sexing up the sepsis six - acute medicine - sexing... · sexing up the sepsis six ... sepsis six...
TRANSCRIPT
Sexing up the Sepsis SixImproving use of the Sepsis Six care bundleShiva Sreenivasan 1 , Chris Custard 1, Rob Stacey 2, Charlie Candish 3, Maria–Belén Espina 1, Elizabeth Dawes 4, Andrew Seaton 51. Unscheduled Care Division (Acute Medicine), 2. Unscheduled Care Division (Emergency Medicine), 3. Department of Clinical Oncology, 4. Clinical Audit Department, 5. Department of Patient Safety
Gloucestershire Hospitals NHS Foundation Trust, Gloucestershire
Use of the Sepsis Six Care Bundle (S6CB) improves mortality in patients with
severe sepsis 1. In September 2010, we identified through incident investigation,
clinical audit, and a short-term mortality alert that there was a problem with
management of severe sepsis at our Trust. Our audit revealed that only 5% of
eligible patients received the full S6CB within the recommended time. We set
out to improve use of the S6CB in patients with severe sepsis.
A Trust-wide Sepsis Six programme was
implemented in February 2012, and comprised
proformas (Figure 1), safety cafés 2 (Figure 2), a
mandatory eLearning package (Figure 5), desktop
screensavers, grand rounds, posters, global emails,
and opportunistic teaching. Improvement was
measured via continuous monthly notes audit and
the statistical process control method.
Our Plan-Do-Study-Act (PDSA) testing ramp (Figure 4) guaranteed form
redesign and pathway review. We set an initial
Unscheduled Care (Emergency Medicine and
Acute Medicine) completion rate target of 75%,
and an initial Ward inpatient completion rate
target of 50%.
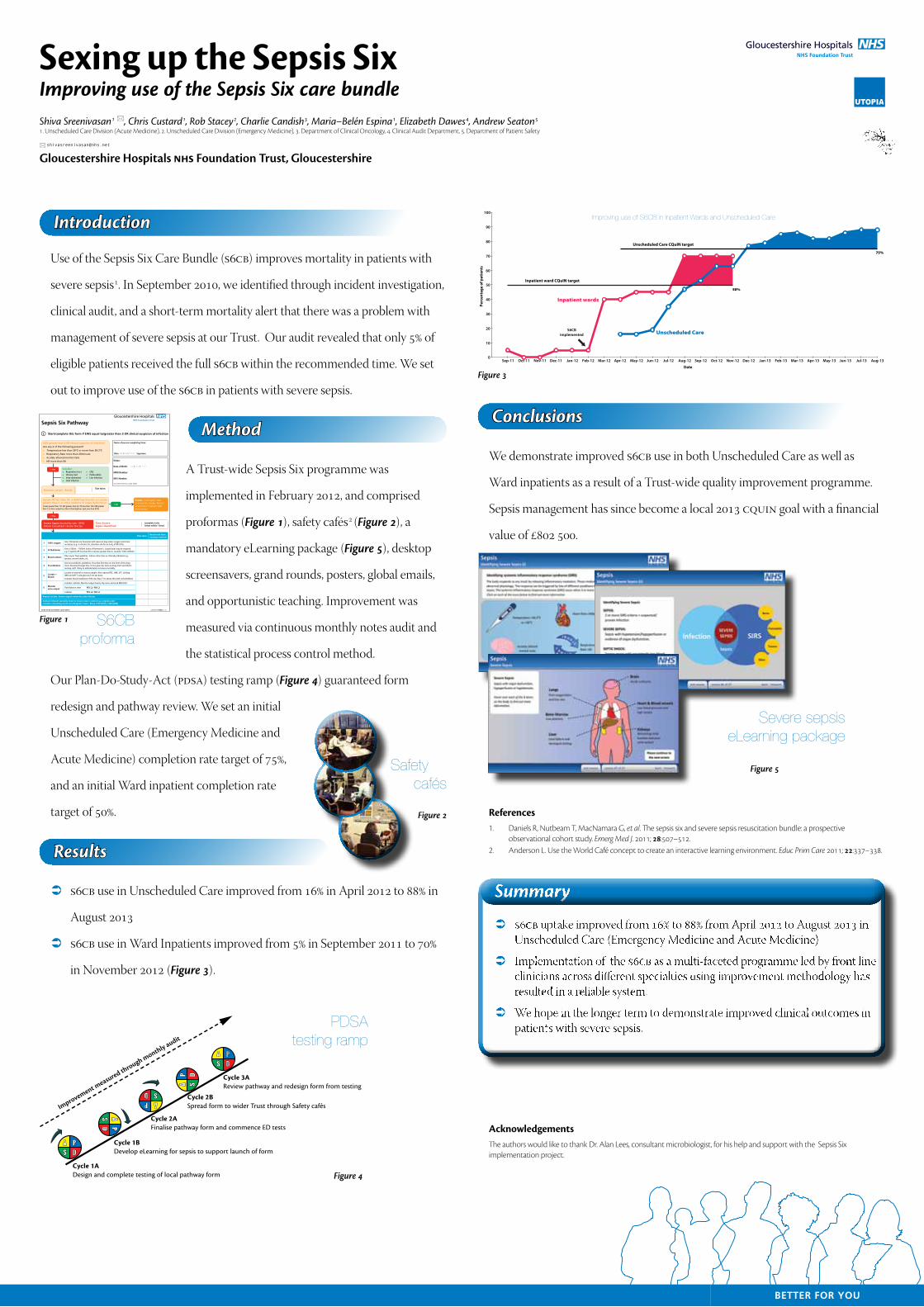
 S6CB use in Unscheduled Care improved from 16% in April 2012 to 88% in
August 2013
 S6CB use in Ward Inpatients improved from 5% in September 2011 to 70%
in November 2012 (Figure 3).
We demonstrate improved S6CB use in both Unscheduled Care as well as
Ward inpatients as a result of a Trust-wide quality improvement programme.
Sepsis management has since become a local 2013 CQuIN goal with a financial
value of £802 500.
References1. Daniels R, Nutbeam T, MacNamara G, et al. The sepsis six and severe sepsis resuscitation bundle: a prospective
observational cohort study. Emerg Med J. 2011; 28:507–512.2. Anderson L. Use the World Café concept to create an interactive learning environment. Educ Prim Care 2011; 22:337–338.
AcknowledgementsThe authors would like to thank Dr. Alan Lees, consultant microbiologist, for his help and support with the Sepsis Six implementation project.
Introduction
Method
Results
Conclusions
Time Severe Sepsis Identified:
(complete tasks below within 1 hour)
Time taken:
Sepsis. Investigate, treat and monitor closely. Restart assessment if patient later deteriorates
Sepsis Six Pathway
EWS greater than 3 OR clinical suspicion of infection?
Are any 2 of the following present?
Temperature less than 36ºC or more than 38.3ºC
Respiratory Rate more than 20/minute
Acutely altered mental state
HR more than 90
Consider: Respiratory tract Urinary tract Intra-abdominal Joint infection
CNS Endocarditis Line infection
Measure Lactate - Result:
Name of person completing form:
Date: DD / MM / YYYY Signature:
Systolic BP less than 90, or MAP less than 65, or Lactate greater than 2, or other evidence of organ dysfunction(Creat greater than 177, Bili greater than 34, Plt less than 100, INR greater than 1.5, Urine output less than 0.5mL/kg/hour, SpO2 less than 90%)
Time doneReason not done. Continue overleaf
1 100% oxygenGive 15L/minute via facemask with reservoir bag unless oxygen restriction necessary (e.g. in chronic CO2 retention aim for an SaO2 of 88-92%).
2 IV fluid bolusGive a 500mL - 1000mL bolus of Hartmann’s. Larger bolus may be required e.g. if systolic BP less than 90 or lactate greater than 4, consider 1500–2000ml
3 Blood culturesTake as per Trust guideline. Culture other sites as clinically indicated e.g. sputum, wound swabs, etc.
4 IV antibioticsUse trust antibiotic guidelines. Prescribe first dose on the front of the drug chart. Document target time (‘to be given by’-time) in drug chart and inform nursing staff. Delay in administration increases mortality.
5Lactate + bloods
Lactate on arterial or venous sample. Also request FBC, U&E, LFT, clotting (INR and APTT) and glucose if not yet done.
Consider blood transfusion if Hb less than 7 (or above this with comorbidities)
6Monitor urine output
Consider catheter. Monitor output hourly. Dip urine and send MSU/CSU.
Fluid balance chart YES / NO
Catheter YES / NO
Repeat Lactate. Ensure urgent review by senior Doctor
Contact relevant specialty team to ensure source control e.g. surgeons and consider contacting Acute Care Response Team - Bleep 1700 (CGH), 2700 (GRH)
If Yes
If No
If Yes
GHNHSFT/Y1055/07_12TO BE FILED IN PATIENT CASE NOTES
Name:
Date of Birth: DD / MM / YYYY
MRN Number:
NHS Number:
(OR AFFIX HOSPITAL LABEL HERE)
Start/complete this form if EWS equal to/greater than 3 OR clinical suspicion of infection
Severe Sepsis (mortality rate ~35%) Inform Consultant / Senior Doctor
Figure 1 S6CB proforma
Safety cafés
Figure 2PD
S A
PD S
A
P DSA
PDS
A
Improvement measured through monthly audit
PDS
A
Cycle 1ADesign and complete testing of local pathway form
Cycle 1BDevelop eLearning for sepsis to support launch of form
Cycle 2AFinalise pathway form and commence ED tests
Cycle 2BSpread form to wider Trust through Safety cafés
Cycle 3AReview pathway and redesign form from testing
Figure 4
PDSA testing ramp
Figure 5
Severe sepsis eLearning package
Figure 3
Aug-13 Sep-11 Oct-11 Nov-11 Dec-11 Jan-12 Feb-12 Mar-12 Apr-12 May-12 Jun-12 Jul-12 Aug-12 Sep-12 Oct-12 Nov-12 Dec-12 Jan-13 Feb-13 Mar-13 Apr-13 May-13 Jun-13 Jul-13
100
0
10
20
30
40
50
60
70
80
90
Date
Perc
enta
ge o
f pat
ient
s
Unscheduled Care CQuIN target
Inpatient ward CQuIN target
S6CBimplemented
50%
75%
Unscheduled Care
Inpatient wards
Improving use of S6CB in Inpatient Wards and Unscheduled Care
UTOPIA
ÂÂ
ÂÂ
ÂÂ
Summary