simulation to guide dose selection for 2014, the american …kinampark.com/plgaref/files/laffont...
TRANSCRIPT

Population Pharmacokinetic Modeling andSimulation to Guide Dose Selection forRBP-7000, A New Sustained-ReleaseFormulation of Risperidone
Celine M. Laffont, PhD1, Roberto Gomeni, PhD2, Bo Zheng, PhD3,Christian Heidbreder, PhD3, Paul J. Fudala, PhD3, and Azmi F. Nasser, PhD3
AbstractRBP-7000 is a long-acting formulation of risperidone designed for once-monthly subcutaneous injection for the treatment of schizophrenia. Theobjective was to estimate clinically effective doses of RBP-7000 based on model simulations and on the comparison with other long-acting injectableantipsychotics. A population pharmacokinetic model of RBP-7000 was developed in 90 clinically stable schizophrenic patients having received single/repeated doses of 60, 90, or 120mg. Model simulations were conducted to compare active moiety plasma exposure after repeated RBP-7000administrations to the published data of long-acting risperidone injection (Risperdal1 Consta1) at 25 and 50mg, and of paliperidone palmitate(Invega1 Sustenna1) at 50 and 100mg equivalent paliperidone. Predictions of dopamine D2 receptor occupancy were derived from the simulatedactive moiety concentrations. Simulations showed similar active moiety plasma exposure at steady-state for 90mg of RBP-7000 and 25mg of long-acting risperidone. In comparison to risperidone, RBP-7000 reached effective concentrations immediately after the first administration. RBP-7000 atthe doses of 60 and 90mg provided similar active moiety plasma concentrations at steady-state compared to 50 and 100mg equivalent paliperidone,respectively. These findings provide guidance for dose selection in Phase III clinical trials and suggest potential benefits for RBP-7000 over competitors.
KeywordsRBP-7000, long-acting risperidone, paliperidone palmitate, dopamine D2 receptor occupancy, dose switching simulation
RBP-7000 is a sustained-release formulation of risperi-done currently being developed for the treatment ofschizophrenia. RBP-7000 has been designed to beadministered by once-monthly subcutaneous (SC) injec-tion in order to address compliance issues associated withoral risperidone intake. Poor adherence to treatment isfrequent in schizophrenic patients prescribed oral anti-psychotic medications and has been identified as a majorbarrier to optimal outcomes as well as an important factorof relapse.1–4
RBP-7000 is injected subcutaneously using theATRIGEL1 delivery system. The ATRIGEL1 deliverysystem is a sterile, polymeric solution of a biodegradablepoly(DL-lactide-co-glycolide), or poly-L-lactic acid co-polymer, dissolved in N-methyl-2-pyrrolidone, a water-miscible, biocompatible solvent.5 The risperidone inRBP-7000 is both dissolved and suspended in thatpolymeric solution. After SC injection, the ATRIGEL1
delivery system solidifies upon contact with body fluidsand the resulting biodegradable implant delivers risperi-done in a controlled fashion over an extended period oftime. The tolerability and safety of RBP-7000 have beenestablished for doses of 60, 90, and 120mg in single andmultiple ascending dose studies performed in clinicallystable schizophrenic patients. The plasma concentration
profiles of risperidone and 9-hydroxyrisperidone afteradministration of RBP-7000 exhibited complex kinetics,presenting a double peak of absorption with a prolongedterminal half-life. These profiles suggest a rapid deliveryof risperidone from the SC injection site and a sustainedrelease from the ATRIGEL1 delivery system.
Pharmacokinetic/pharmacodynamic (PK/PD) model-ing and simulation was integrated throughout the clinicaldevelopment program of RBP-7000.6,7 The objective ofthis initial modeling was to characterize the relationshipbetween the administered doses, the active moietyexposure and efficacy/safety profiles, in order to guidedose selection for future Phase III trials. An importantconsideration for the selection of doses in Phase III trials
The Journal of Clinical Pharmacology55(1) 93–103© 2014, The American College ofClinical PharmacologyDOI: 10.1002/jcph.366
1Pharmacometrica, La Fouillade, France2Alleantis, Research Triangle Park, NC 27709, USA3Reckitt Benckiser Pharmaceuticals Inc., Richmond, Virginia VA23235, USA
Submitted for publication 1 April 2014; accepted 15 July 2014.
Corresponding Author:Azmi Nasser, PhD, Reckitt Benckiser Pharmaceuticals Inc.,Richmond, Virginia, VA 23235, USAE-mail: [email protected]
Pharmacometrics

is the comparison with other long-acting injectableantipsychotics at their clinically effective dosing regi-mens. Risperidone injection was the first approved long-acting injectable atypical antipsychotic with intramuscu-lar injections every 2 weeks (Risperdal1 Consta1;Janssen Pharmaceuticals, Inc.). The recommended dos-age regimen is 25mg but patients not responding to 25 mgmay benefit from a higher dose (37.5 or 50 mg). Oralrisperidone supplementation is recommended for the first3 weeks of treatment in order to ensure adequatetherapeutic plasma concentrations.8 Well-designed clini-cal studies have demonstrated the efficacy of risperidoneinjection and confirmed that its safety and tolerability arecomparable to those of oral risperidone.9–13 Paliperidonepalmitate, the palmitate ester of paliperidone, is a secondgeneration long-acting injectable antipsychotic designedfor the intramuscular route (Invega1 Sustenna1 JanssenPharmaceuticals, Inc.). Paliperidone, the 9-hydroxymetabolite of risperidone, exhibits approximately equalpharmacologic activity to the parent compound.14 As forRBP-7000, paliperidone palmitate is administered on amonthly basis, but the recommended clinical treatmentrequires two loading doses of 150 mg equivalent (mg eq.)paliperidone on day 1 and 100 mg equivalent paliperidoneon day 8, each administered into the deltoid muscle.15 Themonthly maintenance dose is in the range of 25–150 mgequivalent paliperidone injected in either the gluteal ordeltoid muscles, 75 mg equivalent paliperidone being therecommended dose.
The objective of the present analysis was to estimatethe doses of RBP-7000 that are expected to providesimilar active moiety exposure to long-acting risperidoneinjection and paliperidone palmitate during chronictreatment. A population PK model for RBP-7000 wasdeveloped from all available data collected in single andmultiple ascending dose studies in order to refine ourknowledge on the PK of this compound. The populationPK model was further used to predict the active moietyplasma concentration–time profiles after repeated dosesof RBP-7000 at 60, 90, and 120 mg and to compare theseprofiles with the published data of long-acting risperidoneinjection at the doses of 25 and 50 mg and paliperidonepalmitate at the doses of 50 and 100 mg equivalentpaliperidone. Predictions of dopamine (DA) D2 receptoroccupancy were also derived from active moiety plasmaconcentrations using a previously published PK/PDmodel.6
Methods and MaterialsDataThe population PK analysis of RBP-7000 was based ontwo clinical trials conducted in clinically stable schizo-phrenic patients. The first trial was a Phase I, randomized,open label, single ascending dose study where 45 subjects
received a single dose of 60, 90, or 120 mg of RBP-7000.Each of the three dose levels included 15 subjects. Serialblood samples were collected prior to RBP-7000 SCinjection on Day 1 (pre-dose sample) and at various timespost-injection from Day 1 to Day 85 (28 samples) toprovide full plasma concentration–time profiles ofrisperidone and 9-hydroxyrisperidone. All details onstudy design and blood sampling schedule are available inthe reference.6
The second trial was an open-label, Phase IIa, multipleascending dose study conducted in 45 subjects who wereon stable oral risperidone therapy (2, 3, or 4mg oncedaily). Subjects on 2, 3, or 4 mg/day oral risperidone wereswitched to 60, 90, or 120 mg of RBP-7000, respectively.Each of the three dose levels included 15 subjects. RBP-7000 treatment consisted of three monthly SC injectionsadministered on Day 1, Day 29, and Day 57. At the end ofthe third injection follow-up period, subjects werereturned to their original doses of oral risperidone for aperiod of 3 days (Day 85–87). For those subjects whowere not on a stable dose of 2, 3, or 4 mg of oralrisperidone at the beginning of the study, the screeningperiod was followed by a 7-day oral risperidoneconversion and stabilization period starting at 2mg/day.Subsequently, all subjects entered a 7-day pretreatmentperiod, with once daily oral administration of risperidoneat 2, 3, or 4 mg from Day-7 to Day-1 (the day precedingthe first injection of RBP-7000). Serial blood samples forPK assessments of risperidone and 9-hydroxyrisperidonewere collected prior to and after each injection of RBP-7000 throughout the dosing interval (19 samples after thefirst and third injections, 8 samples after the secondinjection) as well as during the initial pretreatment periodand switch-back period under oral risperidone. Furtherdetails on study design and blood sampling schedule areavailable in the published paper.7
The preferred site for RBP-7000 SC injection was theabdomen, in a location with adequate amounts of SCtissue that did not have excessive pigment, nodules,lesions, or hair. When multiple doses were administered,the injection in the abdomen was done on the oppositeside from the previous injection site. The clinical studyprotocol, informed consent forms, and all other appropri-ate study-related documents were reviewed and approvedby an independent and appropriately constituted Institu-tional Review Board. The study was conducted inaccordance with good clinical practice as required byUS Food and Drug Administration (FDA) regulations,International Conference on Harmonization (ICH) guide-lines, and standard operating procedures for clinicalinvestigation and documentation in force at ReckittBenckiser Pharmaceuticals Inc. (RBP). Compliancewith these requirements also indicates conformity withthe ethical principles that have their origins in theDeclaration of Helsinki. Plasma concentrations of
94 The Journal of Clinical Pharmacology / Vol 55 No 1 (2015)

risperidone and 9-hydroxyrisperidone were measuredusing a previously validated and published6 method ofliquid chromatography with tandem mass spectrometry(LC–MS/MS). The lower limit of quantitation (LLOQ)was 0.1 ng/mL for both analytes. The active moietyconcentrations were calculated as the sum of risperidoneand 9-hydroxyrisperidone plasma concentrations cor-rected by the molecular weight: [Active moiety]¼[Risperidone]þ [9-hydroxyrisperidone]� (410/426).
Population Pharmacokinetic AnalysisA population PK analysis was conducted to describejointly risperidone and 9-hydroxyrisperidone plasmaconcentrations collected in the single and repeated dosestudies of RBP-7000. As part of RBP-7000 developmentprogram, two population PK models sharing the samestructure had been successively developed to describe thePK data in each study separately.6,7 Thus, one objective ofthe present analysis was to refine the estimation of modelparameters and to better characterize the effects ofcovariates by pooling the data of the two studies togetherand increasing sample size.
The multiple ascending dose study included apretreatment period with oral risperidone. It was thereforenecessary to account for this initial exposure by modelingrisperidone and 9-hydroxyrisperidone data collectedduring that period. Oral risperidone pretreatment datahad been previously analyzed in previous work7 and thecorresponding estimated population PK model was usedin the present analysis with all parameters fixed. Thestructure of the oral risperidone model is displayed in theSupplemental Material (Figure S1) as well as modelparameter estimates (Table S1). Any details on oralrisperidone model building can be found in the previouspublication.7
The population PK analysis of RBP-7000 was carriedout in NONMEM software version 7.2 using the first-order conditional estimation with interaction (FOCE-I)method.16 NONMEM was run in a Windows Vistaoperating system with the FORTRAN compiler gfortranversion 4.6.0. Interindividual variability was estimatedon all structural model parameters, assuming a log-normal distribution. The residual variability was mod-eled using additive, proportional, and combined errormodel structures. The appropriateness of the model wasevaluated using various goodness-of-fit criteria, includ-ing standard diagnostic plots and the likelihood ratio test.The results for the likelihood ratio test were consideredstatistically significant when the difference in objectivefunction value between two nested models was more than3.84 (P< 0.05, one degree of freedom) throughout thebase model building process. All data preparation,summary statistics, graphics, exploratory analyses, andpost-processing of NONMEM outputs were performed inR software.17
Covariate AnalysisBody weight, body mass index (BMI), age, sex, race,cytochrome P450 2D6 (CYP2D6) phenotype, and RBP-7000 dose level were selected for the analysis. CYP2D6phenotype was predicted from the CYP2D6 genotypeaccording to the classification of ultrarapid, extensive,intermediate, and poor metabolizers as described in theliterature.18 The methodology for CYP2D6 genotypetesting is detailed in Gomeni’s paper.6 A preliminaryscreening of covariates was performed based on theexamination of the Empirical Bayes Estimates (EBEs) ofindividual PK parameters obtained from the base model(without covariates). Covariates showing a significant(P< 0.05) relationship with EBEs were further tested inNONMEM, as well as those for which a significant effectwas reported in previous population PK analyses of RBP-7000.6,7 Covariate model building in NONMEM was astepwise process, consisting of a forward and a backwardselection procedure. The likelihood ratio test was used toevaluate the significance of incorporating or removingfixed effects into the population model based on alphalevels that were set a priori (0.05 for the forward selectionand 0.001 for the backward selection).
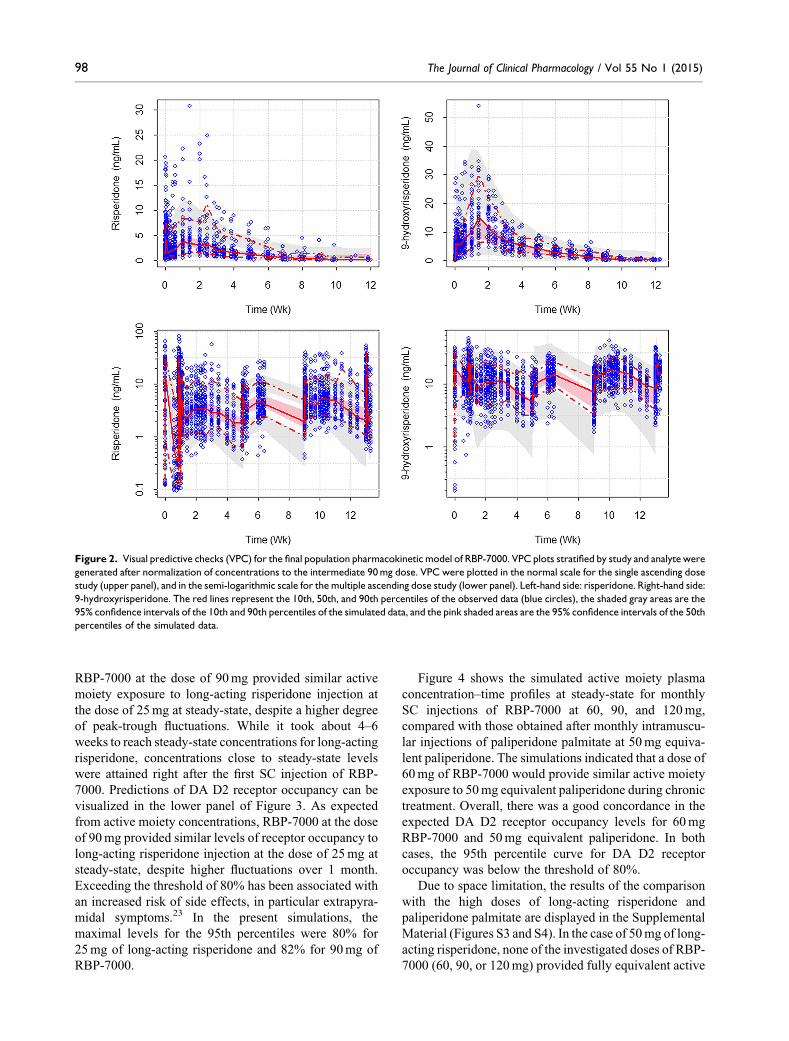
Model EvaluationModel evaluation was based on standard diagnostic plotsand visual predictive checks (VPC). VPC stratified bystudy and analyte were generated to evaluate the abilityof the model to correctly predict risperidone and9-hydroxyrisperidone plasma concentrations after singleand multiple SC injections of RBP-7000. At each nominaltime point, the observed plasma concentrations weresummarized by their 10th, 50th, and 90th percentiles, andthese percentiles were graphically compared to their 95%confidence intervals under the model. The 95% confi-dence intervals were computed by simulation from 500replicates of the original dataset.
Dose Assessment Simulation StudiesThe ultimate objective of the analysis was to estimate thedose of RBP-7000 that would provide similar activemoiety exposure to long-acting risperidone injection andpaliperidone palmitate during chronic treatment. Thereference active moiety plasma concentrations for long-acting risperidone and paliperidone palmitate wereextracted from a previous publication19 which reportedsimulations to evaluate the strategies for switching fromlong-acting risperidone to paliperidone palmitate. Twoscenarios were simulated in this publication: (i) a lowdose scenario, where 25 mg of long-acting risperidonewas switched to 50 mg equivalent paliperidone, and (ii) ahigh dose scenario, where 50 mg of long-acting risperi-done was switched to 100 mg equivalent paliperidone.These simulations were performed in a virtual populationof 5,000 schizophrenic patients receiving five injections
Laffont et al 95

of long-acting risperidone every 2 weeks, followed by 4injections of paliperidone palmitate every 4 weeksstarting 2 weeks after the last dose of long-actingrisperidone. The medians and 90% prediction intervalsof the simulated data were extracted from Samtani’spaper19 and compared to the expected active moietyplasma concentrations after multiple SC injections ofRBP-7000. Three SC injections of RBP-7000 adminis-tered every 4 weeks were simulated for comparison withlong-acting risperidone. These simulations were replicat-ed under steady-state conditions for comparison withpaliperidone palmitate. RBP-7000 simulations wereperformed using the final population PK model ofRBP-7000 for more than 5,000 schizophrenic patientshaving the same covariate distribution as in the originaldataset. Finally, a previously published PK/PD model6
was applied to predict DA D2 receptor occupancy levelsfrom the active moiety plasma concentrations. This wasan Emax model characterized by the following equation:
RO¼ROmax � C
Kd þ C
Where RO is the DA D2 receptor occupancy, ROmax isthe maximal receptor occupancy, C is the active moietyplasma concentration, and Kd is the apparent equilibriumdissociation constant (i.e., the active moiety plasmaconcentration for which 50% of maximal receptoroccupancy is achieved). As formost antipsychotics, ROmax
was fixed to 100%.20 The Kd parameter was reported to10.1 ng/mL.6
ResultsDataPK data were obtained in 90 clinically stable schizo-phrenic patients including 65 males and 25 females.Descriptive statistics of the demographic characteristicsare presented in Table 1. Overall, 7568 observations wereused for the population PK analysis, corresponding to3724 concentrations for risperidone and 3844 concen-trations for 9-hydroxyrisperidone. Drug concentrationsbelow the LLOQ (representing 3.5% of the data) werediscarded from the analysis.
Final Population PK ModelAs in previous PK analyses6,7, risperidone plasmaconcentrations after SC injection of RBP-7000 wereadequately described by a two-compartment model withfirst-order absorption and a transit compartment absorp-tion model. This complex absorption sub-model wasneeded to describe the double peak plasma concentrationprofiles observed for risperidone and its metabolite afterRBP-7000 administration. The first-order absorption rateconstant, ka1, accounts for the rapid absorption of
risperidone from the SC injection site corresponding tothe first peak. The transit compartment absorptionmodel21 mimics the slow delivery from the ATRIGEL1
delivery system corresponding to the second peak. Inagreement with the literature22, systemically-availablerisperidone was partly converted into 9-hydroxyrisper-idone and partly eliminated by other routes (biotransfor-mation into other metabolites and renal excretion). A one-compartment model with first-order elimination wasselected for 9-hydroxyrisperidone. Since there was no PKinformation available after administration of the metabo-lite, the apparent volume of distribution of the metabolitewas not identifiable and was set equal to the apparentcentral volume of distribution of the parent compound upto a constant that was common to all subjects (fixedeffect). The structure of the PK model is representedschematically in Figure 1. Model equations are providedin the Supplemental Material. Note that RBP-7000exhibits flip-flop kinetics where the apparent terminalhalf-life is driven by the slow absorption of risperidonefrom the ATRIGEL1 delivery system. This flip-flopkinetics increases the complexity of the model regardingthe interpretation of PK parameters.
Parameter estimates of the final population PK modelare shown in Table 2. A combined additive andproportional residual error model common to risperidoneand 9-hydroxyrispridone was selected. Interindividualvariability was estimated on all structural modelparameters. BMI and race were the only significantcovariates retained in the final model. BMI was found tohave an impact on ka1, the absorption rate constantassociated with the first peak, with lower values of ka1
in subjects having a higher BMI. This effect was
Table 1. Descriptive Statistics on the Demographic Data
Variable Value
N 90Age (years) 42.8 [9.8]Weight (kg) 87.8 [14.3]BMI (kg/m2) 28.5 [3.9]Sex (%)Female 27.8Male 72.2
Race (%)Black or African American 78.9White 18.9Others 2.2
Phenotype (%)Poor metabolizers 3.3Intermediate metabolizers 23.3Extensive metabolizers 70.0Ultrarapid metabolizers 3.3
Values are expressed as mean [standard deviation] unless stated otherwise.N: number of subjects. BMI: body mass index.
96 The Journal of Clinical Pharmacology / Vol 55 No 1 (2015)

modeled using an exponential relationship: ka1tv ¼
u1exp � u2 � BMI � 29:2ð Þð Þ where ka1tv is the typicalvalue, u1 and u2 are fixed effect parameters, and 29.2 is themedian BMI in the dataset. Race was found to have asignificant effect on ka2, the absorption rate constant ofthe transit compartment absorption model associated withthe second peak. More specifically, a twofold higher ka2
was estimated in Black subjects compared to the rest ofthe subjects (essentially composed of White subjects).Incorporating BMI in the model decreased interindividualvariability on ka1 from 54 to 44%, while incorporatingrace in the model decreased interindividual variability onka2 from 49% to 43%.
VPC stratified by study and analyte are shown inFigure 2. In order to increase to number of data points perplot and to refine the evaluation of the model, drug plasmaconcentrations were normalized to the intermediate 90mgdose (i.e., they were divided by the actual dose level andmultiplied by 90). Overall, the model provided a gooddescription of the data with respect to median concen-trations and variability. The secondary peak of themetabolite was slightly underestimated in the singleascending dose study compared to the multiple ascendingdose study. Also, variability was slightly underestimatedfor the metabolite, while it was well described for theparent compound. Standard diagnostic plots are displayedin the Supplemental Material (Figure S2) and do not showany apparent bias.
Dose Assessment Simulation StudiesThe results of RBP-7000 simulations are shown inFigures 3 and 4 for the comparison with long-actingrisperidone injection and paliperidone palmitate, respec-tively. The upper panel of Figure 3 shows the simulatedactive moiety plasma concentration–time profiles after 3SC injections of RBP-7000 at 60, 90, or 120 mgadministered every 4 weeks, compared with the activemoiety plasma concentration–time profiles of long-actingrisperidone at the dose of 25 mg administered every2 weeks over 10 weeks. The simulations indicated that
Figure 1. Population pharmacokinetic model for risperidone (Risp.) and 9-hydroxyrisperidone (9-OH-Risp.) after single/repeated subcutaneous(SC) injections of RBP-7000. ka1 is the rate constant for the rapid absorption of risperidone from the SC injection site (depot compartment); ka2 andktr are the absorption and transit rate constants of the transit compartment absorption model (compartments 1 to 5) used to mimic to slow deliveryfrom the ATRIGEL1 delivery system; krrp and krpr are the exchange rates between the central and peripheral compartments of risperidone; kr9 isthe rate constant for risperidone conversion into 9-hydroxyrisperidone; krel is the rate constant for risperidone elimination by other processes; k9el isthe elimination rate constant of 9-hydroxyrisperidone.
Table 2. Final Population PK Parameter Estimates (Relative StandardErrors of Estimates in %) for RBP-7000
Parameter Fixed effect Interindividual variability (%)
ka1 u1ð Þ h� 1� �
0.0151 (11) 44 (12)BMI on ka1 u2ð Þ 0.0803 (18)ka2; Blacks h� 1
� �0.0513 (11) 43 (13)
ka2;Others h� 1� �
0.0258 (16) 43 (13)ktr h� 1� �
0.0283 (7.1) 46 (13)V Lð Þ 125 (12) 27 (17)krel h� 1� �
0.0092 (55) 91 (29)kr9 h� 1� �
0.0474 (23) 66 (8.7)krrp h� 1� �
0.537 (11) 57 (11)krpr h� 1� �
0.0226 (12) 59 (14)k9el h� 1� �
0.0620 (5.2) 27 (20)Scaling factor SF 3.65 (17)Add. error (ng/mL) 0.0774 (2.0)Proportional error 0.335 (0.5)
Interindividual variability was expressed as a coefficient of variation(calculated as the standard deviation� 100). The apparent central volumeof distribution of risperidone and the apparent volume of distribution of 9-hydroxyrisperidone were equal V �SF and V, respectively.ka1tv ¼ u1 exp � u2 � BMI � 29:2ð Þð Þ, where ka1tv is the typical value of ka1,u1 and u2 are fixed-effect parameters, and 29.2 is the median value of BMI(body mass index) in the dataset.
Laffont et al 97
RBP-7000 at the dose of 90mg provided similar activemoiety exposure to long-acting risperidone injection atthe dose of 25 mg at steady-state, despite a higher degreeof peak-trough fluctuations. While it took about 4–6weeks to reach steady-state concentrations for long-actingrisperidone, concentrations close to steady-state levelswere attained right after the first SC injection of RBP-7000. Predictions of DA D2 receptor occupancy can bevisualized in the lower panel of Figure 3. As expectedfrom active moiety concentrations, RBP-7000 at the doseof 90 mg provided similar levels of receptor occupancy tolong-acting risperidone injection at the dose of 25 mg atsteady-state, despite higher fluctuations over 1 month.Exceeding the threshold of 80% has been associated withan increased risk of side effects, in particular extrapyra-midal symptoms.23 In the present simulations, themaximal levels for the 95th percentiles were 80% for25mg of long-acting risperidone and 82% for 90mg ofRBP-7000.
Figure 4 shows the simulated active moiety plasmaconcentration–time profiles at steady-state for monthlySC injections of RBP-7000 at 60, 90, and 120 mg,compared with those obtained after monthly intramuscu-lar injections of paliperidone palmitate at 50 mg equiva-lent paliperidone. The simulations indicated that a dose of60 mg of RBP-7000 would provide similar active moietyexposure to 50 mg equivalent paliperidone during chronictreatment. Overall, there was a good concordance in theexpected DA D2 receptor occupancy levels for 60 mgRBP-7000 and 50 mg equivalent paliperidone. In bothcases, the 95th percentile curve for DA D2 receptoroccupancy was below the threshold of 80%.
Due to space limitation, the results of the comparisonwith the high doses of long-acting risperidone andpaliperidone palmitate are displayed in the SupplementalMaterial (Figures S3 and S4). In the case of 50mg of long-acting risperidone, none of the investigated doses of RBP-7000 (60, 90, or 120 mg) provided fully equivalent active
Figure 2. Visual predictive checks (VPC) for the final population pharmacokinetic model of RBP-7000. VPC plots stratified by study and analyte weregenerated after normalization of concentrations to the intermediate 90mg dose. VPC were plotted in the normal scale for the single ascending dosestudy (upper panel), and in the semi-logarithmic scale for the multiple ascending dose study (lower panel). Left-hand side: risperidone. Right-hand side:9-hydroxyrisperidone. The red lines represent the 10th, 50th, and 90th percentiles of the observed data (blue circles), the shaded gray areas are the95% confidence intervals of the 10th and 90th percentiles of the simulated data, and the pink shaded areas are the 95% confidence intervals of the 50thpercentiles of the simulated data.
98 The Journal of Clinical Pharmacology / Vol 55 No 1 (2015)

moiety plasma exposure. The closest plasma concentra-tion levels were achieved with the 120 mg dose of RBP-7000. Additional model simulations showed that a higherdose of RBP-7000 would be required to achieve similaractive moiety plasma exposure to 50 mg of long-actingrisperidone. These aspects are further addressed in thediscussion section. Regarding paliperidone palmitate,RBP-7000 at the dose of 90 mg provided active moietylevels comparable to those obtained with 100 mgequivalent paliperidone.
DiscussionThe population PK analysis, based on two clinical studies,confirmed previous findings obtained by analyzing eachstudy separately.6,7 Especially, BMI was identified as asignificant covariate affecting the first peak of risperidoneand 9-hydroxyrisperidone. The first peak of risperidoneoccurred at a median time of 4–6 hours post-injection,
indicating that a fraction of the dose was not trapped in thebiodegradable implant formed by solidification of theATRIGEL1 delivery system but was readily available forabsorption. The impact of BMI on the first peak suggeststhat the adipose composition at the injection site (in theabdomen) influences the early absorption of risperidonewhich is a lipophilic drug. It is noteworthy that BMI wasalso identified as a significant covariate for the absorptionof paliperidone, also lipophilic, by the intramuscularroute.24
In contrast to previous population PK analyses (thesingle dose study contained almost exclusively Blacksubjects), race was identified as a statistically significantcovariate in the present analysis. Race was found to affectthe absorption rate constant for the second peak (ka2)whose estimate was twice higher in Black subjects than inthe rest of the subjects (essentially White subjects).Despite this difference, race had a limited impacton active moiety plasma concentration profiles: at
Figure 3. Simulation studies to compare active moiety plasma concentrations (upper panel) and dopamine D2 receptor occupancy (lower panel)after repeated doses of RBP-7000 (60, 90, 120mg) administered once per month and repeated doses of risperidone long-acting injectable formulation(25mg) administered every 2 weeks. Active moiety concentration data after long-acting risperidone injection were extracted from a publishedsimulation study19 where subjects received five injections of long-acting risperidone before switching to paliperidone palmitate on week 10. Long-acting risperidone data before week 10 were presented against RPB-7000 simulated data. Dopamine D2 receptor occupancy levels were simulatedfrom active moiety plasma concentrations using a previously published pharmacokinetic/pharmacodynamic model.6 The red curve and shaded pinkarea represent respectively the medians and 90% prediction intervals of RBP-7000 simulated data. The blue curve and shaded gray area representrespectively the medians and 90% prediction intervals of long-acting risperidone data.
Laffont et al 99

steady-state, the maximal plasma concentration (Cmax)was only 3.5% higher for the second peak in typical Blacksubjects than in typical White subjects having a medianBMI of 29 kg/m2, and 11% lower for the first peak. BMIhad a more pronounced effect than race on active moietyplasma concentrations: in typical White subjects, the Cmax
of the active moiety for the first peak was reduced byapproximately 38% as BMI increased from 19 to 35 kg/m2
under steady-state conditions. The secondary peak wasonly marginally affected by an increase in BMI. Since thesecond peak is related to the sustained release ofrisperidone from the ATRIGEL1 delivery systemresulting in prolonged plasma concentrations and showshigher or similar plasma levels compared to the first peak,no BMI-base dose adjustments are expected. Furtherinformation from the Phase III studies will be useful toaddress the BMI effect on the pharmacokinetics of RBP-7000.
Since the conversion of risperidone into 9-hydroxyr-isperidone is mainly driven by CYP2D6 polymorphicenzyme, CYP2D6 phenotype was expected to be aninfluential covariate on the PK of RBP-7000. TheCYP2D6 poor metabolizer phenotype has been shownto be associated with adverse drug reactions anddiscontinuation following risperidone treatment25 butalso with greater clinical improvement in total positiveand negative syndrome scale (PANSS) scores.26 In thepresent study, the preliminary analysis on EBEs sup-ported lower rates of conversion of risperidone to 9-hydroxyrisperidone (kr9) in CYP2D6 poor metabolizers,and higher rates of conversion in CYP2D6 ultrarapidmetabolizers, compared to intermediate or extensivemetabolizers in line with previous PK studies.27,28 Nosignificant difference was seen between CYP2D6intermediate and extensive metabolizers. Due to sizelimitations (only 3 poor metabolizers and 3 ultrarapid
Figure 4. Simulation studies to compare active moiety plasma concentrations (upper panel) and dopamine D2 receptor occupancy (lower panel) atsteady-state after once monthly injections of RBP-7000 (60, 90, 120mg) and once-monthly injections of paliperidone palmitate (50mg equivalentpaliperidone). Active moiety concentration data after paliperidone palmitate injection were extracted from a published simulation study19 wheresubjects received five injections of long-acting risperidone before switching to paliperidone palmitate on week 10. Steady-state data after week 18 arepresented against RPB-7000 simulated data. Dopamine D2 receptor occupancy levels were simulated from active moiety plasma concentrations usinga previously published pharmacokinetic/pharmacodynamic model.6 The red curve and shaded pink area represent respectively the medians and 90%prediction intervals of RBP-7000 simulated data. The blue curve and shaded gray area represent respectively the medians and 90% prediction intervalsof paliperidone palmitate data.
100 The Journal of Clinical Pharmacology / Vol 55 No 1 (2015)

metabolizers were included in the analysis), thesedifferences could not be reasonably tested in NONMEM.Thus, the present findings need to be re-evaluated whendata from larger clinical trials become available.
Overall, model parameter estimates were consistentwith previous parameter estimates obtained from theanalysis of repeated dose study data only.7 Smalldifferences were found with the parameter estimatesobtained from the analysis of single dose study data.6
These differences were mostly attributed to a differentcovariate model structure (no normalization to medianBMI) and to the inclusion of a dose-dependence on thevolume of distribution of risperidone and 9-hydroxyr-isperidone, leading to higher concentration–time profilesat higher doses. Such dose-dependence was not evidencedin the repeated dose study or in the present meta-analysis.
The population PK model of RBP-7000 was used tosimulate active moiety plasma concentrations afterrepeated doses of 60, 90, and 120 mg of RBP-7000 andto compare these concentrations with those expected afterrepeated administrations of long-acting risperidone (25 or50 mg) and paliperidone palmitate (50 or 100 mgequivalent paliperidone. Active moiety concentrationswere calculated to account for the activity of bothrisperidone and 9-hydroxyrisperidone. The pharmacolog-ical properties of the 9-hydroxy metabolite appear to becomparable to those of risperidone itself, both in respectof the profile of interactions with various neurotransmit-ters and its potency, activity, and onset and duration ofaction.33,34 And 9-hydroxyrisperidone has been approvedas paliperidone for the treatment of schizophrenia.Although the two compounds do not necessarily havethe same tissue distribution (especially, the brain-to-plasma concentration ratio is higher for risperidone thanfor its metabolite33), the combined risperidone and 9-hydroxyrisperidone plasma concentration is commonlyused to reflect overall body exposure. Furthermore, theactive moiety concentration has been shown to contributethe overall antipsychotic effects in the treatment and tocorrelate well with efficacy/safety endpoints.35,36
Reference competitor data were extracted from aprevious publication19 which reported the results of a PKsimulation study evaluating the strategies for switchingfrom long-acting risperidone (25 or 50 mg) to paliper-idone palmitate (50 or 100 mg equivalent paliperidone,respectively) in schizophrenic patients. This simulationstudy, in combination with others, was used to support thecurrent dosing recommendations of paliperidone palmi-tate and their approval by the US Food and DrugAdministration (FDA) and other regulatory agenciesaround the world.
The results of the present study indicated that a dose of60 mg of RBP-7000 should provide similar steady-stateactive moiety plasma levels to chronic administration of50 mg equivalent paliperidone, and that a dose of 90 mg of
RBP-7000 should provide similar steady-state activemoiety plasma levels to chronic administration of 25mgof long-acting risperidone. Given the linearity of thekinetics of long-acting risperidone over the dose range of12.5–50 mg8,29 and assuming that RBP-7000 kinetics islinear up to 180 mg, it can be extrapolated that 180 mg ofRBP-7000 would give equivalent active moiety plasmaexposure to 50 mg of long-acting risperidone, which wasconfirmed by additional PK simulations (not shown). Inthe case of paliperidone palmitate, previous studiesshowed that paliperidone exposure increased doseproportionally over the dose-range of 25–150 mg, butthat the peak concentrations were somewhat less thandose proportional for the higher doses due to slowerabsorption.24 More precisely, there was a decrease in theabsorption rate constant with an increase in the injectionvolume (0.5mL for 50 mg equivalent paliperidone, and1 mL for 100 mg equivalent paliperidone). This couldexplain our findings of comparable active moietyconcentration levels between 90 mg RBP-7000 and100 mg equivalent paliperidone in our simulations, while60 mg RBP-7000 and 50 mg equivalent paliperidoneprovided similar active moiety concentrations.
RBP-7000 and paliperidone palmitate are administeredonce per month and seem therefore more convenient forlong-term treatment than long-acting risperidone adminis-tered twice monthly. The results of the simulations showedthat RBP-7000 and paliperidone palmitate providedsustained concentration levels over 1 month of treatment(i.e.,median activemoiety concentration profiles at steady-state were very close for doses of 60mg RBP-7000 and50mg equivalent paliperidone). However, while theinitiation of paliperidone palmitate treatment requirestwo loading doses at Day 1 and at Day 8,15 active moietyconcentrations close to steady-state levels were attainedright after the first SC injection of RBP-7000. For long-acting risperidone, it took approximately 6 weeks from thestart of the therapy to reach steady-state concentrations.Thus, RBP-7000 would present an advantage over thecompetitors in the sense that it does not seem to require anyloading dose or supplementation with oral risperidone asrequired for paliperidone palmitate and long-actingrisperidone injection, respectively.
Our simulations also showed that the active moietyplasma concentrations fluctuated less after administrationof long-acting risperidone than after administration ofRBP-7000. The consequences on drug efficacy and safety(extrapyramidal side effects) were evaluated based on thepredictions of brain DA D2 receptor occupancy using apreviously published PK/PD model.6 DA D2 receptoroccupancy is recognized to be a key driver of clinicalefficacy and safety response to antipsychotic drugs. Thecurrently accepted hypothesis is that DA D2 receptoroccupancy should range from�65% to�80% for optimalantipsychotic effect and minimal extrapyramidal side
Laffont et al 101

effects.23 Available positron emission tomography (PET)data suggest that dosing long-acting risperidone at 25–50mg every 2 weeks is sufficient in attaining clinicalresponse with minimal risk of extrapyramidal symp-toms.30,31 In our simulations, the predicted 95th percen-tiles of DA D2 receptor occupancy were below 80%–82%for 90mg of RBP-7000 and 25 mg of long-actingrisperidone, hence supporting safety. The predicted 5thpercentiles were lower for 90 mg of RBP-7000 than for25mg of long-acting risperidone over the second half ofthe monthly dosing interval for RBP-7000 and the clinicalrelevance of this difference needs to be evaluated. It isnoteworthy that in the multiple ascending dose studyevaluating the switch from oral risperidone to RBP-7000,treatment with RBP-7000 led to similar and stablePANSS scores compared to oral risperidone.7 Thus, itappears that the fluctuations seen on RO predictions forRBP-7000 would have no noticeable impact on clinicalendpoints as assessed from PANSS scores measurements.
Concerning paliperidone palmitate, a recent post-hocanalysis of seven randomized controlled studies showedthat the incidence rates of spontaneously reportedextrapyramidal symptoms were generally lower forpaliperidone palmitate following approximately 90 daysof exposure compared to oral paliperidone followingapproximately 40 days of exposure at comparabledoses.32 Also, the use of medications for the treatmentof emergent extrapyramidal adverse events was signifi-cantly lower in paliperidone palmitate-treated patients(12%) than in oral paliperidone-treated patients (17%,P¼ 0.0035). In these studies, paliperidone palmitate wasadministered at doses ranging from 25 to 150 mgequivalent paliperidone. Since our simulations showedcomparable DA D2 receptor occupancy between 60 mgRBP-7000 and 50 mg equivalent paliperidone on onehand and between 90 mg RBP-7000 and 100 mg equiva-lent paliperidone on the other hand, one may reasonablyassume that the incidence rates of extrapyramidal sideeffects will also be low for RBP-7000 at these doses.
In conclusion, the population PK analysis of RBP-7000 confirmed previous knowledge and identified race asan additional covariate. BMI and race were found to havea statistically significant effect on the absorption of RBP-7000, with race having only limited impact on activemoiety plasma concentrations. Although these findingsneeds to be validated in larger PK studies, the presentsimulations suggest potential benefits of RBP-7000compared to other long-acting antipsychotics and providefurther guidance for dose selection in future Phase IIIclinical trials.
Declaration of Conflicting Interests
At the time this manuscript was submitted for publication, B.Zheng, C. Heidbreder, P.J. Fudala, and A.F. Nasser were full-time employees of Reckitt Benckiser Pharmaceuticals Inc. C.M.
Laffont and R. Gomeni were paid consultants for ReckittBenckiser Pharmaceuticals Inc.
Funding
This work was supported by Reckitt Benckiser PharmaceuticalsInc.
References01. Ayuso-Gutiérrez JL, del Río Vega JM. Factors influencing relapse
in the long-term course of schizophrenia. Schizophr Res.1997;28:199–206.
02. Cramer JA, Rosenheck R. Compliance with medication regimensfor mental and physical disorders. Psychiatr Serv. 1998;49:196–201.
03. Perkins DO. Predictors of noncompliance in patients withschizophrenia. J Clin Psychiatry. 2002;63:1121–1128.
04. Love RC, Conley RJ. Long-acting risperidone injection. Am JHealth Syst Pharm. 2004;61:1792–1800.
05. Malik K, Singh I, Nagpal M, Arora S, Atrigel: . A potentialparenteral controlled drug delivery system. Der Pharmacia Sinica.2010;1:74–81.
06. Gomeni R, Heidbreder C, Fudala PJ, Nasser AF . A model-basedapproach to characterize the population pharmacokinetics and therelationship between the pharmacokinetic and safety profiles ofRBP-7000, a new, long-acting, sustained-release formulation ofrisperidone. J Clin Pharmacol. 2013;53:1010–1019.
07. Laffont CM, Gomeni R, Zheng B, Heidbreder C, Fudala PJ, NasserAF . Population pharmacokinetics and prediction of dopamine D2receptor occupancy after multiple doses of RBP-7000, a newsustained-release formulation of risperidone, in schizophreniapatients on stable oral risperidone treatment. Clin Pharmacokinet.2014.
08. Risperdal1 Consta1 full prescribing information. Available from:http://www.risperdalconsta.com/sites/default/files/RisperdalCon-staPI.pdf [Accessed 2014 Feb].
09. Kane JM, Eerdekens M, Lindenmayer JP, Keith SJ, Lesem M,Karcher K . Long-acting injectable risperidone: efficacy and safetyof the first long-acting atypical antipsychotic. Am J Psychiatry.2003;160:1125–1132.
10. Chue P, Eerdekens M, Augustyns I, et al. Comparative efficacy andsafety of long-acting risperidone and risperidone oral tablets. EurNeuropsychopharmacol. 2005;15:111–117.
11. Fleischhacker WW, Eerdekens M, Karcher K, et al. Treatment ofschizophrenia with long-acting injectable risperidone: a 12-monthopen-label trial of the first long-acting second-generation antipsy-chotic. J Clin Psychiatry. 2003;64:1250–1257.
12. Moller HJ . Long-acting injectable risperidone for the treatment ofschizophrenia: clinical perspectives. Drugs. 2007;67:1541–1566.
13. Keith S . Use of long-acting risperidone in psychiatric disorders:focus on efficacy, safety and cost-effectiveness. Expert RevNeurother. 2009;9:9–31.
14. Heykants J, Huang ML, Mannens G, et al. The pharmacokinetics ofrisperidone inhumans: a summary.JClinPsychiatry. 1994;55:13–17.
15. Invega1 Sustenna1 full prescribing information. Available from:http://www.invegasustenna.com/pdf/invegasustenna-prescribing-info.pdf [Accessed 2014 Feb].
16. Beal S, Sheiner LB, Boeckmann A, Bauer RJ . NONMEM user’sguides-2013). Ellicott City, MD: Icon Development Solutions;1989:2013.
17. R: a language and environment for statistical computing. RFoundation for Statistical Computing; 2013. Available from:http://www.R-project.org [Accessed Sept 2013].
18. Hicks JK, Swen JJ, Thorn CF, et al. Clinical pharmacogeneticsimplementation consortium guideline for CYP2D6 and CYP2C19
102 The Journal of Clinical Pharmacology / Vol 55 No 1 (2015)

genotypes and dosing of tricyclic antidepressants. Clin PharmacolTher. 2013;93:402–408.
19. Samtani MN, Gopal S, Gassmann-Mayer C, Alphs L, Palumbo JM .Dosing and switching strategies for paliperidone palmitate. CNSDrugs. 2011;25:829–845.
20. Nucci G, Gomeni R, Poggesi I . Model-based approaches to increaseefficiency of drug development in schizophrenia: a can’t missopportunity. Expert Opin Drug Discov. 2009;4:837–856.
21. Savic RM, Jonker DM, Kerbusch T, Karlsson MO . Implementationof a transit compartment model for describing drug absorption inpharmacokinetic studies. J Pharmacokinet Pharmacodyn.2007;34:711–726.
22. Mannens G, Huang ML, Meuldermans W, Hendrickx J, Woes-tenborghs R, Heykants J . Absorption, metabolism, and excretion ofrisperidone in humans. Drug Metab Dispos. 1993;21:1134–1141.
23. Pani L, Pira L, Marchese G . Antipsychotic efficacy: relationship tooptimal D2-receptor occupancy. Eur Psychiatry. 2007;22:267–275.
24. Samtani MN, Vermeulen A, Stuyckens K . Population pharmaco-kinetics of intramuscular paliperidone palmitate in patients withschizophrenia: a novel once-monthly, long-acting formulation of anatypical antipsychotic. Clin Pharmacokinet. 2009;48:585–600.
25. De Leon J, Susce MT, Pan RM, Fairchild M, Koch WH, WedlundPJ. The CYP2D6 poor metabolizer phenotype may be associatedwith risperidone adverse drug reactions and discontinuation. J ClinPsychiatry. 2005;66:15–27.
26. Almoguera B, Riveiro-Alvarez R, Lopez-Castroman J, et al.CYP2D6 poor metabolizer status might be associated with betterresponse to risperidone treatment. Pharmacogenet Genomics.2013;23(11):627–630.
27. Vermeulen A, Piotrovsky V, Ludwig EA . Population pharmacoki-netics of risperidone and 9-hydroxyrisperidone in patients withacute episodes associated with bipolar I disorder. J PharmacokinetPharmacodyn. 2007;34:183–206.
28. Feng Y, Pollock BG, Coley K, et al. Population pharmaco-kinetic analysis for risperidone using highly sparse samplingmeasurements from the CATIE study. Br J Clin Pharmacol.2008;66:629–639.
29. Eerdekens M, Van Hove I, Remmerie B, Mannaert E. Pharmacoki-netics and tolerability of long-acting risperidone in schizophrenia.Schizophr Res. 2004;70(1):91–100.
30. Remington G, Mamo D, Labelle A, et al. A PET study evaluatingdopamine D2 receptor occupancy for long-acting injectablerisperidone. Am J Psychiatry. 2006;163(3):396–401.
31. Chue P. Long-acting risperidone injection: efficacy, safety, andcost-effectiveness of the first long-acting atypical antipsychotic.Neuropsychiatr Dis Treat. 2007;3(1):13–39.
32. Gopal S, Liu Y, Alphs L, Savitz A, Nuamah I, Hough D . Incidenceand time course of extrapyramidal symptoms with oral and long-acting injectable paliperidone: a posthoc pooled analysis of sevenrandomized controlled studies. Neuropsychiatr Dis Treat.2013;9:1381–1392.
33. van Beijsterveldt LE, Geerts RJ, Leysen JE, Megens AA, Van denEynde HM, Meuldermans WE, Heykants JJ . Regional braindistribution of risperidone and its active metabolite 9-hydroxy-risperidone in the rat. Psychopharmacology. 1994;114(1):53–62.
34. Heykants J1, Huang ML, Mannens G, Meuldermans W, Snoeck E,Van Beijsterveldt L, Van Peer A, Woestenborghs R . Thepharmacokinetics of risperidone in humans: a summary. J ClinPsychiatry. 1994:13–17.
35. Huang ML, Van Peer A, Woestenborghs R, De Coster R, HeykantsJ, Jansen AAI, Zylicz Z, Visscher HW, Jonkman JHG .Pharmacokinetics of the novel antipsychotic agent risperidoneand the prolactin response in healthy subjects. Clin PharmacolTher. 1993;54:257–268.
36. Regenthal R, Kunstler U, Hesse S, Sabri O, Preiss R. D2 dopaminereceptor occupancy, risperidone plasma level and extrapyramidalmotor symptoms in previously drug-free schizophrenic patients. IntJ Clin Pharmacol Ther. 2005;43(8):370–378.
Supporting InformationAdditional supporting information may be found in theonline version of this article at the publisher’s web-site.
Laffont et al 103