatin
MT5-MMP MMP-24 fibronectin, gelatin, proMMP-2
MT6-MMP MMP-25 type IV collagen, gelatin, proMMP-2, 9
Matrilysin-2,
Endometase
MMP-26 type IV collagen, gelatin, proMMP-9
CMMP (Gallus) MMP-27
epilysin MMP-28 casein

26
Fig. 2. Domain structure of the gelatinases. Pre = signal sequence; Pro = propeptide with zinc ligating thiol (SH) group; Fi = fibronectin like collegen; Zn = zinc-binding site; H = hinge region; Hemopexin domain linked by disulfide (S) bond (modified from Sounni et al. 2003).
MMPs are involved in many physiological processes, such as embryonic growth and tissue morphogenesis, during which they can appear in embryos during the early stage of implantation (Turpeenniemi-Hujanen et al. 1995; Alexander et al. 1996). It is also known that MMPs play an important role in tissue remodeling, wound healing, bone resorption and mammary gland involution (Ravanti & Kähäri 2000). Moreover, the knowledge of their role in angiogenesis and apoptosis is expanding (Folgueras et al. 2004). MMPs also contribute to development and progression of many pathological conditions like rheumatoid arthritis, coronary artery disease and cancer (Libby 1995, Thompson 1995, Nagase & Woessner 1999).
2.3.2 Matrix metalloproteinase-2 and -9
MMP-2 (Gelatinase A, 72kDa type IV collagenase) is a widely studied matrix metalloproteinase. It was first described and purified from highly metastatic murine tumors (Liotta et al. 1979; Salo et al. 1983) and cultured human melanoma cells (Höyhtyä et al. 1990). MMP-2 is abundantly expressed in fibroblasts, endothelial and epithelial cells (Vartio et al. 1982; Salo & Oikarinen 1985; Hipps et al. 1991). Gelatinases are secreted as proenzymes and they need to be activated for catalytic activity. Most MMPs can be activated extracellularly by other already activated MMPs or serine proteinases. MMP-2 is activated at the cell surface and the activation is mediated by the membrane-type metalloproteinase-1 (MT1-MMP). (Ward et al. 1994; Strongin et al. 1995; Visse
27
& Nagase 2003). MMP-2 participates in extracellular matrix degradation (ECM) having a wide range of substrates. It is able to degrade type I, IV, V, VII and X collagens, laminin, elastin, fibronectin and proteoglycans. (Nagase et al. 1999; Woessner 1999; Sternlicht et al. 2001).
MMP-9 (Gelatinase B, 92kDa type IV collagenase) was first purified from human macrophages (Vartio et al. 1982). MMP-9 expression is limited to osteoclasts, macrophages, trophoblasts, hippocampal neurocytes and migrating keratinocytes and it is controlled by growth factors, chemokines and other stimulatory signals (Hipps et al. 1991; Mohan et al. 1998; Munaut et al. 1999). MMP-9 is secreted as an inactive precursor form, proMMP-9. It forms a tight complex with TIMP-1 and TIMP-3. The complex of proMMP-9 and TIMP-1 is a potential inhibitor of MMPs. (Visse et al. Nagase 2003; Nagase et al. 2006) Another activation mechanism is plasminogen/MMP-3 mediated activation. Plasmin can also directly activate proMMP-9 (Mazzieri et al. 1997; Ramos-De Simone et al. 1999).
Although TIMPs are naturally occurring known inhibitors of matrix metalloproteinases that bind MMPs, they also have a role in the activation of certain MMPs. Therefore the TIMPs are naturally occurring inhibitors that bind MMPs. TIMP-1, TIMP-2, TIMP-3 and TIMP-4 have been identified in vertebrates. (Brew et al. 2000) They consist of 184–194 amino acids and have an N-and C-terminal domain. The N-terminal domain folds as a separate unit and can inhibit MMPs (Leco et al. 1994; Visse & Nagase 2003; Björklund et al. 2005). TIMPs are divided into an N-terminal and a C-terminal subdomain, each containing three conserved disulfide bonds and the N-terminal domain. TIMPs inhibit the MMPs proteolytic activity by forming non-covalent 1:1 stoichiometric complexes. TIMP-1, TIMP-2 and TIMP-4, but not TIMP-3, present in soluble form. TIMP-3 is bound to the matrix. (Brew et al. 2000; Visse & Nagase 2003; Nagase et al. 2006) Although all different TIMPs bind tightly to MMPs there are still some differences between them in solubility, regulation of expression and interaction with the proenzyme form of MMPs (Corcoran et al. 1995; Brew et al. 2000). (Table 4)
Unlike TIMP-1, TIMP-2 and TIMP-3 are effective inhibitors of MT-MMPs. TIMP-3 is also a good inhibitor of tumor necrosis factor-α converting enzyme (TACE) (Amour et al. 1998). TIMPs are able to form complexes with the proMMPs, which supports their role in the activation process of MMPs. TIMP-1 forms a specific complex with proMMP-9. The function of the complex is not clear, but it could play a role in the activation of proMMP-9, as is the case with

28
the TIMP-2/MMP-2 complex. The TIMP-2/MMP-2 complex is known to play an important part in the cell-surface activation of proMMP-2. (Goldberg et al. 1992; Murphy et al. 1997; Nagase et al. 1998)
TIMPs also have effects on cell growth and survival. Sobeu et al. have shown that TIMP-1 and TIMP-2 stimulate the bone-resorbing activity of osteoclasts through tyrosine kinase and MAP kinase pathways (Sobue et al. 2001). The cell-growth promoting effects of TIMP-1 and TIMP-2 have been shown in many normal and malignant cell lines (Corcoran & Stetler-Stevenson 1995; Yamasita et al. 1996; Wang et al. 2002). It is thought that TIMP-2 acts through specific, saturable high-affinity receptors and links to G protein and cAMP signaling pathways (Corcoran & Stetler-Stevenson 1995). TIMP-1, TIMP-2 and TIMP-3 are known to reduce tumor cell growth (Gomez et al. 1997; Ahonen et al. 1998; Baker et al. 1999). On the other hand, some TIMPs are associated with tumor progression (Stetler-Stevenson 1997; Jiang et al. 2001). Biological activities of TIMPs are independent of the MMP-inhibitory activity (Ahonen et al. 1998; Valente et al. 1998; Fasisina et al. 2002). TIMP-2 can promote apoptosis in an in vivo colorectal cancer model (Brand et al. 2000), but it has controversially been shown to protect B16 melanoma cells from apoptosis (Ahonen et al. 1998; Valente et al. 1998).
TIMPs can inhibit most MMPs and as such one of their roles is to limit proteolysis during ECM modeling. However, it is now known that the role is not simple. There are studies that show TIMP-4 to be potential antiangiogenic agent as it is able to inhibit tumor growth, angiogenesis and metastasis in a xenograft model of mammary tumor genesis in mice (Wang et al. 2001). These findings on TIMPs’ potential role in inhibiting tumor growth and angiogenesis have led to formation of synthetic matrix metalloproteinase inhibitors. Unfortunately, no major significant benefit has been seen so far in clinical trials of cancer treatment.
Table 5. Common and unique features of TIMPs (modified from Baker et al. 2002).
TIMP-1 TIMP-2 TIMP-3 TIMP-4
n-glycosylation sites 2 0 1 0
Protein kDa 28 21 24/27 22
Protein localization soluble soluble/cell
surface
ECM soluble/cell
surface
Protein association proMMP-9 proMMP-2 proMMP-2/-9 proMMP-2
MMPs poorly inhibited MT1-, MT2-, MT3-
and MT5-MMP,
MMP-19
none none none
29
2.3.3 Regulation of gelatinase activity
MMPs are regulated in many levels although it is not fully understood how MMPs act in the processes of development, homeostasis and diseases. They are tightly regulated transcriptionally and on the posttranslational level. MMPs are secreted as inactive proMMPs. Their activity is controlled at the protein level by their activators, inhibitors and through their cell surface localization.
Most MMPs are closely regulated, mainly at the level of transcription. MMP-2 is an exception. It is expressed and controlled also through a mechanism of enzyme activation and post-transcriptional mRNA stabilization. (Strongin et al. 1995) The gene expression of MMPs is regulated by several stimulatory and suppressive factors that influence multiple signal pathways. For example, the expression of different MMPs can be regulated by phorbol esters, integrin-derived signals, extracellular matrix proteins, cell stress or changes in cell shape (Fini et al. 1998; Sternlicht & Werb 1999). AP-1 complexes are known to play a critical role in the regulation of some MMP genes. An AP-1 binding sequence has been identified in the gene for MMP-9, but not in that for MMP-2 (Sternlict & Werb 2001). Also interferon-α and -γ have been shown to alter the expression of MMP-2 and MMP-9 in cultured melanoma cell lines (Hujanen & Turpeenniemi-Hujanen 1991; Hujanen et al. 1994).
One of the regulation mechanisms for MMPs is the activation on cell surface. There is evidence that cell surface association may be critical for optimal MMP function. MT-MMPs are localized to invalopodias - specialized plasma membrane protrusions believed to constitute the cellular structures that direct invasion – and they lose their proteolytic activity when they appear in secreted forms (Werb et al. 1997; Nakahara et al. 1997; Chen W-T 1996; Hotary et al. 2000).
Most of the MMPs are activated outside the cell, except MMP-11, MMP-28 and membrane bound MMPs containing furin protease cleavage sites. They are activated by intracellular urine-like serine proteases before they reach the cell surface. (Sternlicht & Werb 2001) The activity of MMPs is controlled by several endogenous and exogenous inhibitors. TIMPs are included in the group of endogenous inhibitors but they are not the only ones. α2-macroglobulin is a major endogenous inhibitor of MMPs. (Sottrup-Jensen & Birkedal-Hansen 1989) It is an abundant plasma protein and inhibits MMPs in tissue fluids, whereas TIMPs inhibit MMPs locally in tissues. The inhibition of α2-macroglubulin by MMPs is irreversible. (Sternlich & Werb 2001) Other proteins, like tissue factor pathway inhibitor 2 (TFPI-2) and GPI-anchored glycoprotein called RECK have also been

30
reported to inhibit MMPs. How these proteins inhibit MMPs is not yet known. Protein subdomains are other recently recovered MMP inhibitors. Their structure has similarities with that of TIMPs. (Sternlicht & Werb 2001; Visse & Nagase 2003; Clark et al. 2007)
2.3.4 The prognostic role of gelatinases and their inhibitors in cancer patients
Over the last few years the research of matrix metalloproteinases has increased considerably. It has been shown that many members of the MMP family take part in cancer invasion and metastasis. The overproduction of MMPs in cancer is known to correlate with tumor progression and metastasis and therefore many cancer trials have focused on studying the roles of MMPs and their inhibitors as prognostic markers in different cancer types. The levels of immunoreactive proteins have been studied by different methods in tissue samples from cancer patients’ serum or plasma and also from the urine of cancer patients, especially those with urothelial cancer.
Most data published from MMP-2 and MMP-9 seems to link their roles to aggressive behavior of different cancer types. MMP-2 overexpression is found to correlate with poor survival in breast carcinoma patients (Talvensaaari-Mattila et al. 1998, 1999, 2001, 2003; Sivula et al. 2005). The overexpression of MMP-2 immunoreactive protein indicates a 4.5-fold relative risk of dying from melanoma, and in uveal melanoma it predicts the risk of metastasis (Väisänen et al. 1998, 1999). In gastric cancer, colorectal cancer and also in pancreatic cancer MMP-2 expression seems to correlate with poor prognosis (Grigioni et al. 1994; Ring et al. 1997; Juuti et al. 2006). Increased expression of MMP-2 in prostate or renal carcinoma seems to be associated with poor prognosis (Inoue et al. 2002; Trudel et al. 2003). The role of MMP-2 circulating immunoreactive protein is not so widely studied and not that clear, either. There are studies that state that high serum levels of MMP-2 associate with adverse prognosis in breast cancer, at least in node-positive breast carcinoma (Leppä et al. 2004). Kuvaja et al. in their experiment came to the conclusion that low level of serum proMMP-2 correlates with aggressive behavior (Kuvaja et al. 2006). When viewing hematological malignancies MMP-2 expression seems to indicate a favorable prognosis, and in the same work of Kuittinen et al. MMP-9 expression was instead a marker of poor prognosis (Kuittinen et al. 2002).

31
The function of MMP-9 is quite controversial in other solid tumors than bladder cancer. Scorilas et al. suggest in the conclusion of their study that MMP-9 immunoreactive protein could be a favorable indicator in node-negative breast cancer. On the other hand, Rahko et al. showed that patients with receptor-negative and MMP-9 positive breast carcinoma had a decreased disease-free survival compared to patients having tumors that were negative for both parameters (Rahko et al. 2004). In studies using plasma or serum samples it appeared that MMP-9 could be associated with an increased relapse risk and unfavorable prognosis (Ranuncolo et al. 2003; Talvensaari-Mattila et al. 2005).
The controversial role of TIMPs as inhibitors but also as activators of some MMPs has led to complex results when studying their effects on the prognosis of different cancers. In lung cancer the TIMP-1 overexpression in tissue and elevated serum levels are predictors of worse survival (Ylisirniö et al. 2000; Gouyer et al. 2005). In head and neck squamous cell carcinoma TIMP-1 also associated with poorer survival when measured from either tissue or serum (Ruokolainen et al. 2005). TIMP- 2 seems to be a marker of favorable prognosis, but some authors have found it to be linked to poor prognosis (Remarcle et al. 2000; Nakiopoulou el al. 2002). Rauvala et al. showed in their experiments that preoperative serum TIMP-1 concentration correlated to aggressive behavior of ovarian cancer, and high TIMP-2 levels were controversially associated with better survival, but this was not statistically significant (Rauvala et al. 2005). The relationship between MMP-2 overproduction and tumor progression has led to the development of strategies and clinical trials to study TIMPs’ potential role as a therapeutic agent. Preclinical studies have shown that TIMPs may reduce invasion and spontaneous metastases (Curran et al. 2001; Slaton et al. 2001; Pepper et al. 2001). In contrast, Kruger et al. reported that during batimastat treatment, liver metastases appeared in the treated animals (Kruger et al. 2001). Clinical trials using metalloproteinase inhibitors in the treatment of different cancers have failed to meet the clinical end points (Coussens et al. 2002; Overall & Lopez-Otin 2002; Pavlaki & Zucker 2003).
2.3.5 Tissue inhibitors of metalloproteinases in bladder cancer
In bladder cancer and moreover in urothelial cancer, there are several studies that have tried to establish the function of metalloproteinase invasion and the growth of these tumors. Many of these studies have concentrated on exploring the levels of these markers in the urine. The protein levels of MMP-2, MMP-9 and TIMP-2

32
in urine have recently been suggested as possible non-invasive diagnostic markers for bladder cancer by Eissa et al. 2007. They showed that high sensitivity and specificity of MMP zymography, MMP-9/TIMP-2 ratio and MMP-2/TIMP-2 ratio were reached, more favorably so compared to cytology. (Eissa et al. 2007)
MMP-9 is quite well examined in urothelial and bladder cancer. Whether using tissue samples or serum or urine detection, it seems that high or elevated expression of MMP-9 enzyme correlates to clinical stage or histological grade of the tumor (Gerhards et al. 2000; Monier et al. 2002; Eissa et al. 2003, Guan et al. 2003). In one study of Durkan et al. no correlation to grade was found but instead, the MMP-9 levels measured by enzyme-linked immunoassay (ELISA) correlated to stage when measuring MMP-9 protein in urine samples of bladder cancer patients (Durkan et al. 2003). It has also been found that patients with no relapse had a higher urine MMP-9 protein level than patients with relapses, the difference being statistically significant (Monier et al. 2003). The value of MMP-9s in predicting survival is also controversial. While some studies show no association between survival and MMP-9 expression there are others that show MMP-9 expression as a statistically significant predictor for poor cause-specific survival (Gerhards et al. 2003; Miyata et al. 2004).
Some clinical studies have been able to confirm especially the role of MMP-2 in progression of urothelial carcinoma. Already in 1993 Davies et al. used zymography to measure the levels of type IV collagenase activity in TCC. Levels of active MMP-2 increased with tumor grade and were higher in invasive tumors than in superficial tumors. (Davies et al. 1993) The serum levels of MMP-2 were shown to be elevated in advanced urothelial carcinoma preoperatively before radical cystectomy by Cohji et al. 1996. Patients with elevated serum levels of MMP-2 also had shorter disease-free survival compared to patients with normal MMP-2 levels. (Gohji et al. 1996) Some other studies have also shown a correlation to grade and stage (Kanayama et al. 1998; Kanda et al. 2000; Miyata et al. 2004). Grignon et al., however, did not find any association between the expression of MMP-2 immunoreactive protein in bladder cancer tissue or the grade or stage in TCC (Grignon et. al. 1996). High MMP-2 expression seems to correlate with shorter cause-specific survival (Kanda et al. 2000; Miyata et al. 2004). There are also controversial data from urine and bladder washes concerning the excretion of MMP-2. There are studies that show an association of proMMP-2 to high stage and grade, but in other studies neither latent nor active MMP-2 could be detected in any urine samples of bladder cancer patients (Bianco et al. 1998; Gerhards et al. 2001). Previously Staack et al. showed that the

33
concentration of the circulating MMP-2, detected from the plasma of TCC patients, was higher than in the control group (Staack et al. 2006).
In general, TIMPs inhibit MMPs. TIMPs-2 binds to the active form of MMP-2 and inhibits its proteolytic activity. In fact low doses of TIMP-2 are associated with MTI-MMP-mediated MMP-2 activation. Instead, high TIMP-2 doses inhibit directly both MMP-2 and MT1-MMP-mediated MMP-2 activation. TIMP-2 also binds selectively to proMMP-2, modulating its activation. This complex shows proteolytic activity. (Steteler-Stevenson et al. 1989; Kinoshita et al. 1998; Kurschat et al. 1999)
TIMPs’ role in the prognosis of bladder carcinoma seems to be controversial. Two tissue experiments, of which one was done by reverse transcriptase-polymerase chain reaction (rPCR) and the other by immunohistochemistry, both showed that high expression of TIMP-2 correlated with advancer stage and grade (Kanayama et al. 1998; Gakiopoulou et al. 2003). In the work of Gakiopoulou et al. only positive stromal cell expression, but not that in the cancer cells, associated with stage and grade (Gakiopoulou et al. 2003). Patients with high expression of the gene for TIMP-2 in the primary tumor had an unfavorable prognosis when compared to patients with low TIMP-2 expression in the tumor (Kanayama et al. 1998). In the immunohistochemical study of Miyata et al. there were no statistical correlations between TIMP-2 and stage or tumor grade. TIMP-2 was still a statistically significant predictor of cause-specific survival. (Miyata et al. 2004) Also in another study, moderate or strong stromal TIMP-2 staining correlated strongly with shorter disease-specific survival (Grignon et al. 1996). One study on the release of TIMP-2 in urine showed an opposite correlation between TIMP-2 and high stage or histological grade. The level of TIMP-2 in urine was not informative when concerning disease-free survival in this work. (Monier et al. 2002) In the recently published experiment of Staack et al. plasma concentrations of TIMP-2 showed no correlation with grade. The levels in the group of non-metastasized bladder cancer patients were significantly lower when compared to levels in the control group, but showed no correlation with the plasma TIMP-2 levels of metastasized bladder cancer patients. (Staack et al. 2006)
Fewer data support a meaningful role of TIMP-1 in bladder cancer development. Durkan et al. found that urinary TIMP-1 levels correlated strongly with tumor size and that progression-free survival was shown in patients who had high TIMP-1 levels. The high levels did not, however, correlate with disease-specific survival. (Durkan et al. 2001) Only one study showed that TIMP-1 could
34
be an independent predictor of cause-specific survival. The writers suggest that TIMP-1 expression could be used to select patients for postoperative observation strategies (Miyata et al. 2004).
In different studies there have been calculations of the balance between MMPs and their inhibitors. Previously it has been shown that the calculated ratio of serum MMP-2/TIMP-2 could be an independent indicator for advanced urothelial carcinoma and that an imbalance between the serum levels of MMP-2 and TIMP-2 could be a predictor of recurrence in advanced urothelial cancer patients (Gohji et al. 1998). Monier et al. also came to same conclusion in their study of urine levels of matrix metalloproteinase -2 and -9 and their inhibitors in bladder cancer patients when they showed that the imbalance between increased MMP-9/TIMP-1 ratio and MMP-2/TIMP-2 ratio appears to be associated with tumor stage, grade and clinical events (Monier et al. 2002).

35
3 Aims of the present study
Superficial bladder carcinoma has a good prognosis. The recurrence rate is still over 80%, and about 10 to 15% will progress to muscle-invasive and metastatic tumors. Useful markers for predicting tumor aggressivity are few. Gelatinases MMP-2 and MMP-9 are known to associate with tumor cell invasion and metastatic potential in several malignant tumors. There are only a few and controversial articles concerning gelatinases in bladder cancer. Especially their association with clinical outcome is poorly studied. The need to find more useful biochemical markers is obvious for bladder carcinoma, and gelatinases are potential candidates because they have capacity to promote early cancer development and cancer progression.
The specific aims of the present study were:
1. To study the tumor expression of immunoreactive protein of MMP-2 and its prognostic value in bladder cancer.
2. To investigate whether there are differences in the levels of circulating immunoreactive proteins of TIMP-2 and the MMP-2:TIMP-2 complex between healthy controls and patients with bladder cancer and to study the prognostic role of these markers
3. To investigate the association between tumor MMP-9 and the clinicopathological features of bladder cancer and MMP-9 as a prognostic marker in bladder carcinoma
4. To determine and compare the values of circulating immunoreactive proteins of MMP-2, MMP-9, TIMP-1 and TIMP-2 as prognostic factors in bladder cancer patients.

36
37
4 Materials and methods
4.1 Patients and tissue and serum samples
All histological material of bladder cancer and patients’ blood samples were obtained during therapeutic procedures required by the primary disease. For control group serum samples of the healthy voluntary were collected. 54 consecutive patients for bladder cancer between 1986 and 1991 (I) and 87 patients between the years 1987 and 1992 (III) who had been treated with endoscopic treatment or cystectomy at the Surgical Department of Oulu University Hospital were entered in the study. All samples were primary samples. Serum samples from 44 voluntary bladder cancer patients who were referred to the Department of Clinical Oncology and Radiotherapy between 1996 and 1999 (II) were included in the study and the material was enlarged to 84 by including the patients until year 2005 (IV). All cases with adequate histological material were included in the study (I, III). The staging of the bladder cancer is done in this study according to the International Union Against Cancer (UICC) classification system 1997. In this staging Ta carcinomas were classified as T1 tumors and T2 and T4 is not divided into a and b categories.
4.2 Immunohistochemistry
4.2.1 Immunohistochemical staining
The histological material was fixed in 10% formalin and embedded in paraffin. For immunohistochemistry, 4μm paraffin sections were cut on poly-L-lysine (I) or silane-coated (III) slides (Sigma Chemicals, St Louis, MO, USA) and incubated overnight at 37°C. The slides were deparaffinized in a histological clearing agent (Histo-Clear, National Diagnostics, Atlanta, GA, USA) and hydrated. Endogenous peroxidase activity was blocked by incubating the slides in diluted hydrogen peroxidase. Non-specific binding was blocked by using 10% goat serum. Other specific pretreatments are listed in the original articles (I, III).
The primary antibodies were diluted and added onto the slides. The antibodies used in immunohistochemical staining are listed in Table 5. The slides were incubated at room temperature in a humidified atmosphere. The immuno-histochemical staining was continued using the Histostain bulk kit® (Zymed, San

38
Francisco, CA, USA) (I, III) according to the manufacturer’s protocol. The slides were washed thoroughly with phosphate-buffered saline after each step in the procedure. The antibody reaction was visualized in staining using a fresh substrate solution containing aminoethyl carbazole substrate (AEC, Zymed, San Francisco, CA, USA) (I, III). The sections were counterstained with hematoxylin and mounted with Immu-Mount (Shandon Inc: Pittsburgh, PA, USA). Both negative and positive controls were used.
Table 6. Antigens and their respective antibodies used in immunohistochemistry.
Antigen Antibody Staining pattern Form Source
MMP-2 mouse monoclonal, antihuman
(clone CA4001)
cytoplasmic proMMP-2
free and complexed with
TIMP-2
Diabor, Oulu, Finland
MMP-9 mouse monoclonal, anti-human
(clone GE231)
cytoplasmic pro and active
MMP-9 free and
complexed with TIMP-1
Diabor, Oulu, Finland
4.2.2 Evaluation of the immunostaining
The immunostaining for MMP-2 and MMP-9 was scored by three independent observers in two repeatable experiments, variability giving a good correlation. The clinical data were not analyzed until the immunostaining scores were given. When more than 1% of the cells showed a positive reaction for MMP-2 immunostaining the case was determined as positive (I). When 25% or more of the tumor cells showed positive staining it was considered to represent an overexpression for MMP-9 staining: less than 5% was negative, more than 5% to 25% indicated low levels (+), more than 25% but less than 50% intermediate (++) and more than 50 high (+++) levels of staining (III).
4.3 Enzyme-linked immunoassay
ELISA assays for MMP-9, TIMP-1, TIMP-2 and MMP-2:TIMP-2 complex from serum samples were performed on 96-well microtiter plates using 8-well stripes (Corning Inc., Corning, NY, USA). The total and active MMP-2 levels were detected by using commercial assay kits (Human Biotrak Elisa system for detecting MMP-2 by Amersham Biosciences, Buckinghamshire, England). The total proMMP-2 assay (RPN 2617) recognized

39
both free proMMP-2 and proMMP-2:TIMP-2 complexes, whereas the assessment used in measuring the active MMP-2 (RPN 2631) recognized only free active forms of MMP-2. The assays were conducted following the manufacturer’s instructions.
For measurements of MMP-9, TIMP-1, and TIMP-2, the plates were coated with monoclonal antibody (GE-213 for proMMP-9, DB-102 for TIMP-1 and T2-101 for TIMP-2). Serum samples were diluted immediately prior to adding to the assay and there were followed by the polyclonal antibodies (DB-209 for proMMP-9and anti-TIMP-1 or DB-205 for TIMP-2). After polyclonal detection antibodies, the horseradish peroxidase-labeled antibody (HRP, Chemicon International, Temecula, CA, USA) was added. The peroxidase label was visualized by using the OPD (o-phenylenediamine dihydrochloride) enzyme substrate (Sigma, Steinheim, Germany). The color formation was measured on 492 nm wavelength (Anthos 2001 microplate reader). Windows-based control and evaluation software for Anthos microplate readers (Anthos Labtec Instruments, Wals, Austria) was used for the calculations.
For the assessment of the MMP-2:TIMP-2 complex the plate was coated with monoclonal anti-TIMP-2 antibody (code T2-101). The bound complex was detected by using a polyclonal anti-MMP-2 antibody (code DB-202). All monoclonal and polyclonal antibodies used were from SBA Sciences (Oulu, Finland) (Table 6).
Table 7. Coating antibodies and secondary antibodies used in ELISA according to the measured immunoreactive proteins.
Measured protein Coating antibody (monoclonal) Secondary antibody immunoreactive
(polyclonal)
MMP-9 anti-MMP-9 (GE213) (SBA Sciences,
Oulu, Finland)
anti-MMP-9 (DB-209) (SBA Sciences,
Oulu, Finland)
TIMP-1 anti-TIMP-1 (DB-102) (SBA Sciences,
Oulu, Finland)
anti-TIMP-1 (SBA Sciences, Oulu,
Finland)
TIMP-2 anti-TIMP-2 (T2-101) (SBA Sciences,
Oulu, Finland)
anti-TIMP-2 (DB-205) (SBA Sciences,
Oulu, Finland)
MMP-2:TIMP-2 complex anti-TIMP-2 (T2-101) (SBA Sciences,
Oulu, Finland)
anti-MMP-2 (DB-202) (SBA Sciences,
Oulu, Finland)
proMMP-2 anti-MMP-2 (Amersham,
Buckinghamshire, UK)
peroxidase labeled Fab 1 antibody to
MMP-2
active MMP-2*
*active MMP-2 levels were measured by a commercial KIT (Amersham, Buckinghamshire, UK)

40
4.4 Statistical analysis
The survival time was defined as time in months elapsing from the date of diagnosis to the date of death. Relapse-free survival was likewise determined as time in months from the date of diagnosis to the date of recurrence or metastasis, verification made either histologically or radiologically.
The overall, cancer-specific and relapse-free survival rates were analyzed using the Kaplan-Meier method. Log-rank or Breslow test for dichotomous variable analysis was used to analyze the significance of the differences between subgroups. Receiving operating characteristics (ROC) curve was used to assess the cut-off points for continuous variables for the Kaplan-Meier analyses. Fisher’s exact probability test and Chi-Square test were used when testing the association between MMPs and TIMPs and major prognostic variables in bladder cancer, such as grade and stage.
The multivariate analysis was done with Cox’s proportional regression model (Cox 1972). Statistical analysis was performed using SPSS software system for Windows (SPSS, Chicago, IL). P-values less than 0.05 were considered as statistically significant.
4.5 Ethical aspects
The study protocol was approved by the Ethical Committee of Oulu University Hospital in March 1994, and renewed in July 2002 (EETTMK: 17/2002). Permission to use histological samples retrospectively was given by the National Authority for Medical Affairs, Finland (5180/3200/02). All patients signed a written consent before any blood or urine samples were taken. It included also the permission to use tissue samples and data from medical records.

41
5 Results
5.1 Tumor tissue expression of MMP-2 and MMP-9 immunoreactive protein in bladder carcinoma (I, III)
Positive immunoreaction was usually observed as a diffuse positive staining localized in the cell cytoplasm (Fig. 3A). Of 54 primary bladder carcinomas, 35 (65%) showed positive staining of MMP-2 immunoreactive protein. Most striking positivity typically appeared in the epithelial cells. In 22 out of 54 bladder carcinomas (41%) the staining was moderate or strong (more than 25% of the tumor cells positive). Granular staining was seen in 10 out of 54 cases (18%) (Fig. 3B). 19 cases remained negative for MMP-2 (Fig. 3C).
Fig. 3. The staining results for A) positive, B) granular positive and C) negative MMP-2 staining.
Overexpression of MMP-9 immunoreactive protein was detected in 38% (33 out of 87) of the urinary bladder cancer samples (≥ 25% of the cells appearing as positive). The remaining 44 samples were negative for MMP-9 or showed a weak immunoreactivity (< 25% of the cells appearing as positive).
5.2 Comparison of the levels of circulating MMP-2, TIMP-2 and MMP-2:TIMP-2 complex in patients and controls (II, IV)
The healthy volunteers had a mean serum level of TIMP-2 that was higher compared to bladder cancer patients. The mean serum level of TIMP-2 was 318 ng/ml in controls, while it was 258 ng/ml in bladder cancer patients. This

42
difference was statistically highly significant. (P < 0.0001) (Fig. 4A) The MMP-2:TIMP-2 complex levels were also significantly higher in the healthy volunteers compared to bladder cancer patients. The mean concentration of serum MMP-2:TIMP-2 complex was 628 ng/ml in the healthy volunteers and 316 ng/ml in the bladder cancer patients (P < 0.0001) (Fig. 4B).
Circulating levels of total MMP-2 or proMMP-2 (inactive) were also significantly higher in the control subjects (IV). The median total MMP-2 serum level of the patients was 1193 ng/ml versus 1396 ng/ml in controls (P = 0.009) (Fig. 4C), and median active MMP-2 levels 19.0 ng/ml versus 39.53 ng/ml, respectively (P < 0.001) (Fig. 4D).

43
Fig. 4. Comparison of the levels of circulating immunoreactive protein in patients and controls A) for TIMP-2, B) for MMP-2:TIMP-2 complex, C) for proMMP-2 and D) for active MMP-2, Copyright from Elsevier.
5.3 Correlation of the MMP-2, MMP-9, TIMP-2 and MMP-2:TIMP-2 complex immunoreactive proteins with the traditional clinico-pathological markers
5.3.1 Tissue immunoreactive proteins for MMP-2 and MMP-9 (I, III)
There was a statistical correlation between MMP-2 positivity and the stage of the tumor (P = 0.04), but there was no correlation between MMP-2 positivity and
44
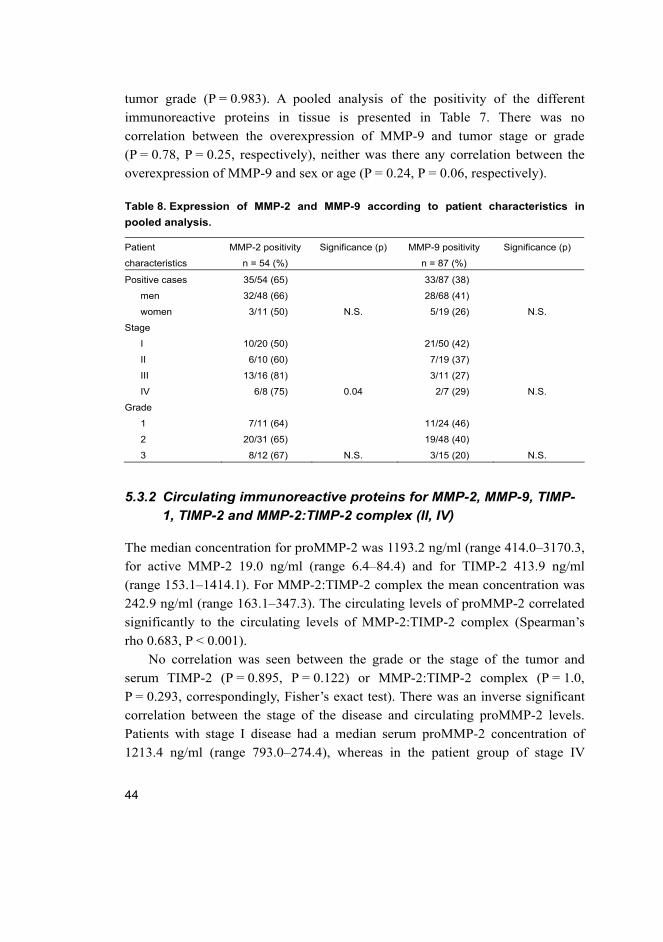
tumor grade (P = 0.983). A pooled analysis of the positivity of the different immunoreactive proteins in tissue is presented in Table 7. There was no correlation between the overexpression of MMP-9 and tumor stage or grade (P = 0.78, P = 0.25, respectively), neither was there any correlation between the overexpression of MMP-9 and sex or age (P = 0.24, P = 0.06, respectively).
Table 8. Expression of MMP-2 and MMP-9 according to patient characteristics in pooled analysis.
Patient
characteristics
MMP-2 positivity
n = 54 (%)
Significance (p) MMP-9 positivity
n = 87 (%)
Significance (p)
Positive cases 35/54 (65) 33/87 (38)
men 32/48 (66) 28/68 (41)
women 3/11 (50) N.S. 5/19 (26) N.S.
Stage
I 10/20 (50) 21/50 (42)
II 6/10 (60) 7/19 (37)
III 13/16 (81) 3/11 (27)
IV 6/8 (75) 0.04 2/7 (29) N.S.
Grade
1 7/11 (64) 11/24 (46)
2 20/31 (65) 19/48 (40)
3 8/12 (67) N.S. 3/15 (20) N.S.
5.3.2 Circulating immunoreactive proteins for MMP-2, MMP-9, TIMP-1, TIMP-2 and MMP-2:TIMP-2 complex (II, IV)
The median concentration for proMMP-2 was 1193.2 ng/ml (range 414.0–3170.3, for active MMP-2 19.0 ng/ml (range 6.4–84.4) and for TIMP-2 413.9 ng/ml (range 153.1–1414.1). For MMP-2:TIMP-2 complex the mean concentration was 242.9 ng/ml (range 163.1–347.3). The circulating levels of proMMP-2 correlated significantly to the circulating levels of MMP-2:TIMP-2 complex (Spearman’s rho 0.683, P < 0.001).
No correlation was seen between the grade or the stage of the tumor and serum TIMP-2 (P = 0.895, P = 0.122) or MMP-2:TIMP-2 complex (P = 1.0, P = 0.293, correspondingly, Fisher’s exact test). There was an inverse significant correlation between the stage of the disease and circulating proMMP-2 levels. Patients with stage I disease had a median serum proMMP-2 concentration of 1213.4 ng/ml (range 793.0–274.4), whereas in the patient group of stage IV

45
disease the median serum proMMP-2 concentration was 1055.2 ng/ml (range 564.5–1901.5) (P = 0.01). We did not find any correlation between serum proMMP-2 and histological grade, patients’ age or sex. For active MMP-2, no significant correlations with clinico-pathological parameters were found, neither were there any correlations with clinico-pathological parameters for MMP-2:TIMP-2 complex, TIMP-2, proMMP-9 or TIMP-1.
5.4 The prognostic value of tumor tissue gelatinases and their tissue inhibitors in bladder cancer
5.4.1 Tissue MMP-2 and MMP-9 as prognostic markers (I, III)
The overexpression of MMP-2 seemed to predict an earlier relapse although the correlation between overexpression of MMP-2 protein and relapse-free survival did not reach significance. Patients with a MMP-2 positive tumor suffered a relapse in less than 7 years of the follow-up, whereas the MMP-2 negative cases enjoyed more often a relapse-free survival of more than 10 years (P = 0.0781). The 5-year relapse-free survival was 30% for MMP-2 positive patients and 68% for MMP-2 negative patients. After a 10-year follow-up the survival rate was 24% versus 68% (P = 0.07).
The urinary bladder cancer relapsed in 67 of the 87 patients (77%). Most of the relapses were local ones (47 of 67 (70%)). Ten patients had lymph node relapses and ten had a hematogenous relapse. Twenty-three out of the 67 (34%) relapsed cases showed positive MMP-9 overexpression. In log rank univariate analysis, the stage correlated significantly with relapse-free survival, but not with grade (P = 0.003, P = 0.26, respectively). In multivariate Cox regression analysis, stage was the most strongly predictive factor, although no statistical significance was reached. The Kaplan Meier analysis showed that a cumulative 5-year disease-free survival of patients with low or negative MMP-9 expression was 19%, whereas the cumulative survival for patients with MMP-9 overexpression was 36% after 5 years of follow-up. This difference did not quite reach statistical significance (P = 0.08).
In this study material, MMP-2 overexpression was significantly associated with disease-specific survival and it was found to be an indicator of poor prognosis. The 5-year disease-specific survival in the MMP-2 positive patient group was 55% compared to 77% in the patients with MMP-2 negative bladder

46
carcinoma. After 10 years of follow-up, there was a distinct difference in disease-specific survival between the MMP-2-positive and negative cases, 30% and 77%, respectively. (P = 0.0353) (Fig. 5A)
Controversially, a statistically significant positive correlation was found between the MMP-9 overexpression and survival of the bladder cancer patients. Patients with MMP-9 overexpression had a 5-year overall survival rate of 68%, when it was only 48% in cases presenting with a low or negative expression of MMP-9 (P = 0.0064) (Fig. 5B). Patients with MMP-9 overexpression in the tumor tended to have better cancer-specific survival than those with low or negative MMP-9 expression, 83% versus 73%; this difference did not quite reach statistical significance, however. Tumor grade and stage and positive MMP-9 staining were all prognostic in univariate Cox regression analysis. The multivariate Cox regression analysis was performed to analyze the independency of the prognostic value of MMP-9. In multivariate analysis, stage was the most significant factor for disease-specific survival. In this material, MMP-9 overexpression appeared as the most significant factor for overall survival.

47
Fig. 5. Survival analysis according A) MMP-2 (n = 54) and B) MMP-9 (n = 87) immunoreactivity, Copywright from IIAR.

48
5.4.2 Circulating proMMP-2, TIMP-2 and MMP-2:TIMP-2 complex as prognostic markers in bladder cancer (II, IV)
The roles of circulating TIMP-2 or MMP-2:TIMP-2 complex as possible prognostic markers for bladder carcinoma were evaluated by correlating high values of the serum protein levels with the clinical behavior of the neoplasm. The cut-off values for the serum levels of TIMP-2 or MMP-2:TIMP-2 complex were determined by studying the distribution of P-values from log rank analyses for survival curves associated with different cut-off values. The selected values were the most appropriate ones, corresponding to the lowest P-values. These were 250 ng/ml for both markers.
The bladder cancer patients with high serum TIMP-2 levels enjoyed a better disease-free survival than did the patients with a low serum level (P = 0.048) (Fig. 6A). The 5-year disease-free survival rate was 28% versus 5.3%, and the 10-year disease-free survival 28% versus 0%, respectively. Similarly, the 5- and 10-year disease-free survival rates of the patients with a high serum level of MMP-2:TIMP-2 complex were favorable compared to that in patients presenting with low levels of MMP-2:TIMP-2-complex (28% versus 0% and 19% versus 0%). The latter difference is distinct in terms of numbers but is not statistically significant (P = 0.191), however.
A distinct difference in cause-specific survival was also found according to the serum TIMP-2 levels. The patients with a low level of circulating TIMP-2 had a poor survival compared to the patients with a high level of serum TIMP-2. In Kaplan Meier analysis the cumulative 5- and 10-year cause-specific survival rates in patients with low levels of circulating TIMP-2 were 18% and 5%, and in the patients with high TIMP-2 levels, 67% and 24%, respectively (P = 0.0052) (Fig. 6B). We were able to replicate these findings in our other research with a larger number of patients. High TIMP-2 serum levels (ln TIMP-2 > 5.50, corresponding to serum concentration of 244.7 ng/ml) also associated with better disease-specific survival. The 5- and 10-year disease-specific survival rates were 66% versus 19% and 18% versus 7%, respectively (P = 0.004)
A statistically significant difference in the cause-specific survival was also seen between the patients with low and high serum levels for MMP-2:TIMP-2-complex (P = 0.007). The 5- and 10-year cause-specific survival rates for the patients with a low level of circulating MMP-2:TIMP-2 complex were considerably lower than for those with a high serum level. The 5-year cause-specific survival was 20%, and 10-year survival only 7%, when the MMP-

49
2:TIMP-2 complex level was low. When the complex level was high, the cause-specific survival was better; the 5-year survival was 60% and 10-year survival 24% (Fig. 6C).
Fig. 6. A) Disease-free survival and B) cause-specific survival according to high (> 250ng/ml) and low (≤ 250ng/ml) levels of serum TIMP-2, C) cause-specific survival according to high (> 250ng/ml) and low (≤ 250ng/ml) serum levels of MMP-2:TIMP-2 complex (II), Copyright from Elsevier.
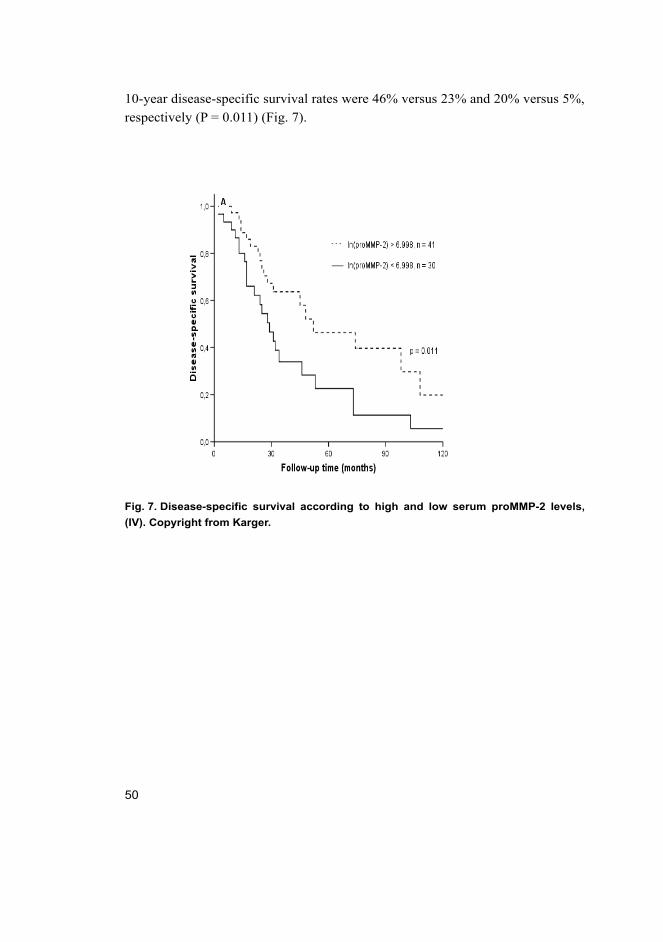
Patients with high levels of circulating proMMP-2 (ln proMMP-2 > 6.998, corresponding to serum concentration of 1094.4 ng/ml) had significantly better disease-specific survival compared to patients with lower levels of serum proMMP-2. In Kaplan-Meier analyses for disease-specific survival, the 5- and
50
10-year disease-specific survival rates were 46% versus 23% and 20% versus 5%, respectively (P = 0.011) (Fig. 7).
Fig. 7. Disease-specific survival according to high and low serum proMMP-2 levels, (IV). Copyright from Karger.

51
6 Discussion
6.1 The prognostic value of MMP-2 and MMP-9 immunoreactive protein in bladder carcinoma
In this study there were few immunohistochemical samples that could be classified either non-invasive Ta tumors or T1 tumor. Those samples were included in T1 group. Non-invasive Ta tumors have different biology and clinical behavior than invasive bladder cancer. The very few cases of Ta tumors in data had however very small effect on the results and conclusions in this study. In the published articles, same criteria for classification of patients were used.
6.1.1 MMP-2
Today, the prognosis of bladder carcinoma is still mostly being determined by stage, grade and multiplicity of the tumor in the bladder. Stage is the most powerful effector of prognosis, the others being good markers for recurrence and tumor progression. We still use these markers for selection of patient management. Many molecular markers are being studied to find more predictive markers, but it is not easy to translate these laboratory findings into a clinical instrument.
Matrix metalloproteinases are known to associate with invasion and tumor angiogenesis and metastasis of several human malignant tumors. Gelatinases, especially MMP-2 and MMP-9, have been shown to be linked to angiogenesis and tumor growth (Itoh et al. 1998; Brooks et al. 1998, Hibner et al. 1998). In general, the role of MMPs in carcinogenesis seems to be very complex, sometimes even controversial, according to some preclinical findings (Duffy & McCarthy 1998; Deryugina & Quigley 2006).
Superficial bladder carcinoma is confined to the mucosal or submucosal layers of the bladder wall. According to the WHO classification, superficial bladder carcinoma is a non-invasive neoplasia with low malignant potential, even though grade 3 tumor is already considered an aggressive disease and therefore has more potential for invasiveness and progression. There are at least two known pathways for progression and invasion for superficial bladder carcinoma 1) activation of the receptor tyrosine kinase (RTK)-Ras pathway and deletion of chromosome 9, and 2) mutation of fibroblast growth factor receptor 3 (FGFR3)

52
(Wu XR 2005; Wolff et al. 2005). These routes may explain the different invasion and metastatic potential of different bladder tumors. In vitro studies have indicated that MMP-2 and MMP-9 activity may determine the invasion capacity of the bladder carcinoma cell line T24, which contains the activated c-Harvey-Ras ongogene (Hamasaki et al. 1998; Kawakami et al. 2001). It is thus possible that these proteinases may confer the clinical behavior of bladder carcinoma. There are clinical bladder carcinoma studies which have confirmed the preclinical findings, showing that gelatinases seem to associate with progression of transitional cell carcinoma of the bladder.
In this study it was shown that MMP-2 protein overexpression in the tumor tissue correlates with the aggressiveness of the bladder cancer. It was also shown for the first time that the overexpression of MMP-2 correlates to the cause-specific survival. It seems to be a marker of shortened relapse-free time, although the difference was not quite statistically significant, probably due to the low number of the cases. The difference was, however, clinically distinct. The 5-year disease-free survival was 32% for MMP-2 positive patients and 68% for MMP-2 negative cases. In a previous publication of Kanayama et al. (1998) it was reported that MMP-2 contributes to the invasive properties of bladder carcinoma (Kanayama et al. 1998). Moreover, in some studies where gelatine zymography was used, the expression of activated MMP-2 was higher in invasive tumor tissue (Davies et. al 1993; Kanda et al. 2000). In the study of Kanda et al. (2000), proMMP-2 expression was higher in invasive tumor tissue and the high levels of active MMP-2 correlated significantly to poor outcome (Kanda et al. 2000). In the present material the positive MMP-2 staining correlated significantly to tumor stage, but not to grade. The results of other studies trying to correlate MMP-2 to grade, stage or invasiveness are very conflicting, regardless of the measuring method used (Grignon et al. 1996; Kanayama et al. 1998; Kanda et al. 2000; Papathoma et al. 2000).
6.1.2 MMP-9
Here, MMP-9 positivity did not correlate to the grade or stage of the tumor, or the sex or age of the patients with bladder cancer. In other immunohistochemical studies by different investigators, correlation with clinico-pathological parameters varies (Grignon et al. 1996; Özemir et al. 1999; Durkan et al. 2003). In the present work the patients with a tumor showing a high expression of MMP-9 immunoreactive protein had a better survival rate compared to patients with

53
negative or low expression. When looking at cancer-specific survival, the patients with high expression of MMP-9 in the primary tumor seemed to have better survival than patients with negative or low expression, but this association did not reach statistical significance (P = 0.272). It is notable, however, that the MMP-9 overexpression did correlate to the overall survival of the bladder cancer patients. One explanation for the discovery in the present study of MMP-9 may be the possible role of MMP-9 in immunological host reactions in cancer patients or in controlling tumor angiogenesis. It is possible that these factors might dominate in early tumor progression. MMP-9, similarly to other MMPs, is produced as an inactive, latent form that requires activation for being enzymatically active. Stromelysin-1 (MMP-3) is one of the most effective activators for MMP-9. (Sternlicht et al. 2001) Other MMPs, such as MMP-2, MMP-7 and MMP-13, as well as some serine proteinases are also able to activate pro-MMP-9. MMPs are known to be needed in degradation of extracellular matrix and basement membranes, but they play also a role in the formation of new capillaries, which is essential for tumor progression (Moses et al. 1997). TIMPs, the endogenous tissue inhibitors of matrix metalloproteinases, regulate the MMP activity, but they have also been found to modulate tumor angiogenesis. It seems that MMPs have a complex role in this process, and that certain MMPs also take part in the inhibition of revascularization (Cornelius et al. 1998). Certain cancer-related MMPs, such as MMP-9, may participate in the inhibition of endothelial cell proliferation and angiogenesis. This is due to the fact that MMPs, including MMP-9, generate antiangiogenic endostatin-containing peptides from collagen XVIII (Heljasvaara et al. 2005). The role of MMP-9 is thus more complicated than the role of MMP-2 and somewhat controversial. Scorilas et al. (2001) found in their work that overexpression of MMP-9 was associated with better survival in breast cancer patients, and they suggested that the balance between latent and active MMP-9 could shift towards the active form when the grade of breast carcinoma is higher (Scorilas et al. 2001). Our results are in line with this suggestion, and it seems that MMP-9 could be a marker of better prognosis in some cancer types.

54
6.2 The prognostic role of circulating MMP-2, its inhibitor TIMP-2 and their complex (MMP-2:TIMP-2) in bladder cancer
6.2.1 MMP-2, TIMP-2 and MMP-2:TIMP-2 complex in bladder cancer patients and in healthy controls
In the present study, healthy volunteers were found to have higher serum levels for proMMP-2, TIMP-2 and of MMP-2:TIMP-2 complex than the bladder cancer patients. This is in line with the fact the patients with low levels of circulating proMMP-2, TIMP-2 or MMP-2:TIMP-2 complex had poorer survival than the patients with high serum levels for proMMP-2, TIMP-2 or MMP-2:TIMP-2 complex. Healthy volunteers were also found to have higher serum levels of activeMMP-2 than bladder cancer patients.
6.2.2 MMP-2
The circulating forms of gelatinases and their inhibitors were studied in the original articles II and IV. It was found that the patients with high levels of the circulating proMMP-2 had significantly better survival compared to patients with lower levels of serum proMMP-2. The 5- and 10-year disease-specific survival rates were 46% versus 23% and 20% versus 5%, respectively (P = 0.011). In these two studies the patients included have more aggressive disease when comparing them to two the immunohistochemical studies. That makes it rather difficult to compare this material and results. Previously Gohji et al. (1996, 1998) investigated the role of elevated serum levels of MMP-2, MMP-3 and TIMP-2 in urothelial carcinoma. There were no differences in the serum levels of MMP-2 between the healthy controls and the patients with superficial bladder cancer, but patients with an advanced urothelial carcinoma had significantly higher serum levels of MMP-2 than those with superficial bladder cancer. The disease-free survival in patients with elevated serum levels of MMP-2 did not differ significantly. (Gohji et. al. 1996; Gohji et al. 1998) Instead, Staack et al. (2006) found recently that plasma levels of MMP-2 were significantly higher when compared between healthy patients and patients with non-metastasized bladder cancer and also between non-metastasized and metastasized bladder cancer patients (Staack et al. 2006). It seems that the role of MMP-2 in cancer is very conflicting. One explanation could be the role of MMP-2 as a potent inhibitor of angiogenesis. MMP-2 is able to cleave ECM components, including plasminogen,

55
which leads to angiostatin release and angiogenesis inhibition. (O’Reilly et al. 1999) Controversially, it has been shown that MMP-2 activity can be blocked by anti-MMP-2 vaccination resulting in antiangiogenic activity (Su et al. 2003).
In the present study we did not find any significant correlation with serum active MMP-2 and histological grade, tumor stage or patient’s sex or age.
Many investigators have tried to find new noninvasive diagnosis methods for bladder cancer. Cystoscopy is invasive and inconvenient for patients and quite expensive to use in diagnosis, and especially in bladder cancer follow-up. More studies have been conducted to investigate urine-based markers than serum markers. As a marker, MMP-9 has been more studied than MMP-2 in urine. Some studies have shown that high urinary MMP-9 levels associates with advanced stage of the tumor. (Bianco et al. 1998; Durkan et al. 2003; Gerhards et al. 2001). Only Gerhards et al. (2001) showed in their study a correlation between high levels of urinary MMP-2 and tumor grade and stage (Gerhards et al. 2001). In our studies we did not find any correlation between the urinary levels of active or proMMP-2 or proMMP-9 levels and the clinico-pathological parameters or survival of the patients.
6.2.3 TIMP-2
No correlation was found in this study between the serum levels of the TIMP-2 and sex, grade or staging. The present results support the concept that TIMP-2 levels predict a favorable clinical course in cancer. A strong association with survival was found with serum TIMP-2. The 5- and 10-year disease-specific survival rates were 66% versus 19% and 18% versus 7%, respectively. For instance, high TIMP-2 levels have previously been found to associate with low stage in colorectal cancer (Ring et al. 1997). In the study of Monier et al. (2002), reduced TIMP-2 and increased levels of active MMP-2 in urine were correlated to grade and stage in bladder cancer (Monier et al. 2002) In contrast to these, Gakiopoulou et al. (2003) found recently in an immunohistochemical study a significant association between stromal expression of TIMP-2 and histological grade as well as the advanced stage of urothelial carcinoma. Further, a significant correlation between stromal TIMP-2 expression and proliferation marker Ki-67 or mutant p53 protein, but not with bcl-2, was seen. (Gakiopoulou et al. 2003)
It has been shown that TIMPs regulate MMP activity. Recent findings have demonstrated that TIMPs also inhibit the mitogenic activity of human microvascular endothelial growth factors, such as VEGF-A and FGF-2. Stetler-

56
Stevenson et al. (2008) have demonstrated a cell surface signaling receptor for a member of the TIMP family. They suggest that TIMP-2 regulates cellular responses to growth factors. (Stetler-Stevenson et al. 2008) The new observations show that TIMP-s has other functions besides inhibition of MMPs and that it is independent of MMPs. TIMP-2 inhibits MMP-2, but is also required in the activation of proMMP-2 (Stetler-Stevenson 1999).
The present study shows that serum TIMP-2 is a prognostic factor in bladder carcinoma and that high levels predict a favorable prognosis.
6.2.4 MMP-2:TIMP-2
The imbalance of MMP-2 and its inhibitor TIMP-2 has previously been shown to be an indicator of recurrence in urothelial carcinoma. Patients with high levels of MMP-2/TIMP-2 ratio measured from the serum of urothelial cancer had a higher risk for recurrence than patients with low levels of this ratio (Gohji et al. 1998). In the present work, a statistically significant difference in the cause-specific survival was also seen between the patients with low and high serum levels for MMP-2:TIMP-2-complex (P = 0.0022). It should be noted that in this study we measured the MMP-2:TIMP-2 complex, but did not calculate the ratio of these two markers. The 5- and 10-year cause-specific survival rates for the patients with low levels of circulating MMP-2:TIMP-2 complex were considerably lower than for those with a high serum level (20% versus 60% and 7% versus 24%). For example Gohji et al. (1998) measured MMP-2 and TIMP-2 levels first and used the calculated values to show that a high serum MMP-/2TIMP-2-ratio could predict later recurrence in patients with urothelial cancer (Gohji et al. 1998).
In the present study, it is shown that a decrease in circulating TIMP-2 and MMP-2:TIMP-2 complex levels associates with unfavorable survival in bladder cancer patients. These results confirm the inhibitory role of TIMP-2. High total TIMP-2 serum levels associated with better 5- and 10-year disease-specific survival (66% versus 18% and 18% versus 7%, respectively; P = 0.004). The differences are also clinically distinct and suggest that this biological marker should be considered as a potential prognostic factor in bladder cancer.

57
7 Conclusions
In the present study, the overexpression of gelatinases and their tissue inhibitors was studied in bladder carcinoma. The potential prognostic value of these markers was also evaluated. Additionally, the role of the circulating levels of MMP-2, TIMP-2 and MMP-2:TIMP-2 immunoreactive proteins was studied in bladder cancer patients and healthy controls.
It is shown here that both circulating and tissue proMMP-2 immunoreactive protein and circulating TIMP-2 and MMP-2:TIMP-2 complex are powerful prognostic makers in bladder carcinoma.
The specific conclusions of this study are as follows:
1. Overexperssion of MMP-2 protein correlates significantly to disease-specific survival.
2. The circulating levels of TIMP-2 and MMP-2:TIMP-2 complex are significantly lower in bladder carcinoma patients than in healthy controls.
3. Tissue MMP-9 expression does not correlate with the tumor stage or grade of bladder carcinoma, whereas overexpression correlates significantly to better overall survival.
4. Low circulating serum proMMP-2 predicts a shorter cancer-specific survival, and low levels of TIMP-2 and MMP-2:TIMP-2 complex are prognostic indicators of shorter cancer-specific survival.

58

59
References Ahonen M, Baker A & Kähäri VM (1998) Adenovirus-mediated gene delivery of tissue
inhibitor of metalloproteinase-3 inhibits invasion and induces apoptosis in melanoma cells. Cancer Res 58: 2310-2315.
Alexander CM, Hansell EJ, Behredtsen O, Flannery ML, Kishnani NS, Hawkes, SP & Werb (1996) Expression and function of matrix metalloproteinases and their inhibitors at the maternal-embryonic boundary during mouse embryo implantation. Development 122: 1723–1736.
Amling CL (2001) Diagnosis and management of superficial bladder cancer. Curr Probl Cancer 25: 219–278.
Amour A, Slocombe PM, Webster A, Butler M, Knight CG, Smith BJ, Stephens PE, Shelley C, Hutton M, Knauper V, Docherty AJ & Murphy G (1998) TNF-alpha converting enzyme (TACE) is inhibited by TIMP-3. FEBS Lett 435: 39–44.
Baker AH, George SJ, Zaltsman AB, Murphy G & Newby AC (1999) Inhibition of invasion and induction of apoptosis cell death of cancer cell lines by overexpression of TIMP-3. Br J Cancer 79: 1347–1355.
Baker AH, Edwards DR & Murphy G (2002) Metalloproteinase inhibitor: biological actions and therapeutic opportunies. J Cell Sci 115: 3719–3727.
Bianco FJ Jr, Gervasi D, Tiguert R, Grignon D, Pontes JE, Crissman JD, Fridman R & Wood DP Jr (1998) Matrix metalloproteinase-9 expression in bladder washes from bladder cancer patients predicts pathological stage and grade. Clin Cancer Res 4: 3011–3016.
Bjerregaard BK, Raaschou-Nielsen O, Sorensen M, Frederiksen K, Christensen J, Tjonneland A, Overvad K, Chapelon FC, Nagel G, Chang-Claude J, Bergmann MM, Boeing H, Trichopoulos D, Trichopoulou A, Oikonomou E, Berrino F, Palli D, Tumino R, Vineis P, Panico S, Peeters PH, Bueno-de-Mesquita HB, Kiemeney L, Gram IT, Braaten T, Lund E, Gonzalez CA, Berglund G, Allen N, Roddam A, Bingham S & Riboli E (2006) Tobacco smoke and bladder cancer – in the European prospective investigation into cancer and nutrition. Int J Cancer 119: 2412–2416.
Björklund M & Koivunen E (2005) Gelatinase-mediated migration and invasion of cancer cells. Biochem Biophys Acta 1755: 32–69.
Bramhall SR, Rosemurgy A, Brown PD, Bowry C & Buckels JA (2001) Marimastat as first-line therapy for patients with unresectable pancreatic cancer: a randomized trial. J Clin Oncol 19: 3447–3455.
Brand K, Baker AH, Perez-Canto A, Possling A, Scharjat M, Geheeb M & Arnold W (2000) Treatment of colorectal liver metastases by adenoviral transfer of tissue inhibitor of metalloproteinases-2 into the liver tissue. Cancer Res 60: 5723–5730.
Brenner DJ & Hall EJ (2006) Bladder cancer risk following primary and adjuvant external beam radiation for prostate cancer. J Urol 175: 788–789, author reply 789.
Brew K, Dinakarpandian D & Nagase H (2006) Tssue inhibitors of metalloproteinases: evolution, structure and function. Biochem Biophys Acta 1477: 267–283.

60
Brooks PC, Silletti S, von Schalscha TL. Friedlander M & Cheresh DA (1998) Disruption of angiogenesis by PEX, a noncatalytic metalloproteinases fragment with integrin binding activity. Cell 92: 391–400.
Chen WT (1996) Proteases associated with invadopodia, and their role in degradation of extracellular matrix. 29: 59–71.
Cheng L, Weaver AL, Leibovich BC, Ramnanai DM, Neumann RM, Scherer BG, Nehra A, Zincke H & Bostwick DG (2000) Predicting the survival of bladder carcinoma patients treated with radical cystectomy. Cancer 88: 2326–2332.
Clark JC, Thomas DM, Choong PF & Dass CR (2007) RECK—a newly discovered inhibitor of metastasis with prognostic significance in multiple forms of cancer. Cancer Metastasis Rev 26: 675–683.
Corcoran ML & Stetler-Stevenson WG (1995) Tissue inhibitor of metalloproteinase-2 stimulates fibroblast proliferation via cAMP-dependent mechanism. J Biol Chem 270: 13453–13459.
Corcoran ML, Kleiner DE Jr & Stetler-Stevenson WG (1995) Regulation of matrix metalloproteinases during extracellular matrix turnover. Adv Exp Med Biol 385: 151–159; discussion 179–184.
Cornelius LA, Nehring LC, Harding E, Bolanowski M, Welgus HG, Kobayashi DK, Pierce RT & Shapiro SD (1998) Matrix metalloproteinases generate angiostatin: effects on neovascularization. J Immunol 161: 6845–6852.
Coussens LM, Fingleton B & Matrisian LM (2002) Matrix metalloproteinase inhibitors and cancer: trials and tribulations. Science 295: 2387–2392.
Curigliano G, Zhang YJ, Wang LY, Flamini G, Alcini A, Ratto C, Giustacchini M, Alcini E, Cittadini A & Santella RM (1996) Immunohistochemical quantititation of 4-aminobiphenyl-DNA adducts and p53 nuclear overexpression in T1 bladder cancer of smokers and nonsmokers. Carcinogenesis 17: 911–916.
Curran S & Murray GI (1999) Matrix metalloproteinases in tumour invasion and metastasis. J Pathol 189: 300–308.
Curran S & Murray GI (2000) Matrix metalloproteinases: molecular aspects of their roles in tumour invasion and metastasis. Eur J Cancer 36: 1621–1630.
Davies B, Waxmann J, Wasan H, Abel P, Williams G, Krausz T, Neal D, Thomas D, Handy A & Balkwill F (1993) Levels of matrix metalloproteinases in bladder cancer correlate with tumor grade and invasion. Cancer Res 53: 5365–5369.
Deryugina EI & Quigley JP (2006) Matrix metalloproteinases and tumour metastasis. Cancer Metastasis Rec 25: 9–34.
Duffy MJ & McCarthy K (1998) Matrix metalloproteinases in cancer: prognostic markers and targets for therapy. Int J Oncol 12: 1343–1348.
Durkan GC, Nutt JE, Marsh C, Rajjayabun PH, Robinson MC, Neal DE, Lunec J & Mellon K (2003) Alteration in urinary matrix metalloproteinase-9 to tissue inhibitor of metalloproteinase-1 ratio predicts recurrence in nonmuscle-invasive bladder cancer. Clin Cancer Res 9: 2576–2582.
Egeblad M & Werb Z (2002) New functions for the matrix metalloproteinases in cancer progression. Nat Rev Cancer 2: 161–174.

61
Eissa S, Labib RA, Mourad MS, Kamel K & El-Ahmady O (2003) Comparison telomerase activity and matrixmetalloproteinase-9 in voided urine and bladder wash samples as a useful tool for bladder cancer. Eur Urol 44: 687–694.
Eissa S, Ali-Labib R, Swellam M, Bassiony M, Tash F & El-Zayat TM (2007) Noninvasive diagnosis of bladder cancer by detection of matrix metalloproteinase (MMP-2 and MMP-9) and their inhibitor (TIMP-2) in urine. Eur Urol 52: 1388–1396.
Fassina G, Ferrari N, Brigati C, Benelli R, Santi L, Noonan DM & Albini A (2002) Tissue inhibitors of metalloproteinases: regulation and biological activities. Clin & Exp Metastasis 18: 111–120.
Fini ME, Cook JR, Mohan R & Brinckerhoff CE (1998) Regulation of matrix metalloproteinase gene expression. In WC Parks & RP Mecham (eds) Matrix metalloproteinases. New York Academic: 299–356.
Folguers AR, Pendas AM, Sanchez LM & Lopez-Otin C (2004) Matrix metalloproteinases in cancer. From new functions to improved inhibition strategies. Int J Dev Biol 48: 411–424.
Fosså S, Reitan J, Ous S, Odegaar A & Loeb M (1985) Prediction of tumor progression in superficial bladder carcinoma. Eur Urol 11: 1–5.
Gakiopoulou H, Nakopoulou L, Siatelis A, Mavrommatis I, Panaytopoulou EG, Tsirmpa I, Stravodimos C & Giannopoulos A (2003) Tissue inhibitor of metalloproteinase-2 as a multifunctional molecule of which the expression is associated with adverse prognosis of patients with urothelial bladder carcinomas. Clin Cancer Res 9: 5573–5581.
Gerhards S, Jung K, Koening F, Daniltchenko D, Hauptman S, Schnorr D & Loening SA (2001) Excretion of matrix metalloproteinase 2 and 9 in urine is associated with a high stage and grade of bladder carcinoma. Urology 57: 675–679.
Gohji K, Fujimoto N, Komiyama, Fujii A, Ohkawa J, Kamidono S & Motowo N (1996) Elevation of serum levels of matrix metalloproteinase-2 and -3 as new predictors of recurrence in patients with urothelial carcinoma. Cancer 78: 2379–2387.
Gohji K, Fujimoto N, Ohkawa J, Fujii A & Nakajima M (1998) Imbalance of serum matrix metalloproteinase-2 and its inhibitor as a predictor of recurrence of urothelial cancer. Br J Cancer 77: 650–655.
Goldberg GI, Strongin A, Collier IE, Genrich LT & Marmer BL (1992) Interaction of 92-kDa type IV collagenase with the tissue inhibitor of metalloproteinases prevents dimerization, complex formation with stromelysin. J Biol Chem 267: 4583–4591.
Gomez DE, Alonso DF, Yoshiji H & Thorgeirsson UP (1997) Tissue inhibitors of metalloproteinases: structure, regulation and biological functions. Eur J Cell 74: 111–122.
Grigioni WF, D'Errico A, Fiorentino M, Baccarini P, Onisto M, Caenazzo C, Stetler-Stevenson WG, Garbisa S & Mancini AM (1994) Gelatinase A (MMP-2) and its mRNA detected in both neoplastic and stromal cells of tumors with different invasive and metastatic properties. Diagn Mol Pathol 3: 163–169.

62
Grignon DJ, Sakr W, Toth M, Ravery V, Angulo J, Shamsa F, Pontes JE, Crissman J & Fridman R (1996) High levels of tissue inhibitor of metalloproteinases-2 (TIMP-2) expression are associated with poor outcome in invasive bladder cancer. Cancer Res 56: 1654–1659.
Gouyer V, Conti M, Devos P, Zerimech F, Copin MC, Creme E, Wurtzt, Porte H & Huet G (2005) Tissue inhibitor of metalloproteinase 1 is an independent predictor of prognosis in patient with nonsmall cell lung carcinoma who undergo resection with curative intent. Cancer 103: 1676–1684.
Guan KP, Ye HY, Yan Z, Wang Y & Hou SK (2003) Serum levels of endostatain and matrix metalloproteinase-9 associated with high stage and grade primary transitional cell carcinoma of the bladder. Urology 61: 719–723.
Habuchi T, Ogawa O, Kakehi Y, Ogura O, Koshiba M, Sugiyama T & Yoshida O (1992) Allelic loss of chromosome 17p in urothelial cancers: strong association with invasive phenotype. J Urol 148: 1595–1599.
Habuchi T, Marberger M, Droller M, Hemstreet III G, Grossman B, Schalken J, Schmitz-Dräder B, Murphy W, Bono A, Goebell P, Getzenberg R, Hautmann S, Messing E, Fradet Y & Lokeshwar V (2005) Prognostic marker for bladder cancer: international consensus panel bladder tumor markers. Urol 66: 64–74.
Hamasaki T, Hattori T, Kimura G & Nakazawa N (1998) Tumor progression and expression of matrix metalloproteinase-2 (MMP-2) mRNA by human urinary bladder cells. Urol Res 26: 371–376.
Heljasvaara R, Nyberg P, Luostarinen J, Parikka M, Heikkilä P, Rehn M, Sorsa T, Salo T & Pihlajaniemi T (2005) Generation of biologically active endostatin fragments from human collagen XVIII by distinct matrix metalloproteinases. Exp Cell Res 307: 292–304.
Hermanek P, Sobin LH & editors (1992) UICC TNM classification of malignant tumours. 4th ed. 2ndrev. Berlin: Springer-Verlag.
Herr HW, Schwald DM, Zhang ZF, Sogani PC, Fair WR, Whotmoer WF Jr & Oettgen HF (1995) Intravesical bacillus Calmette-Guérin therapy prevents tumor progression and death from superficial bladder cancer: ten-year follow-up of a prospective randomized trial. J Clin Oncol 13: 1404–1408.
Herr HW, Shipley W & Bajorn D (2001) Cancer of the bladder. In: DeVita VT, Hellman S & Rosenberg S (eds) Cancer: principles and practice of oncology. Philadelphia, Lippincott Williams & Wilkins, pp.1396–1418.
Hibner B, Cad A, & Flynn C (1998) BAY 12-9566, a novel, biphenyl matrix angiogenic properties, Proc. Am. Assoc. Cancer Res 39: A2063.
Hipps DS, Hembry RM, Docherty AJ, Reynolds JJ & Murphy G (1991) Purification and characterization of human 72-kDa gelatinase (type IV collagenase). Use of immunolocalisation to demonstrate the non-coordinate regulation of the 72-kDa and 95-kDa gelatinases by human fibroblasts. Biol Chem Hoppe-Seyler 372: 287–296.
Hotary K, Allen E, Punturieri A, Yana I & Stephen JW (2000) Regulation of cell invasion and morphogenesis in a three-dimensional type I collagen matrix by membrane-type matrix metalloproteinases 1, 2 and 3. J Cell Biol 149: 1309–1323.

63
Hujanen ES & Turpeenniemi-Hujanen T (1991) Recombinant interferon alpha and gamma modulate the invasive potential of human melanoma in vitro. Int J Cancer 47: 576–581.
Hujanen ES, Väisänen A, Zheng A, Trygvason K & Turpeenniemi-Hujanen T (1994) Modulation of M(r) 72,000 and M(r) 92.000 type-IV collagenase (gelatinase A and B) gene expression by interferons alpha and gamma in human melanoma. Int J Cancer 58: 582–586.
Höyhtyä M, Hujanen E, Turpeenniemi-Hujanen T, Thorgeirsson U, Liotta LA & Tryggvason K (1990) Modulation of type-IV collagenase activity and invasive behavior of metastatic human melanoma (A2058) cells in vitro by monoclonal antibodies to type-IV collagenase. Int J Cancer 46: 282–286.
Inoue K, Kamada M, Slaton JW, Fukata S, Yoshikiwa C, Tamboli P, Dinney CP & Shuin T (2002) The prognostic value of angiogenesis and metastasis related genes for progression of transitional cell carcinoma of renal pelvis and ureter. Clin Cancer Res 8: 1863–1870.
Itoh T, Tanioka M, Yoshida H, Nishimoto H & Itohara S (1998) Reduced angiogenesis and tumour progression in gelatinase A-deficient mice. Cancer Res 58: 1048–1051.
Jiang Y, Wang M, Celiker M, Liu Y, Sang Q, Goldberg I & Shi Y (2001) Stimulation of mammary tumorgenesis by systemic inhibitor of matrix metalloproteinase 4 gene delivery. Cancer Res 61: 2365–2370.
Juuti A, Lundin J, Nordling S, Louhimo J & Haglund C (2006) Epithelial MMP-2 expression correlates with worse prognosis in pancreatic cancer. Oncology 71: 61–68.
Kaasinen, Wijkström H, Malmström P-U, Hellsten S, Duchek M, Mestad O & Rintala E (2003) Alternating mitomycin C and BCG instillations versus BCG alone intreatment of carcinoma in situ of the urinary bladder: a Nordic study. Eur Urol 43: 627–645.
Kaldor JM, Day NE, Kittelmann B, Petterson F, Langmark F, Pedersen D, Prior P, Neal F, Karjalainen S & Bell J (1995) Bladder tumors following chemotherapy and radiotherapy for ovarian cancer. A case–control study. Int J Cancer 63: 1–6.
Kanayama H, Yokota K, Kurokawa Y, Murakami Y, Nishitani M & Kagawa S (1998) Prognostic values of matrix metalloproteinase-2 and tissue inhibitor of metalloproteinase-2 expression in bladder cancer. Cancer 82: 1359–1366.
Kanda K, Takahashi Y, Murakami H, Kanayama H & Kagawa S (2000) The role of the activated form of matrix metalloproteinase-2 in urothelial cancer. BJU Int 86: 553–557.
Kaufman DS, Winter K, Shipley W, Heney N, Chetner M, Souhami L, Zlotecki R, Sause W & True L (2000) The initial results in muscle-invading bladder cancer of RTOG 95-06: Phase I/II trial of transurethral surgery plus radiation therapy with concurrent cisplatin and 5-fluorouracil followed by selective bladder preservation or cystectomy depending on the initial response. Oncologist 5: 471–476.
Kawakami S, Kageyama Y, Fujii Y, Kihara K & Oshima H (2001) Inhibitory effect of N-acetylcysteine on invasion and MMP-9 production of T24 human bladder cancer cells. Anticancer Res 21: 213–219.

64
Kiemeney L, Witjes J, Heijbroek R, Verbeek A & Debruyne F (1993) Predictability of recurrent and progressive disease in individual patients with primary superficial bladder cancer. J Urol 150: 60–64.
Kinoshita T, Sato H, Okada A, Ohuchi E, Imai K, Okada Y & Seiki M (1998) TIMP-2 promotes activation of progelatinase A by membrane-type 1 matrix metalloproteinase immobilized on agarose beads. J Biol Chem 273: 16098–16103.
Kirkali Z, Chan T, Manoharan M, Algaba F, Busch C, Cheng L, Kiemeney L, Kriegmair M, Montironi R, Murphy W, Sesterheen I, Tachibana M & Weider J (2005) Bladder cancer: epidemiology, staging and grading and diagnosis. J Urol 66: 4–34.
Kleiner DE & Stetler-Stevenson WG (1999) Matrix metalloproteinases and metastasis. Cancer Chemother Pharmacol 43: S42–S51.
Kogevinas M, Manenetje A, Cordier S, Ranft U, Gonzales C, Vineis P, Chang-Glaude J, Lymge E, Wahrendorf J, Tzonou A, Jöckel K-H, Serra C, Porru S, Hours M, Greiser E & Bofetta P (2003) Occupation and bladder cancer among men in Western Europe. Cancer Causes Control 14: 907–914.
Kruger A, Soeltl R, Sopov I, Kopitz C, Arlt M, Magdolen V, Harbeck N, Gansbacher B & Schmitt M (2001) Hydroxamate-type matrix metalloproteinase inhibitor batimastat promotes liver metastasis. Cancer Rres 15: 1272–1275.
Kurschat P, Zigrino P, Nischt T, Breitkopf K, Steurer P, Klein CE, Krieg T & Mauch C 81999) Tissue inhibitor of matrix metalloproteinase-2 regulated matrix metalloproteinase-2 activation. J Biol Chem 274: 21056–21062.
Kuittinen O, Soini Y & Turpeenniemi-Hujanen T (2002) Diverse role of MMP-2 and MMP-9 in the clinicopathological behavior of Hodgkin's lymphoma. Eur J Haematol 69: 205–212.
Kuvaja P, Talvensaari-Mattila A, Pääkkö P & Turpeenniemi-Hujanen T (2006) Low serum levels of pro-matrix metalloproteinase 2 correlates with aggressive behavior in breast carcinoma. Hum Pathol 37: 1316–1323.
Lamm DL (2000) Preventing progression and improving survival with BCG maintenance. Eur Urol 37: 9–15.
Leco KJ, Khohka R, Paloff N, Hawkes S & Edwards D (1994) Tissue inhibitor of metalloproteinase-3 (TIMP) is an extracellular matrixassociated protein with a distinctive pattern of expression in mouse cells and tissues. J Biol Chem 269: 9352–9360.
Leissner J, Hohenfellner R, Thuroff JW & Wolf HK (2000) Lymphadenectomy in patients with transitional cell carcinoma of the urinary bladder: significance for staging and prognosis. Br J Urol Int 85: 817–823.
Leppä S, Saarto T, Vehmanen L, Blomqvist K & Elomaa I (2004) A high serum matrix metalloproteinase-2 levels is associated with an adverse prognosis in node- positive breast carcinoma. Clin Cancer Res 10: 1057–1063.
Libby P (1995) Molecular bases of the acute coronary syndromes. Circulation 91: 2844–2850.
65
Liotta LA, Abe S, Robey PG & Martin GR (1979) Preferential digestion of basement membrane collagen by an enzyme derived from a metastatic murine tumor. Proc Natl Acad Sci U S A 76: 2268–2272.
Liotta LA, Tryggvason K, Garbisa S, Hart I, Foltz CM & Shafie S (1980) Metastatic potential correlates with enzymatic degradation of basement membrane collagen. Nature 284: 67–68.
Logothetis CJ, Xu HJ, Ro JY, Hu SX, Sahin A, Ordonez N & Benedict WF Altered expression of retinoblastoma protein and known prognostic variables in locally advanced bladder cancer. J Natl Cancer Inst 84: 1256–1261.
von der Maase H, Hansen S, Roberts J, Dogliotti L, Moore M. Bodrogi I, Albers P, Knuth A, Lippert C, Kerbart P, Sanchez Rovira P, Wersall P, Cleall S, Roychowdhury D, Tomlin I, Visseren-Grul C & Conte P (2000) Gemcitabine and cisplatin versus methotrexate, vinblastine, doxorubicin and cisplatin in advanced or metastatic bladder cancer: results of large, randomized, multinational, multicenter, phase III study. J Clin Oncol 17: 3068–3077.
Malats N, Bustos A, Nascimento C, Fernandez F, Rivas M, Puente D, Kogevinas M & Real F (2005) P53 as a prognostic marker for bladder cancer: a meta-analysis and review. Lancet Oncol 6: 678–686.
Marcus P, Hayes R, Vinesis P, Garcia-Closas M, Caporaso N, Autrup H, Branch R, Brockmöller J, Ishizaki T, Karakaya AE, Ladero J, Mommsen S, Okkels H, Romkes, M, Roots I & Rothman N (2000) Cigarette smoking , N-acetyltransferase 2 acetylation status and bladder cancer risk: A case –series meta-analysis of a gene-environment interaction. Cancer Epidemiol Biomarker Prev 9: 461–467.
Mazzieri R, Masiero L, Zanetta L, Monea S, Onisto M, Garbisa S & Mignatti P (1997) Control of type IV collagenase activity by components of the urokinase-plasmin system: a regulatory mechanism with cellbound reactants. EMBO J 16: 2319–2331.
Miyata Y, Kanda S, Nomata K, Hayashida Y & Kanetake H (2004) Expression of metalloproteinase-2, metalloprteinase-9 and tissue inhibitor of metalloproteinase-1 in transitional cell carcinoma of upper tract: correlation with tumor stage and survival. Urology 63: 602–608.
Mohan R, Rinehart WB, Bargagna-Mohan P & Fini ME (1998) Gelatinase B/lacZ transgenic mice, a model for mapping gelatinase B expression during development and injury-related tissue remodeling. J Biol Chem 273: 25903–25914.
Monier F, Mollier S, Guillot M, Rambeaud JJ, Morel F & Zaoui P (2002) Urinary release of 72 and 92kDa gelatinases, TIMPs, N-Gal and conventional prognostic factors in urothelial carcinomas. Eur Urol 42: 356–363.
Moses MA (1997) The regulation of neovascularization of matrix metalloproteinases and their inhibitors. Stem Cells 15: 180–189.
Munaut C, Salonurmi T, Kintusaari S, Reponen P, Morita T, Foidart JM & Tryggvason K (1999) Murine matrix metalloproteinase 9 gene. 5'-upstream region contains cis-acting elements for expression in osteoclasts and migrating keratinocytes in transgenic mice. J Biol Chem 274: 5588–5596.

66
Murphy G & Knäuper V (1997) Relating matrix metalloproteinase structure to function: why the ‘hemopexin’ domain? Matrix Biol 15: 511–518.
Nagase H (1998) Cell surface activation of progelatinase A (proMMP-2) and cell migration. Cell Res 8: 179–186.
Nagase H, Visse R & Murphy G (2006) Structure and function of matrix metalloproteinases and TIMPs. Cardiovasc Res 69: 562–573.
Nagase H & Woessner JF, Jr. (1999) Matrix metalloproteinases. J Biol Chem 274: 21491–21494.
Nakahara H, Howard L, Thompson EW, Sato H, Seiki M, Yeh Y & Chen WT (1997) Transmembrane/cytoplasmic domain-mediated membrane type 1-matrix metalloproteinase docking to invadopodia is required for cell invasion. Proc Natl Acad Sci USA 94: 7959–7964.
Nakopoulou L, Giannopoulou I, Stefanaki K, Panayotopoulou E, Tsirmpa I, Alexandrou P, Mavrommatis J, Katsarou S & Davaris P (2002) Enhanced mRNA expression of tissue inhibitor of metalloproteinase-1 (TIMP-1) in breast carcinomas in correlated with adverse prognosis. J Pathol 197: 307–313.
Negri E & la Vecchia C (2001) Epidemiology and prevention of bladder cancer. Eur J Cancer Prev 10: 7–14.
O’Reilly MS, Wiederschain D, Stetler-Stevenson WG, Folkman J & Moses MA (1999) Regulation of angiostatin production by matrix metalloproteinase-2 in a model of concomitant resistance. J Biol Chem 274: 29568–29571.
Overall CM & Kleifeld O (2006a) Towards third generation matrix metalloproteinase inhibitors for cancer therapy. Br J Cancer 94: 941–946.
Overall CM & Kliefeld O (2006b) Validating matrix metalloproteinases as a drug targets and anti-targets for cancer therapy. Nat Rev Cancer 6: 227–239.
Overall CM & Lopez-Otin C (2002) Strategies for MMP inhibition in cancer. Innovations for post-trial era. Nat Rev Cancer 2: 657–672.
Özemir E, Kakehi Y, Okuno H & Yoshida O (1999) Role of matrix metalloproteinase-9 in the basement membrane destruction of superficial urothelial carcinomas. J Urol 161: 1359–1363.
Ozen HA, Akdas A, Alkibay T, Altuğ U & Remzi D (1986) Prognostic factors in superficial bladder cancer. Int Urol Nephrol 18: 417–420.
Pagano F, Garbeglio A, Milani C, Bassi P & Pegoravo V (1987) Prognosis of bladder cancer. I. Risk factors in superficial transitional cell carcinoma. Eur Urol 13: 145–149.
Papathoma AS, Petraki C, Grigorakis A, Papakonstatninou H, Karavana V, Stefanakis S, Sotsiou F & Pintzas A (2000) Prognostic significance of matrix metalloproteinases 2 and 9 in bladder cancer. Anticancer Res 20: 2009–2014.
Parkin DM, Bray F, Ferlay J & Pisani P (2005) Global cancer statistics, 2002. CA Cancer J Clin 55: 74–108.
Pavlaki M & Zucker S (2003) Matrix metalloproteinase inhibitors (MMPIs): the beginning of phase I or the termination of phase III clinical trials. Cancer Met Rev 22: 177–203.
Pepper MS (2001) Role of the matrix metalloproteinase and plasminogen activator-plasmin systems in angiogenesis. Arterioscler Thromb Vasc Biol 21: 1104–1117.

67
Rahko E, Jukkola A, Melko J, Pääkkö P, Bloigu R, Talvensaari-Mattila A & Turpeenniemi-Hujanen T (2004) Matrix metalloproteinase-9 (MMP-9) immunoreactive protein has a modest prognostic value in locally advanced breast carcinoma patients treated with adjuvant antiestrogen therapy. Anticancer Res 24: 4247–4253.
Ramos-DeSimona N, Hahn-Dantona E, Sipley J, Nagase H, French DL & Quigley JP (1999) Activation of matrix metalloproteinase-9 (MMP-9) via a converging plasmin/stromelysin-1 cascade enhances tumor cell invasion. J Biol Chem 274: 13066–13076.
Ranunclo SM, Armanasco E, Cresta C, Bal De Kier Joffe E & Puricelli L (2003) Plasma MMP-9 (92kDa-MMP) activity is useful in follow-up and in the assessment of prognosis in breast cancer patients. Int J Cancer 20: 745–751.
Rauvala M, Puistola U & Turpeenniemi-Hujanen T (2005) Gelatinase and their tissue inhibitors in ovarion tumors: TIMP-1 is a predictive as well as a prognostic factor. Gynecol Oncol 99: 656–663.
Ravanti L & Kähäri VM (2000) Matrix metalloproteinases in wound repair. Int J Mol Med 6: 391–407.
Remacle A, McCarthy K, Noel A, Maguire T McDermott E, O'Higgins N, Foidrat JM & Duffy MJ (2000) High levels of TIMP-2 correlate with adverse prognosis in breast cancer. Int J Cancer 89: 118–121.
Ring P, Johannson K, Höyhtyä M, Rubin K & Lindmark G (1997) Expression of tissue inhibitor of metalloproteinases TIMP-2 in human colorectal cancer—a predictor of tumour stage. Br J Cancer 76: 805–811.
Ruokolainen H, Pääkkö P & Turpeenniemi-Hujanen T (2005) Tissue inhibitor of matrix metalloproteinase-1 is a prognostic in head and neck squamous cell carcinoma. Comparison of the circulating and tissue immunoreactive protein. Clin Cancer Res 11: 3257–3264.
Salo T, Liotta LA & Tryggvason K (1983) Purification and characterization of a murine basement membrane collagen-degrading enzyme secreted be metastatic tumor cells. J Biol Chem 258: 3058–3063.
Salo T & Oikarinen J (1985) Regulation of type IV collagen degrading enzyme by cortisol during human skin fibroblasts growth. Biochem Biophys Res Commun 130: 588–595.
Scorilas A, Karamelis A, Arnogiannaki N, Ardavanis A, Bassilopoulos P, Trangas T & Talieri M (2001) Overexpression of matrix-metalloproteinase-9 in human breast cancer: a potential favorable indicator in node negative patients. Br J Cancer 84: 1488–1496.
Shipley WU, Kaufman DS, Zehr E, Heney NM, Lane SC, Thakral HK, Althausen AF & Zietman AL (2002) Selective bladder preservation by combined modality protocol treatment: long-term outcomes of 190 patients with invasive bladder cancer. Urology 60: 62–67.
Slaton JW, Inoue K, Perrotte P, El-Naggar AK, Swanson DA, Fidler IJ & Dinney CP (2001) Expression levels of genes that regulate metastasis and angiogenesis correlate with advanced pathological stage of renal carcinoma. Am J Pathol 158: 735–743.

68
Sobue T, Hakeda Y, Kobayashi Y, Hayakawa H, Yamashita H, Aoki T, Kumegawa M, Noguchi T & Hayakawa T (2001) Tissue inhibitor of metalloproteinases 1 and 2 directly stimulate the bone-resorbing activity if isolated mature osteoclasts. J Bone Miner Res 16: 2205–2214.
Soini Y, Turpeenniemi-Hujanen T, Kamel D, Autio-Harmainen H, Risteli J, Risteli L, Nuorva K, Pääkkö P & Vähäkangas K (1993) p53 immunohistochemistry in transitional cell carcinoma and dysplasia of the urinary bladder correlates with disease progression. Br J Cancer 68: 1029–1035.
Sottrup-Jensen L & Birkendal-Hansen H (1989) Human fibroblasts collagenase-α-macroglobulin interactions. Localization of cleavage sites in the bait regions of five mammalian α-macroglobulin. J Biol Chem 264: 393–401.
Sounni N, Janssen J, Foidart A & Noel A (2003) Mebrane type-1 matrix metalloproteinase and TIMP-2 in tumor angiogenesis. Matrix Biology 22: 55–61.
Staack A, Badendieck S, Schnorr D, Loening SA & Jung K (2006) Combined determination of plasma MMP2, MMP-9 and TIMP1 improves the non-invasive detection of transitional cell carcinoma of the bladder. BMC Urology 10(6): 19.
Stein J, Lieskovsky G, Cote R, Groshen S, Feng A-C, Boyd S, Skinner E, Bochner B, Thangathurai D, Mikhail M, Raghavan D & Skinner D (2000) Radical cystectomy in the treatment of invasive bladder cancer: Long-term results in 1,054 patients. J Clin Oncol 19: 666–675.
Sternberg C & Calabro F (2005) Adjuvant chemotherapy for bladder cancer. Expert Rev Anticancer Ther 5: 987–991.
Sternberg C, Yagoda A, Scher H, Watson R, Ahmed T, Weiselberg L, Geller N, Hollander P, Herr H, Sogani PC (1985) Preliminary results of M-VAC (methotrexate, vinblastine, doxorubicin and cisplatin) for transitional cell carcinoma of urothelium. J Urol 133: 403–407.
Sternlicht MD & Werb Z (2001) How matrix metalloproteinases regulate cell behavior. Ann Rev Cell Biol 17: 463–516.
Stetler-Stevenson WG (2001) The role of matrix metalloproteinases in tumor invasion, metastasis and angiogenesis. Surg Oncol Clin N Am 10: 383–392.
Steteler-Stevenson WG, Krutzsch HC & Liotta LA (1989) Tissue inhibitor of metalloproteinase-2 (TIMP-2). J Biol Chem 264: 17374–17378.
Stetler-Stevenson WG, Liotta LA & Kleiner DE, Jr. (1993) Extracellular matrix 6: role of matrix metalloproteinases in tumor invasion and metastasis. FASEB J 7: 1434–1441.
Stetler-Stevenson M, Manor A, Lim MS, Fukushima P Karl J, Marti G, Ptaszynski K, Wand J & Stetler-Stevenson WG (1997) Expression of matrix metalloproteinases and tissue inhibitors of metalloproteinases (TIMPs) in reactive and neoplastic lymphnodes. Blood 89: 1708–1715.
Steteler-Stevenson WG (1999) Matrix metalloproteinases in angiogenesis: A moving target for therapeutic intervention. JCO 103: 1237–1241.
Stetler-Stevenson WG (2008) The tumor microenvironment: regulation by MMP-independent effects of tissue inhibitor of metalloproteinases-2. Cancer Met Rev 27: 57–66.

69
Strongin AY, Collier I, Bannikov G, Marmer BL, Grant G & Golberg G (1995) Mechanism of cell surface activation of 72-kDa type IV collagenase. J Biol Chem 270: 5331–5338.
Su JM, Wei YQ, Tian L, Zhao X, Yang, L, He QM, Wang Y, Lu Y, Wu Y, Liu F, Liu JY, Yang JL, Lou YY, Hu B, Niu T, Wen YJ, Xiao F, Deng HX, Li J & Kan B (2003) Active immunogene therapy of cancer with vaccine on the basis of chicken homologous matrix metalloproteinase-2. Cancer Res 63: 600–607.
Talvensaari-Mattila A, Pääkkö P, Blanco-Sequeiros G & Turpeenniemi-Hujanen T (2001) Matrix metalloproteinase-2 (MMP-2) is associated with risk for a relapse in postmenopausal patients with node positive breast carcinoma treated with antiestrogen adjuvant therapy. Breast Cancer Res Trat 65: 55–61.
Talvensaari-Mattila A, Pääkkö P, Höyhtyä M, Blanco-Sequeiros G & Turpeenniemi-Hujanen T (1998) Matrix metalloproteinase-2 immunoreactive protein. A marker of aggressiveness in breast carcinoma. Cancer 83: 1153–1162.
Talvensaari-Mattila A, Pääkkö P & Turpeenniemi-Hujanen T (1999) MMP-2 positivity and age less than 40 years increases the risk for recurrence in premenopausal patients with node-positive breast carcinoma. Breast Cancer Res Treat 58: 287–293.
Talvensaari-Mattila A, Pääkkö P & Turpeenniemi-Hujanen T (2003) Matrix metalloproteinase-2 (MMP-2) is associated with survival in breast carcinoma. Br J Cancer 89: 1270–1275.
Talvensaari-Mattila A & Turpeenniemi-Hujanen (2005) preoperative serum MMP-9 immunoreactive protein is a prognostic indicator for relapse-free survival in breast carcinoma. Cancer Let 20: 237–242.
Thompson RW, Mertens RA, Liao S, Holmes DR, Mecham RP, Welgys HG & Parks WC (1995) Production and localization of 92-kD gelatinase in abdominal aortic aneurysm: an elastolytic metalloproteinase expressed by aneurysm-infiltrating macrophages. J Clin Invest 96: 318–326.
Trudel D, Fradet Y, Meyer F, Harel F,& Tệtu B (2003) Significance of MMP-2 expression in prostate cancer: an immunohistochemical study. Cancer Res 63: 8511–8515.
Tryggvason K, Höyhtyä M & Pyke C (1993) Type IV collagenase in invasive tumors. Breast Cancer Re Treat 24: 209–218.
Turpeenniemi-Hujanen T, Thorgeirsson US, Hart IR, Grant SS & Liotta LA (1985) Expression of collagenase IV (basement membrane collagenase) activity in murine tumor cell hybrids that differ in metastatic potential. J Natl Cancer Inst 75: 99–103.
Turpeenniemi-Hujanen T, Feinberg RF, Kauppila A & Puistola U (1995) Extracellular matrix interactions in early human embryos: implication for normal implantation events. Fertil Steril 64: 132–138.
Valente P, Fassina G, Melchiori A, Masiello L, Cilli M, Vacca A, Onisto M, Santi L, Stetler-Stevenson WG & Albini A (1998) TIMP-2 over-expression reduces invasion and angiogenesis and protects B16F10 melanoma cells from apoptosis. Int J Cancer 75: 246–253.

70
Vartio T & Vaheri A (1981) A gelatin-binding 70,000-dalton glycoprotein synthesized distinctly from fibronectin by normal and malignant adherent cells. J Biol Chem 256: 13085–13090.
Vartio T, Hovi t & Vaheri A (19829 Human macrophages synthesize and secrete a major 95,000-dalton gelatin binding protein distinct from fibronectin. J Biol Chem 257: 8862–8866.
Vineis P & Simonato L (1991) Proportion of lung and bladder cancers in male resulting from occupation a systematic approach. Arch Environ Health 46: 6–15.
Visse R & Nagase H (2003) Matrix metalloproteinases and tissue inhibitors of metalloproteinases: structure, function and biochemistry. Circ Res 92: 827–839.
Väisänen A, Kallioinen M, von Dickhoff K, Laatikainen L, Höyhtyä M & Turpeenniemi-Hujanen T (1999) Matrix metalloproteinase-2 (MMP2) immunoreactive protein-a new prognostic marker in uveal melanoma? J Pathol 188: 56–62.
Väisänen A, Kallioinen M, Taskinen PJ & Turpeenniemi-Hujanen T (1998) Prognostic value of MMP-2 immunoreactive protein (72kDa type IV collagenase) in primary skin melanoma. J Pathol 186: 51–58.
Wang H, Li Q, Shao L & Zhu C (2001) expression of matrix metalloproteinase-2, -9, -14 and tissue inhibitors of metalloprotinases-1, -2, -3 in the endometrium and placenta of resus monkey (macaca mulatta) during early pregnancy. Biol Reprod 65: 31–40.
Werb Z (1997) ECM and cell surface proteolysis regulating cellular ecology. Cell 91: 439–442.
Winquist E, Kirchner TS, Segal R, Chin J & Lukka H (2004) Neoadjuvant chemotherapy for transitional cell carcinoma of the bladder: a systematic review and meta-analysis. J Urol 171: 561–569.
Witty JP, Lempka T, Coffey RJ, Jr. & Matrisian LM (1995) Decreased tumor formation in 7,12-dimethylbanzanthracene-treated stromelysin-1 transgenic mice is associated with alterations in mammary epithelial cell apoptosis. Cancer Res 55: 1402–1406.
Woessner JF Jr. (1999) Matrix metalloproteinses. J Biol Chem 274: 21491–21494. Wolff EM, Liang G & Jones PA (2005) Mechanism of disease: genetic and epigenetic
alterations that drive bladder cancer. Nat Clin Prac Urol 2: 502–510. Wu XR (2005) Urothelial tumorgenesis: a tale of divergent pathways. Nat Rev Cancer 5:
713–725. Yamasita K, Suzuki M, Iwata H, Koike T, Hamaguchi M, Shinagawa A, Noguchi T &
Hayakawa T (1996) Tyrosine phosforylation is crucial for growth signaling by tissue inhibitors of metalloproteinases (TIMP-1 and TIMP-2). FEBS Lett 396: 103–107.
Ylisirniö S, Höyhtyä M & Turpeenniemi-Hujanen T (2000) Serum matrix metalloproteinase-2, -9 and tissue inhibitors of metalloproteinases -1, -2 in lung cancer – TIMP-1 as a prognostic marker. Anticancer Res 20: 1311–1316.
Zeegers MP, Goldbohm RA & van den Brandt PA (2001) Are retinol, vitamin C, vitamin E, folate and carotenoids intake associated with bladder cancer risk? Result from the Netherlands Cohort Study. Br J Cancer 85: 977–83.

71
Zeegers MP, Kellen E, Buntix F & van den Brandt PA (2004) The association between smoking, beverage consumption, diet and bladder cancer: a systematic literature review. World J Urol 21: 392–401.

72

73
Original articles
I Vasala K, Pääkkö P & Turpeenniemi-Hujanen T (2003) Matrix metalloproteinase-2 immunoreactive protein as a prognostic marker in bladder cancer. Urology 62: 952–957.
II Vasala K & Turpeenniemi-Hujanen T (2007) Serum tissue inhibitor of metalloproteinase-2 (TIMP-2) and matrix metalloproteinase-2 in complex with the inhibitor (MMP-2:TIMP-2) as prognostic markers in bladder cancer. Clin Biochem 40(9–10): 640–644.
III Vasala K, Pääkkö P & Turpeenniemi-Hujanen T (2008) Matrix metalloproteinase 9 (MMP-9) immunoreactive protein in urinary bladder cancer: A marker of favorable prognosis. Anticancer Res 28(3B): 1757–1761.
IV Vasala K, Kuvaja P & Turpeenniemi-Hujanen T (2008) Low circulating levels of proMMP-2 are associated with adverse prognosis in bladder cancer. Tumor Biol 29: 279–286.
Reprinted with permission from Elsevier (I and II), IIAR (III), and Karger (IV).
Original publications are not included in the electronic version of the dissertation.

74

A C T A U N I V E R S I T A T I S O U L U E N S I S
Distributed byOULU UNIVERSITY LIBRARY
P.O. Box 7500, FI-90014University of Oulu, Finland
Book orders:OULU UNIVERSITY PRESSP.O. Box 8200, FI-90014University of Oulu, Finland
S E R I E S D M E D I C A
968. Heikka, Helena (2008) Sosiaali- ja terveysjohtajan työn sisältö ja kompetenssit
969. Juntti, Hanna (2008) Association of respiratory syncytial virus infection withasthma and atopic allergy
970. Winqvist, Satu (2008) Alcohol misuse in relation to traumatic brain injury. TheNorthern Finland 1966 birth cohort study
971. Makkonen, Saara (2008) Teknillisestä apulaisesta laboratoriohoitajaksi. Turunlaboratoriohoitajakoulutuksen kehitys vuosina 1955–1990
972. Liljeroos, Mari (2008) Toll-like receptor 2 (TLR2) and TLR4 signaling in the innateresponse against bacterial components
973. Vierimaa, Outi (2008) Multiple Endocrine Neoplasia Type 1 (MEN1) and PituitaryAdenoma Predisposition (PAP) in Northern Finland
974. Muhonen, Virpi (2008) Bone–Biomaterial Interface. The effects of surfacemodified NiTi shape memory alloy on bone cells and tissue
975. Oikarinen, Arja (2008) Kainuulaisten miesten terveyskäyttäytyminen —kulttuurinen näkökulma
976. Kantojärvi, Liisa (2008) Personality disorders in the Northern Finland 1966 BirthCohort Study
977. Valkealahti, Maarit (2008) The effects of bisphosphonates and COX-2 inhibitorson the bone remodelling unit
978. Hiiri, Anne (2008) Community-wide Oral Health Promotion in the PitkärantaDistrict of Russian Karelia – a case study
979. Koivunen, Kirsi (2008) Alaraajojen valtimonkovettumistautia sairastavienterveyteen liittyvä elämänlaatu sekä hoitomenetelmien kustannukset
980. Palosaari, Kari (2008) Quantitative and semiquantitative imaging techniques indetecting joint inflammation in patients with rheumatoid arthritis. Phase-shiftwater-fat MRI method for fat suppression at 0.23 T, contrast-enhanced dynamicand static MRI, and quantitative 99mTc-nanocolloid scintigraphy
981. Perkiömäki, Marja Riitta (2008) Craniofacial shape and dimensions as indicators oforofacial clefting and palatal form. A study on cleft lip and palate and Turnersyndrome families
982. Tolonen, Pekka (2008) Laparoscopic adjustable gastric banding for morbidobesity. Primary, intermediate, and long-term results including quality of lifestudies

ABCDEFG
UNIVERS ITY OF OULU P.O.B . 7500 F I -90014 UNIVERS ITY OF OULU F INLAND
A C T A U N I V E R S I T A T I S O U L U E N S I S
S E R I E S E D I T O R S
SCIENTIAE RERUM NATURALIUM
HUMANIORA
TECHNICA
MEDICA
SCIENTIAE RERUM SOCIALIUM
SCRIPTA ACADEMICA
OECONOMICA
EDITOR IN CHIEF
PUBLICATIONS EDITOR
Senior Assistant Jorma Arhippainen
University Lecturer Elise Kärkkäinen
Professor Hannu Heusala
Professor Olli Vuolteenaho
Senior Researcher Eila Estola
Information officer Tiina Pistokoski
University Lecturer Seppo Eriksson
Professor Olli Vuolteenaho
Publications Editor Kirsti Nurkkala
ISBN 978-951-42-8873-9 (Paperback)ISBN 978-951-42-8874-6 (PDF)ISSN 0355-3221 (Print)ISSN 1796-2234 (Online)
U N I V E R S I TAT I S O U L U E N S I S
MEDICA
ACTAD
D 983
ACTA
Kaija Vasala
OULU 2008
D 983
Kaija Vasala
MATRIX METALLOPROTEINASEMMP-2 AND MMP-9 AND THEIR INHIBITORS TIMP-1 AND TIMP-2 IN BLADDER CARCINOMA
FACULTY OF MEDICINE,INSTITUTE OF CLINICAL MEDICINE, DEPARTMENT OF ONCOLOGY AND RADIOTHERAPY,UNIVERSITY OF OULU