sigmoidal myotomy for acute diverticulitis
TRANSCRIPT
Sigmoidal Myotomy for Acute Diverticulitis ~
MICHAEL REILLY, M.S., F .R.C.S .
Plymouth, England
Acu-rE diverticulitis is a condition com- monly seen in patients in southwest Eng- land, where the inhabitants of htrge rural communities live on a diet consisting largely of cream, but ter and pastry.
During the past nine years, the attthor has encountered 96 patients suffering with acute diverticulitis who have required hos- pitalization. Of these, 60 per cent were women with an average age of 70 ?ears, and 40 per cent were men, averaging 66 years of age. In the mildest cases, 47 pa- tients complained of pain and spasm in the left iliac fossa accompanied by flatulence and disturbance of the bowel habit. The diagnosis in these patients was confirmed by roentgenologic examination, and the}.' were treated conservatively "along medical lines."
Four patients, "in extremis," were ad- mit ted to the hospital with fecal peritonitis. Of these four, one died "too ill for any oper- ation," and the other three died after emer- gency cecostomy or colostomy.
The 45 remaining patients required surgi- cal management , which varied from simple laparotomy and drainage (when only a single perforated divert iculum was found) to proximal colostomy if there was a large mass in the pelvis with symptoms of ob- struction. Fourteen patients were included in this category, requiring the traditional operat ion of proximal co!ostomy and later resection of the involved segment and anas- tomosis. Of these patients four, who were elder!y, died "postoperatively" of cardiac or pulmonary complications.
I t was on routine inspection, two or three ?'ears ago, of portions of resected colon in such cases, that the author "first realized that there did not seem to be anything seriously the mat ter with the colon" once the pericolic inf lammation subsided. The re was no ulceration, inf lammat ion nor thick- ening of the muscle layer due to fibrosis. I t was, however., sufficient to cause a long stricture, fairly well demarcated at each end, and situated invariably in the lower half of the sigmoid flexure. This was in the region where there is a sort of physio- logic sphincter which relaxes normally at intervals to allow passage of feces into the rectum prior to evacuation. I t occurred to the author that the "pr imary lesion was not the condition of diverticulosis or diverticulitis but spasm or hyper t rophy of this circular muscle leading to rup- ture of diverticula from increased intra- luminar pressure." I t appeared to h im that
Abridgment of original article read at the joint meeting of the American Proctologic Society and the Section of Proctology of the Royal Society of Medicine, Philadelphia, Pennsylvania, May 9 to 14, 1964.
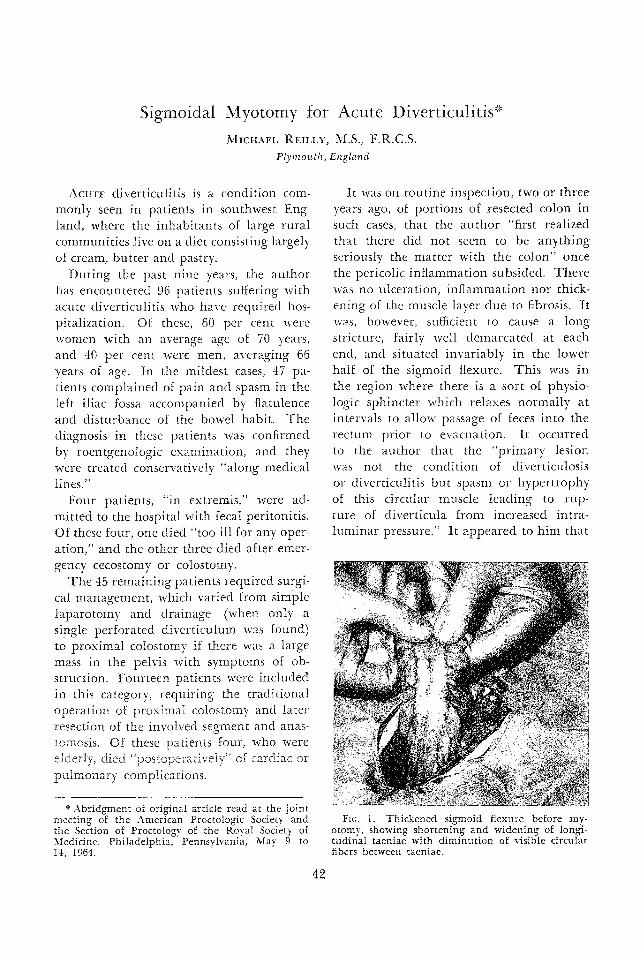
Fro. 1. Thickened sigmoid flexure before my- otomy, showing shortening and widening of longi- tudinal taeniae with diminut ion of visible circular fibers between taeniae.
42

SIGMOIDAL MYOTOMY FOR ACUTE DIVERTICULITIS 4.3
it migh t be a mistake to remove rou t ine ly
such relat ively hea l thy bowel, and be- sides, an anastomosis in such dtses is diffi-
cult because of shor t en ing and th icken ing of the mesentery which often is the only
visible resul t of past in f lammat ion , lVurther - more, such an anastomosis may break down
and leave a fecal fistula. He wondered if a less drastic and less hazardous opera t ion would suffice, i n view of the fact that the
sigmoid flexure is th ickened and the longi- tud ina l taeniae are shor tened and widened
(Fig. l), i t occurred to h i m that myotomy, s imilar to that of the Frede t -Ramsted t oper-
a t ion for hyper t rophic pyloric stenosis, migh t provide satisfactory resuhs.
Therefore , d u r i n g the last 18 m o n t h s , he has per formed such an opera t ion u p o n
the s igmoid flexure, e i ther with or w i thou t a p r e l imina ry colostomy, of 14 pa t ien t s - - the
first two were elderly patients, and they died of p u h n o n a r y embol i sm and coronary
sclerosis. T h e results in the r e m a i n i n g 12 pat ients have beer~ "highly satisfactory," b u t
the a u t h o r feels that it is too early to make an appraisa l of the pe rmanency of the re-
Fic. 2. Same specimen of colon with longitudinal myotomy carried out down to mucous membrane. Thickened longitudinal and circular muscle fibers can be seen wi~h some of the latter not yet divided. The mucous membrane can be seen bulging through.
~Fm. 3. Preoperative roentgenogram showing nan-owing and irregularity of lower sigmoid.
Fro. 4. Roentgenogram of same colon three months after operation, showing return of almosl: normal contour to affected s%m~lent of sigmnid~ although diverticula can still be seen. (The ap- pearance above the affected segment is out of the operative area and is due to an overlap of de- pendent transverse colon.)

44 Bm~Fom~
sults, the longest postoperative period being only nine months.
" T h e operat ion itself," he says, "is sur- prisingly easy." A longitudinal incision is made along the antecolic taenia over the length of the thickened bowel about ~ to 1 inch onto the normal bowel above and below (Fig. 2). T h e first incision is made with a scalpel and subsequently it is deep- ened carefully, using scissors, down to the mucous membrane , which should bulge through the length of the incision. I t is helpful, when cutting the deeper strands
of circular muscle between the haustra, if gentle lateral traction is made on the mar- gins of the incision with tissue forceps. Usu- ally, there is very little b leeding and cau- tery or ligation is rarely necessary.
Prior to operation, roentgenologic stud?: reveals typical narrowing and irregularity of the sigmoid flexure (Fig. 3). After a lapse of a few months, roentgenologic examina- tion reveals that the contour of the involved segment of bowel has become practically normal. However, in some instances, diver- ticula can be seen (Fig. 4).
Sigmoldovaginal Fistula Complicating Sigmoidal Diverticulitis'*
Report of Two Cases
FRED ~E. BRADFORD, M.D. ~b'onz the Department of Proctology, California Hospital,
Los Angeles, Calilornia
SrNc~ 1954, a more aggressive approach is being advocated in the management of diverticulitis of the colon. Prior to that time, surgical t reatment usually was re- served for perforation, abscesses and Other complications, and diverticulitis was man- aged conservatively as a medical problem.
Dur ing the past decade, the author be- lieves that a wholesome change has become apparen t in the at t i tude regarding treat- merit. Preventive or prophylactic resection of the involved port ion of the colon with immediate anastomosis in one stage is recommended, selecting an interval after the acute phase has subsided and before complications occur. Many authori~ties sup- ported this opinion in repor, ts published f rom 1956 to 1959. Recently an even bolder approach has been advocated, in which a resection is performed in one stage even in the presence of abscess formation, perito- nitis or perforation.
* Abridgment of ori~nal article read by title at the joint meeting of the American Proctologic So- ciety and the Section of Proctology of the Royal Society of Medicine, Philadelphia, Pennsylvania, May 9 to 14, 1964.
T h e author ventures .the opinion that many complications will be forestalled and fistula format ion may become a rarity if the current surgical trend con,tinues.
At present, fistulas, a c~istressing compli- cation of diverticulitis, are still encoun,tered occasionally and several varieties of fis- tulas are reported. In 1961, Bacon and McGregor 1 gave an accoun, t of 21 patients treated for sigmoidovesicat and sigmoido- u t e r ine fistulas, bu t none were afflicted with the sigmoidovaginal type. Careful review of medical li, terature discloses that colo- vaginal or sigmoidovaginal fistulas are often mertt ioned as possible complications, bu t rarely ,are any reported. Marshak 2 repor ted two such cases in 1948, and Morton3 listed four cases of colovaginal fistulas in 1946.
T h e author presents case reports of two patients encountered by him; a method for visualizing ,the course of such a fistula is provided in some detail and surgical treat- ment is discussed.
R e p o r t of Cases Case 1: "The first patient was an afebrile, white
woman, 39 years of age, who was first seen on