severe acute malnutrition in an ... - nrcmis.mp.gov.innrcmis.mp.gov.in/circulars/40/baby of...
TRANSCRIPT

Severe Acute Malnutrition in an Extremely Low Birth Weight Child
TIWARI PRAGYA* AND MATHEWS NISHI **
* Deputy Director, Child Health Nutrition, NHM GoMP **State Nutrition Consultant, NHM GoMP
From Child Health Nutrition Section, National Health Mission, Bhopal, Madhya Pradesh .
Correspondence to: Dr Tiwari Pragya Deputy Director, Child Health Nutrition Department of Health and Family Welfare, National Health Mission, Government of Madhya Pradesh 8, Arera Hills, Bhopal- 462002 [email protected]
Background: Infants <6m are a unique group due to their exclusive breastfeeding needs, physiological and developmental differences, vulnerability to different pathologies and increased mortality risk as compared to older children. These children with Severe Acute Malnutrition (SAM) are most vulnerable to death and disability due to inadequate dietary intake resulting from various causes like reduced breastfeeding potential, inadequate artificial feeding, maternal and infant diseases. Case characteristics: A low birth weight baby girl age 1 month and 28 days with diminish prospects of breastfeeding, suffering from recurrent episodes of diarrhoea, pneumonia and severe anaemia - a typical case of SAM requiring immediate medical attention. Outcome: Successfully managed through prompt medical treatment and nutritional care Message: Malnutrition is an intergenerational vicious cycle which needs to be addressed by giving due attention to maternal and child nutrition without bias Keywords: SST, SAM, NRC,
India is home to approximately 80 lakh
children with severe acute malnutrition i.e. one third of severely wasted children worldwide. Situational analysis of nutrition and health status of children state wise, within the country, reveals that Madhya Pradesh is in the epitome of this nutritional crisis, with 12.6 lakhs severely wasted children; the highest in the country as per National Family Health Survey (NFHS-III);2005-06. Recently released data of Rapid Survey of Children (RSOC; 2013-14) has documented a reduction in SAM load to 5.4%. Since mortality rate in these children is approximately 9 times higher than a healthy child, it becomes imperative to provide them with immediate medical treatment and nutritional rehabilitation. Presently, Madhya Pradesh has the highest number of 314 Nutrition Rehabilitation Centres (NRCs) wherein children below 5 years of age with severe acute malnutrition are admitted along with their mothers/ caregivers for nutritional care and medical treatment. Infants <6m form a unique cohort on account of their exclusive breastfeeding needs, physiological and developmental differences. Also the needs of a 1 month old are dissimilar to the needs of a 12 month old infant. Internationally, there is little clarity on management of malnutrition in infants <6 m, making them more prone to death and disability. However, the State of MP caters to the needs of such children and admits in its NRCs, infants <6m having difficulties in breastfeeding (Mother Milk Insufficiency
"MMI" or too weak/feeble to suckle effectively) and failure of appropriate weight gain along with presence of bipedal pitting oedema and weight for Length <-3SD. CASE REPORT An extremely low birth weight baby boy age 1 month and 28 days was referred to the NRC in Sagar district Hospital, Madhya Pradesh; with complaints of diarrhea, pneumonia and severe anemia, co-existent with severe acute malnutrition. The child was born to a family having very poor economic status. The infant’s parents were unemployed and had low level of education (upto 8th Std). Medical history of the child revealed that the child was normally delivered in Sagar District Hospital on 18.03.2015 weighing 878 gms with no evidence of fetal distress. On delivery, breast feeding could not be initiated because the infant was too weak to suckle. It was then admitted in Sick New Born Care Unit (SNCU) in Sagar District Hospital on 20.03.15 and discharged on 25.04.15. During its 36 days stay in SNCU, the infant was given antibiotics and supportive treatment. As the infant was too weak to suckle, it was fed through expressed breast milk. However, the mother of infant was admitted in the surgical ward due to a surgical emergency of intestinal obstruction, during which infant was wet nursed. The surgical intervention led to decline in galactopoeisis in the mother. At the time of discharge from SNCU the infant weighed 1200 gms. It is pertinent to point out that the Body Mass Index (BMI) of the infant’s mother (Mrs. Neha Rajput) was only 17 which clearly depicts the intergenerational vicious cycle of malnutrition.
CASE REPORT
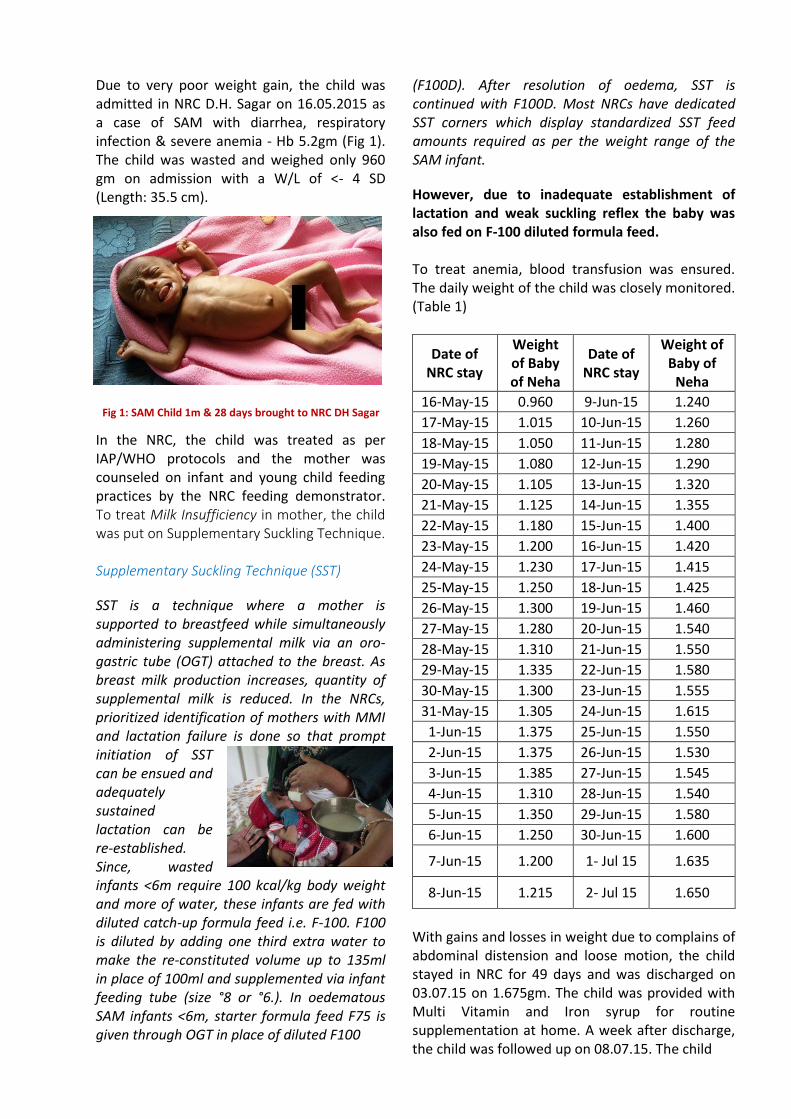
Due to very poor weight gain, the child was admitted in NRC D.H. Sagar on 16.05.2015 as a case of SAM with diarrhea, respiratory infection & severe anemia - Hb 5.2gm (Fig 1). The child was wasted and weighed only 960 gm on admission with a W/L of <- 4 SD (Length: 35.5 cm).
In the NRC, the child was treated as per IAP/WHO protocols and the mother was counseled on infant and young child feeding practices by the NRC feeding demonstrator. To treat Milk Insufficiency in mother, the child was put on Supplementary Suckling Technique. Supplementary Suckling Technique (SST)
SST is a technique where a mother is supported to breastfeed while simultaneously administering supplemental milk via an oro-gastric tube (OGT) attached to the breast. As breast milk production increases, quantity of supplemental milk is reduced. In the NRCs, prioritized identification of mothers with MMI and lactation failure is done so that prompt initiation of SST can be ensued and adequately sustained lactation can be re-established. Since, wasted infants <6m require 100 kcal/kg body weight and more of water, these infants are fed with diluted catch-up formula feed i.e. F-100. F100 is diluted by adding one third extra water to make the re-constituted volume up to 135ml in place of 100ml and supplemented via infant feeding tube (size °8 or °6.). In oedematous SAM infants <6m, starter formula feed F75 is given through OGT in place of diluted F100
(F100D). After resolution of oedema, SST is continued with F100D. Most NRCs have dedicated SST corners which display standardized SST feed amounts required as per the weight range of the SAM infant.
However, due to inadequate establishment of lactation and weak suckling reflex the baby was also fed on F-100 diluted formula feed. To treat anemia, blood transfusion was ensured. The daily weight of the child was closely monitored. (Table 1)
Date of NRC stay
Weight of Baby of Neha
Date of NRC stay
Weight of Baby of
Neha
16-May-15 0.960 9-Jun-15 1.240
17-May-15 1.015 10-Jun-15 1.260
18-May-15 1.050 11-Jun-15 1.280
19-May-15 1.080 12-Jun-15 1.290
20-May-15 1.105 13-Jun-15 1.320
21-May-15 1.125 14-Jun-15 1.355
22-May-15 1.180 15-Jun-15 1.400
23-May-15 1.200 16-Jun-15 1.420
24-May-15 1.230 17-Jun-15 1.415
25-May-15 1.250 18-Jun-15 1.425
26-May-15 1.300 19-Jun-15 1.460
27-May-15 1.280 20-Jun-15 1.540
28-May-15 1.310 21-Jun-15 1.550
29-May-15 1.335 22-Jun-15 1.580
30-May-15 1.300 23-Jun-15 1.555
31-May-15 1.305 24-Jun-15 1.615
1-Jun-15 1.375 25-Jun-15 1.550
2-Jun-15 1.375 26-Jun-15 1.530
3-Jun-15 1.385 27-Jun-15 1.545
4-Jun-15 1.310 28-Jun-15 1.540
5-Jun-15 1.350 29-Jun-15 1.580
6-Jun-15 1.250 30-Jun-15 1.600
7-Jun-15 1.200 1- Jul 15 1.635
8-Jun-15 1.215 2- Jul 15 1.650
With gains and losses in weight due to complains of abdominal distension and loose motion, the child stayed in NRC for 49 days and was discharged on 03.07.15 on 1.675gm. The child was provided with Multi Vitamin and Iron syrup for routine supplementation at home. A week after discharge, the child was followed up on 08.07.15. The child
Fig 1: SAM Child 1m & 28 days brought to NRC DH Sagar

was alert, active with weight gain of 1700gm and length 42cm. At home the child was fed on cow’s milk as the mother was unable to breastfeed. The mother was counseled on IYCF practices along with continued supplementation of Multi Vitamin and Iron syrup to the child. On his 1st follow up visit dated 15th July 2015, the child weighed 1715 gm, on 2nd follow up on 29th July 2015 his weight was 1890 gm. On the 3rd follow up on 12.08.15 the child had further gained weight and weighed 2.090gm, length 45cm and W/L <-1SD. Thus, the child had recovered from its SAM status by the 3rd Follow-up. On his 4th follow up on 26.08.15, the child weighed 2325gm (Fig 2)
Discussion
Experiences from MP show that anthropometric
data collection in <6m, have higher proportion of
missing measurements and discrepant recordings.
Erratic diagnosis of SAM in infants <6m is also a
major concern as majority of the infants <6m do
not fulfill standard anthropometric criteria for
SAM (<-3WHZ). Critical analysis of NRC data also
reveals that though the cure % in the NRCs is
~57%, the proportion of admissions discharged as
cured is significantly higher in infants <6m than in
infants aged 6 to 59m. Infants <6m can be
categorized broadly into 2 groups: clinically stable
but with reported feeding problems and clinically
unwell infants. There are varied experiences with
supplementary suckling across the centers of the
state which elicit staff time, age of infants, co-
existing maternal morbidity and experience of the
care givers as most important factors. Probability
of achieving successful re-lactation progressively
decreases with elapsing time from the date of
admission. Nevertheless, the State of MP is
promoting Infant and Young Child Feeding (IYCF)
practices in its NRCs through Supplementary
Suckling Technique (SST) as well as addressal of feeding problems by correcting breast feeding positioning and attachment. The admission profile for the year 2014-15 reflects that admission of infants <6m accounted for 4% (n=2,911) of the total admissions (n= 73,200) in NRCs. SST was introduced in 27.4% of total 2,911 admitted SAM infants aged <6m. Re-lactation from SST was successfully established in 71% (n=565) infants. 2,015 mothers of admitted SAM children <6m were subjected only to breastfeeding counselling, out of which, successful re-lactation was established in 74% mother (n=1487). Rest 99 <6m old SAM infants either defaulted or were referred to higher facility for treatment References
1. Rapid Survey of Children (RSOC) , 2013–14
2. National Family. Health Survey (NFHS-3), 2005–06
3. Management of Acute Malnutrition in Infants (MAMI) project, Summary report, October, 2009, www.ennonline.net/research
4. Management of severe malnutrition: a manual for physicians and other senior health workers. Geneva, World Health Organization, 1999
5. Supportive care to re-establish breastfeeding is described in IMCI management of the child with a serious inflection or severe malnutrition: guidelines for care at the first referral level in developing countries (p 99-104)
6. Reference Manual for Medical and Paramedical staff of NRC, Madhya Pradesh, 2011
Acknowledgement
1. Mr. Faiz Ahmed Kidwai, IAS, Mission Director, GoMP.
2. UNICEF Field Office for Madhya Pradesh for their technical support to NRCs
Fig 2: Child on his 4th
follow-up
